
Initial Displacement and Stress Distribution of Upper Central Incisor Extrusion with Clear Aligners and Various Shapes of Composite Attachments Using the Finite Element Method


Abstract
:1. Introduction
2. Materials and Methods
- Model 1: no composite attachment
- Model 2: rectangular beveled attachment
- Model 3: ellipsoid attachment
- Model 4: horizontal rectangular attachment
3. Results
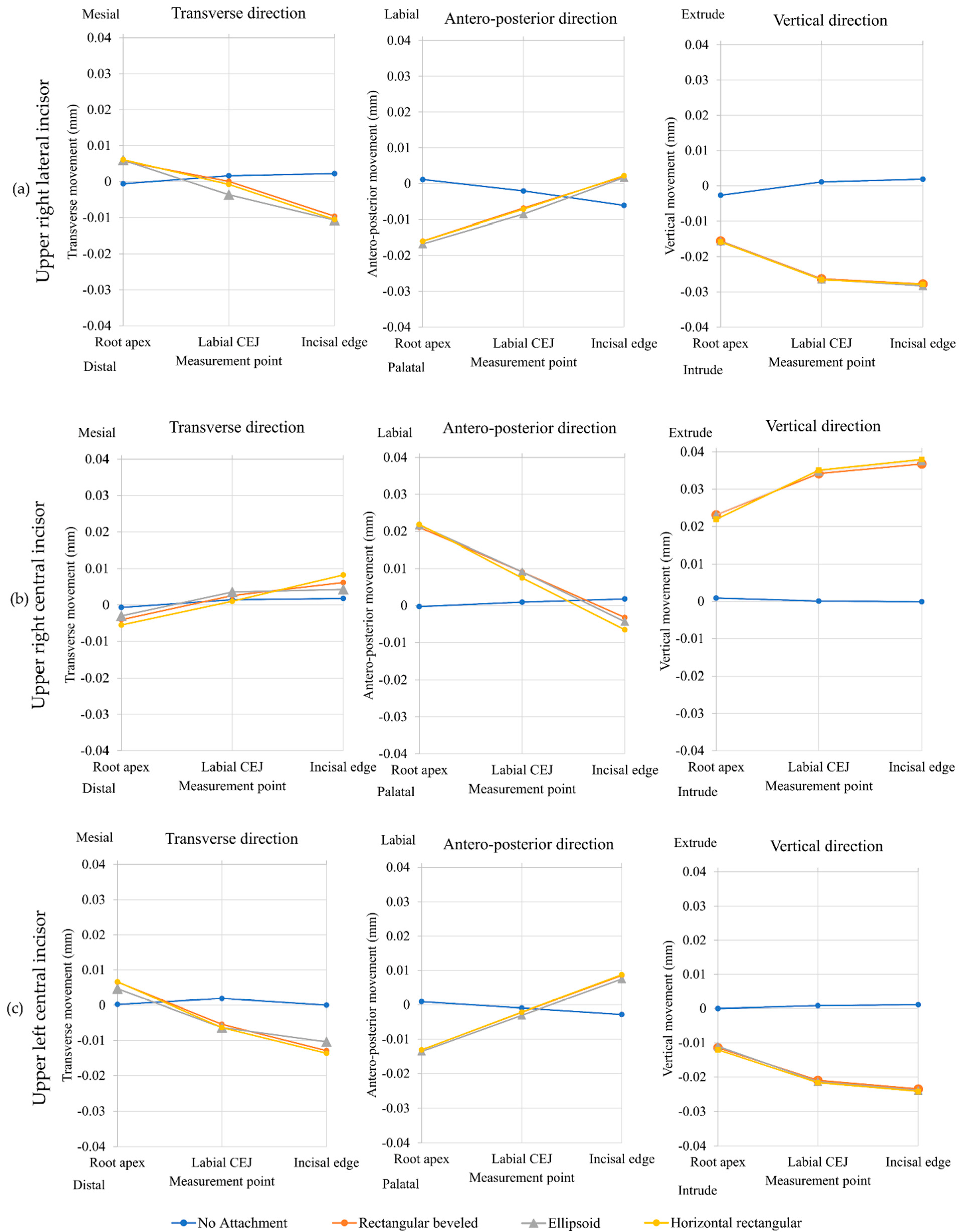
3.1. Initial Displacement
3.1.1. Upper Right Central Incisor
3.1.2. Upper Right Lateral Incisor and Upper Left Central Incisor
