

Ergonomic Analysis of Dental Work in Different Oral Quadrants: A Motion Capture Preliminary Study among Endodontists
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measuring System
2.3. Experimental Setup and Realisation
- Task 1
- An already prepared rubber dam was positioned by the dentist. The dental assistant provided assistance.
- Task 2
- Trepanation of the tooth was undertaken so that all canals could be probed with an ISO 20 K-file [46].
- Task 3
- Root canal preparation was undertaken with hand files (K-files, ISO 35-45 [46]) using circumferential filing with a specified working length (WL); adjustment of the WL was made by the dental assistant.
- Task 4
- The rubber dam was removed by the dentist. The dental assistant provided assistance.
2.4. Rapid Upper Limb Assessment (RULA)
2.5. Data Processing
- RULA score:
- 2.
- Relative average risk score over time (Rel. av. RST):
- RULA total score (“Final overall”): this includes the body parts from the right or left with the greater risk in each case;
- RULA—total score on the right (“Final overall right”): this looks at the right half of the body (Step 1 right, Step 2 right, Step 3 + 4 right, Step 9, Step 10);
- RULA—total score on the left (“Final overall left”): this considers the left half of the body (Step 1 left, Step 2 left, Step 3 + 4 left, Step 9, Step 10);
- Local scores:
| - | Upper Arm Score (left and right) | - | RULA Step 1 |
| - | Lower Arm Score (left and right) | - | RULA Step 2 |
| - | Wrist Score (left and right) | - | RULA Steps 3 + 4 |
| - | Neck Score | - | RULA Step 9 |
| - | Trunk Score | - | RULA Step 10 |
2.6. Statistical Analysis
3. Results
3.1. RULA Score
3.2. Relative Average Risk Score over Time (Rel. av. RST)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 13, e0208628. [Google Scholar] [CrossRef] [PubMed]
- Chenna, D.; Pentapati, K.C.; Kumar, M.; Madi, M.; Siddiq, H. Prevalence of musculoskeletal disorders among dental healthcare providers: A systematic review and meta-analysis. F1000Research 2022, 11, 1062. [Google Scholar] [CrossRef] [PubMed]
- Jacquier-Bret, J.; Gorce, P. Prevalence of Body Area Work-Related Musculoskeletal Disorders among Healthcare Professionals: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 841. [Google Scholar] [CrossRef] [PubMed]
- Soo, S.Y.; Ang, W.S.; Chong, C.H.; Tew, I.M.; Yahya, N.A. Occupational ergonomics and related musculoskeletal disorders among dentists: A systematic review. Work 2023, 74, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Suganthirababu, P.; Parveen, A.; Krishna, P.M.; Sivaram, B.; Kumaresan, A.; Srinivasan, V.; Vishnuram, S.; Alagesan, J.; Prathap, L. Prevalence of work-related musculoskeletal disorders among health care professionals: A systematic review. Work 2023, 74, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Pai, K.M.; Vineetha, R. Occupation-related musculoskeletal disorders among dental professionals. Med. Pharm. Rep. 2020, 93, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Zarra, T.; Lambrianidis, T. Musculoskeletal disorders amongst Greek endodontists: A national questionnaire survey. Int. Endod. J. 2014, 47, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.; Zafar, H.; Iqbal, Z.A. Work-related musculoskeletal disorders among dental professionals in Saudi Arabia. J. Phys. Ther. Sci. 2015, 27, 1107–1112. [Google Scholar] [CrossRef]
- Marklin, R.W.; Cherney, K. Working Postures of Dentists and Dental Hygienists. J. Calif. Dent. Assoc. 2005, 33, 133–136. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Erbe, C.; Nowak, J.; Hauck, I.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Constrained posture in dentistry—A kinematic analysis of dentists. BMC Musculoskelet. Disord. 2017, 18, 291. [Google Scholar] [CrossRef]
- De Sio, S.; Traversini, V.; Rinaldo, F.; Colasanti, V.; Buomprisco, G.; Perri, R.; Mormone, F.; La Torre, G.; Guerra, F. Ergonomic risk and preventive measures of musculoskeletal disorders in the dentistry environment: An umbrella review. PeerJ 2018, 6, e4154. [Google Scholar] [CrossRef] [PubMed]
- Nassiri, N.; Maas, M.; Basin, M.; Cacciamani, G.E.; Doumanian, L.R. Urethral complication after gender reassignment surgery: A systematic review. Int. J. Impot. Res. 2020, 33, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Holzgreve, F.; Schulte, L.; Oremek, G.; Ohlendorf, D. Allgemeine und arbeitsplatzbezogene Risikofaktoren von Muskel-Skelett-Erkrankungen und deren Bestimmungsmethoden. Zentralblatt Arbeitsmedizin Arbeitsschutz Ergon. 2023, 73, 182–189. [Google Scholar] [CrossRef]
- Al-Rawi, N.H.; El Khatib, H.; Rajoub, L.; El-Sayed, M.; Naji, R.; Youssef, R.; Al Kawas, S. Work-related Musculoskeletal Pain among Different Dental Specialists in United Arab Emirates. J. Contemp. Dent. Pract. 2016, 17, 639–644. [Google Scholar] [CrossRef]
- Onety, G.C.D.S.; Leonel, D.V.; Saquy, P.C.; Da Silva, G.P.; Ferreira, B.; Varise, T.G.; De Sousa, L.G.; Verri, E.D.; Siéssere, S.; Semprini, M.; et al. Analysis of Endodontist Posture Utilizing Cinemetry, Surface Electromyography and Ergonomic Checklists. Braz. Dent. J. 2014, 25, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesetzliche Unfallversicherung (DGUV). Mensch und Arbeitsplatz–Physische Belastungen. 2019. Available online: https://publikationen.dguv.de/widgets/pdf/download/article/3499 (accessed on 7 June 2023).
