

The Incidence of Dental Caries in Children with Down Syndrome: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion Criteria
2.3. Selection Process
2.4. Data Extraction
2.5. Methodological Quality Assessment
2.6. Data Synthesis and Meta-Analysis
3. Results
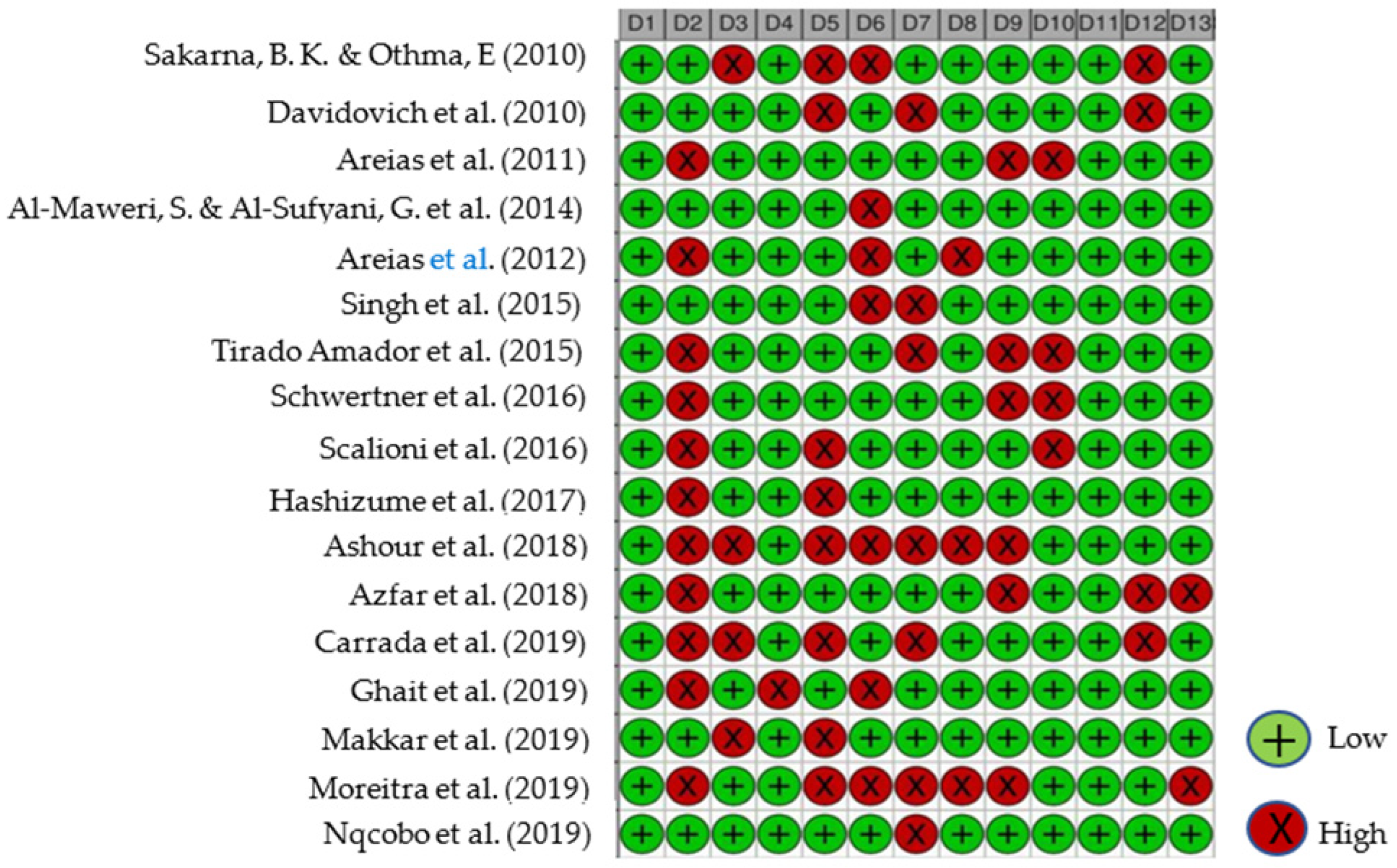
3.1. Risk of Bias
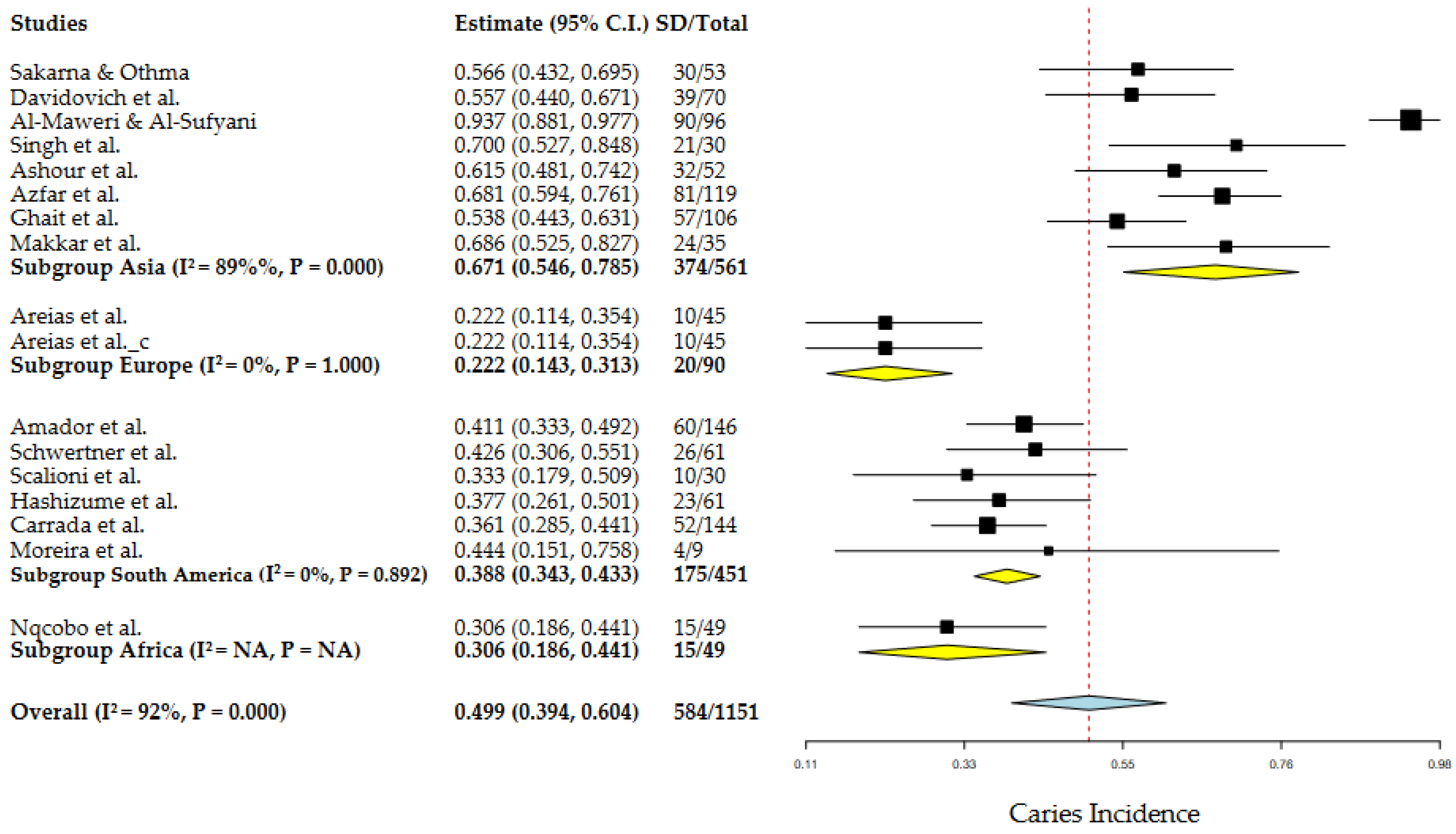
3.2. Meta-Analysis
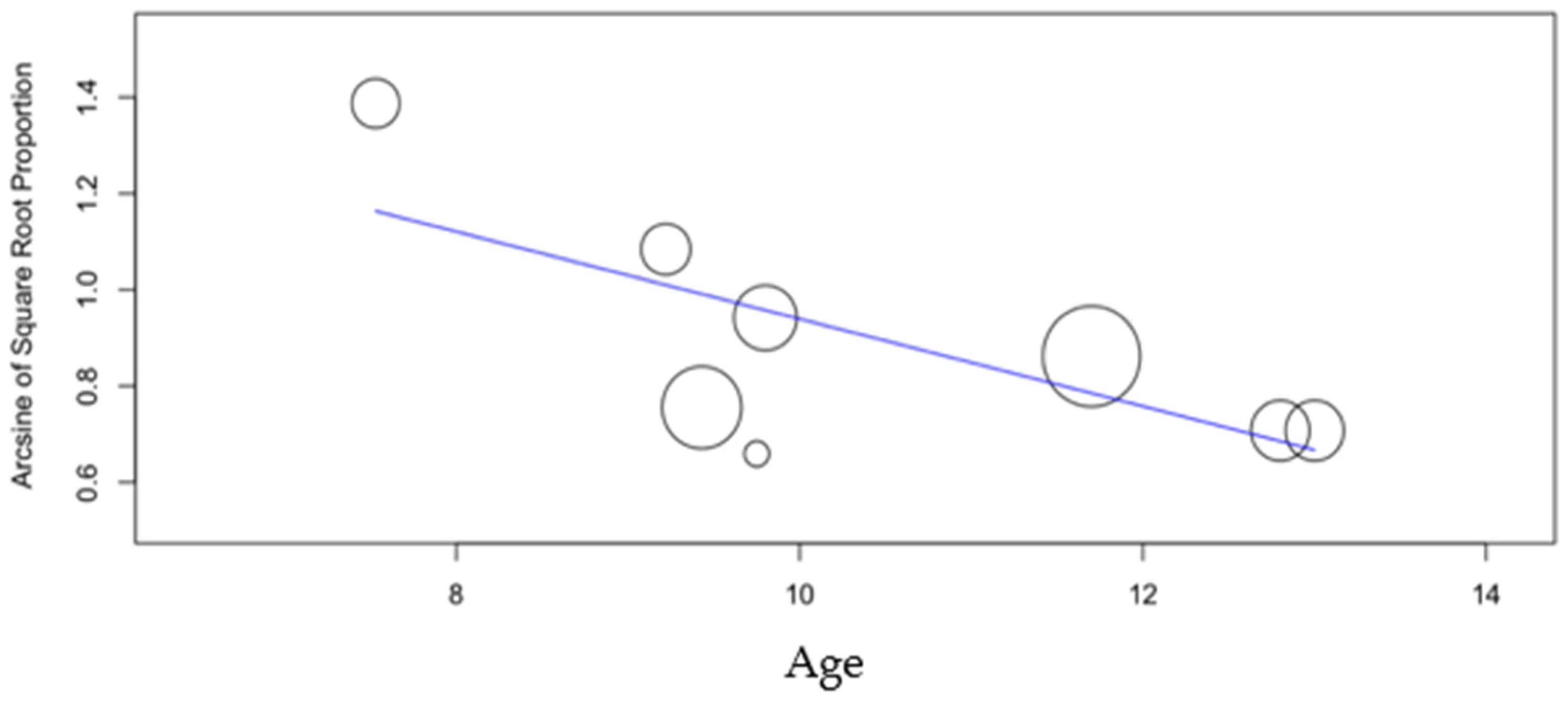
3.3. Age
3.4. Male/Female Ratio
3.5. DMFT/dmft Indices
3.6. Latitude
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 2 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 2 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 3 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 3 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | 3 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | 3 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | 3 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | 3 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | 4 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | 4 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | 3 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | 3,4 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | 3,4 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | 3,4 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | 3,4 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | 3,4 | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | 3,4 | |
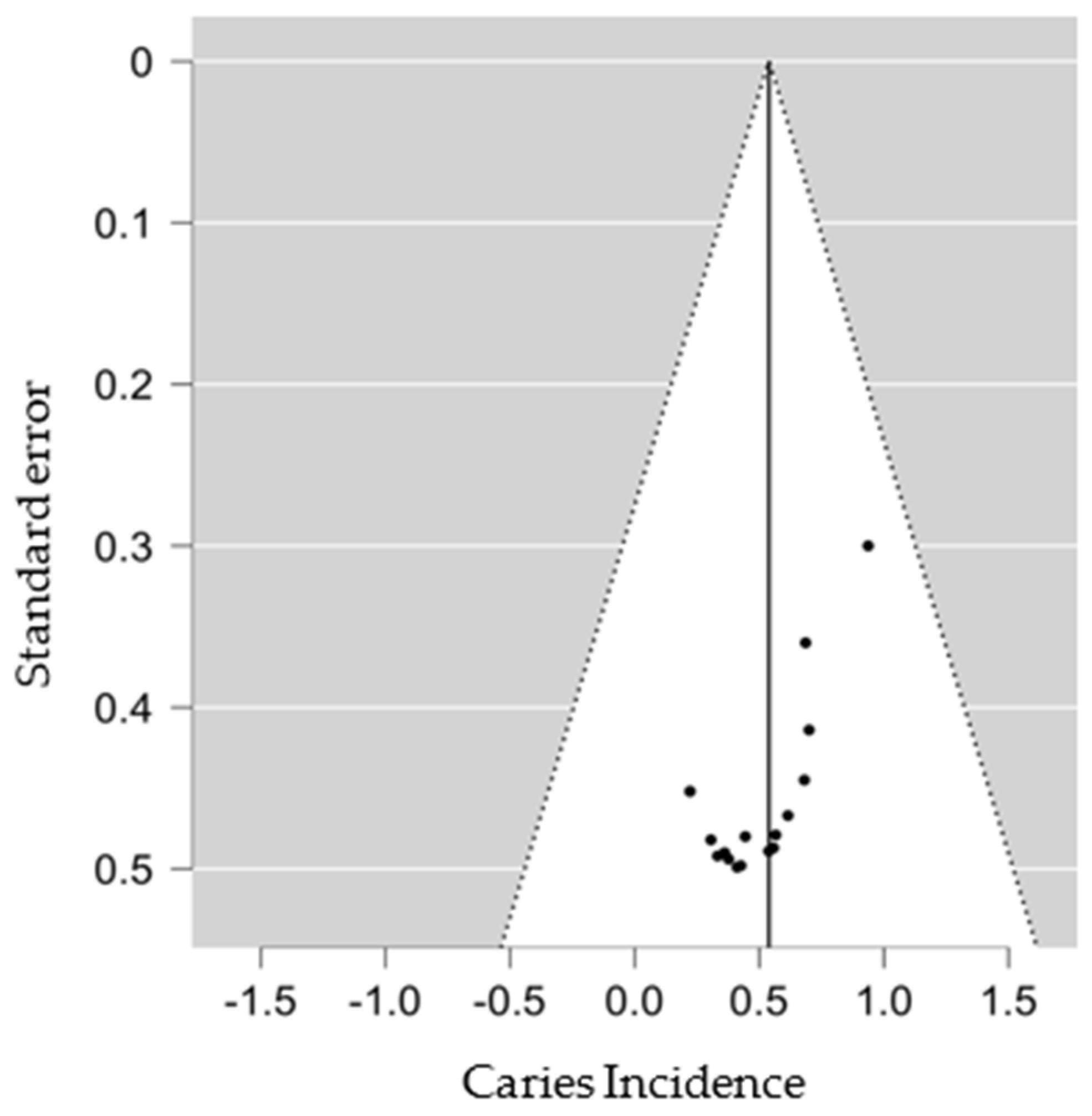
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | 4 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | 4 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | 4 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | 4–5 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | 4–5 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | 7 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimates and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | 