
Comparison of the Accuracy of a Mounting Fixture for Dental Implants for Implant Position Transfer and Open-Tray Implant Level Impression—An In Vitro Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Master Model Construction
2.2. Impression Tray Design
2.3. Impression Protocol
2.4. Stone Cast Production Protocol
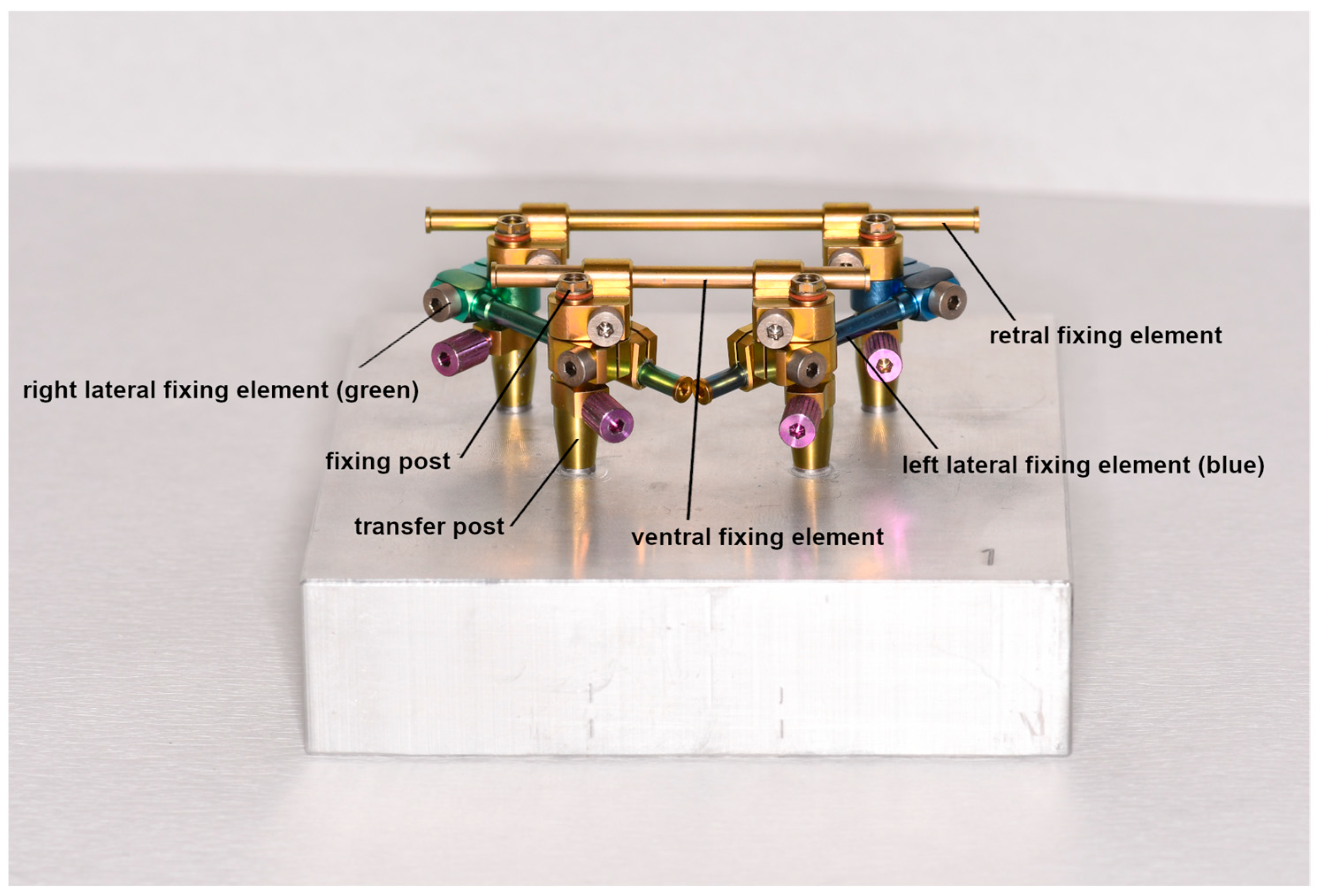
2.5. Protocol Using the nt-VAL-Jig
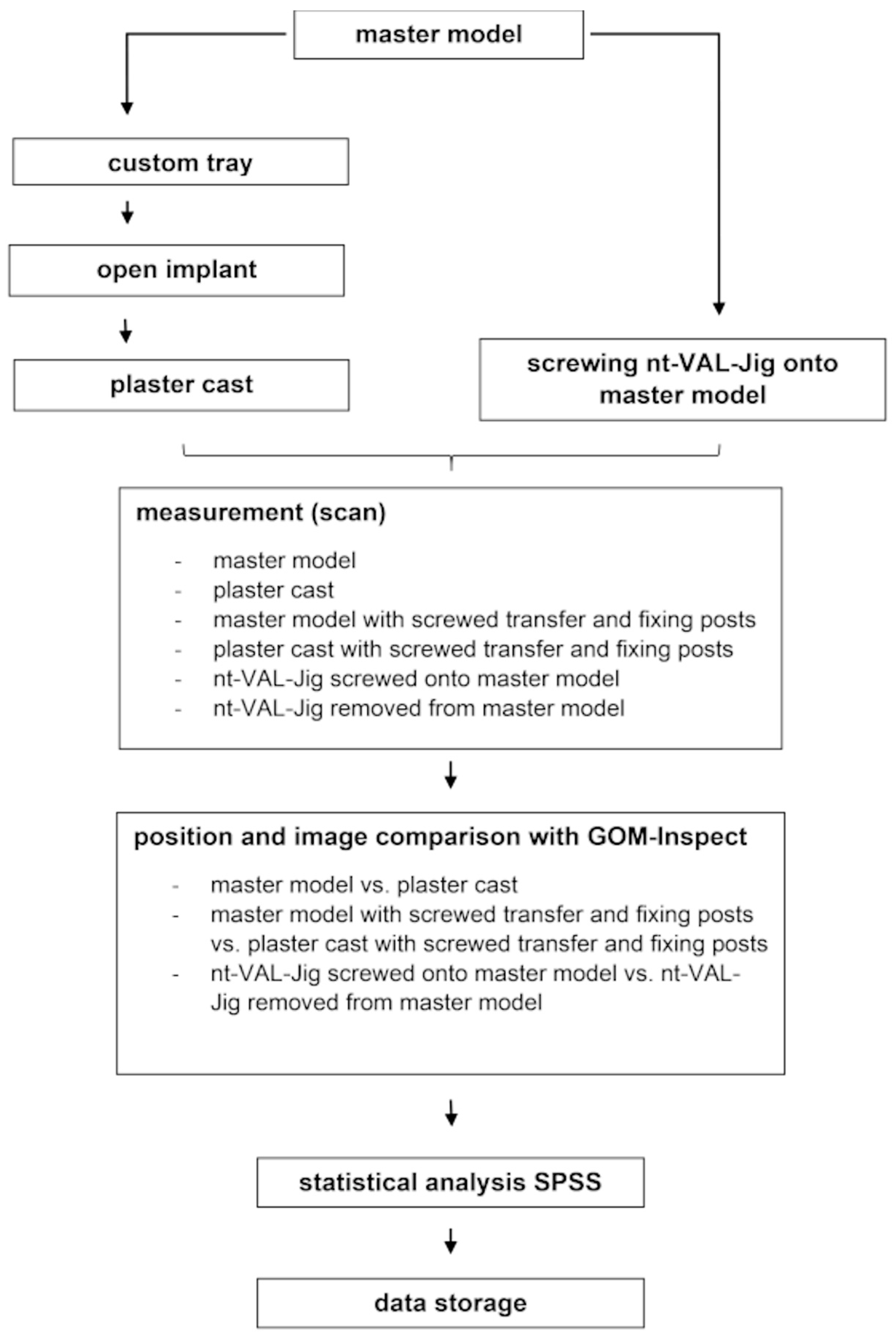
2.6. Measurement Protocol
2.7. Comparison of Implant Position
2.8. Evaluation of Measurements
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manea, A.; Baciut, G.; Baciut, M.; Pop, D.; Comsa, D.S.; Buiga, O.; Trombitas, V.; Colosi, H.; Mitre, I.; Bordea, R.; et al. New Dental Implant with 3D Shock Absorbers and Tooth-Like Mobility-Prototype Development, Finite Element Analysis (FEA), and Mechanical Testing. Materials 2019, 12, 3444. [Google Scholar] [CrossRef]
- Boldt, J.; Knapp, W.; Proff, P.; Rottner, K.; Richter, E.-J. Measurement of tooth and implant mobility under physiological loading conditions. Ann. Anat. 2012, 194, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Liaw, K.; Delfini, R.H.; Abrahams, J.J. Dental Implant Complications. Semin. Ultrasound CT MR 2015, 36, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Berglundh, T.; Ericsson, I.; Liljenberg, B.; Marinello, C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin. Oral Implants Res. 1992, 3, 9–16. [Google Scholar] [CrossRef]
- Stoichkov, B.; Kirov, D. Analysis of the causes of dental implant fracture: A retrospective clinical study. Quintessence Int. 2018, 49, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, A.; Renvert, S.; Dahlen, G. Microbial findings at failing implants. Clin. Oral Implants Res. 1999, 10, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; So, J.S.; Hochstedler, J.L.; Ercoli, C. The accuracy of implant impressions: A systematic review. J. Prosthet. Dent. 2008, 100, 285–291. [Google Scholar] [CrossRef]
- Khan, S.A.; Singh, S.; Neyaz, N.; Jaiswal, M.M.; Tanwar, A.S.; Singh, A. Comparison of Dimensional Accuracy of Three Different Impression Materials Using Three Different Techniques for Implant Impressions: An In Vitro Study. J. Contemp. Dent. Pract. 2021, 22, 172–178. [Google Scholar] [CrossRef]