- Pejčić, N.; Petrović, V.; Marković, D.; Miličić, B.; Dimitrijević, I.I.; Perunović, N.; Čakić, S. Assessment of risk factors and preventive measures and their relations to work-related musculoskeletal pain among dentists. Work 2017, 57, 573–593. [Google Scholar] [CrossRef] [PubMed]
- Adulyawat, W.; Chokechanachaisakul, U.; Janwantanakul, P. Poor neck posture and longer working duration during root canal treatment correlated with increased neck discomfort in dentists with <5-years‘ experience in endodontics. J. Occup. Health 2022, 64, e12362. [Google Scholar] [CrossRef] [PubMed]
- Kierklo, A.; Kobus, A.; Jaworska, M.; Botuliński, B. Work-related musculoskeletal disorders among dentists—A questionnaire survey. Ann. Agric. Environ. Med. 2011, 18, 79–84. [Google Scholar]
- Hayes, M.; Cockrell, D.; Smith, D.R. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009, 7, 159–165. [Google Scholar] [CrossRef]
- Younis, U.; Shakoor, A.; Chaudhary, F.A.; Din, S.U.; Sajjad, S.; Younis, M.; Javed, M.Q.; Alam, M.K. Work-Related Musculoskeletal Disorders and Their Associated Risk Factors among Pakistani Dental Practitioners: A Cross-Sectional Study. BioMed Res. Int. 2022, 2022, 4099071. [Google Scholar] [CrossRef]
- Hussein, A.; Mando, M.; Radisauskas, R. Work-Related Musculoskeletal Disorders among Dentists in the United Arab Emirates: A Cross-Sectional Study. Medicina 2022, 58, 1744. [Google Scholar] [CrossRef] [PubMed]
- Alnaser, M.Z.; Almaqsied, A.M.; Alshatti, S.A. Risk factors for work-related musculoskeletal disorders of dentists in Kuwait and the impact on health and economic status. Work 2021, 68, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; McCullough, M.; Panisset, M.G.; Galea, M.P. Prevention of work-related musculoskeletal disorders among dental professionals: A scoping review. Work 2022, 72, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Roll, S.C.; Tung, K.D.; Chang, H.; Sehremelis, T.A.; Fukumura, Y.E.; Randolph, S.; Forrest, J.L. Prevention and rehabilitation of musculoskeletal disorders in oral health care professionals: A systematic review. J. Am. Dent. Assoc. 2019, 150, 489–502. [Google Scholar] [CrossRef] [PubMed]
- Lietz, J.; Ulusoy, N.; Nienhaus, A. Prevention of Musculoskeletal Diseases and Pain among Dental Professionals through Ergonomic Interventions: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 3482. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Maltry, L.; Hänel, J.; Betz, W.; Erbe, C.; Maurer-Grubinger, C.; Holzgreve, F.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; et al. SOPEZ: Study for the optimization of ergonomics in the dental practice—Musculoskeletal disorders in dentists and dental assistants: A study protocol. J. Occup. Med. Toxicol. 2020, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Blume, K.S.; Holzgreve, F.; Fraeulin, L.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; Maurer-Grubinger, C.; Groneberg, D.A.; et al. Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data. Int. J. Environ. Res. Public Health 2021, 18, 10550. [Google Scholar] [CrossRef] [PubMed]
- Holzgreve, F.; Fraeulin, L.; Betz, W.; Erbe, C.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; Groneberg, D.A.; Maurer-Grubinger, C.; Ohlendorf, D. A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics. Sensors 2022, 22, 805. [Google Scholar] [CrossRef] [PubMed]
- Weitbrecht, M.; Holzgreve, F.; Fraeulin, L.; Haenel, J.; Betz, W.; Erbe, C.; Maurer-Grubinger, C.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; et al. Ergonomic Risk Assessment of Oral and Maxillofacial Surgeons—RULA Applied to Objective Kinematic Data. Hum. Factors J. Hum. Factors Ergon. Soc. 2022, 65, 1655–1673. [Google Scholar] [CrossRef]
- Nowara, R.; Holzgreve, F.; Golbach, R.; Wanke, E.M.; Maurer-Grubinger, C.; Erbe, C.; Brueggmann, D.; Nienhaus, A.; Groneberg, D.A.; Ohlendorf, D. Testing the Level of Agreement between Two Methodological Approaches of the Rapid Upper Limb Assessment (RULA) for Occupational Health Practice—An Exemplary Application in the Field of Dentistry. Bioengineering 2023, 10, 477. [Google Scholar] [CrossRef]
- Kamal, A.M.; Ahmed, D.R.M.; Habib, S.F.K.; Al-Mohareb, R.A. Ergonomics of preclinical dental students and potential musculoskeletal disorders. J. Dent. Educ. 2020, 84, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Corrales Zúniga, I.A.; Sauceda Malespín, N.L.; Vega Vílchez, A.L.; Duarte Frenky, O.J.; Hong, G.; Vanegas Sáenz, J.R. Evaluation of the ergonomic sitting position adopted by dental students while using dental simulators. J. Dent. Sci. 2023, 18, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Xsens. MVN User Manual; Xsens: Enschede, The Netherlands, 2017. [Google Scholar]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl. Ergon. 2013, 44, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Vignais, N.; Bernard, F.; Touvenot, G.; Sagot, J.-C. Physical risk factors identification based on body sensor network combined to videotaping. Appl. Ergon. 2017, 65, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Arbeitsmedizin und Umweltmedizin (DGAUM), Gesellschaft für Arbeitswissenschaft (GfA). Körperliche Belastungen des Rückens durch Lastenhandhabung und Zwangshaltungen im Arbeitsprozess S1-Leitlinie. 2013. Available online: https://register.awmf.org/assets/guidelines/002-029l_S1_K%C3%B6rperliche_Belastungen_des_R%C3%BCckens_2014-01-abgelaufen.pdf (accessed on 11 March 2024).
