Delirium Stigma Among Healthcare Staff


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Key Points:
- People with delirium occupy more than one third of acute medical beds and require increased medical attention and treatment.
- Professionals working in communities and medical wards have high levels of stigmatisation of delirium patients.
- Delirium stigmatisation was not related to professionals’ own experiences of delirium, their educational and professional backgrounds, or them having delirium education. However, working closely with people with delirium seems to have a positive impact on the de-stigmatisation of this population among health professionals.
- These findings need to be translated into a meaningful educational intervention with an emphasis placed on direct patient-oriented educational interventions.
1. Introduction
2. Materials and Methods
2.1. Recruitment of Participants
2.2. Assessment Scales
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Participants’ Characteristics
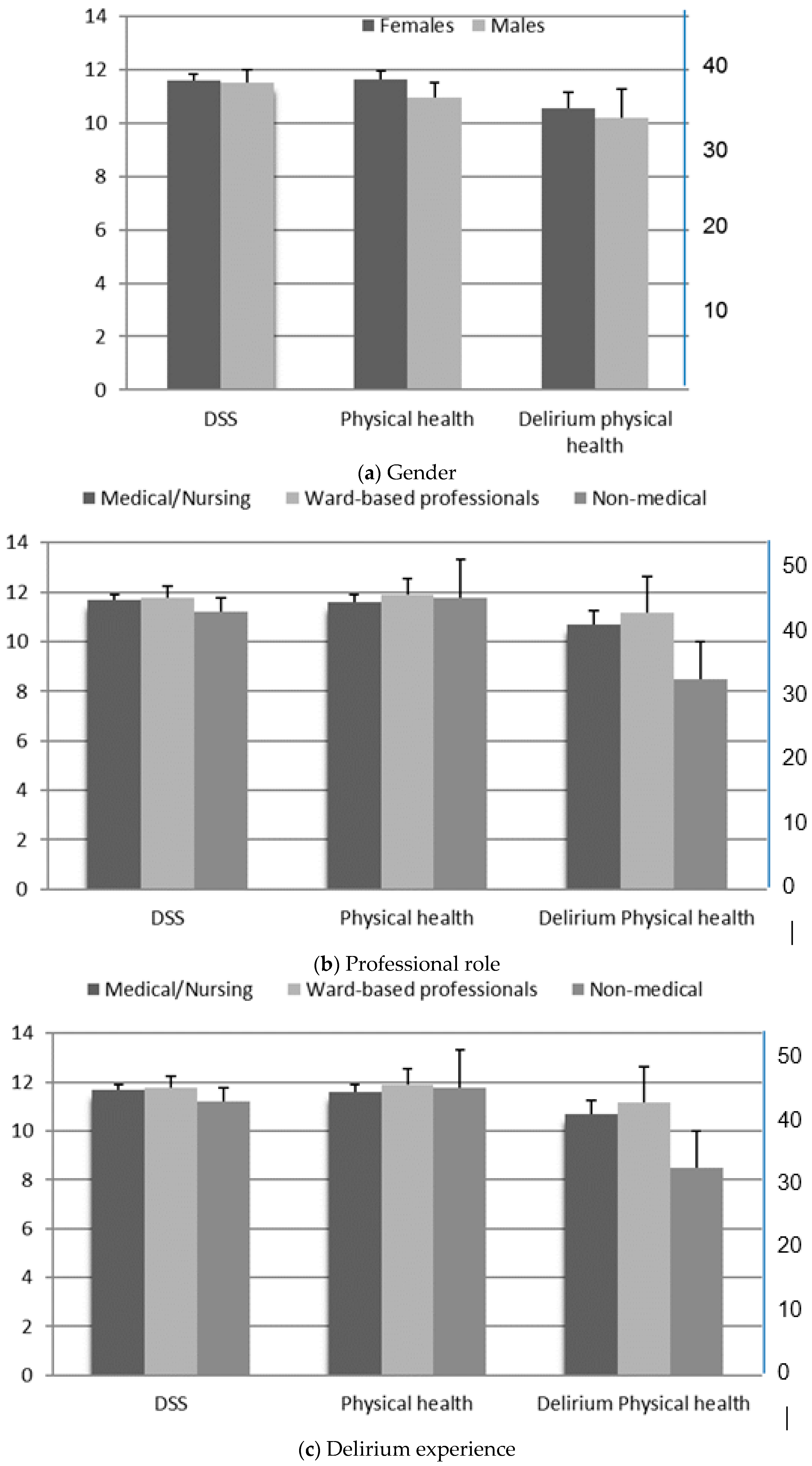
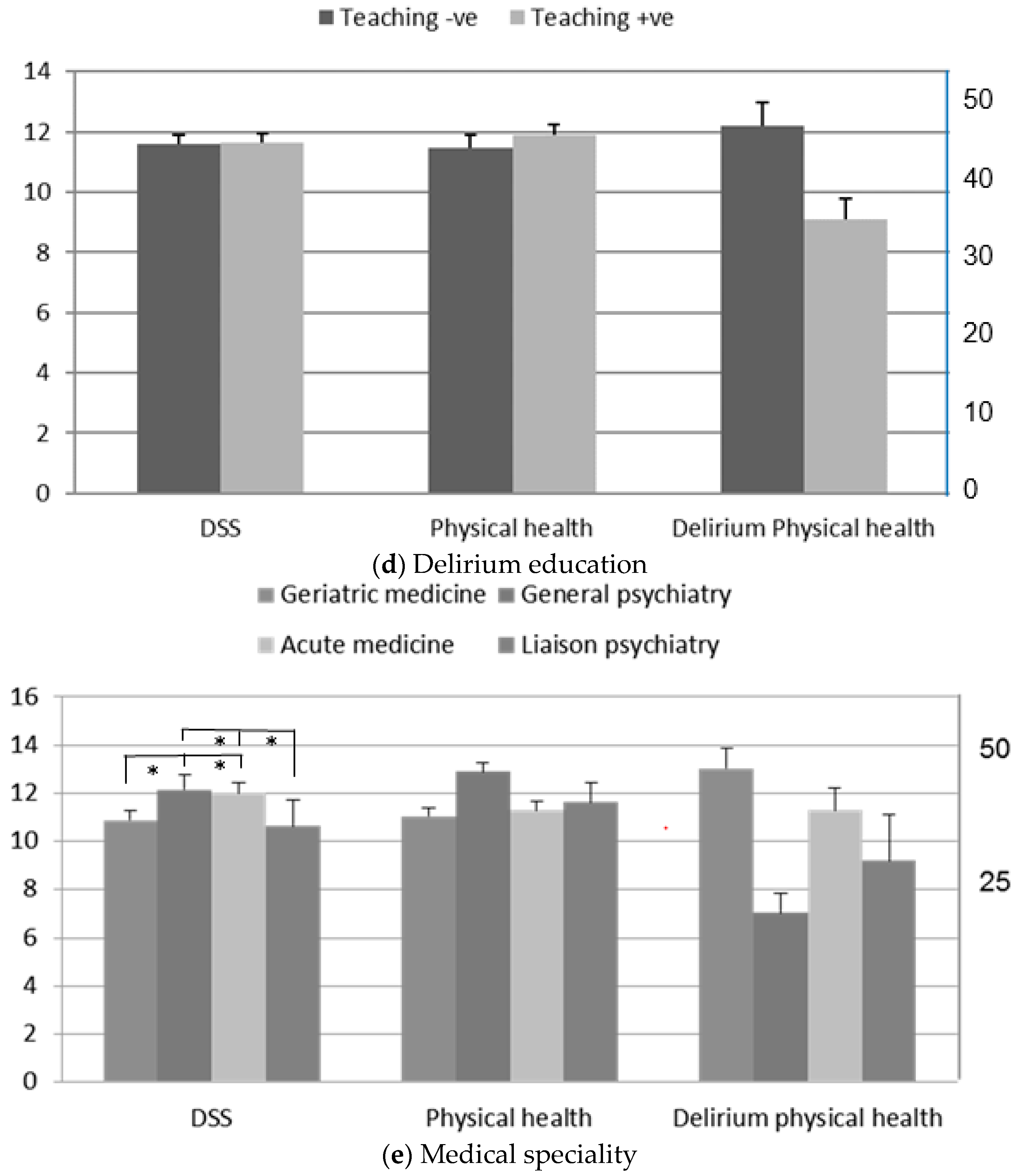
3.2. Delirium Stigma
3.3. Physical Health (EQ-5D-5L Analysis)
3.4. Physical Health with Delirium (EQ-VAS Analysis)