6–13 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | 6–13 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | 6–13 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | 6–13 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | 6–13 | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | 6–13 |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | 6–13 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 14–15 |
| 23b | Discuss any limitations of the evidence included in the review. | 14–15 | |
| 23c | Discuss any limitations of the review processes used. | 14–15 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | 14–15 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | 3 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | 3 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | 3 | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | - |
| Competing interests | 26 | Declare any competing interests of review authors. | - |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | 17–24 |



References
- Santangelo, C.N.; Gomes, D.P.; Vilela, L.O.; de Deus, T.S.; Vilela, V.O.; Santos, E.M. Avaliação das características bucais em pacientes portadores de síndrome de Down da APAE de Mogi das Cruzes—SP. ConScientiae Saúde 2008, 7, 29–34. [Google Scholar] [CrossRef]
- Gupta, N.A.; Kabra, M. Diagnosis and management of Down syndrome. Indian J. Pediatr. 2014, 81, 560. [Google Scholar] [CrossRef] [PubMed]
- Descamps, I.; Fernandez, C.; Van Cleynenbreugel, D.; Van Hoecke, Y.; Marks, L. Dental care in children with down syndrome: A questionnaire for belgian dentists. Med. Oral Patol. Oral Cirugía Bucal 2019, 24, 3851. [Google Scholar] [CrossRef] [PubMed]
- Faria, F.G.; Lauria, R.A.; Bittencourt, M.A.V. Dental and skeletal characteristics of patients with Down Syndrome. RGO Rev. Gauch. Odontol. 2013, 61, 121. [Google Scholar]
- Macho, V.M.P.; Seabra, M.; Pinto, A.; Soares, D.; Andrade, C. Alterações craniofaciais e particularidades orais na trissomia 21. Acta Pediatr. Port. 2008, 39, 190. [Google Scholar]