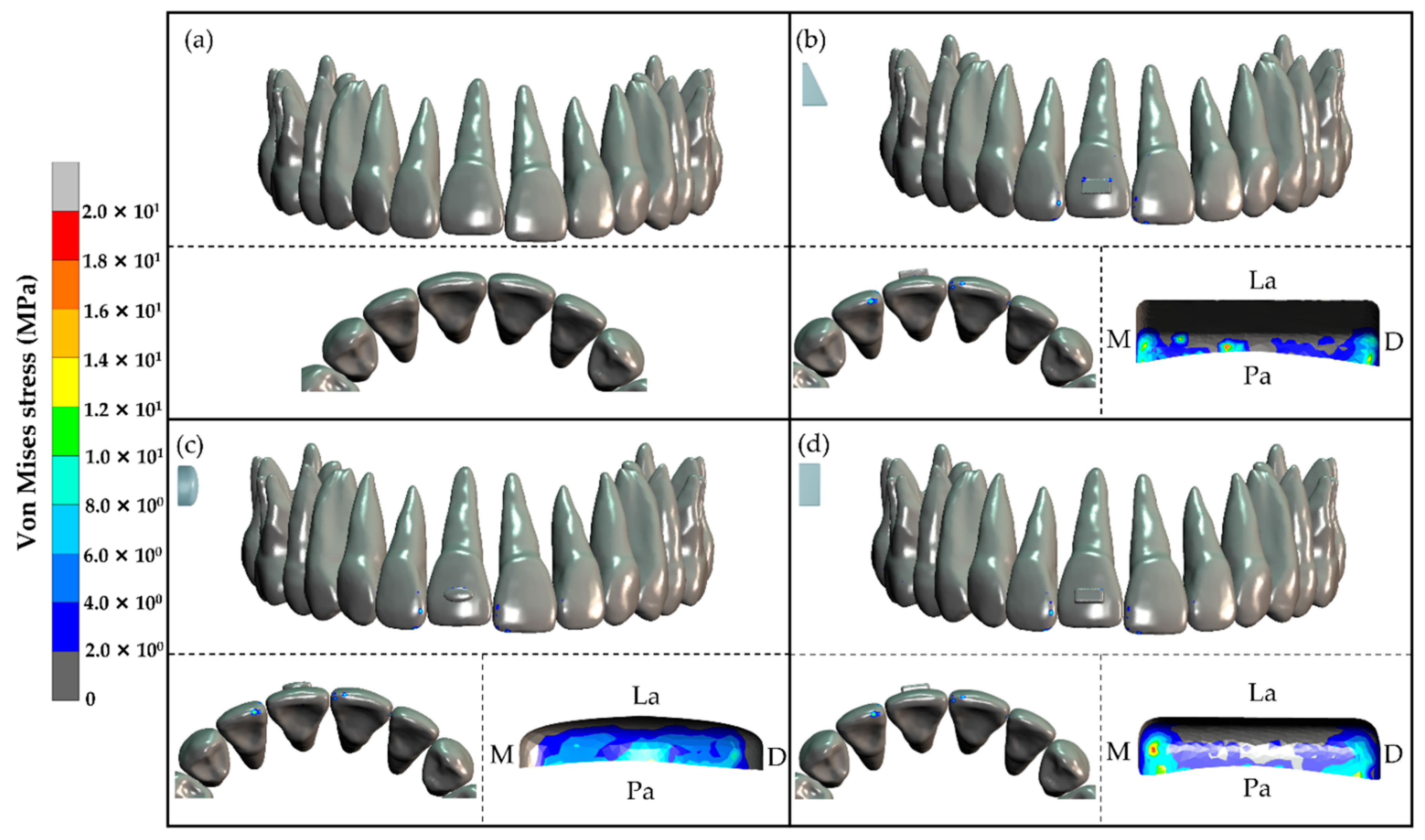
3.2. Stress Distribution
3.2.1. Stress Distribution in Tooth and Composite Attachment
3.2.2. Stress Distribution in the PDL
4. Discussion
5. Conclusions
- The three composite attachment shapes including horizontal rectangular attachment, ellipsoid attachment, and rectangular beveled attachment can be used to perform upper central incisor extrusion.
- Upper central incisor extrusion was caused by a force from the clear aligner applied at the cervical portion of the composite attachment.
