
Emerging Pattern of Post-COVID-19 Parosmia and Its Effect on Food Perception

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Recruitment
2.2. The Questionnaire
2.3. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Origin and Progression of Olfactory Dysfunction
3.2.1. Aetiology
3.2.2. Timings of Smell Loss
3.2.3. Severity of COVID-19
3.2.4. Intermittent Recovery of Olfactory Function
3.2.5. Changes in Taste and Chemesthesis
3.3. Distortion, Disgust, and Strength of Triggers Foods
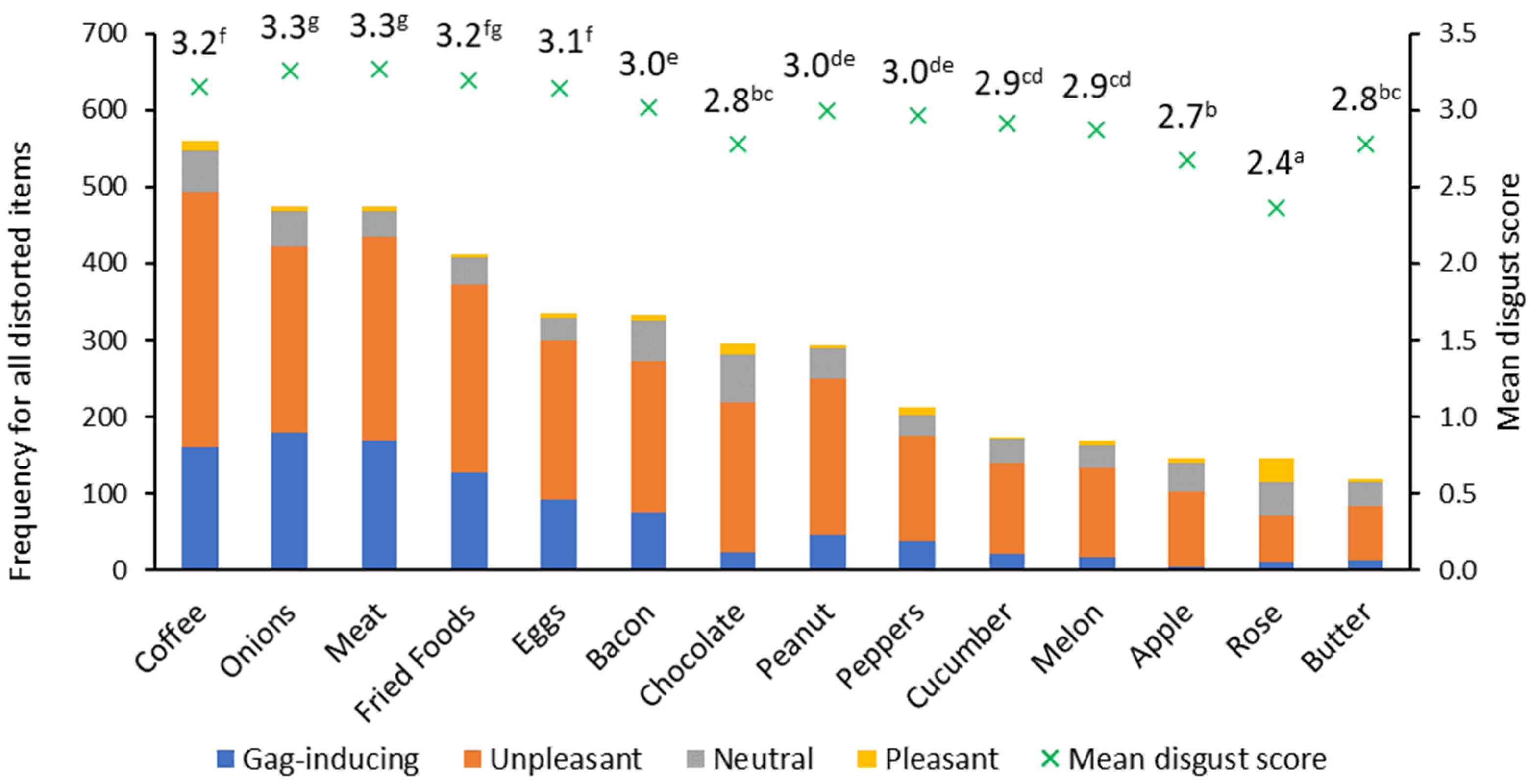
3.3.1. Key Trigger Foods
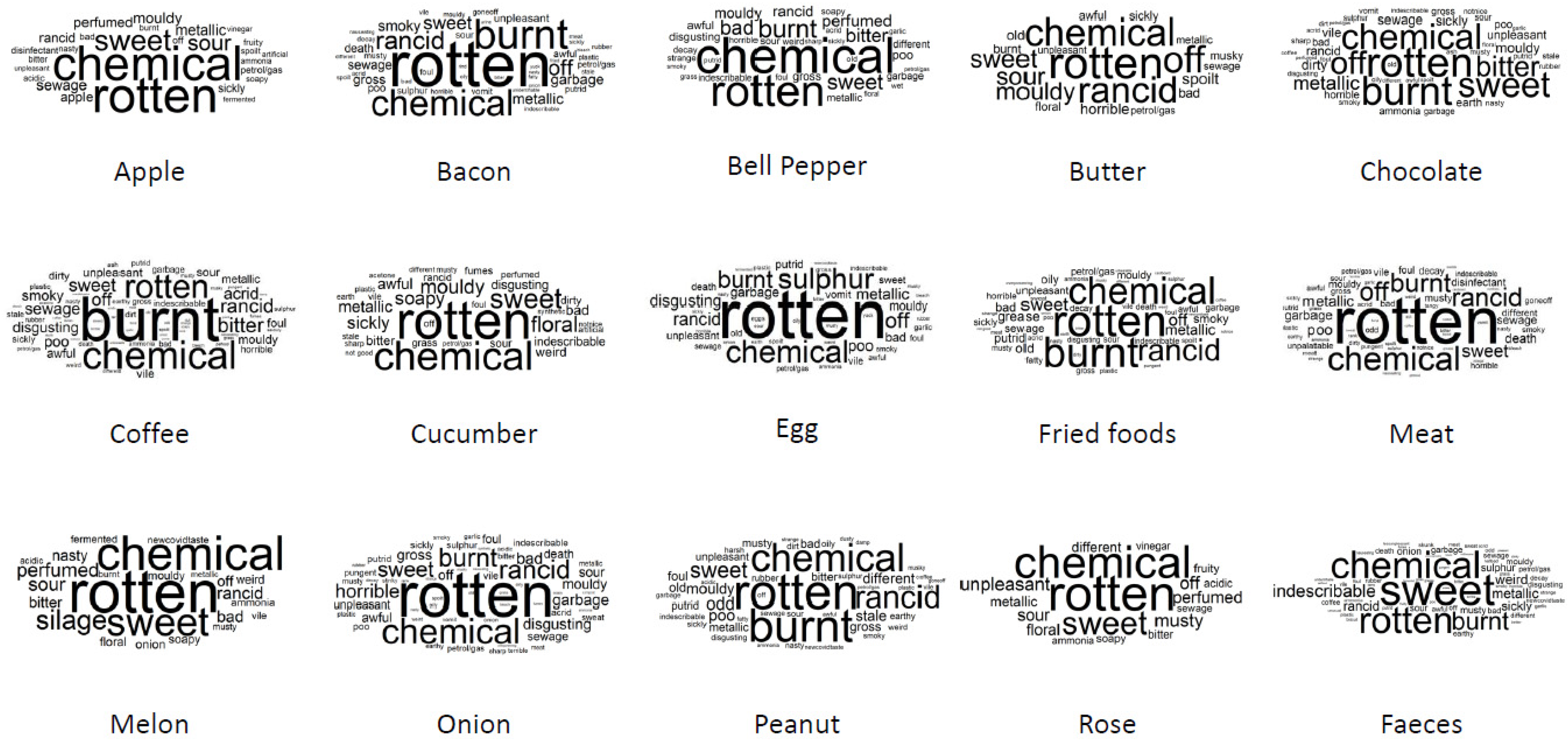
3.3.2. Characterisation of Distortions
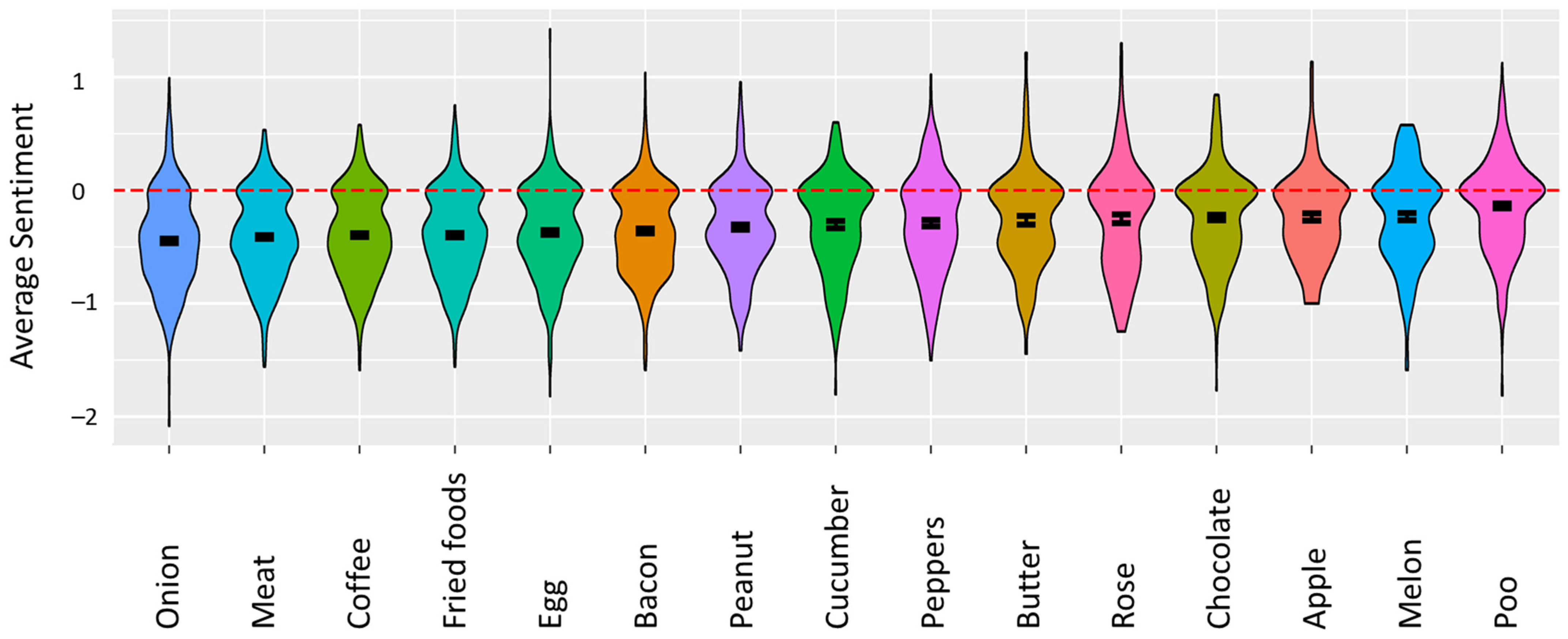
3.3.3. Valence of Distortions
3.3.4. Strength of Distortions
3.3.5. Faecal Odour
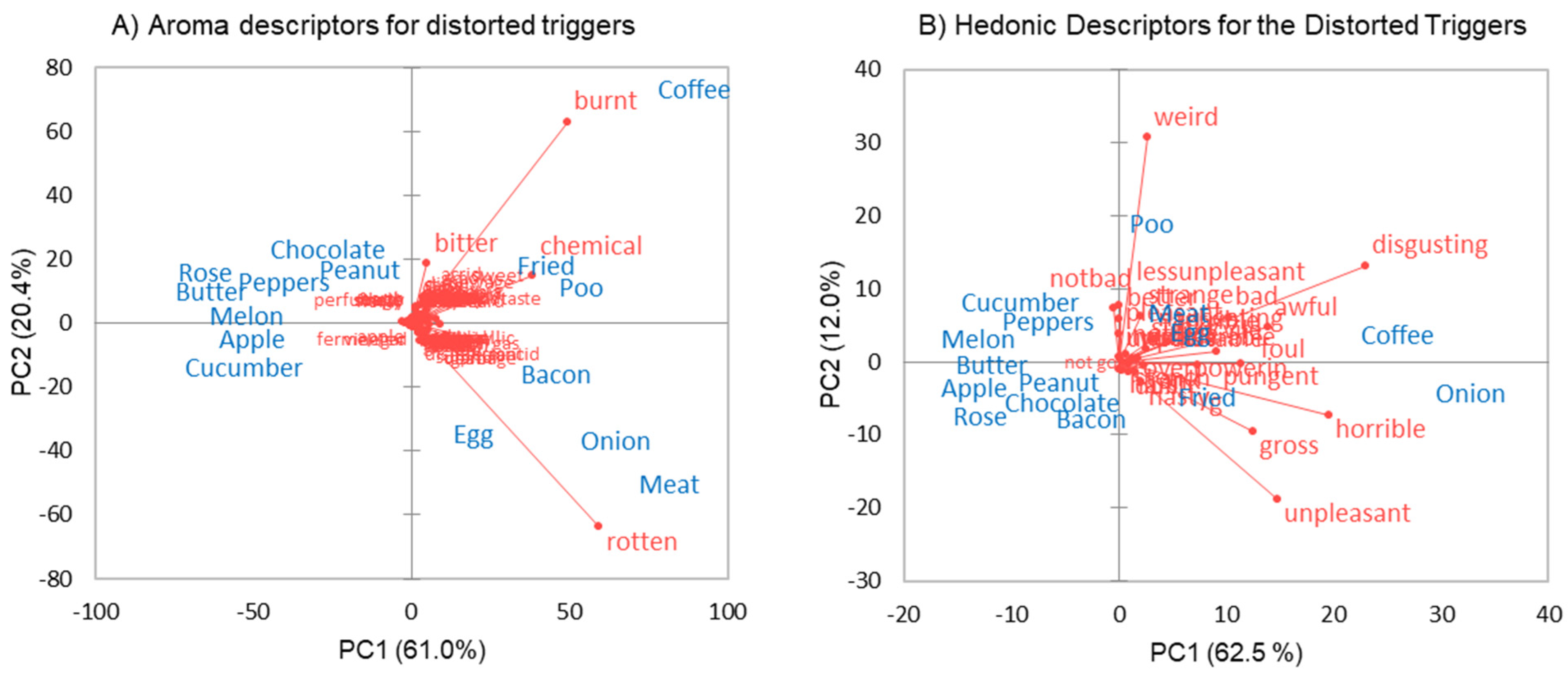
3.3.6. Additional Triggers of Distortion (CATA)
3.3.7. Additional Triggers (Free Text)