- Araújo, D.L.; Brito, M.V.D.S.; Felipe, L.C.S. Pacientes com síndrome de Down na odontologia: Revisão de literatura. Facit Bus. Technol. J. 2022, 2, 145. [Google Scholar]
- Leites, A.C.B.R.; Pinto, M.B.; Sousa, E.R. Aspetos microbiológicos da cárie dental. Rev. Salusvita 2006, 25, 135. [Google Scholar]
- Meyer, F.; Enax, J. Early Childhood Caries: Epidemiology, Aetiology, and Prevention. Int. J. Dent. 2018, 2018, 1415873. [Google Scholar] [CrossRef] [Green Version]
- Narvai, P.C. Cárie dentária e flúor: Uma relação do século XX. Ciência Saúde Coletiva 2000, 5, 381. [Google Scholar] [CrossRef] [Green Version]
- Pereira, C.M.; Santos, N.S.; Carlos, L.A.; Neto, O.A.T.; Andrade, L.A. Avaliação de doença periodontal e cárie em pacientes com síndrome Down: Incidência, características e conduta preventiva. Espec. Med. Saúde 2022, 22, 136. [Google Scholar] [CrossRef]
- Mesquita, T.M.S.M. O Paciente Odontopediátrco Com Síndrome Down Em Clinica Dentária; Mestrado, Universidade Fernando Pessoa: Porto, Portugal, 2014. [Google Scholar]
- Pereira, E. Levantamento das Doenças Bucais Prevalentes Nos Portadores de Síndrome Down: Uma Revisão de Literatura; Cirurgião-dentista, Centro Universitário Uniguairacá: Paraná, Brasil, 2021. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deps, T.D.; Angelo, G.L.; Martins, C.C.; Paiva, S.M.; Pordeus, I.A.; Borges-Oliveira, A.C. Association between Dental Caries and Down Syndrome: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0127484. [Google Scholar] [CrossRef]
- Robertson, M.D.; Schwendicke, F.; Araujo, M.P.; Radford, J.R.; Harris, J.C.; Mcgregor, S.; Innes, N.P.T. Dental caries experience, care index and restorative index in children with learning disabilities; A systematic review and meta-analysis. BMC Oral Health 2019, 19, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.C.P.M.; Lyra, M.C.A.; Almeida, H.C.R.; Filho, A.V.A.; Heimer, M.V.; Rosenblatt, A. Caries experience in children and adolescents with Down Syndrome: A systematic review and meta-analysis. Arch. Oral Biol. 2020, 115, 104715. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 2012, 65, 934. [Google Scholar] [CrossRef] [PubMed]