- In the three models each with a composite attachment, the stress distribution in the PDL was found to have the same pattern. Maximum tensile stress was found around the apical area of the upper right central incisor. Maximum compressive stresses were observed around the apical area of the upper right lateral incisor and left central incisor since these teeth served as the anchorage for the upper right central incisor extrusion.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Melsen, B. Northcroft lecture: How has the spectrum of orthodontics changed over the past decades? J. Orthod. 2011, 38, 134–143. [Google Scholar] [CrossRef]
- Rosvall, M.D.; Fields, H.W.; Ziuchkovski, J.; Rosenstiel, S.F.; Johnston, W.M. Attractiveness, acceptability, and value of orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 276-e1. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Kusnoto, B.; Begole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef]
- Krieger, E.; Seiferth, J.; Marinello, I.; Jung, B.A.; Wriedt, S.; Jacobs, C.; Wehrbein, H. Invisalign(R) treatment in the anterior region: Were the predicted tooth movements achieved? J. Orofac. Orthop. 2012, 73, 365–376. [Google Scholar] [CrossRef]
- Djeu, G.; Shelton, C.; Maganzini, A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 292–298. [Google Scholar] [CrossRef]
- Kassas, W.; Al-Jewair, T.; Preston, C.B.; Tabbaa, S. Assessment of Invisalign treatment outcomes using the ABO Model Grading System. J. World Fed. Orthod. 2013, 2, e61–e64. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Beers, A.C.; Choi, W.; Pavlovskaia, E. Computer-assisted treatment planning and analysis. Orthod. Craniofacial Res. 2003, 6 (Suppl. 1), 117–125. [Google Scholar] [CrossRef]
- Dasy, H.; Dasy, A.; Asatrian, G.; Rozsa, N.; Lee, H.F.; Kwak, J.H. Effects of variable attachment shapes and aligner material on aligner retention. Angle Orthod. 2015, 85, 934–940. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; He, B.; Yang, X.; Yao, J. Optimization of configuration of attachment in tooth translation with transparent tooth correction by appropriate moment-to-force ratios: Biomechanical analysis. Biomed. Mater. Eng. 2015, 26 (Suppl. 1), S507–S517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savignano, R.; Valentino, R.; Razionale, A.V.; Michelotti, A.; Barone, S.; D’anto, V. Biomechanical Effects of Different Auxiliary-Aligner Designs for the Extrusion of an Upper Central Incisor: A Finite Element Analysis. J. Healthc. Eng. 2019, 2019, 9687127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, R.; Calheiros, F.C.; Ballester, R.Y.; Gonçalves, F. Effect of three different attachment designs in the extrusive forces generated by thermoplastic aligners in the maxillary central incisor. Dent. Press J. Orthod. 2020, 25, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, P.M.; Dalstra, M.; Melsen, B. The finite element method: A tool to study orthodontic tooth movement. J. Dent. Res. 2005, 84, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Konda, P.; Sa, T. Basic principles of finite element method and its applications in orthodontics. J. Pharm. Biomed. Sci. 2012, 16, 1–8. [Google Scholar]
- Yokoi, Y.; Arai, A.; Kawamura, J.; Uozumi, T.; Usui, Y.; Okafuji, N. Effects of Attachment of Plastic Aligner in Closing of Diastema of Maxillary Dentition by Finite Element Method. J. Healthc. Eng. 2019, 2019, 1075097. [Google Scholar] [CrossRef]
- Gomez, J.P.; Pena, F.M.; Martinez, V.; Giraldo, D.C.; Cardona, C.I. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis. Angle Orthod. 2015, 85, 454–460. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-Y.; Su, M.-Z.; Chang, H.-H.; Chiang, Y.-C.; Tao, S.-H.; Cheng, J.-H.; Fuh, L.-J.; Lin, C.-P. Tension-compression viscoelastic behaviors of the periodontal ligament. J. Formos. Med. Assoc. 2012, 111, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Cortona, A.; Rossini, G.; Parrini, S.; Deregibus, A.; Castroflorio, T. Clear aligner orthodontic therapy of rotated mandibular round-shaped teeth: A finite element study. Angle Orthod. 2020, 90, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Rong, Q.; Lin, J.; Xu, B. Torque control of the maxillary incisors in lingual and labial orthodontics: A 3-dimensional finite element analysis. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 316–322. [Google Scholar] [CrossRef]