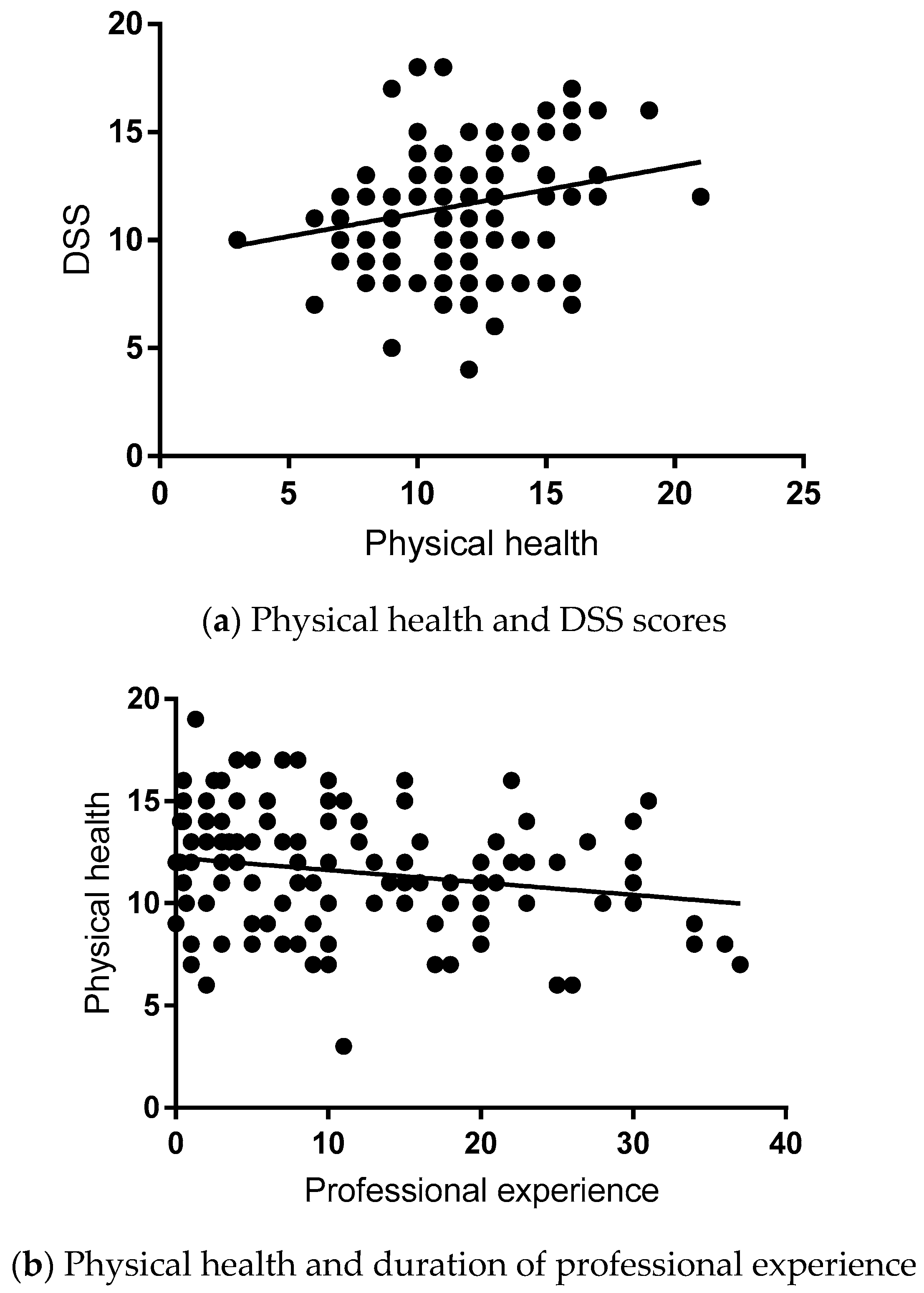
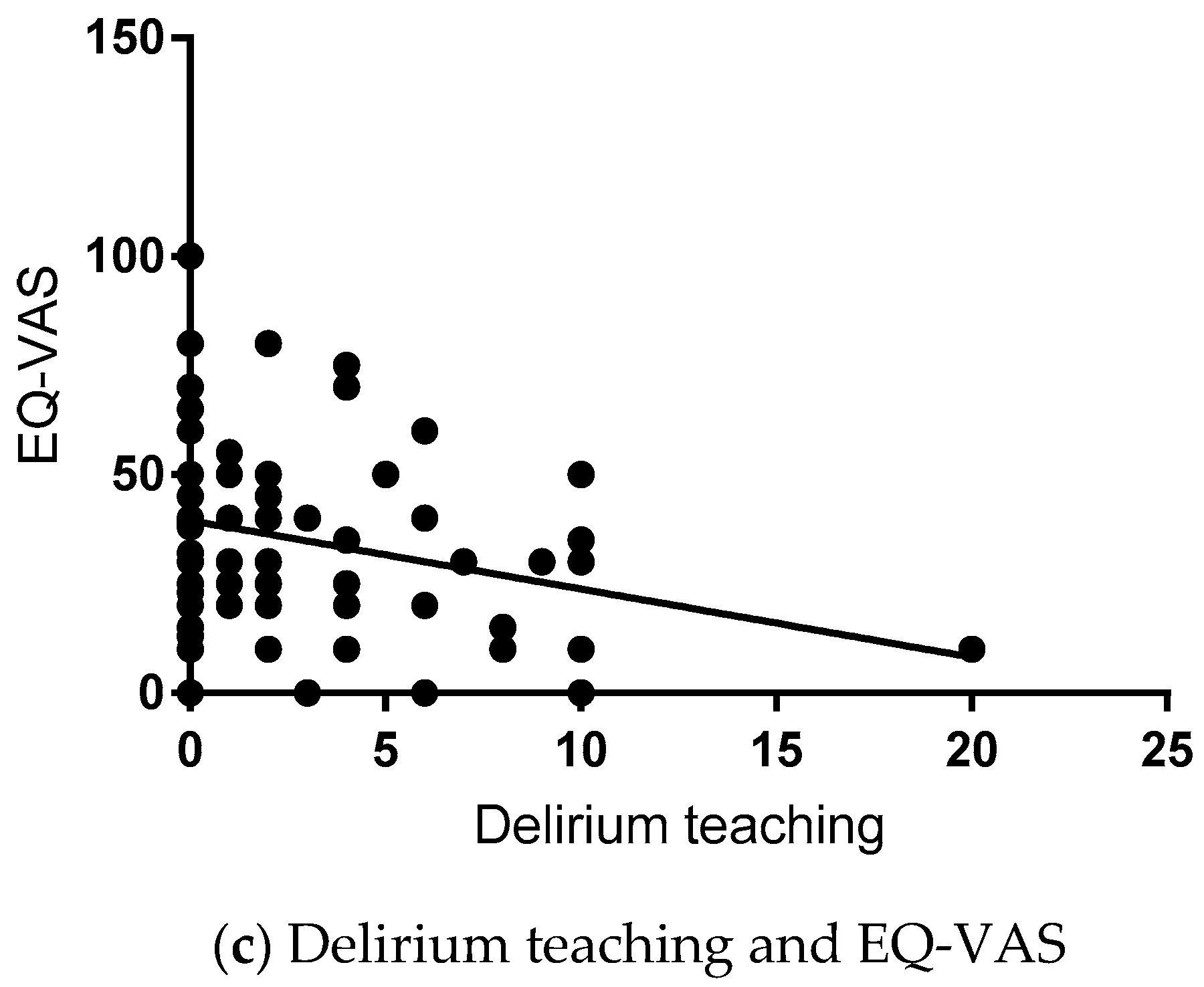
3.5. Correlation Analysis
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Gender (M/F)
- Age ______________ years
- Professional role: ____________________________________________________
- Do you work with people with delirium (Yes/No)
- If yes, duration of your experience ____________ years.