- Maurer-Grubinger, C.; Holzgreve, F.; Fraeulin, L.; Betz, W.; Erbe, C.; Brueggmann, D.; Wanke, E.M.; Nienhaus, A.; Groneberg, D.A.; Ohlendorf, D. Combining Ergonomic Risk Assessment (RULA) with Inertial Motion Capture Technology in Dentistry—Using the Benefits from Two Worlds. Sensors 2021, 21, 4077. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, M.-È.; Imbeau, D.; Aubry, K.; Delisle, A. Comparing the results of eight methods used to evaluate risk factors associated with musculoskeletal disorders. Int. J. Ind. Ergon. 2012, 42, 478–488. [Google Scholar] [CrossRef]
- Fang, Z.; Woodford, S.; Senanayake, D.; Ackland, D. Conversion of Upper-Limb Inertial Measurement Unit Data to Joint Angles: A Systematic Review. Sensors 2023, 23, 6535. [Google Scholar] [CrossRef]
- Kimmel, K. Ein Identifikationssystem für die zahnärztliche Ausrüstung. Zahnarztl. Mitt. 1973, 65, 522–527. [Google Scholar]
- Kimmel, K. Der zahnärztliche Arbeitsplatz: Funktion und Gestaltung. Zahnärztliche Welt. 1980, 89, 40–52. [Google Scholar]
- Kimmel, K. Die Basiskonzepte Grundlage der Behandlungsplatzgestaltung. Quintessenz Zahntech. 1989, 40, 2251–2258. [Google Scholar]
- Kimmel, K. Zahnärztliche Praxis- und Arbeitsgestaltung: Ergonomie als Grundlage der Leistungs- und Lebensqualität; Dt. Zahnärzteverl, DÄV-Hanser: München, Germany, 2001. [Google Scholar]
- DIN EN ISO 3630-1:2020-01; Dentistry-Endodontic Instruments- Part 1: General Requirements. Beuth Verlag GmbH: Berlin, Germany, 2020.
- Garcia, P.P.N.S.; Pugliesi, P.M.S.; Wajngarten, D.; Neves, T.d.C.; Pazos, J.M.; Dovigo, L.N. Development and assessment of an indirect vision training programme for operatory dentistry: Effects on working posture. Eur. J. Dent. Educ. 2021, 26, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Katano, K.; Nakajima, K.; Saito, M.; Kawano, Y.; Takeda, T.; Fukuda, K. Effects of Line of Vision on Posture, Muscle Activity and Sitting Balance During Tooth Preparation. Int. Dent. J. 2021, 71, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (baua). Körperzwangshaltung Art der Gefährdungen und ihre Wirkungen. Available online: https://www.baua.de/DE/Themen/Arbeitsgestaltung-im-Betrieb/Gefaehrdungsbeurteilung/Expertenwissen/Physische-Belastung/Zwangshaltung/Zwangshaltung_dossier.html?pos=1 (accessed on 11 June 2023).