- Moreira, A.H.J.; Rodrigues, N.F.; Pinho, A.C.M.; Fonseca, J.C.; Vilaça, J.L. Accuracy comparison of implant impression techniques: A systematic review. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. S2), e751–e764. [Google Scholar] [CrossRef]
- Moura, R.V.; Kojima, A.N.; Saraceni, C.H.C.; Bassolli, L.; Balducci, I.; Özcan, M.; Mesquita, A.M.M. Evaluation of the accuracy of conventional and digital impression techniques for implant restorations. J. Prosthodont. 2018, 28, e530–e535. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.-J.; Gallucci, G.O.; Doukoudakis, A.; Weber, H.-P.; Chronopoulos, V. Accuracy of implant impressions for partially and completely edentulous patients: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 836–845. [Google Scholar] [CrossRef]
- Parameshwari, G.; Chittaranjan, B.; Sudhir, N.; Anulekha-Avinash, C.-K.; Taruna, M.; Ramureddy, M. Evaluation of accuracy of various impression techniques and impression materials in recording multiple implants placed unilaterally in a partially edentulous mandible—An in vitro study. J. Clin. Exp. Dent. 2018, 10, e388–e395. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Prasad, K.; Vakil, H.; Jain, A.; Chowdhary, R. Accuracy of impressions with different impression materials in angulated implants. Niger. J. Clin. Pract. 2013, 16, 279–284. [Google Scholar] [CrossRef]
- Shim, J.S.; Ryu, J.J.; Shin, S.W.; Lee, J.Y. Effects of implant angulation and impression coping type on the dimensional accuracy of impressions. Implant Dent. 2015, 24, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Balouch, F.; Jalalian, E.; Nikkheslat, M.; Ghavamian, R.; Toopchi, S.; Jallalian, F.; Jalalian, S. Comparison of dimensional accuracy between open-tray and closed-tray implant impression technique in 15° angled implants. J. Dent. 2013, 14, 96–102. [Google Scholar]
