Evaluation of in Vivo Response of Three Biphasic Scaffolds for Osteochondral Tissue Regeneration in a Sheep Model

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scaffold Design and Realization
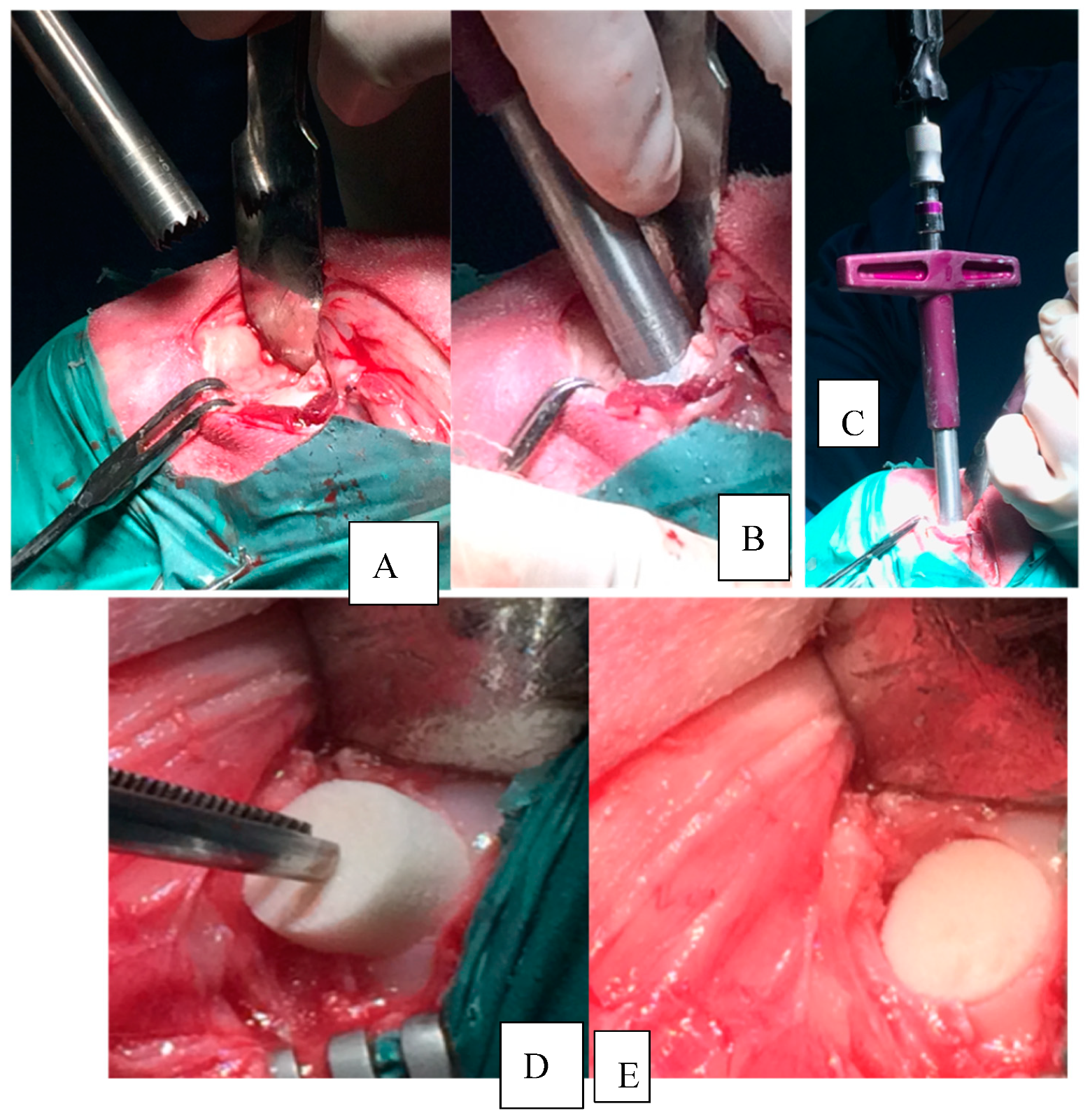
2.2. Management of the Animals and Surgical Procedures
2.3. Protocol of the Study
2.4. CT Evaluation
2.5. Macroscopic Evaluation
3. Results
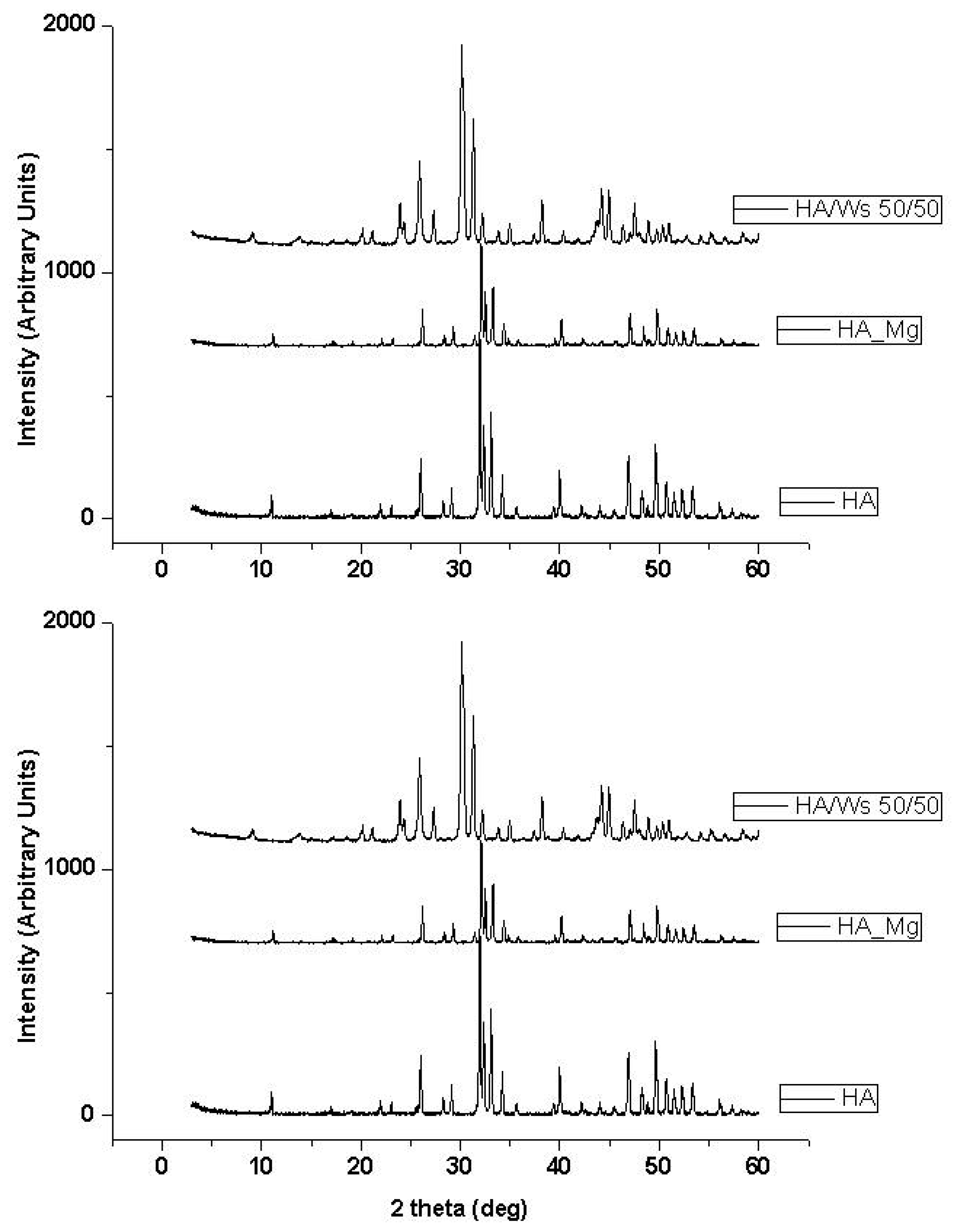
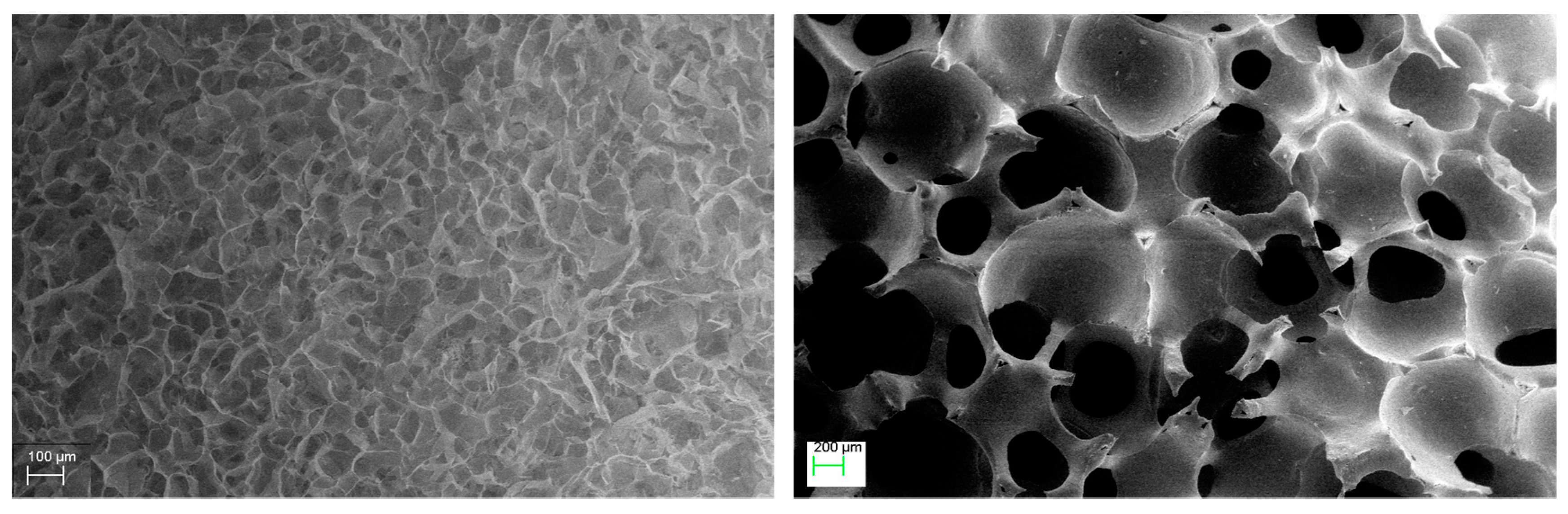
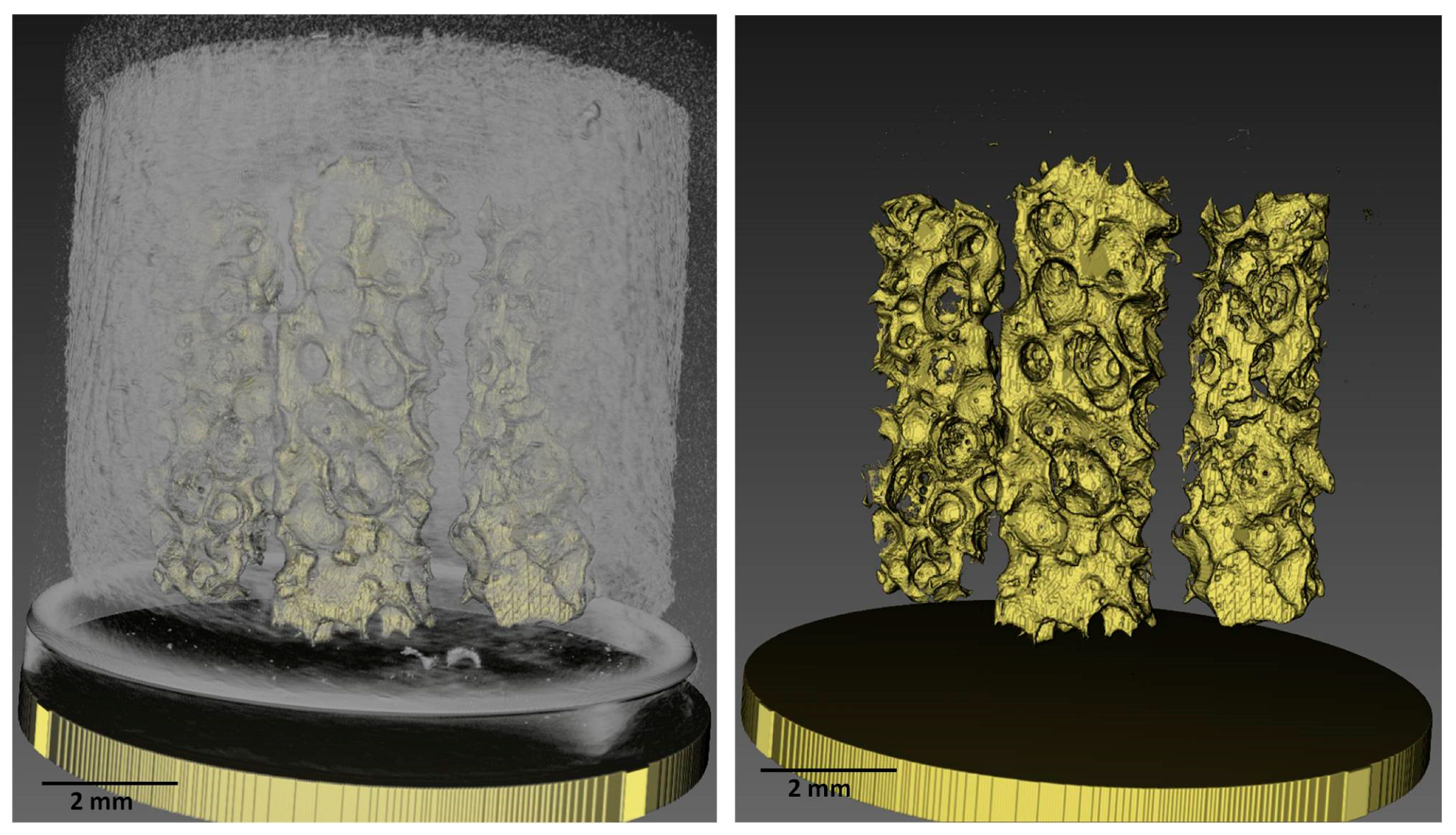
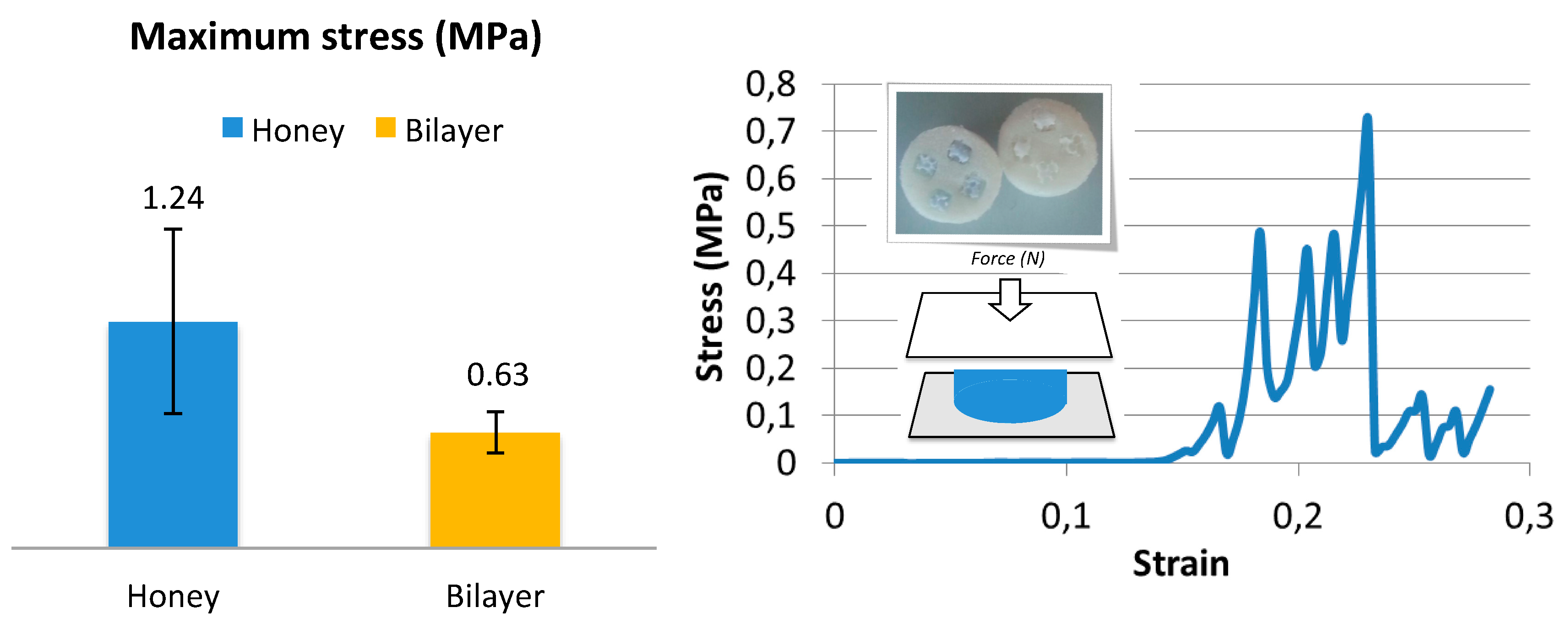
3.1. Pre-Implant Osteochondral Scaffolds Characterization
3.2. In Vivo Results
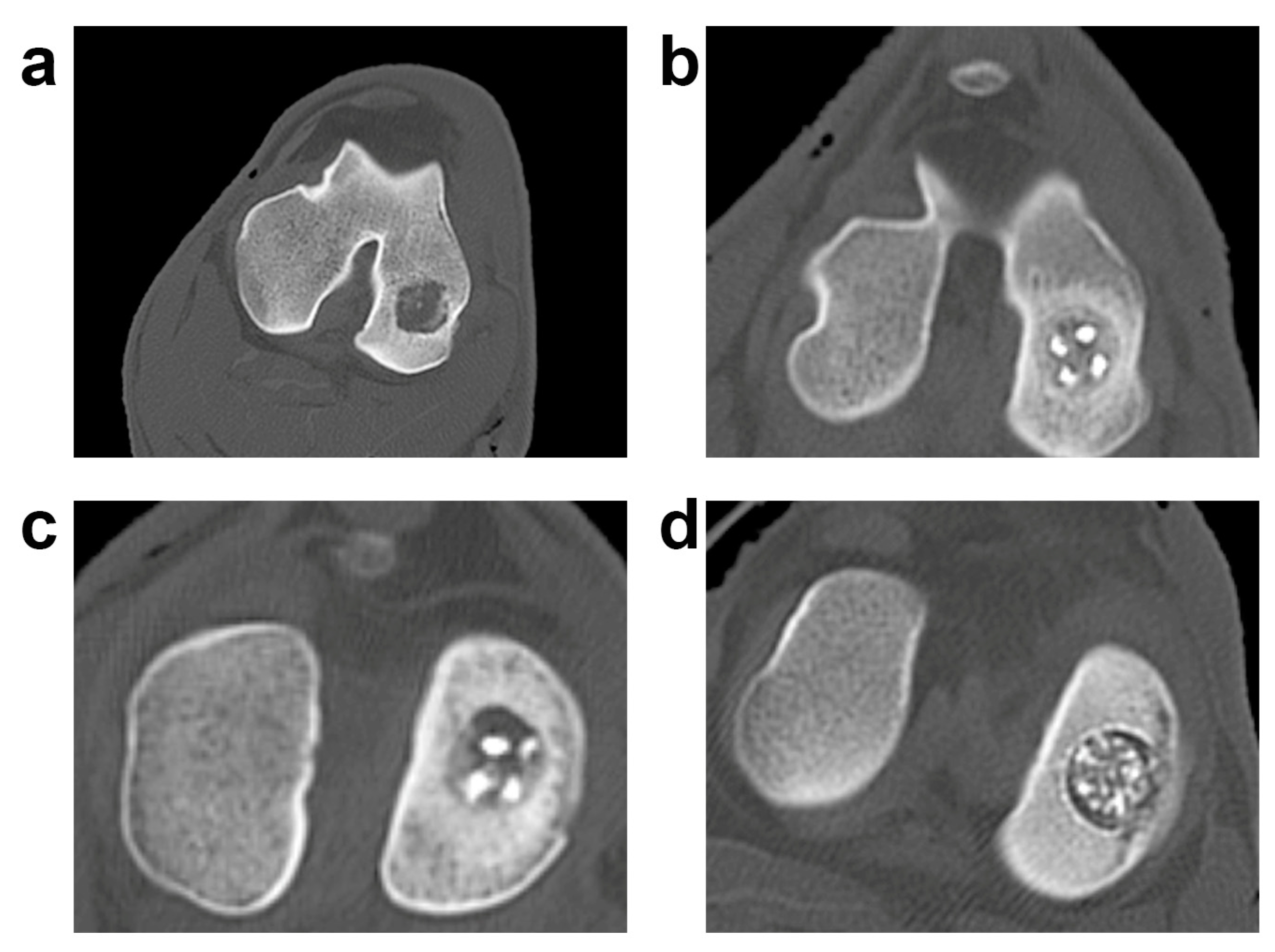
3.3. Radiological Evaluation
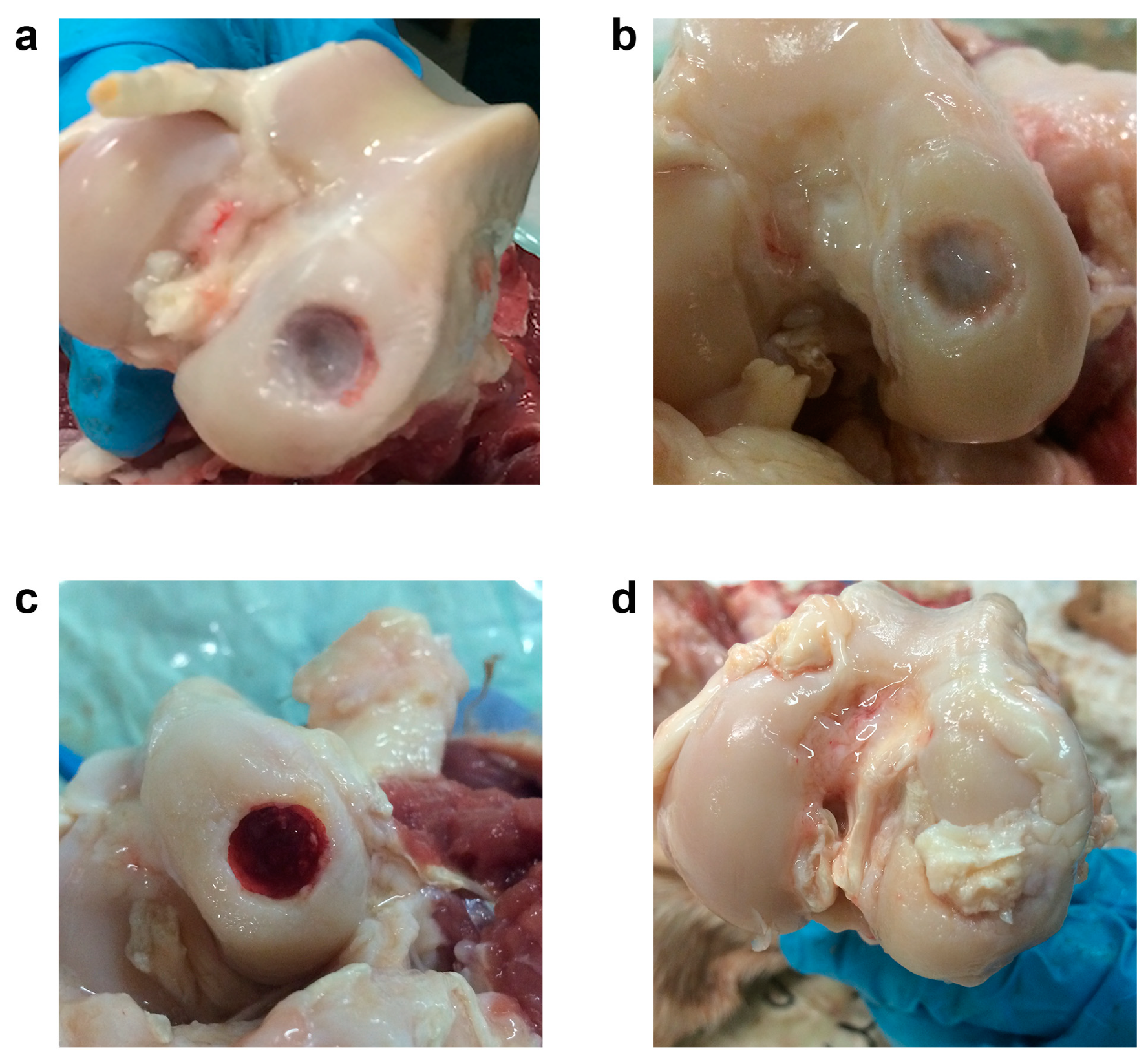
3.4. Macroscopic Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Madry, H.; van Dijk, C.N.; Mueller-Gerbl, M. The basic science of the subchondral bone. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 419–433. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhou, X.; Li, W.; Novotny, J.E.; Doty, S.B.; Wang, L. In situ measurement of transport between subchondral bone and articular cartilage. J. Orthop. Res. 2009, 27, 1347–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijlsma, J.W.; Berenbaum, F.; Lafeber, F.P. Osteoarthritis: An update with relevance for clinical practice. Lancet 2011, 377, 2115–2126. [Google Scholar] [CrossRef]