- Bud, M.; Jitaru, S.; Lucaciu, O.; Korkut, B.; Dumitrascu-Timis, L.; Ionescu, C.; Cimpean, S.; Delean, A. The advantages of the dental operative microscope in restorative dentistry. Med. Pharm. Rep. 2020, 94, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Plessas, A.; Delgado, M.B. The role of ergonomic saddle seats and magnification loupes in the prevention of musculoskeletal disorders. A systematic review. Int. J. Dent. Hyg. 2018, 16, 430–440. [Google Scholar] [CrossRef]
- Rafeemanesh, E.; Jafari, Z.; Kashani, F.O.; Rahimpour, F. A study on job postures and musculoskeletal illnesses in dentists. Int. J. Occup. Med. Environ. Health 2013, 26, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Thacker, H.; Yasobant, S.; Viramgami, A.; Saha, S. Prevalence and determinants of (work-related) musculoskeletal disorders among dentists—A cross sectional evaluative study. Indian J. Dent. Res. 2023, 34, 24. [Google Scholar] [CrossRef] [PubMed]
- Eyvazlou, M.; Asghari, A.; Mokarami, H.; Hosseinabadi, M.B.; Jazari, M.D.; Gharibi, V. Musculoskeletal disorders and selecting an appropriate tool for ergonomic risk assessment in the dental profession. Work 2021, 68, 1239–1248. [Google Scholar] [CrossRef]
- Holzgreve, F.; Fraeulin, L.; Maurer-Grubinger, C.; Betz, W.; Erbe, C.; Weis, T.; Janssen, K.; Schulte, L.; de Boer, A.; Nienhaus, A.; et al. Effects of Resistance Training as a Behavioural Preventive Measure on Musculoskeletal Complaints, Maximum Strength and Ergonomic Risk in Dentists and Dental Assistants. Sensors 2022, 22, 8069. [Google Scholar] [CrossRef]
- Valentim, D.P.; Sato, T.d.O.; Comper, M.L.C.; da Silva, A.M.; Boas, C.V.; Padula, R.S. Reliability, Construct Validity and Interpretability of the Brazilian version of the Rapid Upper Limb Assessment (RULA) and Strain Index (SI). Braz. J. Phys. Ther. 2017, 22, 198–204. [Google Scholar] [CrossRef]