3.4. Analysis of the Free Text Question
“It is really hard to find words to describe the new smells. I talked to my doctor three times since March, and his suggestions underlines the need for more knowledge and awareness. He answered me as if he really did not understand that the smells are different now …”.
“I only sense one unpleasant smell. Everything that has distorted smell, smells almost the same”.
“I seem to have two types of distortion ‘categories’—coffee, chocolate, onions etc taste like a musky, nutty, rancid, earthy taste. And things like peppers and melon taste more chemical, like something that would be flammable”.
“For me, my feaces [sic], urine and sweat have the same bad smell like the other distorted smells (like onion and fried meat). The bad smell is not familiar to me from before and it messes my head that my food smells like my body waste”.
“Shampoos, cleaning products, soaps, perfumes, etc.,smell so strong I feel like my nose burns”.“I have a weird constant taste in my mouth which matches the weird smell I keep smelling in everything”.
“My diet is quite limited at present so there may be other foods that smell distorted but I haven’t tried to eat them in the last week”.
“I am on a strict diet of fresh corn […], apricots, peaches, plums, grapes, cherries, cucumber, Fairlife protein shakes, diet Dr Pepper (coke and other sodas taste like pure dirt/mud), fresh mozzarella (all other hard cheeses, especially yellow cheddar, are rancid)”.
“Weight is increasing as the only tolerable foods are all sugary, stodgy, high fat, high calorie”.
“I am very sad and losing weight it feels worse every day that passes”.
“Distortion of smells fluctuates. Sometimes I can smell something and it smells normal, then I smell it again and it is distorted or I can’t smell it at all”.
“The distorted odours fluctuate in strength but are never totally absent. Sometimes they linger even after the source is removed, and the memory of the odour alone can be enough to make me conscious of it, as though I can smell it, even if there is no odour source present”.
“I still smell very little but sometimes have an initial weak or distorted ‘whiff’ of an item but on a second sniff I cannot smell anything. This has been happening since about 3 months after losing sense of smell”.
“I never lost my sense of smell. Parosmia came on suddenly. There was no absence of smell transition as implied in many questions”.
“Parosmia really affects mental health. Cannot eat out or socialise. … It is the weirdest thing but nobody believes you if you try to explain it. Cannot face the not knowing of how long it might last”.