- Ding, D.C.; Chang, Y.H.; Shyu, W.C.; Lin, S.Z. Human umbilical cord mesenchymal stem cells: A new era for stem cell therapy. Cell Transplant. 2015, 24, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Lories, R.J.; Luyten, F.P. The bone-cartilage unit in osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 43–49. [Google Scholar] [CrossRef]
- Sellam, J.; Berenbaum, F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat. Rev. Rheumatol. 2010, 6, 625–635. [Google Scholar] [CrossRef]
- Pape, D.; Filardo, G.; Kon, E.; van Dijk, C.N.; Madry, H. Disease-specific clinical problems associated with the subchondral bone. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 448–462. [Google Scholar] [CrossRef]
- Intema, F.; Hazewinkel, H.A.W.; Gouwens, D.; Bijlsma, J.W.J.; Weinans, H.; Lafeber, F.P.J.G.; Mastbergen, S.C. In early OA, thinning of the subchondral plate is directly related to cartilage damage: Results from a canine ACLT-meniscectomy model. Osteoarthr. Cartil. 2010, 18, 691–698. [Google Scholar] [CrossRef]
- Verdonk, R.; Madry, H.; Shabshin, N.; Dirisamer, F.; Peretti, G.M.; Pujol, N.; Spalding, T.; Verdonk, P.; Seil, R.; Condello, V.; et al. Early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1753–1762. [Google Scholar]
- Peretti, G.M.; Tessaro, I.; Montanari, L.; Polito, U.; Di, A.G.; Di, M.G.; Marmotti, A.; Montaruli, A.; Roveda, E.; Mangiavini, L. Histological changes of the meniscus following an osteochondral lesion. J. Biol. Regul. Homeost. Agents 2017, 31, 129–134. [Google Scholar]
- Peretti, G.M.; Pozzi, A.; Ballis, R.; Deponti, D.; Pellacci, F. Current surgical options for articular cartilage repair. Acta Neurochir. Suppl. 2011, 108, 213–219. [Google Scholar] [PubMed]