- Kee, D. Comparison of LEBA and RULA Based on Postural Load Criteria and Epidemiological Data on Musculoskeletal Disorders. Int. J. Environ. Res. Public Health 2022, 19, 3967. [Google Scholar] [CrossRef] [PubMed]
- Kee, D. Systematic Comparison of OWAS, RULA, and REBA Based on a Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 595. [Google Scholar] [CrossRef] [PubMed]
- Yazdanirad, S.; Khoshakhlagh, A.H.; Habibi, E.; Zare, A.; Zeinodini, M.; Dehghani, F. Comparing the Effectiveness of Three Ergonomic Risk Assessment Methods-RULA, LUBA, and NERPA-to Predict the Upper Extremity Musculoskeletal Disorders. Indian J. Occup. Environ. Med. 2018, 22, 17–21. [Google Scholar] [PubMed]
- Huang, C.; Kim, W.; Zhang, Y.; Xiong, S. Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace. Int. J. Environ. Res. Public Health 2020, 17, 6050. [Google Scholar] [CrossRef]
- Rodrigues, M.S.; Leite, R.D.V.; Lelis, C.M.; Chaves, T.C. Differences in ergonomic and workstation factors between computer office workers with and without reported musculoskeletal pain. Work 2017, 57, 563–572. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Dentist | Dental Assistant |
|---|---|---|
| Gender | ||
| Male | 8 | 1 |
| Female | 7 | 14 |
| Age (years) | 32.7 ± 4.3 [22.91; 42.42] | 27.4 ± 6.1 [13.33; 41.33] |
| Height (cm) | 176.6 ± 8.9 [156.23; 196.97] | 170.8 ± 6.7 [155.36; 186.24] |
| Weight (kg) | 72.1 ± 11.9 [44.88; 99.25] | 69.3 ± 8.4 [49.65; 88.85] |
| Worksheet Steps | Parameters | Modifications of the RULA Parameters |
|---|---|---|
| Step 1 | Raise shoulder Abduction of the upper arm Resting/leaning on the forearm | The IMC system calculates the elevation of the shoulder girdle; if the angle was >5°, then +1 was added to the “Upper Arm Position” [39]. For an angle > 45°, +1 was added to the “Upper Arm Position” [37]. As there is generally no support for the arms during dental work, the value was set to 0 across the board [37]. |