- Rajendran, R.; Chander, N.G.; Anitha, K.V.; Muthukumar, B. Dimensional accuracy of vinyl polyether and polyvinyl siloxane impression materials in direct implant impression technique for multiple dental implants. Eur. Oral Res. 2021, 55, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.R. Multi-unit implant impression accuracy: A review of the literature. Quintessence Int. 2014, 45, 39–51. [Google Scholar] [CrossRef]
- Lee, S.-E.; Yang, S.-E.; Lee, C.-W.; Lee, W.-S.; Lee, S.Y. Accuracy of new implant impression technique using dual arch tray and bite impression coping. J. Adv. Prosthodont. 2018, 10, 265–270. [Google Scholar] [CrossRef]
- Siadat, H.; Saeidi, Z.; Alikhasi, M.; Zeighami, S. Comparative evaluation of the effect of impression materials and trays on the accuracy of angulated implants impressions. J. Clin. Exp. Dent. 2018, 10, e1096–e1102. [Google Scholar] [CrossRef]
- Chaffee, N.R.; Bailey, J.H.; Sherrard, D.J. Dimensional accuracy of improved dental stone and epoxy resin die materials. Part II: Complete arch form. J. Prosthet. Dent. 1997, 77, 235–238. [Google Scholar] [CrossRef]
- Jørgensen, K.D. Study of the setting expansion of gypsum. Acta Odontol. Scand. 1963, 21, 227–254. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-Dimensional Accuracy of Digital Impression versus Conventional Method: Effect of Implant Angulation and Connection Type. Int. J. Dent. 2018, 2018, 3761750. [Google Scholar] [CrossRef] [PubMed]
- Basaki, K.; Alkumru, H.; de Souza, G.; Finer, Y. Accuracy of Digital vs. Conventional Implant Impression Approach: A Three-Dimensional Comparative In Vitro Analysis. Int. J. Oral Maxillofac. Implants 2017, 32, 792–799. [Google Scholar] [CrossRef]
- Pesce, P.; Pera, F.; Setti, P.; Menini, M. Precision and accuracy of a digital impression scanner in full-arch implant rehabilitation. Int. J. Prosthodont. 2018, 31, 171–175. [Google Scholar] [CrossRef]
- Elshenawy, E.A.; Alam-Eldein, A.M.; Abd Elfatah, F.A. Cast accuracy obtained from different impression techniques at different implant angulations (in vitro study). Int. J. Implant Dent. 2018, 4, 9. [Google Scholar] [CrossRef]