- Tessaro, I.; Nguyen, V.T.; Di, G.A.; Agnoletto, M.; Verdoni, F.; Domenicucci, M.; Scurati, R.; Peretti, G.M.; Mangiavini, L. Animal models for cartilage repair. J. Biol. Regul. Homeost. Agents 2018, 32, 105–116. [Google Scholar] [PubMed]
- Marmotti, A.; Bruzzone, M.; Bonasia, D.E.; Castoldi, F.; Rossi, R.; Piras, L.; Maiello, A.; Realmuto, C.; Peretti, G.M. One-step osteochondral repair with cartilage fragments in a composite scaffold. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2590–2601. [Google Scholar] [CrossRef] [PubMed]
- Marmotti, A.; Bruzzone, M.; Bonasia, D.E.; Castoldi, F.; Von Degerfeld, M.M.; Bignardi, C.; Mattia, S.; Maiello, A.; Rossi, R.; Peretti, G.M. Autologous cartilage fragments in a composite scaffold for one stage osteochondral repair in a goat model. Eur. Cell Mater. 2013, 26, 15–31. [Google Scholar] [CrossRef]
- Scotti, C.; Buragas, M.S.; Mangiavini, L.; Sosio, C.; Di Giancamillo, A.; Domeneghini, C.; Fraschini, G.; Peretti, G.M. A tissue engineered osteochondral plug: An in vitro morphological evaluation. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 1363–1369. [Google Scholar] [CrossRef]
- Fisher, J.N.; Tessaro, I.; Bertocco, T.; Peretti, G.M.; Mangiavini, L. The Application of Stem Cells from Different Tissues to Cartilage Repair. Stem Cells Int. 2017, 2017, 2761678. [Google Scholar] [CrossRef]
- Hunziker, E.B. Articular cartilage repair: Basic science and clinical progress. A review of the current status and prospects. Osteoarthr. Cartil. 2002, 10, 432–463. [Google Scholar] [CrossRef]
