
Design and Initial Evaluation of a Novel Oral Hygiene Technology for a Special Needs Population: A New Way to Clean

Abstract
:
1. Introduction
2. Methods
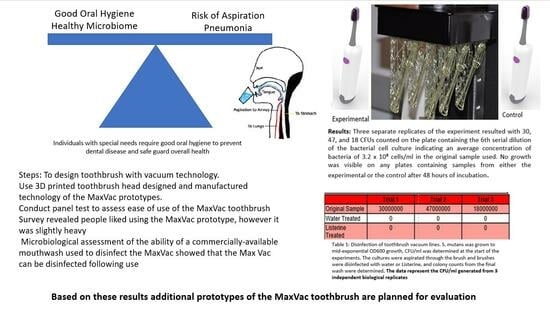
Prototype Design Manufacturing
3. Methods and Materials
3.1. Sensory Testing
3.2. Microbiological Evaluation Methods
4. Results
4.1. Microbiological Study
4.2. Results for the Sensory Testing and Prototype Comparison of Version 2.0 with 3.0
4.3. Conclusions for Both Sensory Testing and Microbiological Testing
5. Discussion
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olsen, I.; Hicks, S.D. Oral microbiota and autism spectrum disorder (ASD). J. Oral Microbiol. 2020, 12, 1702806. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Wu, M.; Feng, Y.; Zhou, Z.; Chen, L.; Chen, F. Alterations of oral microbiota distinguish children with autism spectrum disorders from healthy controls. Sci. Rep. 2018, 8, 1597. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Evidence-Based Update on Diagnosis and Management of Gingivitis and Periodontitis. Dent. Clin. N. Am. 2019, 63, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Uriarte, S.M.; Edmisson, J.S.; Jimenez-Flores, E. Human neutrophils and oral microbiota: A constant tug-of-war between a harmonious and a discordant coexistence. Immunol. Rev. 2016, 273, 282–298. [Google Scholar] [CrossRef] [PubMed]
- Loos, B.G.; Van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontology 2000 2020, 83, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Naka, S.; Yamana, A.; Nakano, K.; Okawa, R.; Fujita, K.; Kojima, A.; Ooshima, T. Distribution of periodontopathic bacterial species in Japanese children with developmental disabilities. BMC Oral Health 2009, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- El-Solh, A.A. Association between pneumonia and oral care in nursing home residents. Lung 2011, 189, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, P.; Wardh, I.; Zimmerman, M.; Almstahl, A.; Wikstrom, M. Oral Care and Mortality in Older Adults with Pneumonia in Hospitals or Nursing Homes: Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2016, 64, 2109–2115. [Google Scholar] [CrossRef] [PubMed]
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.M. Powered versus manual toothbrushing for oral health. Cochrane Database Syst. Rev. 2014, 2014, CD002281. [Google Scholar] [CrossRef] [PubMed]
- Strickland, M.; Scoopo, F.; Migliore, L.; Mahevich, R.; Janal, M. Effect of the power toothbrush on the disabled. J. Dent. Res. 2005, 84, Abst 83. [Google Scholar]
- Van Leeuwen, M.P.C.; Van der Weijden, F.A.; Slot, D.E.; Rosema, M.A.M. Toothbrush wear in relation to toothbrushing effectiveness. Int. J. Dent. Hyg. 2019, 17, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. How much saliva is enough for avoidance of xerostomia? Caries Res. 2004, 38, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. The prevalence of dysphagia among adults in the United States. Otolaryngol. Head Neck Surg. 2014, 151, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.P.; Chen, Y.W.; Wang, M.J.; Pinelis, E. National Trends in Admission for Aspiration Pneumonia in the United States, 2002–2012. Ann. Am. Thorac. Soc. 2017, 14, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Caffrey, C.; Sengupta, M.; Moss, A.; Harris-Kojetin, L.; Valverde, R. Home health care and discharged hospice care patients: United States, 2000 and 2007. In National Health Statistics Reports; U.S. Department of Health and Human Services: Washington, DC, USA, 2011; pp. 1–27. [Google Scholar]
