
The Influence of Physical, Mental, and Cognitive Factors on Health-Related Quality of Life among Community-Dwelling Older Adults: A Focus on Central Sensitization-Related Symptoms
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
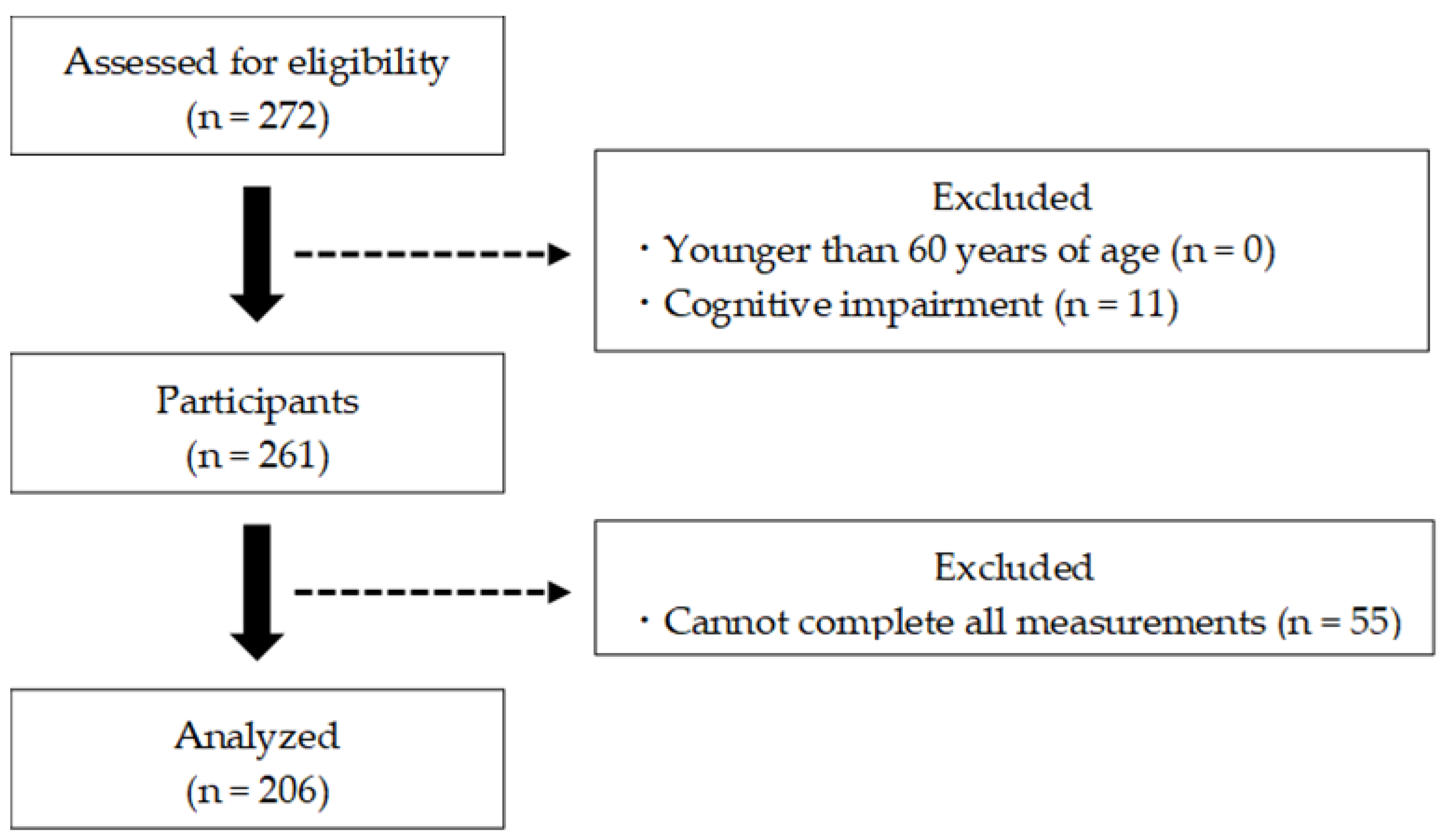
2.1. Participants
2.2. Measures
2.2.1. HRQOL
2.2.2. Physical Factors
2.2.3. Mental Factors
2.2.4. Cognitive Factors
2.2.5. Central Sensitization-Related Symptoms (CSS)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Prospects. Summary of Results. Available online: https://www.un.org/development/desa/pd/content/World-Population-Prospects-2022 (accessed on 16 August 2023).