- Emmerson, B.C.; Görtz, S.; Jamali, A.A.; Chung, C.; Amiel, D.; Bugbee, W.D. Fresh osteochondral allografting in the treatment of osteochondritis dissecans of the femoral condyle. Am. J. Sports Med. 2007, 35, 907–914. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Perdisa, F.; Balboni, F.; Marcacci, M. Autologous osteochondral transplantation for the treatment of knee lesions: Results and limitations at two years’ follow-up. Int. Orthop. 2014, 38, 1905–1912. [Google Scholar] [CrossRef]
- Gross, A.E.; Kim, W.; Las Heras, F.; Backstein, D.; Safir, O.; Pritzker, K.P.H. Fresh osteochondral allografts for posttraumatic knee defects: Long-term followup. Clin. Orthop. Relat. Res. 2008, 466, 1863–1870. [Google Scholar] [CrossRef]
- Hangody, L.; Fules, P. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: Ten years of experimental and clinical experience. J. Bone Jt. Surg. Am. 2003, 85, 25–32. [Google Scholar] [CrossRef]
- Gobbi, A.; Scotti, C.; Lane, J.G.; Peretti, G.M. Fresh osteochondral allografts in the knee: Only a salvage procedure? Ann. Transl. Med. 2015, 3, 164. [Google Scholar] [PubMed]
- Izadifar, Z.; Chen, X.; Kulyk, W. Strategic design and fabrication of engineered scaffolds for articular cartilage repair. J. Funct. Biomater. 2012, 3, 799–838. [Google Scholar] [CrossRef] [PubMed]
- Longley, R.; Ferreira, A.M.; Gentile, P. Recent Approaches to the Manufacturing of Biomimetic Multi-Phasic Scaffolds for Osteochondral Regeneration. Int. J. Mol. Sci. 2018, 19, 1755. [Google Scholar] [CrossRef] [PubMed]