“This needs to be over, it’s ruining my life and not worth getting up for this is severely effecting my way of life and it’s nice to know others care”.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Other Distorted Smells Personal Care | Count 1 | Other Distorted Smells Home and Environment | Count 1 | Other Distorted Smells Foods and Beverages | Count 1 |
|---|---|---|---|---|---|
| Daily washing/ grooming (445) | Home cleaning (223) | Herbs (119) | |||
| soap | 132 | cleaning products | 110 | mint | 81 |
| deodorants/antiperspirant | 106 | detergents | 75 | herbs | 15 |
| shower gel | 91 | fabric softner | 38 | basil | 12 |
| personal care products | 63 | Sanitisers (98) | rosemary | 11 | |
| cosmetics and toiletries | 35 | sanitisers | 46 | Fruit (114) | |
| nail care | 12 | bleach | 39 | citrus (lemon, orange, lime) | 83 |
| sun cream | 6 | wipes | 13 | strawberries | 31 |
| Personal Fragrances (272) | Environment (96) | Alcoholic beverages (103) | |||
| perfume | 223 | water | 44 | wine | 63 |
| candles | 30 | air | 14 | beer | 22 |
| aftershave | 19 | garbage | 10 | rubbing alcohol | 8 |
| Hair care (247) | chlorine | 9 | gin | 7 | |
| shampoo | 178 | coast | 8 | cider | 3 |
| conditioner | 44 | rain/petrichor | 6 | Carbohydrates (101) | |
| hair products | 25 | manure | 4 | bread | 46 |
| Oral care (146) | tarmac | 1 | cookies biscuits | 15 | |
| toothpaste | 133 | Essential oils (95) | baked goods | 14 | |
| mouthwash | 13 | other essential oils | 39 | rice, rice cakes | 12 |
| Body aromas (132) | eucalyptus/Vicks | 27 | pasta | 11 | |
| other body odour | 76 | lavender | 27 | tortilla | 3 |
| urine | 44 | rose essential oil | 2 | Dairy (55) | |
| breath | 7 | Garden (90) | cheese | 24 | |
| new born baby/husband | 5 | grass | 47 | tea | 15 |
| flowers | 20 | milk | 11 | ||
| plants, leaves | 12 | dairy | 5 | ||
| soil, earth | 6 | Vegetables and pulses (54) | |||
| trees | 5 | brassica | 21 | ||
| Miscellaneous (58) | salad | 15 | |||
| everything | 41 | peas and beans, pinto | 14 | ||
| marijuana | 17 | chickpeas | 2 | ||
| Car (43) | soya | 2 | |||
| petrol/diesel fumes | 42 | Spices (48) | |||
| plastic/interior | 1 | coriander, cilantro | 19 | ||
| Pets (32) | ginger (beer, tea, lotion) | 9 | |||
| petfood | 16 | mustard | 5 | ||
| pet | 13 | clove | 4 | ||
| cat litter | 3 | cinnamon | 4 | ||
| Smoke (28) | cumin | 4 | |||
| smoke | 22 | paprika | 3 | ||
| bonfire | 6 | Fish (18) | |||
| Home (4) | fish, tuna | 18 | |||
| pens/crayons | 2 |
References
- Spence, C. Just how much of what we taste derives from the sense of smell? Flavour 2015, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Croy, I.; Nordin, S.; Hummel, T. Olfactory Disorders and Quality of Life—An Updated Review. Chem. Senses 2014, 39, 185–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burges Watson, D.L.; Campbell, M.; Hopkins, C.; Smith, B.; Kelly, C.; Deary, V. Altered Smell and Taste: Anosmia, parosmia and the impact of long COVID-19. PLoS ONE 2020, 16, e0256998. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundags, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position paper on olfactory dysfunction. Rhinol. Suppl. 2017, 54, 1–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, A.; Malaspina, D. Hidden consequences of olfactory dysfunction: A patient report series. BMC Ear Nose Throat Disord. 2013, 13, 8. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, C.; Surda, P.; Vaira, L.A.; Lechien, J.R.; Safarian, M.; Saussez, S.; Kumar, N. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinology 2020, 59, 26–31. [Google Scholar] [CrossRef]
- Olofsson, J.K.; Ekesten, F.; Nordin, S. Smell distortions: Prevalence, longevity and impact of parosmia in a population-based, longitudinal study spanning 10 years. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Parker, J.K.; Kelly, C.E.; Kirkwood, A.F.; Smith, B.C.; Hopkins, C.; Gane, S. Patients’ Perspectives on Qualitative Olfactory Dysfunction: Thematic Analysis of Social Media Posts. JMIR Form. Res. 2021, 5, e29086. [Google Scholar] [CrossRef]
- Teaima, A.A.; Salem, O.M.; Teama, M.; Mansour, O.I.; Taha, M.S.; Badr, F.M.; Khater, S.S.; Abdou, K.; Mahmoud, M.S. Patterns and clinical outcomes of olfactory and gustatory disorders in six months: Prospective study of 1031 COVID-19 patients. Am. J. Otolaryngol. 2022, 43, 103259. [Google Scholar] [CrossRef]
- Parker, J.K.; Kelly, C.E.; Gane, S.B. Molecular Mechanism of Parosmia. medRxiv 2021. [Google Scholar] [CrossRef]
- Ooms, J. Hunspell: High-Performance Stemmer, Tokenizer, and Spell Checker (3.0.1) [Computer Software]. 2020. Available online: https://cran.r-project.org/web/packages/hunspell/index.html (accessed on 15 February 2022).