- Der Simonian, R.; Laird, N. Meta-Analysis in Clinical Trials revisited. Contemporary Clin. Trials 2015, 45, 139. [Google Scholar] [CrossRef] [Green Version]
- Wallace, B.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Arora, R.; Bhayya, D.; Singh, D.; Sarvaiya, B.; Mehta, D. Comparison of relationship between salivary electrolyte levels and dental caries in children with down syndrome. J. Nat. Sci. Biol. Med. 2015, 6, 144. [Google Scholar] [CrossRef] [Green Version]
- Scalioni, F.; Carrada, C.; Machado, F.; Devito, K.; Ribeiro, L.C.; Cesar, D.; Ribeiro, R. Salivary density of Streptococcus mutans and Streptococcus sobrinus and dental caries in children and adolescents with down syndrome. J. Appl. Oral Sci. 2017, 25, 250. [Google Scholar] [CrossRef] [Green Version]
- Sakarna, B.K.; Othma, E. Dentofacial changes and oral health status in individuals with down syndrome in jordan—Cross sectional study. Pak. Oral Dent. J. 2010, 30, 159–161. [Google Scholar]
- Davidovich, E.; Afromian, D.J.; Shapira, J.; Peretz, B. A comparison of the sialochemistry, oral pH, and oral health status of down syndrome children to healthy children. Intern. J. Paediatr. Dent. 2010, 20, 235. [Google Scholar] [CrossRef] [PubMed]
- Areias, C.M.; Sampaio-Maia, B.; Guimarães, H.; Melo, P.; Andrade, D. Caries in portuguese children with down syndrome. Clinics 2011, 66, 1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Maweri, S.; Al-Sufyani, G. Dental caries and treatment needs of Yemeni children with down syndrome. J. Dent. Res. 2014, 11, 631. [Google Scholar]
- Areias, C.M.; Sampaio-Maia, B.; Pereira, M.L.; Azevedo, A.; Melo, P.; Andrade, C.; Scully, C. Reduced salivary flow and colonization by mutans streptococci in children with Down syndrome. Clinics 2012, 67, 1007. [Google Scholar] [CrossRef]