- Ramalho, A.; Antunes, P.V. Reciprocating wear test of dental composites against human teeth and glass. Wear 2007, 263, 1095–1104. [Google Scholar] [CrossRef] [Green Version]
- Likitmongkolsakul, U.; Smithmaitrie, P.; Samruajbenjakun, B.; Aksornmuang, J. Development and Validation of 3D Finite Element Models for Prediction of Orthodontic Tooth Movement. Int. J. Dent. 2018, 2018, 4927503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hohmann, A.; Wolfram, U.; Geiger, M.; Boryor, A.; Sander, C.; Faltin, R.; Faltin, K.; Sander, F.G. Periodontal Ligament Hydrostatic Pressure with Areas of Root Resorption after Application of a Continuous Torque Moment: A Study Using Identical Extracted Maxillary Human Premolars. Angle Orthod. 2007, 77, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.M. Tissue changes incidental to orthodontic tooth movement. Int. J. Orthod. Oral Surg. Radiogr. 1932, 18, 331–352. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | Young’s Modulus (MPa) | Poisson’s Ratio | Mesh Size (mm) |
|---|---|---|---|
| Maxilla | 1.37 × 103 | 0.30 | 0.2–0.5 |
| PDL | 6.67 × 10−1 | 0.45 | 0.1 |
| Teeth | 1.96 × 104 | 0.30 | 0.2 |
| Composite attachment | 1.25 × 104 | 0.36 | 0.2 |
| Clear aligner | 528 | 0.36 | 0.2 |
| Models | Location | Displacement (×10−2 mm) | ||
|---|---|---|---|---|
| Transverse (x) | Antero-Posterior (y) | Vertical (z) | ||
| No composite attachment | Root apex | −0.0680 | −0.0265 | 0.0886 |
| Labial CEJ | 0.1450 | 0.0944 | 0.0078 | |
| Incisal edge | 0.1789 | 0.1796 | −0.0105 | |
| Rectangular beveled attachment | Root apex | −0.4063 | 2.1039 | 2.3086 |
| Labial CEJ | 0.2583 | 0.9132 | 3.4200 | |
| Incisal edge | 0.6166 | −0.3218 | 3.6786 | |
| Ellipsoid attachment | Root apex | −0.3020 | 2.1653 | 2.3101 |
| Labial CEJ | 0.0356 | 0.9139 | 3.4731 | |
| Incisal edge | 0.4274 | −0.4352 | 3.7606 | |
| Horizontal rectangular attachment | Root apex | −0.5532 | 2.1848 | 2.1896 |
| Labial CEJ | 0.5533 | 0.7496 | 3.5094 | |
| Incisal edge | 0.8252 | −0.6546 | 3.7991 | |
| Models | Teeth | Maximum Average Normal Stress at PDL around Root Apex (MPa) |
|---|---|---|
| No composite attachment | URLI | <0.001 |
| URCI | <0.001 | |
| ULCI | <0.001 | |
| Rectangular beveled attachment | URLI | −0.076 |
| URCI | 0.125 | |
| ULCI | −0.073 | |
| Ellipsoid attachment | URLI | −0.090 |
| URCI | 0.128 | |
| ULCI | −0.073 | |
| Horizontal rectangular attachment | URLI | −0.090 |
| URCI | 0.130 | |
| ULCI | −0.081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laohachaiaroon, P.; Samruajbenjakun, B.; Chaichanasiri, E. Initial Displacement and Stress Distribution of Upper Central Incisor Extrusion with Clear Aligners and Various Shapes of Composite Attachments Using the Finite Element Method. Dent. J. 2022, 10, 114. https://doi.org/10.3390/dj10060114
Laohachaiaroon P, Samruajbenjakun B, Chaichanasiri E. Initial Displacement and Stress Distribution of Upper Central Incisor Extrusion with Clear Aligners and Various Shapes of Composite Attachments Using the Finite Element Method. Dentistry Journal. 2022; 10(6):114. https://doi.org/10.3390/dj10060114
Chicago/Turabian StyleLaohachaiaroon, Pratchawin, Bancha Samruajbenjakun, and Ekachai Chaichanasiri. 2022. "Initial Displacement and Stress Distribution of Upper Central Incisor Extrusion with Clear Aligners and Various Shapes of Composite Attachments Using the Finite Element Method" Dentistry Journal 10, no. 6: 114. https://doi.org/10.3390/dj10060114