- Have you had a formal training or education on delirium (Yes/No)
- If yes, how many hours in the last 5 years _________ hour
- Have you experienced an episode of delirium? (Yes/No)
- Have you a close relative who had a delirium? (Yes/No)
| 0 | 1 | 2 | 3 |
| Strongly disagree | Disagree | Agree | Strongly agree |
| 1. | ________ | Delirium patients have a sense of alienation from other people following an episode of delirium. |
| 2. | ________ | People with delirium seem to harm people around them. |
| 3. | ________ | People with delirium feel other people are looking at them strangely. |
| 4. | ________ | People with delirium are embarrassed or ashamed that they have experienced delirium. |
| 5. | ________ | People with delirium are nervous that they may have dementia or a mental disorder. |
| 6. | ________ | People with delirium are concerned their delirium could reoccur. |
- People with delirium could not recall the delirium episode
- They could partially recall the delirium episode
- They could totally recall the delirium episode
- They do not have problems in walking about
- They have slight problems in walking about
- They have moderate problems in walking about
- They have severe problems in walking about
- They are unable to walk about
- They do not have problems washing or dressing themselves
- They have slight problems washing or dressing themselves
- They have moderate problems washing or dressing themselves
- They have severe problems washing or dressing themselves
- They are unable to wash or dress themselves
- They have no problems doing their usual activities
- They have slight problems doing their usual activities
- They have moderate problems doing their usual activities
- They have severe problems doing their usual activities
- They are unable to do their usual activities
- They have no pain or discomfort
- They have slight pain or discomfort
- They have moderate pain or discomfort
- They have severe pain or discomfort
- They have extreme pain or discomfort
- They are not anxious or depressed
- They are slightly anxious or depressed
- They are moderately anxious or depressed
- They are severely anxious or depressed
- They are extremely anxious or depressed


References
- NICE Clinical Guideline. Delirium: Prevention, Diagnosis and Management. Clinical Guideline [CG103]. July 2010. Available online: https://www.nice.org.uk/Guidance/CG103 (accessed on 6 August 2018).
- Vidal, E.I.; Villas Boas, P.J.; Valle, A.P.; Cerqueira, A.T.; Fukushima, F.B. Delirium in older adults. BMJ 2013, 346, f2031. [Google Scholar] [CrossRef] [PubMed]
- Timmons, S.; O’Shea, E.; O’Neill, D.; Gallagher, P.; de Siún, A.; McArdle, D.; Gibbons, P.; Kennelly, S. Acute hospital dementia care: Results from a national audit. BMC Geriatr. 2016, 16, 113. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.C.; Fisher, T.J.; Greenspan, H.N.; Heinrich, T.W. Pharmacologic and nonpharmacologic approaches to the prevention and management of delirium. Int. J. Psychiatry Med. 2016, 51, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Cerejeira, J.; Firmino, H.; Vaz-Serra, A.; Mukaetova-Ladinska, E.B. The neuroinflammatory hypothesis of delirium. Acta Neuropathol. 2010, 119, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.H.; Kreisel, S.H.; Muniz Terrera, G.; Hall, A.J.; Morandi, A.; Boustani, M.; Neufeld, K.J.; Lee, H.B.; Maclullich, A.M.; Brayne, C. The epidemiology of delirium: Challenges and opportunities for population studies. Am. J. Geriatr. Psychiatry 2013, 21, 1173–1189. [Google Scholar] [CrossRef] [PubMed]
- Teodorczuk, A.; Mukaetova-Ladinska, E.; Corbett, S.; Welfare, M. Reconceptualizing models of delirium education: Findings of a Grounded Theory study. Int. Psychogeriatr. 2013, 25, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Link, B.G.; Phelan, J.C. Conceptualizing stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Corrigan, P.; Druss, B.; Perlick, D. The impact of mental illness stigma on seeking and participating in mental health care. Psychol. Sci. Public Interest 2014, 15, 37–70. [Google Scholar] [CrossRef]
- WHO—WPA (Geneva) 2002: Reducing Stigma and Discrimination against Older People with Mental Disorders. A Technical Consensus Statement. Available online: http://www.wpanet.org/uploads/Sections/Old_Age_Psychiatry/reducing-stigma-discrimination.pdf (accessed on 18 April 2017).