- Amador, L.T.; Cárdenas, S.D.; Martínez, K.R. Salud bucal en escolares con síndrome de Down en Cartagena (Colombia). Rev. Clin. Med. Fam. 2015, 8, 110. [Google Scholar] [CrossRef] [Green Version]
- Schwertner, C.; Moreira, M.J.S.; Faccini, L.S.; Hashizume, L.N. Biochemical composition of the saliva and dental biofilm of children with Down syndrome. Int. J. Paediatr. Dent. 2016, 26, 134. [Google Scholar] [CrossRef]
- Hashizume, L.N.; Schwertner, C.; Moreira, M.J.S.; Coitinho, A.S.; Faccini, L.S. Salivary secretory IgA concentration and dental caries in children with Down syndrome. Spec. Care Dent. 2017, 37, 115. [Google Scholar] [CrossRef]
- Ashour, N.A.; Ashour, A.A.; Basha, S. Association between body mass index and dental caries among special care female children in Makkah City. Ann. Saudi Med. 2018, 38, 28. [Google Scholar] [CrossRef] [Green Version]
- Azfar, M.; Khan, I.; Iqbal, N.; Khawar, N.; Abid, K. Oral Health of Individuals with Down Syndrome in Karachi, Pakistan. J. Pak. Dent. Assoc. 2018, 27, 190. [Google Scholar] [CrossRef] [Green Version]
- Carrada, C.F.; Scalioni, F.A.R.; Abreu, L.G.; Ribeiro, R.A.; Paiva, S.M. Impact of oral conditions of children/adolescents with Down syndrome on their families’ quality of life. Spec. Care Dent. 2020, 40, 175. [Google Scholar] [CrossRef]
- Ghaith, B.; Al Halabi, M.; Khamis, A.H.; Kowash, M. Oral Health Status among Children with Down Syndrome in Dubai, United Arab Emirates. J. Int. Soc. Prev. Community Dent. 2019, 9, 232. [Google Scholar] [CrossRef] [PubMed]
- Makkar, A.; Indushekar, K.R.; Saraf, B.G.; Sardana, D.; Sheoran, N. A cross sectional study to evaluate the oral health status of children with intellectual disabilities in the National Capital Region of India (Delhi-NCR). J. Intellect. Disabil. Res. 2019, 63, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, M.J.S.; Klaus, N.M.; Dall’Onder, A.P.; Grando, D.; Parolo, C.C.F.; Faccini, L.S.; Hashizume, L.N. Genotypic diversity and acidogenicity of Streptococcus mutans in Down syndrome children. Spec. Care Dent. 2019, 39, 578. [Google Scholar] [CrossRef] [PubMed]