- Osman, M.S.; Ziada, H.M.; Abubakr, N.H.; Suliman, A.M. Implant impression accuracy of parallel and non-parallel implants: A comparative in-vitro analysis of open and closed tray techniques. Int. J. Implant Dent. 2019, 5, 4. [Google Scholar] [CrossRef]
- Tsagkalidis, G.; Tortopidis, D.; Mpikos, P.; Kaisarlis, G.; Koidis, P. Accuracy of 3 different impression techniques for internal connection angulated implants. J. Prosthet. Dent. 2015, 114, 517–523. [Google Scholar] [CrossRef]
- Martínez-Rus, F.; García, C.; Santamaría, A.; Özcan, M.; Pradíes, G. Accuracy of definitive casts using 4 implant-level impression techniques in a scenario of multi-implant system with different implant angulations and subgingival alignment levels. Implant Dent. 2013, 22, 268–276. [Google Scholar] [CrossRef]
- Conrad, H.J.; Pesun, I.J.; DeLong, R.; Hodges, J.S. Accuracy of two impression techniques with angulated implants. J. Prosthet. Dent. 2007, 97, 349–356. [Google Scholar] [CrossRef]
- Assunção, W.G.; Britto, R.C.; Ricardo Barão, V.A.; Delben, J.A.; dos Santos, P.H. Evaluation of impression accuracy for implant at various angulations. Implant Dent. 2010, 19, 167–174. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| I1 | I2 | I3 | I4 | |||||
|---|---|---|---|---|---|---|---|---|
| Cast | Angle * | Tilt ** | Angle * | Tilt ** | Angle * | Tilt ** | Angle * | Tilt ** |
| 1 | 90° | 0° | 90° | 0° | 90° | 0° | 90° | 0° |
| 2 | 100° | 10° to o | 90° | 0° | 90° | 0° | 100° | 10° to o |
| 3 | 80° | 10° to v | 90° | 0° | 90° | 0° | 80° | 10° to v |
| 4 | 80° | 10° to d | 90° | 0° | 90° | 0° | 80° | 10° to d |
| 5 | 100° | 10° to m | 90° | 0° | 90° | 0° | 100° | 10° to m |
| 6 | 90° | 0° | 100° | 10° to o | 100° | 10° to o | 90° | 0° |
| 7 | 90° | 0° | 80° | 10° to v | 80° | 10° to v | 90° | 0° |
| 8 | 90° | 0° | 80° | 10° to d | 80° | 10° to d | 90° | 0° |
| 9 | 90° | 0° | 60° | 30° to d | 60° | 30° to d | 90° | 0° |
| 10 | 115° | 25° to o | 90° | 0° | 90° | 0° | 115° | 25° to o |
| aluminum master model | aluminum master model with screwed transfer and fixing posts | nt-VAL-Jig screwed on master model | |
| stone model | comparison group 1 (open-tray implant level impression) | --- | --- |