| Step 3 | Lateral hand bend | For a radial deviation > 10° or an ulnar deviation < −10°, +1 was added to the “Wrist Score” [37]. |
| Step 4 | Turning the forearm or hand | For twists in the neutral range between 45° and −45°, +1 was added to the “Wrist Twist Score”; for twists in the final range of movement between 90° and 45° or between −45° and −90°, +2 was added [39]. |
| Step 6 | Muscle use with “Wrist & Arm Score” | For static or repetitive muscle work, +1 was added. Static muscle work: calculation of the intervals based on the angular velocities (ω) of the shoulder joint that define static/dynamic movements. The static movement started when ω < 5°/s and ended when ω ≥ 10°/s or the angular difference was ≥ 7.5° and duration > 10 s. The sagittal and frontal movements of the shoulder joint were taken into account. In addition, no support of the arm was permitted; the centre of the wrist had to be above L5. Repetitive muscle work: calculation of the mean power frequency (MPF) taking into account the wrist movement (extension/flexion) and forearm rotation (wrist and elbow rotation). For the MPF of a joint > 0.5 Hz, +1 was added. |
| Step 7 + 14 | Force or load for “Wrist & Arm Score” (Step 7) and “Neck, Trunk, Leg Score” (Step 14) | Since all dental instruments weigh less than 2 kg, the value was set to 0 across the board. |
| Step 9 | Neck rotation and neck tilt to the side (frontal plane) | For a rotation or inclination > 10° or <−10°, a value of +1 was added to the “Neck Score” [37]. |
| Step 10 | Upper body rotation and upper body tilt (frontal plane) | For a rotation or inclination > 10° or <−10°, a value of +1 was added to the “Trunk Score” [37]. |