- Horner, B.; Boldy, D.P. The benefit and burden of “ageing-in-place” in an aged care community. Aust. Health Rev. 2008, 32, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Makino, K.; Lee, S.; Bae, S.; Jung, S.; Shinkai, Y.; Chiba, I.; Shimada, H. Pain characteristics and incidence of functional disability among community-dwelling older adults. PLoS ONE 2019, 14, e0215467. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Leung, J.; Lau, E. Prevalence and correlates of musculoskeletal pain in Chinese elderly and the impact on 4-year physical function and quality of life. Public Health 2009, 123, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Goesling, J.; Clauw, D.J.; Hassett, A.L. Pain and depression: An integrative review of neurobiological and psychological factors. Curr. Psychiatry Rep. 2013, 15, 421. [Google Scholar] [CrossRef] [PubMed]
- Bell, T.; Franz, C.E.; Kremen, W.S. Persistence of pain and cognitive impairment in older adults. J. Am. Geriatr. Soc. 2022, 70, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Lapane, K.L.; Quilliam, B.J.; Benson, C.; Chow, W.; Kim, M.S. Impact of noncancer pain on health-related quality of life. Pain Pract. 2015, 15, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Reina, E.; Valdellós, J.; Ocaña-Riola, R.; García-Merino, M.R.; Aguilar-Cano, L.; Ariza-Zafra, G.; Bellido-Estévez, I. Factors associated with health-related quality of life in community-dwelling older adults: A multinomial logistic analysis. J. Clin. Med. 2019, 8, 1810. [Google Scholar] [CrossRef] [PubMed]
- Paladini, A.; Fusco, M.; Coaccioli, S.; Skaper, S.D.; Varrassi, G. Chronic pain in the elderly: The case for new therapeutic strategies. Pain Physician 2015, 18, E863–E876. [Google Scholar]
- Yunus, M.B. Fibromyalgia and overlapping disorders: The unifying concept of central sensitivity syndromes. Semin. Arthritis Rheum. 2007, 36, 339–356. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain. 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Druce, K.L.; McBeth, J. Central sensitization predicts greater fatigue independently of musculoskeletal pain. Rheumatology 2019, 58, 1923–1927. [Google Scholar] [CrossRef]
- de Tommaso, M.; Delussi, M.; Vecchio, E.; Sciruicchio, V.; Invitto, S.; Livrea, P. Sleep features and central sensitization symptoms in primary headache patients. J. Headache Pain 2014, 15, 64. [Google Scholar] [CrossRef]
- Kim, J.J.; Diamond, D.M. The stressed hippocampus, synaptic plasticity and lost memories. Nat. Rev. Neurosci. 2002, 3, 453–462. [Google Scholar] [CrossRef]
- Yunus, M.B. Central sensitivity syndromes: A new paradigm and group nosology for fibromyalgia and overlapping conditions, and the related issue of disease versus illness. Semin. Arthritis Rheum. 2008, 37, 339–352. [Google Scholar] [CrossRef]
- Koga, M.; Shigetoh, H.; Tanaka, Y.; Morioka, S. Characteristics of clusters with contrasting relationships between central sensitization-related symptoms and pain. Sci. Rep. 2022, 12, 2626. [Google Scholar] [CrossRef]
- Mibu, A.; Nishigami, T.; Tanaka, K.; Manfuku, M.; Yono, S. Difference in the impact of central sensitization on pain-related symptoms between patients with chronic low back pain and knee osteoarthritis. J. Pain Res. 2019, 12, 1757–1765. [Google Scholar] [CrossRef]
- Ide, K.; Yasuda, T.; Hasegawa, T.; Yamato, Y.; Yoshida, G.; Banno, T.; Arima, H.; Oe, S.; Mihara, Y.; Ushirozako, H.; et al. Evaluation of the Central Sensitization Inventory score in elderly adults with musculoskeletal examination. Mod. Rheumatol. 2021, 31, 885–889. [Google Scholar] [CrossRef]