- Livingston, J.D. Mental Illness-Related Structural Stigma: The Downward Spiral of Systemic Exclusion; Mental Health Commission of Canada: Calgary, AB, Canada, 2013; Available online: http://www.mentalhealthcommission.ca (accessed on 14 December 2018).
- Knaak, S.; Mantler, E.; Szeto, A. Mental illness-related stigma in healthcare. Barriers to access and care and evidence-based solutions. Healthc. Manag. Forum 2017, 30, 111–116. [Google Scholar] [CrossRef] [Green Version]
- King, M.; Dinos, S.; Shaw, J.; Watson, R.; Stevens, S.; Passetti, F.; Weich, S.; Serfaty, M. The Stigma Scale: Development of a standardised measure of the stigma of mental illness. Br. J. Psychiatry 2007, 190, 248–254. [Google Scholar] [CrossRef]
- Angermeyer, M.C.; Schomerus, G. State of the art of population-based attitude research on mental health: A systematic review. Epidemiol. Psychiatr. Sci. 2016, 30, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Abiri, S.; Oakley, L.D.; Hitchcock, M.E.; Hall, A. Stigma related avoidance in people living with severe mental illness (SMI): Findings of an integrative review. Community Ment. Health J. 2016, 52, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Banerjee, S.; Byng, R.; Tylee, A.; Bhugra, D.; Macdonald, A. Primary care professionals’ perceptions of depression in older people: A qualitative study. Soc. Sci. Med. 2006, 63, 1363–1373. [Google Scholar] [CrossRef]
- Haralambous, B.; Dow, B.; Goh, A.; Pachana, N.A.; Bryant, C.; LoGiudice, D.; Lin, X. ‘Depression is not an illness. It’s up to you to make yourself happy’: Perceptions of Chinese health professionals and community workers about older Chinese immigrants’ experiences of depression and anxiety. Australas J. Ageing 2016, 35, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.; Mohapatra, M.K.; Panda, B. Prevalence of and factors contributing to anxiety, depression and cognitive disorders among urban elderly in Odisha—A study through the health systems’ Lens. Arch. Gerontol. Geriatr. 2018, 80, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.; Dobbs, D.; Roth, E.G.; Goldman, S.; Peeples, A.D.; Wallace, B. Promoting and Protecting Against Stigma in Assisted Living and Nursing Homes. Gerontologist 2016, 56, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B.G. Stigma as a fundamental cause of population health inequalities. Am. J. Public Health 2013, 103, 813–821. [Google Scholar] [CrossRef]
- Kane, A.; Murphy, C.; Kelly, M. Assessing implicit and explicit dementia stigma in young adults and care-workers. Dementia (London) 2018. [Google Scholar] [CrossRef]
- Smith, M. Stigma. Adv. Psychiatr. Treat. 2002, 8, 317–325. [Google Scholar] [CrossRef]
- Corrigan, P. The impact of stigma on severe mental illness. Cogn. Behav. Pract. 1999, 5, 201–222. [Google Scholar] [CrossRef]
- Thornicroft, G. Stigma and discrimination limit access to mental health care. Epidemiol. Psichiatr. Soc. 2008, 17, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Kim, J.M.; Kim, S.W.; Kang, H.J.; Lee, J.Y.; Bae, K.Y.; Shin, I.S.; Yoon, J.S. Perceived stigma and quality of life in patients following recovery from delirium. J. Clin. Psychiatry 2017, 78, e744–e749. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using, 3rd ed.; SPSS: London, UK, 2009; pp. 675–676. [Google Scholar]
- Kim, S.W.; Polari, A.; Melville, F.; Moller, B.; Kim, J.M.; Amminger, P.; Herrman, H.; McGorry, P.; Nelson, B. Are current labelling terms suitable for people who are at risk of psychosis? Schizophr. Res. 2017, 188, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Bahm, A.; Forchuk, C. Interlocking oppressions: The effect of a comorbid physical disability on perceived stigma and discrimination among mental health consumers in Canada. Health Soc. Care Community 2009, 17, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Pelleboer-Gunnink, H.A.; Van Oorsouw, W.M.; Van Weeghel, J.; Embregts, P.J. Mainstream health professionals’ stigmatising attitudes towards people with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2017, 61, 411–434. [Google Scholar] [CrossRef] [PubMed]