- Nqcobo, C.; Ralephenya, T.; Kolisa, Y.M.; Esan, T.; Yengopal, V. Caregivers’ perceptions of the oral-health-related quality of life of children with special needs in johannesburg, south africa. Health SA Gesondheid 2019, 24, a1056. [Google Scholar] [CrossRef] [PubMed]
- Mbatna, J.J.; Mendes, N.U.; Joaquim, D.C.; Cruz, G.S.; Benedito, F.C.S.; Sousa, D.F.; Silva, C.H.F.; Leite, A.C.R.M. Manifestações orais em crianças com síndrome de down: Uma revisão integrativa da literatura. Braz. J. Dev. 2020, 6, 20401. [Google Scholar] [CrossRef]
- Pinto, J.M.; Calisto, V.; Guachamin, V.; Mendieta, F. Patologías bucales asociadas a una población infantil con Síndrome de Down de la fundación el triángulo de Quito. Ecuador. Rev. KIRU 2019, 16, 164. [Google Scholar] [CrossRef]
- Gonçalves, S.S.; Canalli, C.D.S.E.; Babinski, S.G.; Babinski, J.W.; Miasato, J.M. Levantamento das condições de cárie e doença periodontal na associação de portadores da síndrome de Down em Teresópolis-RJ. Rev. Odontol. Univ. Cid. São Paulo 2017, 22, 19. [Google Scholar] [CrossRef] [Green Version]
- Ritwik, P.; Patterson, K.K. Diagnosis of tooth agenesis in childhood and risk for neoplasms in adulthood. Ochsner J. 2018, 18, 345. [Google Scholar] [CrossRef]
- Shukla, D.; Bablani, D.; Chowdhry, A.; Thapar, R.; Gupta, P.; Mishra, S. Dentofacial and Cranial Changes in Down Syndrome. Osong Public Health Res. Perspect. 2014, 5, 339. [Google Scholar] [CrossRef] [Green Version]
- Kalyoncu, I.Ö.; Giray, F.E.; Tanboga, I. Parent’s attitudes and knowledge on oral health in a group of individuals with Down syndrome in Turkey. J. Pak. Med. Assoc. 2018, 68, 1368. [Google Scholar]