- Maia, F.R.; Carvalho, M.R.; Oliveira, J.M.; Reis, R.L. Tissue Engineering Strategies for Osteochondral Repair. Adv. Exp. Med. Biol. 2018, 1059, 353–371. [Google Scholar] [PubMed]
- Ansari, S.; Khorshidi, S.; Karkhaneh, A. Engineering of gradient osteochondral tissue: From nature to lab. Acta Biomater. 2019, 87, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, B.; Scalera, F.; Soloperto, G.T.; Scialla, S.; Gervaso, F. Recent Strategies in Osteochondral Substitutes Design: Towards the Mimicking of a Multifaceted Anatomical Unit from the Nano to the Macro Level. J. Nanomed. Nanotechnol. 2017, 8, 2. [Google Scholar]
- Mow, V.C.; Ratcliffe, A.; Poole, A.R. Cartilage and diarthrodial joints as paradigms for hierarchical materials and structures. Biomaterials 1992, 13, 67–97. [Google Scholar] [CrossRef]
- Gervaso, F.; Scalera, F.; Kunjalukkal Padmanabhan, S.; Sannino, A.; Licciulli, A. High performance hydroxyapatite scaffolds for bone tissue engineering applications. Int. J. Appl. Ceram. Technol. 2012, 9, 507–516. [Google Scholar] [CrossRef]
- Kunjalukkal Padmanabhan, S.; Gervaso, C.M.; Scalera, F.; Sannino, F.; Licciulli, A. Mechanical performance and in vitro studies of hydroxyapatite/wollastonite scaffold for bone tissue engineering. Key Eng. Mater. 2011, 855, 493–494. [Google Scholar]
- Gervaso, F.; Scalera, F.; Padmanabhan, S.K.; Licciulli, A.; Deponti, D.; Di Giancamillo, A.; Domeneghini, C.; Peretti, G.; Sannino, A. Development and Mechanical Characterization of a Collagen/Hydroxyapatite Bilayered Scaffold for Ostechondral Defect Replacement. Key Eng. Mater. 2012, 493, 890–895. [Google Scholar] [CrossRef]