- Pennec, E.; Slowikowski, K. Ggwordcloud: A Word Cloud Geom for ‘ggplot2’, 0.3.0 [Computer Software]. 2018. Available online: https://cran.r-project.org/web/packages/ggwordcloud/vignettes/ggwordcloud.html (accessed on 15 February 2022).
- Rinker, T.W. Sentimentr: Calculate Text Polarity Sentiment, (2.7.1) [R Package]. 2019. Available online: https://github.com/trinker/sentimentr (accessed on 15 February 2022).
- Koyama, S.; Ueha, R.; Kondo, K. Loss of Smell and Taste in Patients with Suspected COVID-19: Analyses of Patients’ Reports on Social Media. J. Med. Internet Res. 2021, 23, e26459. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Mainland, J.D.; Kelly, C.E.; Parker, J.K.; Hummel, T. Prevalence and Correlates of Parosmia and Phantosmia among Smell Disorders. Chem. Senses 2021, 46, bjab046. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-C.; Holbrook, E.H.; Leopold, D.A.; Hummel, T. Distorted olfactory perception: A systematic review. Acta Oto-Laryngol. 2012, 132, S27–S31. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Sandison, A.; Manca, A.; Machouchas, N.; Turilli, D.; Lechien, J.R.; Barillari, M.R.; Salzano, G.; Cossu, A.; et al. Olfactory epithelium histopathological findings in long-term coronavirus disease 2019 related anosmia. J. Laryngol. Otol. 2020, 134, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Borsetto, D.; Hopkins, C.; Philips, V.; Obholzer, R.; Tirelli, G.; Polesel, J.; Boscolo-Rizzo, P. Self-reported alteration of sense of smell or taste in patients with COVID-19: A systematic review and meta-analysis on 3563 patients. Rhinology 2020, 58, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Gane, S.B.; Kelly, C.; Hopkins, C. Isolated sudden onset anosmia in COVID-19 infection. A novel syndrome? Rhinology 2020, 58, 299–301. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Beckers, E.; Mustin, V.; Ducarme, M.; Journe, F.; Marchant, A.; Jouffe, L.; Barillari, M.R.; Cammaroto, G.; et al. Prevalence and 6-month recovery of olfactory dysfunction: A multicentre study of 1363 COVID-19 patients. J. Intern. Med. 2021, 290, 451–461. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-L 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Ostrander, B.T.; DeConde, A.S. Self-reported olfactory loss associates with outpatient clinical course in COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 821–831. [Google Scholar] [CrossRef] [Green Version]
- Cooper, K.W.; Brann, D.H.; Farruggia, M.C.; Bhutani, S.; Pellegrino, R.; Tsukahara, T.; Weinreb, C.; Joseph, P.V.; Larson, E.D.; Parma, V.; et al. COVID-19 and the Chemical Senses: Supporting Players Take Center Stage. Neuron 2020, 107, 219–233. [Google Scholar] [CrossRef]
- Parma, V.; Ohla, K.; Veldhuizen, M.G.; Niv, M.Y.; Kelly, C.E.; Bakke, A.J.; Cooper, K.W.; Bouysset, C.; Pirastu, N.; Dibattista, M.; et al. More than smell—COVID-19 is associated with severe impairment of smell, taste, and chemesthesis. Chem. Senses 2020, 45, 609–622. [Google Scholar] [CrossRef] [PubMed]
- Alon, E.E.; Glikson, E.; Shoshani, Y.; Dobriyan, A.; Yahalom, R.; Yakirevitch, A. Six-month smell and taste recovery rates in coronavirus disease 2019 patients: A prospective psychophysical study. J. Laryngol. Oto. 2021, 135, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Ohla, K.; Veldhuizen, M.G.; Green, T.; Hannum, M.E.; Bakke, A.J.; Moein, S.T.; Tognetti, A.; Postma, E.M.; Pellegrino, R.; Hwang, L.-D.; et al. Increasing incidence of parosmia and phantosmia in patients recovering from COVID-19 smell loss. Rhinology, 2021; in press. [Google Scholar]