- Manfuku, M.; Nishigami, T.; Mibu, A.; Tanaka, K.; Kitagaki, K.; Sumiyoshi, K. Comparison of central sensitization-related symptoms and health-related quality of life between breast cancer survivors with and without chronic pain and healthy controls. Breast Cancer 2019, 26, 758–765. [Google Scholar] [CrossRef]
- Haruyama, Y.; Sairenchi, T.; Uchiyama, K.; Suzuki, K.; Hirata, K.; Kobashi, G. A large-scale population-based epidemiological study on the prevalence of central sensitization syndromes in Japan. Sci. Rep. 2021, 11, 23299. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of value set based on DCE and/or TTO data: Scoring for EQ-5D-5L health states in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef]
- Ikeda, S.; Shiroiwa, T.; Igarashi, A.; Noto, S.; Fukuda, T.; Saito, S.; Shimozuma, K. Developing a Japanese version of the EQ-5D-5L value set. J. Natl. Inst. Public Health 2015, 64, 47–55. [Google Scholar]
- Yamada, Y.; Watanabe, Y.; Ikenaga, M.; Yokoyama, K.; Yoshida, T.; Morimoto, T.; Kimura, M. Comparison of single- or multifrequency bioelectrical impedance analysis and spectroscopy for assessment of appendicular skeletal muscle in the elderly. J. Appl. Physiol. 2013, 115, 812–818. [Google Scholar] [CrossRef]
- Nakatani, T.; Nadamoto, M.; Mimura, K.; Itoh, M. Validation of a 30-sec chair-stand test for evaluating lower extremity muscle strength in Japanese elderly adults. Jpn J. Phys. Educ. Health Sport Sci. 2002, 47, 451–461. [Google Scholar] [CrossRef]
- Goda, A.; Murata, S.; Nakano, H.; Matsuda, H.; Yokoe, K.; Mitsumoto, H.; Shiraiwa, K.; Abiko, T.; Horie, J. Temporal patterns in performance of the 30 second chair-stand test evince differences in physical and mental characteristics among community-dwelling older adults in Japan. Healthcare 2020, 8, 146. [Google Scholar] [CrossRef]
- Kurosawa, C.; Shimazu, N.; Yamamoto, S. Where do healthy older adults take more time during the Timed Up and Go test? J. Phys. Ther. Sci. 2020, 32, 663–668. [Google Scholar] [CrossRef]
- Kikuchi, Y.; Murata, S.; Abiko, T.; NaKano, H.; Shiraiwa, K.; Gouda, A.; Horie, J. Influence of physical and psychological function and pain on vital function of community-dwelling elderly women. Jpn J. Health Promot. 2021, 23, 159–167. [Google Scholar]
- Imai, R.; Imaoka, M.; Nakao, H.; Hida, M.; Tazaki, F.; Omizu, T.; Ishigaki, T.; Nakamura, M. Association between chronic pain and pre-frailty in Japanese community-dwelling older adults: A cross-sectional study. PLoS ONE 2020, 15, e0236111. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Murata, C.; Hirai, H.; Kondo, N.; Kondo, K.; Ueda, K.; Ichida, N. Predictive validity of GDS5 using AGES project data. Kousei Shihyou 2014, 61, 7–12. (In Japanese) [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Goda, A.; Murata, S.; Nakano, H.; Shiraiwa, K.; Abiko, T.; Nonaka, K.; Iwase, H.; Anami, K.; Horie, J. Subjective and objective mental and physical functions affect subjective cognitive decline in community-dwelling elderly Japanese people. Healthcare 2020, 8, 347. [Google Scholar] [CrossRef]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Heilbronner, R.L.; Henry, G.K.; Buck, P.; Adams, R.L.; Fogle, T. Lateralized brain damage and performance on trail making A and B, digit span forward and backward, and TPT memory and location. Arch. Clin. Neuropsychol. 1991, 6, 251–258. [Google Scholar] [CrossRef]
- Loeser, J.D.; Treede, R.D. The Kyoto protocol of IASP basic pain terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef]
- Yunus, M.B. Role of central sensitization in symptoms beyond muscle pain, and the evaluation of a patient with widespread pain. Best Pract. Res. Clin. Rheumatol. 2007, 21, 481–497. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef]