- Padmanabhan, S.K.; Gervaso, F.; Carrozzo, M.; Scalera, F.; Sannino, A.; Licciulli, A. Wollastonite/hydroxyapatite scaffolds with improved mechanical, bioactive and biodegradable properties for bone tissue engineering. Ceram. Int. 2013, 39, 619–627. [Google Scholar] [CrossRef]
- Gervaso, F.; Padmanabhan, S.K.; Scalera, F.; Sannino, A.; Licciulli, A. Mechanical stability of highly porous hydroxyapatite scaffolds during different stages of in vitro studies. Mater. Lett. 2016, 185, 239–242. [Google Scholar] [CrossRef]
- Parisi, C.; Gervaso, F.; Scalera, F.; Kunjalukkal, S.; Nobile, C.; Cozzoli, P.D.; Silvio, L.D.; Sannino, A. Influence of the precipitation temperature on properties of nanohydroxyapatite powder for the fabrication of highly porous bone scaffolds. Bioceramics 2014, 25, 587. [Google Scholar] [CrossRef]
- Scalera, F.; Gervaso, F.; Sanosh, K.P.; Sannino, A.; Licciulli, A. Influence of the calcination temperature on morphological and mechanical properties of highly porous hydroxyapatite scaffolds. Ceram. Int. 2013, 39, 4839–4846. [Google Scholar] [CrossRef]
- Sosio, C.; Di Giancamillo, A.; Deponti, D.; Gervaso, F.; Scalera, F.; Melato, M.; Campagnol, M.; Boschetti, F.; Nonis, A.; Domeneghini, C.; et al. Osteochondral repair by a novel interconnecting collagen-hydroxyapatite substitute: A large-animal study. Tissue Eng. Part A 2015, 21, 704–715. [Google Scholar] [CrossRef]