- Deems, D.A.; Doty, R.L.; Settle, R.G.; Moore-Gillon, V.; Shaman, P.; Mester, A.F.; Kimmelman, C.P.; Brightman, V.J.; Snow, J.B., Jr. Smell and Taste Disorders, A Study of 750 Patients from the University of Pennsylvania Smell and Taste Center. Arch. Otorhinolaryngol. Head Neck Surg. 1991, 117, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Siviero, M.; Teixeira, M.J.; Siqueira, J.T.; Siqueira, S.R. Central mechanisms in burning mouth syndrome involving the olfactory nerve: A preliminary study. Clinics 2011, 66, 509–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, R.J.; Mahmut, M.K.; Horstmann, A.; Hummel, T. The Aetiology of Olfactory Dysfunction and Its Relationship to Diet Quality. Brain Sci. 2020, 10, 769. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y.; Han, P.; Burghardt, S.; Knaapila, A.; Schriever, V.; Hummel, T. Influence of olfactory dysfunction on the perception of food. Eur. Arch. Oto-Rhino-L 2019, 276, 2811–2817. [Google Scholar] [CrossRef]
- Kershaw, J.C.; Mattes, R.D. Nutrition and taste and smell dysfunction. World J. Otorhinolaryngol. Head Neck Surg. 2018, 4, 3–10. [Google Scholar] [CrossRef]
- Pellegrino, R.; Hummel, T.; Emrich, R.; Chandra, R.; Turner, J.; Trone, T.; Dorminy, C.; Luckett, C.R. Cultural determinants of food attitudes in anosmic patients. Appetite 2020, 147, 104563. [Google Scholar] [CrossRef]
- Chaaban, N.; Hoier, A.T.Z.B.; Andersen, B.V. A Detailed Characterisation of Appetite, Sensory Perceptional, and Eating-Behavioural Effects of COVID-19: Self-Reports from the Acute and Post-Acute Phase of Disease. Foods 2021, 10, 892. [Google Scholar] [CrossRef]
- Rawal, S.; Duffy, V.B.; Berube, L.; Hayes, J.E.; Kant, A.K.; Li, C.-M.; Graubard, B.I.; Hoffman, H.J. Self-Reported Olfactory Dysfunction and Diet Quality: Findings from the 2011-2014 National Health and Nutrition Examination Survey (NHANES). Nutrients 2021, 13, 4561. [Google Scholar] [CrossRef]
- Leopold, D. Distortion of olfactory perception: Diagnosis and treatment. Chem. Senses 2002, 27, 611–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doty, R.L. The mechanisms of smell loss after SARS-CoV-2 infection. Lancet Neurol. 2021, 20, 693–695. [Google Scholar] [CrossRef]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.J.; Fletcher, R.B.; et al. Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef] [PubMed]



| Statistic | Count | Percent | |
|---|---|---|---|
| Total Respondents | 727 | ||
| Sex | Male | 76 | 10% |
| Female | 651 | 90% | |
| Age | Range (years) | 18–75 | |
| Mean (years) | 43 | ||
| Country of Residence | UK | 330 | 45% |
| USA | 297 | 41% | |
| Canada | 15 | 2% | |
| Spain | 9 | 1% | |
| The Netherlands | 8 | 1% | |
| Others (<1%) | 68 | 9% | |
| Ethnicity | White European | 396 | 54% |
| White North American | 205 | 28% | |
| White Other | 30 | 4% | |
| Other Ethnic Group | 20 | 3% | |
| White South American | 17 | 2% | |
| South Asian | 11 | 2% | |
| Prefer not to say | 10 | 1% | |
| Others (<1%) | 38 | 5% | |
| Smoking status | Smoker | 52 | 7% |
| Non-smoker | 531 | 73% | |
| Ex-smoker | 144 | 20% | |
| Aetiology | COVID-19 (diagnosed) | 367 | 50% |