- Nishigami, T.; Tanaka, K.; Mibu, A.; Manfuku, M.; Yono, S.; Tanabe, A. Development and psychometric properties of short form of Central Sensitization Inventory in participants with musculoskeletal pain: A cross-sectional study. PLoS ONE 2018, 13, e0200152. [Google Scholar] [CrossRef]
- Tanaka, K.; Nishigami, T.; Mibu, A.; Manfuku, M.; Yono, S.; Yukioka, M.; Miki, K. Cutoff value for short form of Central Sensitization Inventory. Pain Pract. 2020, 20, 269–276. [Google Scholar] [CrossRef]
- Sheather, S. A Modern Approach to Regression with R; Springer Science & Business Media: New York, NY, USA, 2009; pp. 263–364. [Google Scholar]
- Shiroiwa, T.; Noto, S.; Fukuda, T. Japanese Population Norms of EQ-5D-5L and Health Utilities Index Mark 3: Disutility Catalog by Disease and Symptom in Community Settings. Value Health 2021, 24, 1193–1202. [Google Scholar] [CrossRef] [PubMed]
- Kyle, S.D.; Morgan, K.; Espie, C.A. Insomnia and health-related quality of life. Sleep. Med. Rev. 2010, 14, 69–82. [Google Scholar] [CrossRef]
- Fortier-Brochu, E.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Relations between sleep, fatigue, and health-related quality of life in individuals with insomnia. J. Psychosom. Res. 2010, 69, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Wang, X.; Ma, Q.; Sun, H.P.; Xu, Y.; Wang, P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci. Rep. 2015, 5, 17301. [Google Scholar] [CrossRef]
- Aili, K.; Andersson, M.; Bremander, A.; Haglund, E.; Larsson, I.; Bergman, S. Sleep problems and fatigue as predictors for the onset of chronic widespread pain over a 5- and 18-year perspective. BMC Musculoskelet. Disord. 2018, 19, 390. [Google Scholar] [CrossRef] [PubMed]
- Rief, W.; Hessel, A.; Braehler, E. Somatization symptoms and hypochondriacal features in the general population. Psychosom. Med. 2001, 63, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Nishigami, T.; Mibu, A.; Manfuku, M.; Yono, S.; Shinohara, Y.; Tanabe, A.; Ono, R. Validation of the Japanese version of the Central Sensitization Inventory in patients with musculoskeletal disorders. PLoS ONE 2017, 12, e0188719. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Tan, L.; Cicuttini, F.M.; Fairley, J.; Romero, L.; Estee, M.; Hussain, S.M.; Urquhart, D.M. Does aerobic exercise effect pain sensitisation in individuals with musculoskeletal pain? A systematic review. BMC Musculoskelet. Disord. 2022, 23, 113. [Google Scholar] [CrossRef]
- Larun, L.; Brurberg, K.G.; Odgaard-Jensen, J.; Price, J.R. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst. Rev. 2019, 10, CD003200. [Google Scholar] [CrossRef]
- Fank, F.; Pereira, F.D.S.; Dos Santos, L.; de Mello, M.T.; Mazo, G.Z. Effects of exercise on sleep in older adults: An overview of systematic reviews and meta-analyses. J. Aging Phys. Act. 2022, 30, 1101–1117. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.C.; Lee, A.T.C.; Lam, L.C.W. Exercise for the prevention and treatment of neurocognitive disorders: New evidence and clinical recommendations. Curr. Opin. Psychiatry 2021, 34, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Cedraschi, C.; Ludwig, C.; Allaz, A.F.; Herrmann, F.R.; Luthy, C. Pain and health-related quality of life (HRQoL): A national observational study in community-dwelling older adults. Eur. Geriatr. Med. 2018, 9, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Tansuğ, M.; Kahraman, T.; Genç, A. Differences in pain characteristics and functional associations between nursing home residents and community-dwelling older adults: A cross-sectional study. Ann. Geriatr. Med. Res. 2021, 25, 187–196. [Google Scholar] [CrossRef]