- Castilho, A.R.F.; Marta, S.N. Avaliação da incidência de cárie em pacientes com syndrome de down após sua inserção em um programa preventivo. Rev. Ciência Saúde Coletiva 2010, 15, 3249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laranjo, E.; Baptista, S.; Norton, A.A.; Macedo, A.P.; Andrade, C.; Areias, C. A cárie precoce da infância: Uma atualização. Rev. Port. Med. Geral E Fam. 2017, 33, 426. [Google Scholar] [CrossRef]
- Sala, E.C.; García, P.B. Odontología Preventiva y Comunitaria, Princípios Métodos y Aplicaciones, 4th ed.; Elsevier Espana, S.L., Ed.; Elsevier Masson: Barcelona, España, 2013. [Google Scholar]








| Study | Study Group (SD) | Control Group | Country | Continent | Latitude | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Dimension | Indices | Prev. Cavitation | Age (years) | Ratio M/F (%) | Sample Dimension | Indices | Prev. de Cavitation | Age (years) | Ratio M/F (%) | ||||||||||
| F | M | T | DMFT | dmft | F | M | T | DMFT | dmft | ||||||||||
| [22] | 15 | 38 | 53 | N/A | 1.84 | 30 | 11.09 | 253.3 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Jordan | Asia | 31.963 |
| [23] | 26 | 44 | 70 | N/A | N/A | 39 | 4.41 | 169.2 | 9 | 23 | 32 | N/A | N/A | 25 | 9.22 | 139.1 | Israel | Asia | 31.769 |
| [24] | 23 | 22 | 45 | N/A | N/A | 10 | 13 | 95.7 | 18 | 27 | 45 | N/A | N/A | 19 | 13 | 150 | Portugal | Europe | 41.150 |
| [25] | 36 | 60 | 96 | 2.45 | 4.44 | 90 | 10.15 | 166.7 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Yemeni | Asia | 15.369 |
| [26] | N/A | N/A | 45 | 0.71 | 0.31 | 10 | 12.7 | N/A | N/A | N/A | 45 | 1.42 | 0.42 | 19 | 12.8 | N/A | Portugal | Europe | 41.150 |
| [20] | 14 | 16 | 30 | 0.90 | 1 | 21 | N/A | 114.3 | 14 | 16 | 30 | 2.47 | 2.33 | 25 | N/A | 114.3 | India | Asia | 24.571 |
| [27] | N/A | N/A | 146 | N/A | N/A | 60 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Colombia | South America | −10.300 |
| [28] | 26 | 35 | 61 | N/A | N/A | 26 | 9 | 134.6 | 38 | 45 | 83 | N/A | N/A | 39 | 9.43 | 118.4 | Brasil | South America | −30.028 |