| COVID-19 (self-diagnosed) | 239 | 33% | |
| Viral non-COVID-19 pre-Dec 2019 | 58 | 8% | |
| Viral non-COVID-19 post-Dec 2019 | 5 | 1% | |
| Accident, head/brain injury | 14 | 2% | |
| Unexplained (idiopathic) | 12 | 2% | |
| Other | 7 | 1% | |
| Do not know | 25 | 3% | |
| Severity of COVID-19 | Loss of smell only | 66 | 11% |
| Mild | 194 | 32% | |
| Moderate | 226 | 37% | |
| Severe | 117 | 19% | |
| Very severe (hospitalised) | 3 | 0.5% |
| COVID-19 n = 606 | Non-COVID-19 n = 63 | |
|---|---|---|
| very suddenly, before the other symptoms of infection appeared | 127 (21%) | 1 (2%) |
| very suddenly, during the infection | 344 (57%) | 29 (46%) |
| very suddenly, after the infection | 69 (11%) | 9 (14%) |
| gradually, I only noticed it was gone when I was recovering from the infection | 66 (11%) | 24 (28%) |
| COVID-19 | Non-COVID-19 | |
|---|---|---|
| no recovery of normal sense of smell | 108 (18%) | 46 (73%) |
| just a few hints that a sense of smell was returning and nothing else | 171 (28%) | 11 (17%) |
| partial recovery of a normal sense of smell | 206 (34%) | 5 (8%) |
| full recovery of a normal sense of smell | 121 (20%) | 1 (2%) |
| Item | Reported as Distorted Freq (%) 1 | Item | Reported as Not Detected Freq (%) 1 | Item | Reported as Normal Freq (%) 1 |
|---|---|---|---|---|---|
| Butter | 18 | Coffee | 7 | Meat | 11 |
| Apple | 23 | Onion | 18 | Coffee | 11 |
| Rose | 25 | Meat | 18 | Onion | 12 |
| Cucumber | 29 | Fried foods | 18 | Egg | 18 |
| Melon | 32 | Bacon | 21 | Fried foods | 20 |
| Peppers | 36 | Peanuts | 24 | Bacon | 22 |
| Chocolate | 43 | Chocolate | 27 | Peanuts | 26 |
| Peanuts | 50 | Egg | 29 | Chocolate | 30 |
| Egg | 53 | Cucumber | 30 | Peppers | 31 |
| Bacon | 57 | Peppers | 33 | Melon | 34 |
| Fried foods | 61 | Melon | 33 | Rose | 36 |
| Onion | 70 | Apple | 36 | Butter | 39 |
| Meat | 71 | Rose | 39 | Cucumber | 40 |
| Coffee | 82 | Butter | 44 | Apple | 41 |
| Distorted Aromas | Count 1 | Distorted Aromas (Contd) | Count 1 | Distorted Aromas (Contd) | Count 1 |
|---|---|---|---|---|---|
| Coffee | 570 | Peanuts | 301 | Celery | 142 |
| Garlic | 496 | Bananas | 289 | Carrots | 131 |
| Onion | 495 | Popcorn | 288 | Peaches | 130 |
| Meat | 490 | Cigarettes | 277 | Vanilla | 130 |
| Room freshener | 435 | Peppers | 217 | Mango | 122 |
| Fried foods | 424 | Tomatoes | 204 | Hazelnuts | 122 |
| Cola drinks | 356 | Cucumber | 178 | Butter | 120 |
| Egg | 350 | Melon | 171 | Walnuts | 115 |
| Bacon | 340 | Rose | 148 | Grapefruit | 112 |
| Toast | 336 | Apple | 147 | Passionfruit | 84 |
| Petrol | 318 | Raspberries | 146 | Honey | 80 |
| Chocolate | 302 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parker, J.K.; Methven, L.; Pellegrino, R.; Smith, B.C.; Gane, S.; Kelly, C.E. Emerging Pattern of Post-COVID-19 Parosmia and Its Effect on Food Perception. Foods 2022, 11, 967. https://doi.org/10.3390/foods11070967
Parker JK, Methven L, Pellegrino R, Smith BC, Gane S, Kelly CE. Emerging Pattern of Post-COVID-19 Parosmia and Its Effect on Food Perception. Foods. 2022; 11(7):967. https://doi.org/10.3390/foods11070967
Chicago/Turabian StyleParker, Jane K., Lisa Methven, Robert Pellegrino, Barry C. Smith, Simon Gane, and Christine E. Kelly. 2022. "Emerging Pattern of Post-COVID-19 Parosmia and Its Effect on Food Perception" Foods 11, no. 7: 967. https://doi.org/10.3390/foods11070967