| Step 11 | Leg position | As the test subject’s legs and feet were permanently supported and balanced by their activity, a value of +1 was awarded across the board. |
| Step 13 | Muscle use for “Neck, Trunk, Leg Score” | For static or repetitive muscle work, +1 was added. Static muscle work: analogous to “Step 6”, on the basis of angular velocities (ω) of the neck/cervical spine and lower back/lumbar spine with the condition that all three degrees of freedom of the cervical spine or lumbar spine had to be <5°/s. Repetitive muscle work: analogous to “Step 6”, taking into account all three degrees of freedom of the cervical spine and lumbar spine. For an MPF > 0.5 Hz of a joint, in one of the three degrees of freedom, +1 was added. |
| Body Part (Maximum RULA Score) | Quadrant 1 | Quadrant 2 | Quadrant 3 | Quadrant 4 | ||||
|---|---|---|---|---|---|---|---|---|
| RULA Score (IQR) | Rel. av. RST (IQR) | RULA Score (IQR) | Rel. av. RST (IQR) | RULA Score (IQR) | Rel. av. RST (IQR) | RULA Score (IQR) | Rel. av. RST (IQR) | |
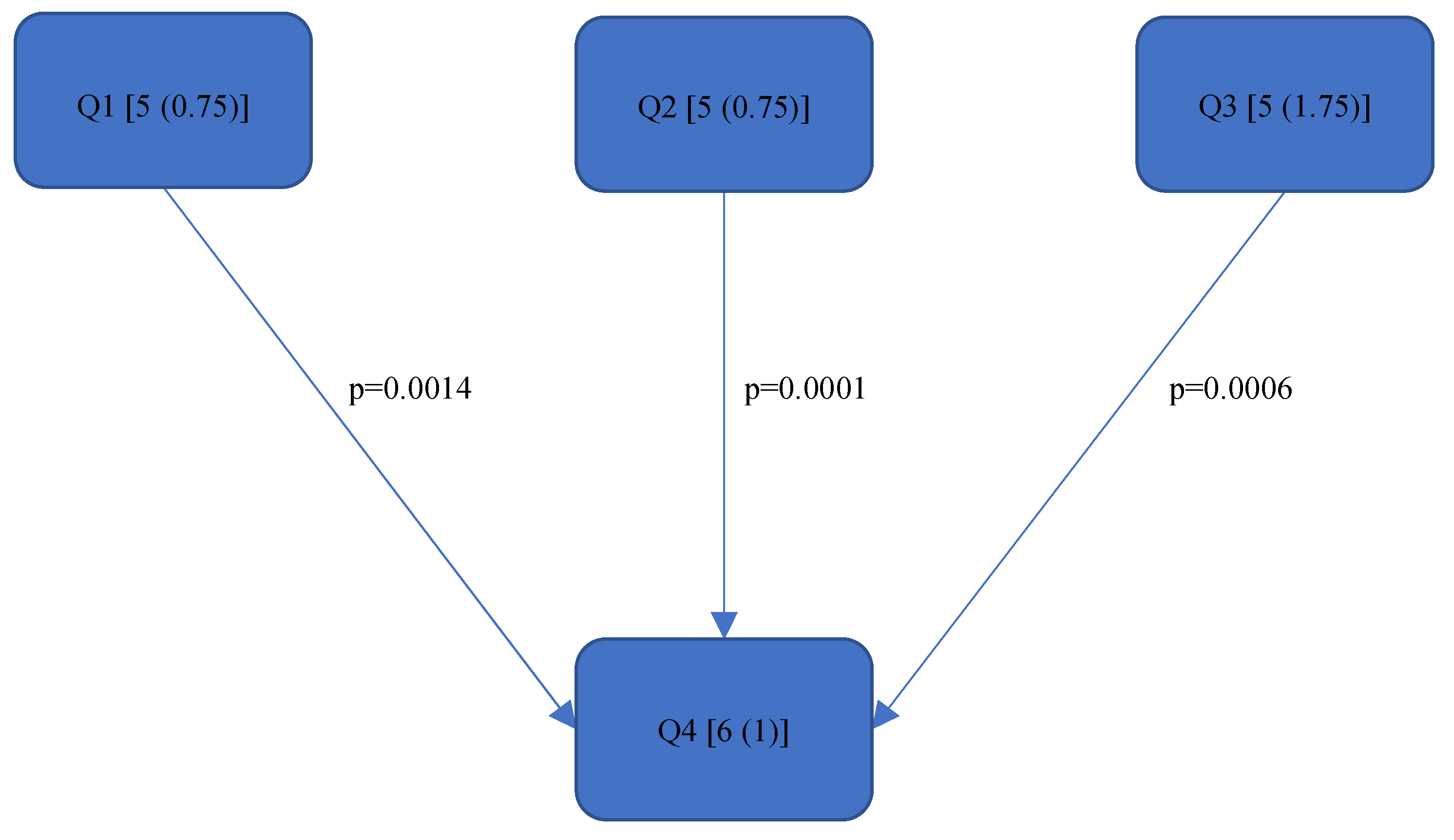
| Final overall (7) | 5 (0.75) | 5.07 (0.69) | 5 (0.75) | 5.05 (0.65) | 5 (1.75) | 5.05 (0.75) | 6 (1) | 5.31 (0.57) |
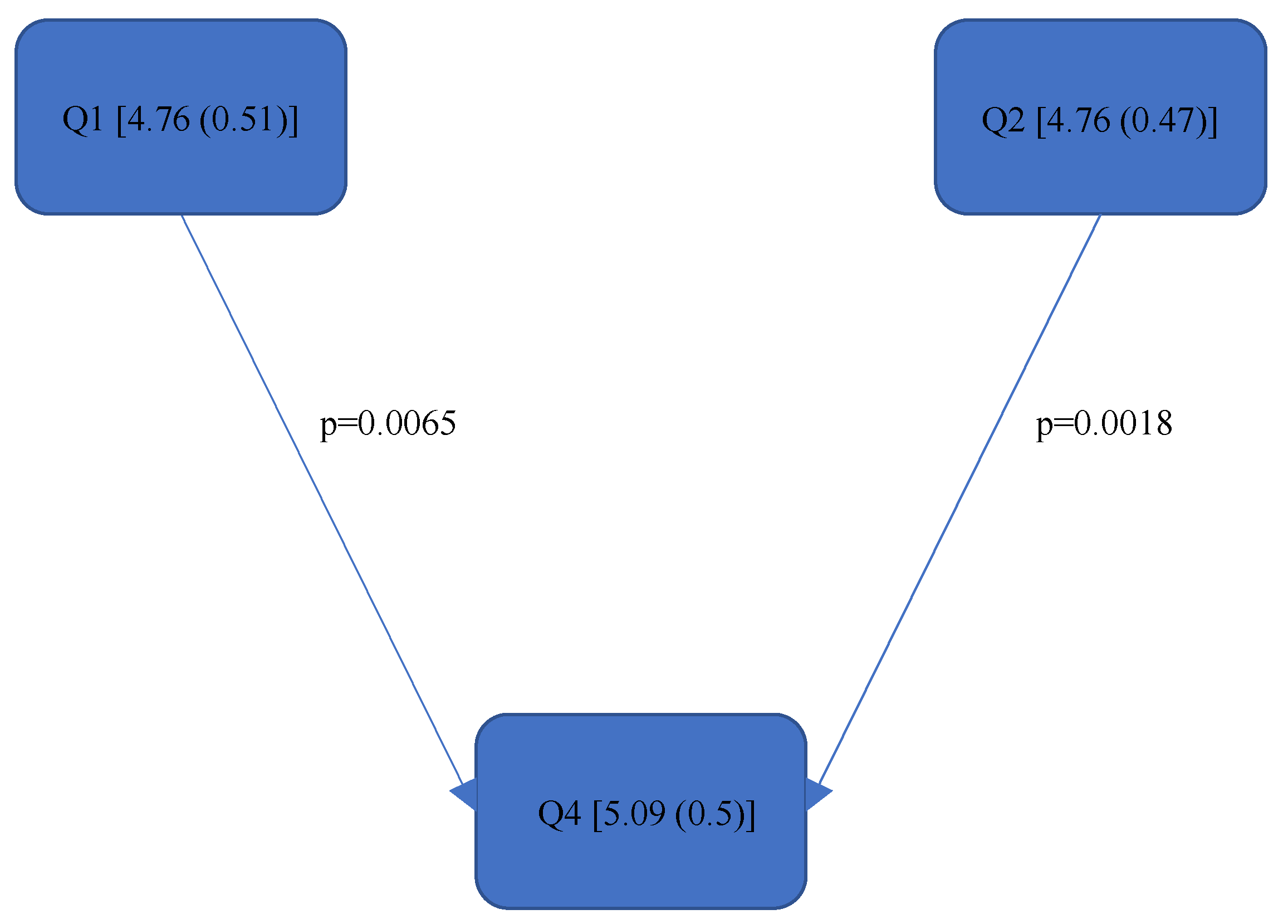
| Final overall right (7) | 5 (1) | 4.76 (0.51) | 5 (1) | 4.76 (0.47) | 5 (1.25) | 4.84 (0.61) | 5 (1) | 5.09 (0.50) |
| Final overall left (7) | 5 (1) | 4.86 (0.78) | 5 (1) | 4.83 (0.76) | 5 (1) | 4.84 (0.80) | 5 (1.50) | 5.06 (0.56) |
| Left Upper Arm—Step 1 (6) | 1 (1) | 1.57 (0.43) | 1.50 (1) | 1,60 (0.54) | 2 (1) | 1.69 (0.35) | 2 (1) | 1.55 (0.40) |
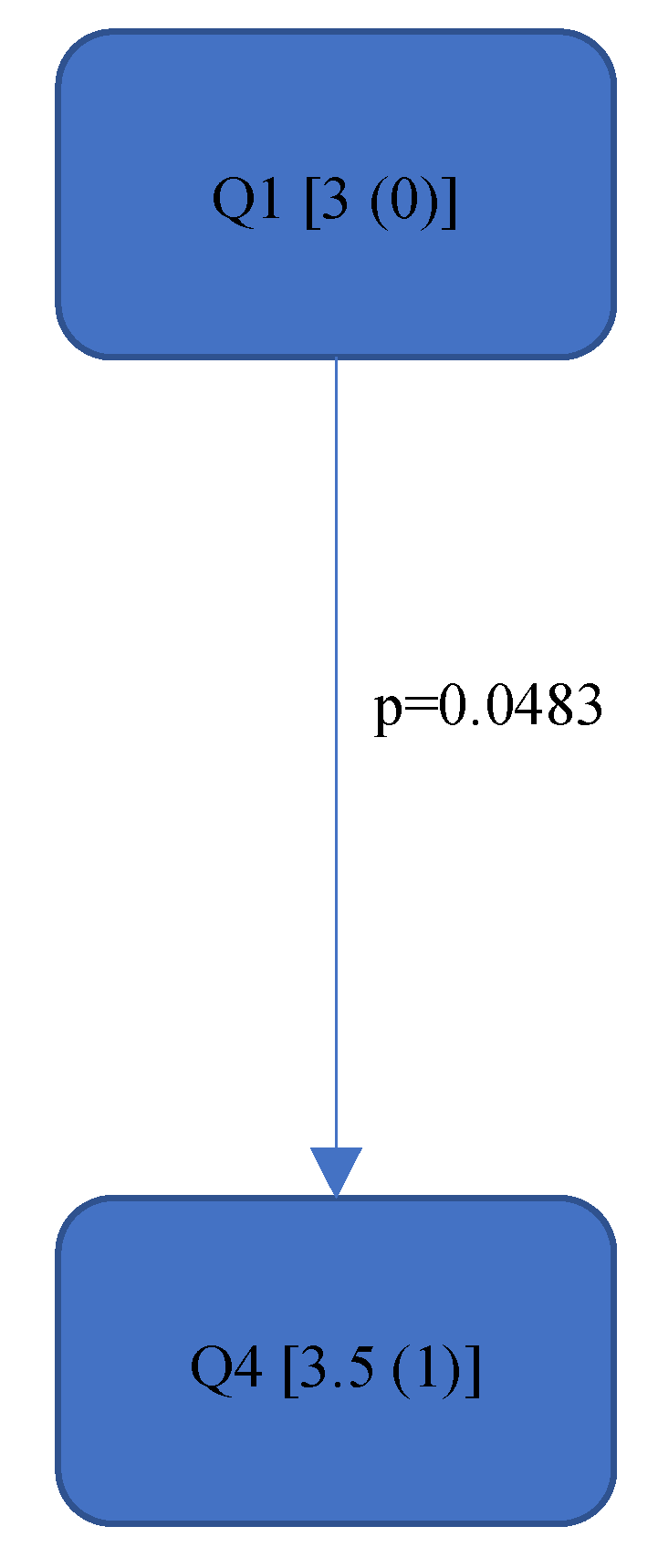
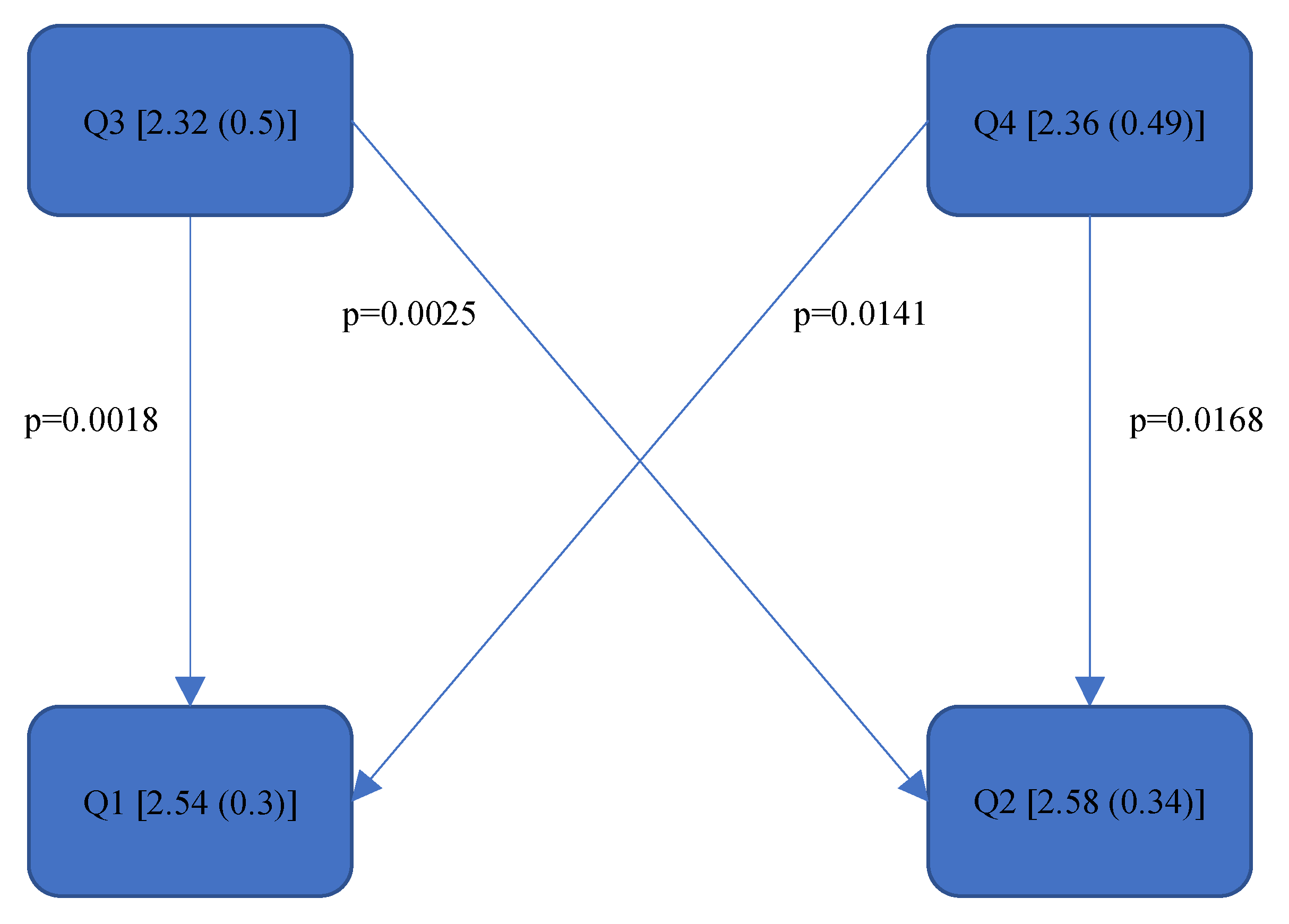
| Left Lower Arm—Step 2 (3) | 3 (0.75) | 2.54 (0.30) | 3 (0.50) | 2.58 (0.34) | 2 (1) | 2.32 (0.50) | 2 (1) | 2.36 (0.49) |