| [21] | 13 | 17 | 30 | N/A | N/A | 10 | 6.37 | 30.8 | 16 | 14 | 30 | N/A | N/A | 29 | 7.53 | 87.5 | Brasil | South America | −21.764 |
| [29] | 36 | 25 | 61 | 0.36 | 1.84 | 23 | 9.15 | 69.4 | 32 | 20 | 52 | 0.49 | 0.98 | 34 | 9.80 | 62.5 | Brasil | South America | −30.028 |
| [30] | N/A | N/A | 52 | 1.40 | 1 | 32 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Saudi Arabia | Asia | 21.427 |
| [31] | 43 | 76 | 119 | N/A | N/A | 81 | 14.19 | 176.7 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Pakistan | Asia | 24.926 |
| [32] | 67 | 77 | 144 | N/A | N/A | 52 | N/A | 114.9 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Brasil | South America | −21.764 |
| [33] | 43 | 63 | 106 | 2.73 | N/A | 57 | 9.3 | 146.5 | 70 | 55 | 125 | 1.65 | N/A | 72 | 11.7 | 78.8 | United Arab Emitades | Asia | 25.277 |
| [34] | N/A | N/A | 35 | 1.54 | 0.60 | 24 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | India | Asia | 28.645 |
| [35] | N/A | N/A | 9 | N/A | N/A | 4 | 9.11 | N/A | N/A | N/A | 8 | N/A | N/A | 3 | 9.75 | N/A | Brasil | South America | −30.028 |
| [36] | N/A | N/A | 49 | N/A | N/A | 15 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | South Africa | Africa | −26.95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, M.; Mascarenhas, P.; Evangelista, J.G.; Barahona, I.; Tavares, V. The Incidence of Dental Caries in Children with Down Syndrome: A Systematic Review and Meta-Analysis. Dent. J. 2022, 10, 205. https://doi.org/10.3390/dj10110205
Martins M, Mascarenhas P, Evangelista JG, Barahona I, Tavares V. The Incidence of Dental Caries in Children with Down Syndrome: A Systematic Review and Meta-Analysis. Dentistry Journal. 2022; 10(11):205. https://doi.org/10.3390/dj10110205
Chicago/Turabian StyleMartins, Mariana, Paulo Mascarenhas, José Grillo Evangelista, Isabel Barahona, and Vitor Tavares. 2022. "The Incidence of Dental Caries in Children with Down Syndrome: A Systematic Review and Meta-Analysis" Dentistry Journal 10, no. 11: 205. https://doi.org/10.3390/dj10110205