- Molander, P.; Dong, H.J.; Äng, B.; Enthoven, P.; Gerdle, B. The role of pain in chronic pain patients’ perception of health-related quality of life: A cross-sectional SQRP study of 40,000 patients. Scand. J. Pain 2018, 18, 417–429. [Google Scholar] [CrossRef]
- Wettstein, M.; Eich, W.; Bieber, C.; Tesarz, J. Pain intensity, disability, and quality of life in patients with chronic low back pain: Does age matter? Pain Med. 2019, 20, 464–475. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n = 206 | |||
|---|---|---|---|
| Mean ± SD | |||
| Age | years | 77.4 ± 6.0 | |
| Gender | n (%) | Male/Female | 38 (18.4)/168 (81.6) |
| Height | cm | 151.8 ± 11.6 | |
| Weight | kg | 51.9 ± 8.9 | |
| BMI | 22.6 ± 3.4 | ||
| Educational history | years | 11.6 ± 2.3 | |
| HRQOL score | 0.896 ± 0.120 | ||
| Hand grip | kgf | 21.8 ± 6.1 | |
| Knee extension | kgf | 24.2 ± 7.7 | |
| CS-30 | repetitions | 20.1 ± 6.2 | |
| One-leg standing time | seconds | 31.6 ± 35.9 | |
| TUG | seconds | 7.0 ± 3.9 | |
| Pain | n (%) | 119 (57.8) | |
| Pain intensity | points | 2.3 ± 2.4 | |
| Number of pain sites | n (%) | 0 | 87 (42.2) |
| 1 | 60 (29.1) | ||
| 2 | 42 (20.4) | ||
| 3 | 14 (6.8) | ||
| 4 | 2 (1.0) | ||
| 5 | - | ||
| 6 | 1 (0.5) | ||
| GDS-5 | points | 0.7 ± 1.0 | |
| MMSE | points | 28.2 ± 1.9 | |
| TMT | seconds | 137.7 ± 53.3 | |
| CSI-9 | points | 6.5 ± 4.8 | |
| n = 206 | |||||
|---|---|---|---|---|---|
| Age | Height | Weight | BMI | Educational History | |
| HRQOL score | −0.157 * | −0.048 | −0.031 | −0.013 | 0.048 |
| n = 206 | ||||||
|---|---|---|---|---|---|---|
| Hand Grip | Knee Extension | CS-30 | One-Leg Standing | TUG | ||
| HRQOL score | 0.114 | 0.156 * | 0.267 ** | 0.189 ** | −0.259 ** | |
| Pain intensity | Number of pain sites | GDS-5 | MMSE | TMT-A | CSI-9 | |
| HRQOL score | −0.456 ** | −0.418 ** | −0.268 ** | 0.172 * | −0.069 | −0.409 ** |
| n = 206 | |||||||
|---|---|---|---|---|---|---|---|
| Dependent Variables | HRQOL Score | ||||||
| B | β | 95% CI | p Value | VIF | |||
| Lower | Upper | ||||||
| Independent variables | Age | −0.002 | −0.085 | −0.004 | 0.001 | 0.219 | 1.381 |
| Knee extension | 0.000 a | −0.032 | −0.003 | 0.002 | 0.635 | 1.320 | |
| CS-30 | 0.002 | 0.081 | −0.001 | 0.004 | 0.275 | 1.563 | |
| One-leg standing time | 0.000 b | 0.011 | 0.000 | 0.000 | 0.873 | 1.353 | |
| TUG | 0.002 | 0.058 | −0.002 | 0.005 | 0.352 | 1.093 | |
| Pain intensity | −0.011 | −0.217 | −0.020 | −0.002 | 0.017 | 2.344 | |
| Number of pain sites | −0.014 | −0.126 | −0.034 | 0.006 | 0.161 | 2.315 | |
| GDS-5 | −0.004 | −0.029 | −0.019 | 0.012 | 0.657 | 1.253 | |
| MMSE | 0.006 | 0.101 | −0.002 | 0.015 | 0.116 | 1.191 | |
| CSI-9 | −0.007 | −0.277 | −0.010 | −0.003 | p < 0.001 | 1.474 | |
| Adjusted R2 | 0.287 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikuchi, Y.; Nakano, H.; Goda, A.; Mori, K.; Abiko, T.; Mitsumaru, N.; Murata, S. The Influence of Physical, Mental, and Cognitive Factors on Health-Related Quality of Life among Community-Dwelling Older Adults: A Focus on Central Sensitization-Related Symptoms. Geriatrics 2024, 9, 11. https://doi.org/10.3390/geriatrics9010011
Kikuchi Y, Nakano H, Goda A, Mori K, Abiko T, Mitsumaru N, Murata S. The Influence of Physical, Mental, and Cognitive Factors on Health-Related Quality of Life among Community-Dwelling Older Adults: A Focus on Central Sensitization-Related Symptoms. Geriatrics. 2024; 9(1):11. https://doi.org/10.3390/geriatrics9010011
Chicago/Turabian StyleKikuchi, Yuki, Hideki Nakano, Akio Goda, Kohei Mori, Teppei Abiko, Nozomi Mitsumaru, and Shin Murata. 2024. "The Influence of Physical, Mental, and Cognitive Factors on Health-Related Quality of Life among Community-Dwelling Older Adults: A Focus on Central Sensitization-Related Symptoms" Geriatrics 9, no. 1: 11. https://doi.org/10.3390/geriatrics9010011