- Deponti, D.; Giancamillo, A.D.; Gervaso, F.; Domenicucci, M.; Domeneghini, C.; Sannino, A.; Peretti, G.M. Collagen scaffold for cartilage tissue engineering: The benefit of fibrin glue and the proper culture time in an infant cartilage model. Tissue Eng. Part A 2014, 20, 1113–1126. [Google Scholar] [CrossRef]
- Gullotta, F.; Izzo, D.; Scalera, F.; Palazzo, B.; Martin, I.; Sannino, A.; Gervaso, F. Biomechanical evaluation of hMSCs-based engineered cartilage for chondral tissue regeneration. J. Mech. Behav. Biomed. Mater. 2018, 86, 294–304. [Google Scholar] [CrossRef]
- Gervaso, F.; Mangiavini, L.; Di, A.G.; Boschetti, F.; Izzo, D.; Zani, D.D.; Di Giancamillo, M.; Tessaro, I.; Domenicucci, M.; Domenicucci, M.; et al. Comparison of three novel biphasic scaffolds for one-stage treatment of osteochondral defects in a sheep model. J. Biol. Regul. Homeost. Agents 2016, 30, 24–31. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Dittler, M.L.; Unalan, I.; Grünewald, A.; Beltrán, A.M.; Grillo, C.A.; Destch, R.; Gonzalez, M.C.; Boccaccini, A.R. Bioactive glass (45S5)-based 3D scaffolds coated with magnesium and zinc-loaded hydroxyapatite nanoparticles for tissue engineering applications. Colloids Surf. B 2019, 182, 110346. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, L.; Niada, S.; Arrigoni, E.; Di Giancamillo, A.; Domeneghini, C.; Dadsetan, M.; Yaszemski, M.J.; Gastaldi, D.; Vena, P.; Taffetani, M.; et al. Repair of osteochondral defects in the minipig model by OPF hydrogel loaded with adipose-derived mesenchymal stem cells. Regen. Med. 2015, 10, 135–151. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Osteochondral Scaffold Sketch | Osteochondral Scaffold Configuration | Sample Name | Scaffold Material | ||