- Allesøe, K.; Søgaard, K.; Aadahl, M.; Boyle, E.; Holtermann, A. Are hypertensive women at additional risk of ischaemic heart disease from physically demanding work? Eur. J. Prev. Cardiol. 2016, 23, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2014, 11, CD002892. [Google Scholar]
- Mark, G.; Smith, A.P. Occupational stress, job characteristics, coping, and the mental health of nurses. Br. J. Health Psychol. 2012, 17, 505–521. [Google Scholar] [CrossRef]
- Kerrien, M.; Pougnet, R.; Garlantézec, R.; Pougnet, L.; Le Galudec, M.; Loddé, B.; Dewitte, J.D. Prevalence of anxiety disorders and depression among junior doctors and their links with their work. Presse Med. 2015, 44 Pt 1, e84–e91. [Google Scholar] [CrossRef]
- Alamgir, H.; Yu, S.; Drebit, S.; Fast, C.; Kidd, C. Are female healthcare workers at higher risk of occupational injury? Occup. Med. (Lond.) 2009, 59, 149–152. [Google Scholar] [CrossRef] [Green Version]
- Singhal, V.; Bora, D.; Singh, S. Hepatitis B in health care workers: Indian scenario. J. Lab. Physicians 2009, 1, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Parmeggiani, C.; Abbate, R.; Marinelli, P.; Angelillo, I.F. Healthcare workers and health care-associated infections: Knowledge, attitudes, and behavior in emergency departments in Italy. BMC Infect. Dis. 2010, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Litton, K.A. Delirium in the critical care patient: What the professional staff needs to know. Crit. Care Nurs. Q. 2003, 26, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Moyle, W.; Cooke, M.; O’Dwyer, S.T. An educational programme to improve acute care nurses’ knowledge, attitudes and family caregiver involvement in care of people with cognitive impairment. Scand. J. Caring Sci. 2017, 31, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Couture, S.M.; Penn, D.L. Interpersonal contact and the stigma of mental illness: A review of the literature. J. Ment. Health 2003, 12, 291–305. [Google Scholar] [CrossRef] [Green Version]
- Phelan, J.C.; Link, B.G. Fear of people with mental illnesses: The role of personal and impersonal contact and exposure to threat or harm. J. Health Soc. Behav. 2004, 45, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Link, B.G.; Cullen, F.T.; Frank, J.; Wozniak, J.F. The Social Rejection of Former Mental Patients: Understanding Why Labels Matter. Am. J. Sociol. 1987, 92, 1461–1500. [Google Scholar] [CrossRef]




© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukaetova-Ladinska, E.B.; Cosker, G.; Chan, M.; Coppock, M.; Scully, A.; Kim, S.-Y.; Kim, S.-W.; McNally, R.J.Q.; Teodorczuk, A. Delirium Stigma Among Healthcare Staff. Geriatrics 2019, 4, 6. https://doi.org/10.3390/geriatrics4010006
Mukaetova-Ladinska EB, Cosker G, Chan M, Coppock M, Scully A, Kim S-Y, Kim S-W, McNally RJQ, Teodorczuk A. Delirium Stigma Among Healthcare Staff. Geriatrics. 2019; 4(1):6. https://doi.org/10.3390/geriatrics4010006
Chicago/Turabian StyleMukaetova-Ladinska, Elizabeta B., Glynis Cosker, Mahathir Chan, Michael Coppock, Ann Scully, Seon-Young Kim, Sung-Wan Kim, Richard J. Q. McNally, and Andrew Teodorczuk. 2019. "Delirium Stigma Among Healthcare Staff" Geriatrics 4, no. 1: 6. https://doi.org/10.3390/geriatrics4010006
APA StyleMukaetova-Ladinska, E. B., Cosker, G., Chan, M., Coppock, M., Scully, A., Kim, S.-Y., Kim, S.-W., McNally, R. J. Q., & Teodorczuk, A. (2019). Delirium Stigma Among Healthcare Staff. Geriatrics, 4(1), 6. https://doi.org/10.3390/geriatrics4010006