- Okuda, K.; Adachi, M.; Iijima, K. The efficacy of antimicrobial mouth rinses in oral health care. Bull. Tokyo Dent. Coll. 1998, 39, 7–14. [Google Scholar] [PubMed]
- Leder, S.B. Serial fiberoptic endoscopic swallowing evaluations in the management of patients with dysphagia. Arch. Phys. Med. Rehabil. 1998, 79, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- de Lima Alvarenga, E.H.; Dall’Oglio, G.P.; Murano, E.Z.; Abrahao, M. Continuum theory: Presbyphagia to dysphagia? Functional assessment of swallowing in the elderly. Eur. Arch. Oto-Rhino-Laryngol. 2017, 275, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.; Yamazaki, K. Can oral bacteria affect the microbiome of the gut? J. Oral Microbiol. 2019, 11, 1586422. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Beydoun, H.A.; Hossain, S.; El-Hajj, Z.W.; Weiss, J.; Zonderman, A.B. Clinical and Bacterial Markers of Periodontitis and Their Association with Incident All-Cause and Alzheimer’s Disease Dementia in a Large National Survey. J. Alzheimer’s Dis. 2020, 75, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Sadrameli, M.; Bathini, P.; Alberi, L. Linking mechanisms of periodontitis to Alzheimer’s disease. Curr. Opin. Neurol. 2020, 33, 230–238. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| CFU/mL | Trial 1 | Trial 2 | Trial 3 |
|---|---|---|---|
| Starting culture | 3.00 × 107 | 4.70 × 107 | 1.82 × 107 |
| Water treatment | 0 | 0 | 0 |
| Listerine treatment | 0 | 0 | 0 |
| Toothbrush Version | N | Mean | Std. Deviation | Median | Mean Rank | p-Value |
|---|---|---|---|---|---|---|
| 2.0 | 10 | 0.70 mL | 036 | 0.70 | 9.4 | p = 0.436 |
| 3.0 | 10 | 0.80 mL | 0.19 | 0.80 | 11.6 |
| Survey Question | Version 2.0 | Version 3.0 | ||||
|---|---|---|---|---|---|---|
| Total | n | % | n | % | ||
| Q 1. What Toothbrush currently | 1-manual | 8 | 4 | 40.0 | 4 | 40.0 |
| 2-electric | 9 | 4 | 40.0 | 5 | 50.0 | |
| 3-both | 3 | 2 | 20.0 | 1 | 10.0 | |
| Q 2. How does the new technology compare | Worse | 2 | 0 | 0.0 | 2 | 20.0 |
| slightly worse | 3 | 1 | 10.0 | 2 | 20.0 | |
| same | 6 | 2 | 20.0 | 4 | 40.0 | |
| Slightly better | 4 | 3 | 30.0 | 1 | 10.0 | |
| better | 5 | 4 | 40.0 | 1 | 10.0 | |
| Q 3. How long do you brush | 30 s | 0 | 0 | 0.0 | 0 | 0.0 |
| 1.5 m | 12 | 6 | 60.0 | 6 | 60.0 | |
| 2 m | 8 | 4 | 40.0 | 4 | 40.0 | |
| Q 4. Ease of use | Too light | 0 | 0 | 0.0 | 0 | 0.0 |
| light | 4 | 1 | 10.0 | 3 | 30.0 | |
| moderate | 7 | 3 | 30.0 | 4 | 40.0 | |
| Heavy | 8 | 6 | 60.0 | 2 | 20.0 | |
| too heavy | 1 | 0 | 0.0 | 1 | 10.0 | |
| Q 5. Would you recommend | Most likely not | 1 | 1 | 10.0 | 0 | 0.0 |
| likely not | 1 | 0 | 0.0 | 1 | 10.0 | |
| indifferent | 0 | 0 | 0.0 | 0 | 0.0 | |
| Likely yes | 10 | 4 | 40.0 | 6 | 60.0 | |
| most likely yes | 8 | 5 | 50.0 | 3 | 30.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strickland, M.; Mills, S.; Dasari, B.; Markowitz, K.; Cugini, C. Design and Initial Evaluation of a Novel Oral Hygiene Technology for a Special Needs Population: A New Way to Clean. Dent. J. 2023, 11, 224. https://doi.org/10.3390/dj11090224
Strickland M, Mills S, Dasari B, Markowitz K, Cugini C. Design and Initial Evaluation of a Novel Oral Hygiene Technology for a Special Needs Population: A New Way to Clean. Dentistry Journal. 2023; 11(9):224. https://doi.org/10.3390/dj11090224
Chicago/Turabian StyleStrickland, Maxine, Steven Mills, Bhargavi Dasari, Kenneth Markowitz, and Carla Cugini. 2023. "Design and Initial Evaluation of a Novel Oral Hygiene Technology for a Special Needs Population: A New Way to Clean" Dentistry Journal 11, no. 9: 224. https://doi.org/10.3390/dj11090224