|---|---|---|---|---|---|
| Top View | Side View | Cartilage Scaffold | Bone Scaffold | ||
 |  | Bilayer | BWS | Collagen | Blend WS/HA |
 |  | Honey | HWS | Collagen | Blend WS/HA |
 |  | Honey | HMG | Collagen | Mg-doped HA |
 | |||||
| Voltage (kV) | Current (µA) | Voxel Size (µm3) | Exposure Time (s) | Projections | Scan Time (min) |
|---|---|---|---|---|---|
| 65 | 145 | 12.5 × 12.5 × 12.5 | 1.250 | 1400 | 176 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crovace, A.M.; Giancamillo, A.D.; Gervaso, F.; Mangiavini, L.; Zani, D.; Scalera, F.; Palazzo, B.; Izzo, D.; Agnoletto, M.; Domenicucci, M.; et al. Evaluation of in Vivo Response of Three Biphasic Scaffolds for Osteochondral Tissue Regeneration in a Sheep Model. Vet. Sci. 2019, 6, 90. https://doi.org/10.3390/vetsci6040090
Crovace AM, Giancamillo AD, Gervaso F, Mangiavini L, Zani D, Scalera F, Palazzo B, Izzo D, Agnoletto M, Domenicucci M, et al. Evaluation of in Vivo Response of Three Biphasic Scaffolds for Osteochondral Tissue Regeneration in a Sheep Model. Veterinary Sciences. 2019; 6(4):90. https://doi.org/10.3390/vetsci6040090
Chicago/Turabian StyleCrovace, Alberto M., Alessia Di Giancamillo, Francesca Gervaso, Laura Mangiavini, Davide Zani, Francesca Scalera, Barbara Palazzo, Daniela Izzo, Marco Agnoletto, Marco Domenicucci, and et al. 2019. "Evaluation of in Vivo Response of Three Biphasic Scaffolds for Osteochondral Tissue Regeneration in a Sheep Model" Veterinary Sciences 6, no. 4: 90. https://doi.org/10.3390/vetsci6040090