| stone model with screwed transfer and fixing posts | --- | comparison group 2 (open-tray implant level impression with screwed transfer and fixing posts) | --- |
| nt-VAL-Jig removed from master model | --- | --- | comparison group 3 (nt-VAL-Jig) |
| open implant impression | open implant impression with screwed fixing and transfer posts | nt-VAL-Jig | |
| open implant impression | --- | 0.005 * | 0.959 |
| open implant impression with screwed fixing and transfer posts | 0.005 * | --- | 0.009 * |
| nt-VAL-Jig | 0.959 | 0.009 * | --- |
| Comparison Group | Cast | Implant Analog | Direction | Local Difference (mm) |
|---|---|---|---|---|
| 1 | --- | --- | --- | No local differences |
| 2 | 2 | I1 | Distal | 1.00 |
| 5 | I4 | Distal | 1.00 | |
| 7 | I1 + I3 | Distal | 0.60 | |
| 8 | I1 + I3 | Distal | 0.60 | |
| 9 | I1 | Distal | 0.60 | |
| 10 | I4 | Distal | 1.00 | |
| 3 | 2 | I1 | Distal | 0.73 |
| 6 | I1 + I3 | Distal | ≥0.46 | |
| 9 | I1 + I2 | Distal | ≥0.73 |
| open implant impression | open implant impression with screwed fixing and transfer posts | nt-VAL-Jig | |
| open implant impression | --- | 0.018 * | 0.005 * |
| open implant impression with screwed fixing and transfer posts | 0.018 * | --- | 0.210 |
| nt-VAL-Jig | 0.005 * | 0.210 | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, A.; Dirksen, D.; Runte, C. Comparison of the Accuracy of a Mounting Fixture for Dental Implants for Implant Position Transfer and Open-Tray Implant Level Impression—An In Vitro Study. Dent. J. 2023, 11, 208. https://doi.org/10.3390/dj11090208
Becker A, Dirksen D, Runte C. Comparison of the Accuracy of a Mounting Fixture for Dental Implants for Implant Position Transfer and Open-Tray Implant Level Impression—An In Vitro Study. Dentistry Journal. 2023; 11(9):208. https://doi.org/10.3390/dj11090208
Chicago/Turabian StyleBecker, Alexander, Dieter Dirksen, and Christoph Runte. 2023. "Comparison of the Accuracy of a Mounting Fixture for Dental Implants for Implant Position Transfer and Open-Tray Implant Level Impression—An In Vitro Study" Dentistry Journal 11, no. 9: 208. https://doi.org/10.3390/dj11090208