| Left Wrist—Steps 3 + 4 (6) | 4 (1) | 4.23 (0.44) | 4 (0.50) | 4.27 (0.26) | 4 (0) | 4.25 (0.25) | 4.5 (1) | 4.45 (0.30) |
| Right Upper Arm—Step 1 (6) | 2 (0.25) | 1.97 (0.47) | 2 (0) | 1.96 (0.33) | 2 (0) | 2.07 (0.39) | 2 (0.25) | 2.17 (0.52) |
| Right Lower Arm—Step 2 (3) | 2 (0) | 2.24 (0.20) | 2 (0) | 2.21 (0.30) | 2 (0) | 2.34 (0.14) | 2 (0) | 2.34 (0.12) |
| Right Wrist—Steps 3 + 4 (6) | 4 (0.25) | 4.09 (0.42) | 4 (0) | 4.14 (0.17) | 4 (0) | 4.21 (0.32) | 4 (0) | 4.02 (0.38) |
| Neck—Step 9 (6) | 3 (0) | 3.36 (0.31) | 3 (0.25) | 3.45 (0.29) | 3 (0.50) | 3.45 (0.42) | 3.50 (1) | 3.55 (0.43) |
| Trunk—Step 10 (6) | 2 (1) | 2.42 (0.81) | 2 (1) | 2.41 (0.95) | 2 (1) | 2.45 (0.76) | 2 (1) | 2.49 (0.75) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feige, S.; Holzgreve, F.; Fraeulin, L.; Maurer-Grubinger, C.; Betz, W.; Erbe, C.; Nienhaus, A.; Groneberg, D.A.; Ohlendorf, D. Ergonomic Analysis of Dental Work in Different Oral Quadrants: A Motion Capture Preliminary Study among Endodontists. Bioengineering 2024, 11, 400. https://doi.org/10.3390/bioengineering11040400
Feige S, Holzgreve F, Fraeulin L, Maurer-Grubinger C, Betz W, Erbe C, Nienhaus A, Groneberg DA, Ohlendorf D. Ergonomic Analysis of Dental Work in Different Oral Quadrants: A Motion Capture Preliminary Study among Endodontists. Bioengineering. 2024; 11(4):400. https://doi.org/10.3390/bioengineering11040400
Chicago/Turabian StyleFeige, Sophie, Fabian Holzgreve, Laura Fraeulin, Christian Maurer-Grubinger, Werner Betz, Christina Erbe, Albert Nienhaus, David A. Groneberg, and Daniela Ohlendorf. 2024. "Ergonomic Analysis of Dental Work in Different Oral Quadrants: A Motion Capture Preliminary Study among Endodontists" Bioengineering 11, no. 4: 400. https://doi.org/10.3390/bioengineering11040400