



Night-Time Hot Spring Bathing Is Associated with a Lower Systolic Blood Pressure among Japanese Older Adults: A Single-Institution Retrospective Cohort Study

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Statistical Methods
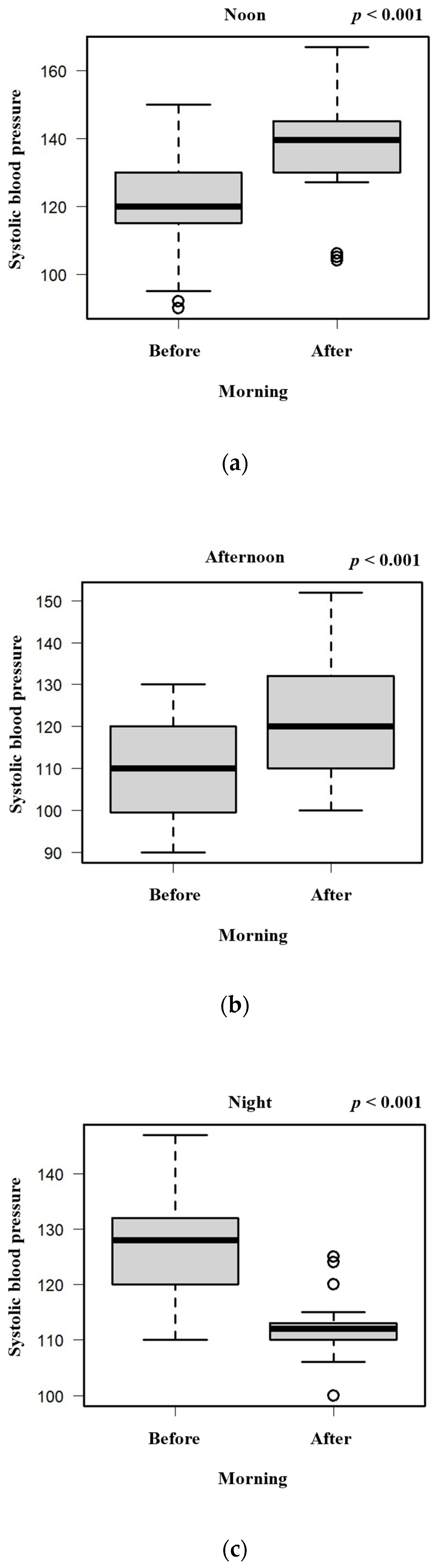
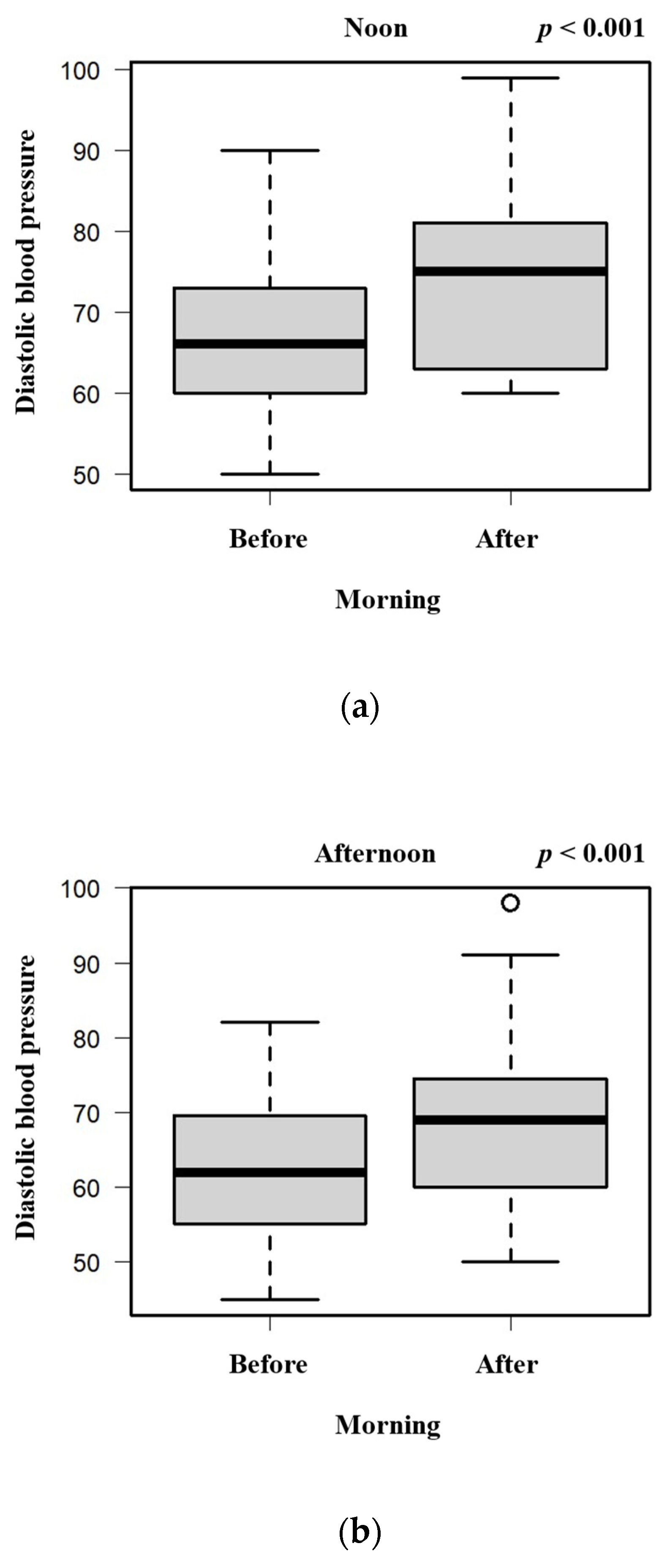
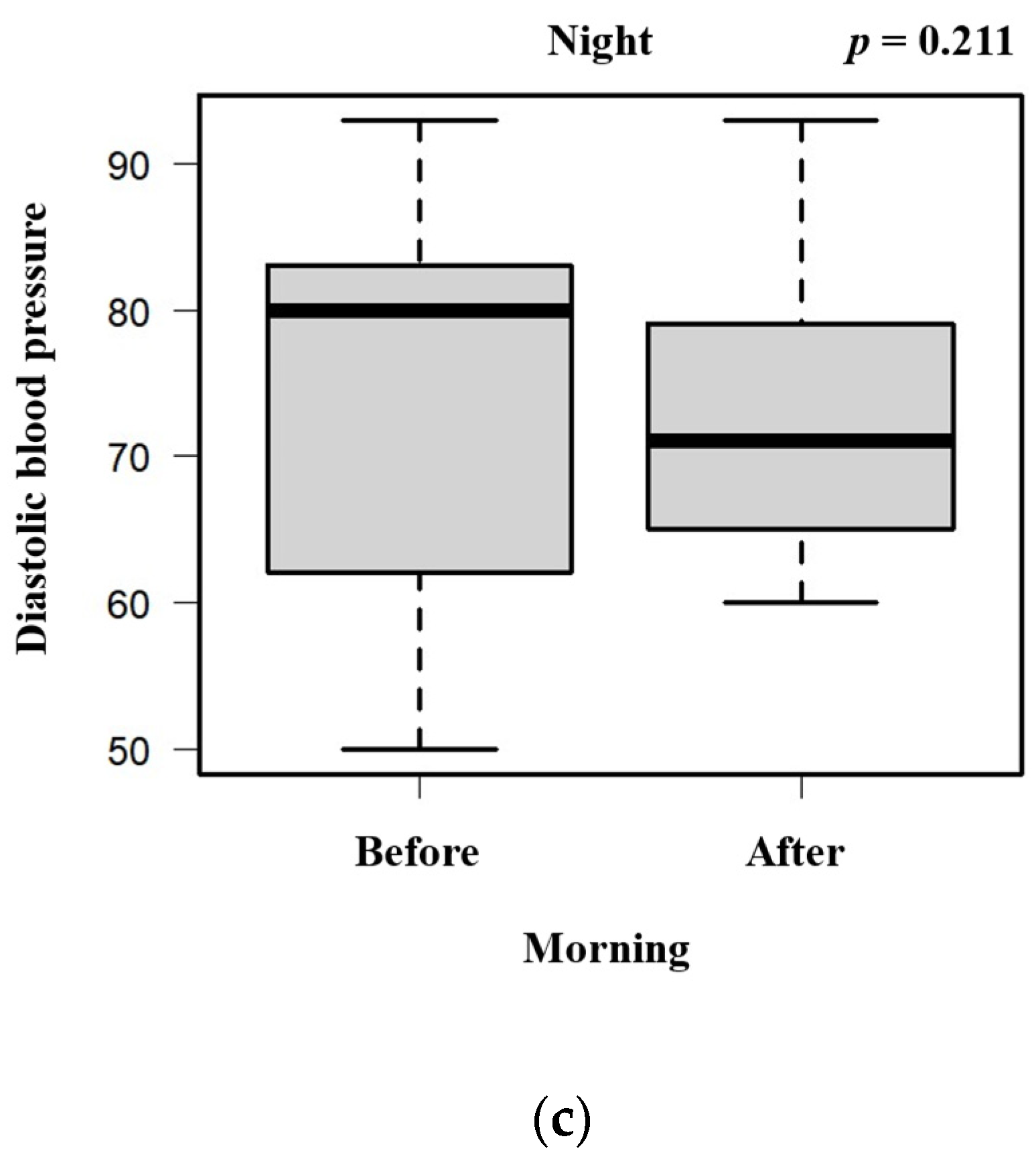
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoon, S.S.; Gu, Q.; Nwankwo, T.; Wright, J.D.; Hong, Y.; Burt, V. Trends in Blood Pressure Among Adults with Hypertension. Hypertension 2015, 65, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Carey, R.M.; Gidding, S.; Jones, D.W.; Taler, S.J.; Wright, J.T., Jr.; Whelton, P.K. Potential US Population Impact of the 2017 ACC/AHA High Blood Pressure Guideline. Circulation 2018, 137, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T.; Segawa, H.; Kadota, A.; Ohkubo, T.; Arima, H.; Miura, K. Epidemiology of hypertension in Japan: Beyond the new 2019 Japanese guidelines. Hypertens. Res. 2020, 43, 1344–1351. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; MacGregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- Tuck, M.L.; Sowers, J.; Dornfeld, L.; Kledzik, G.; Maxwell, M. The Effect of Weight Reduction on Blood Pressure, Plasma Renin Activity, and Plasma Aldosterone Levels in Obese Patients. N. Engl. J. Med. 1981, 304, 930–933. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Stampfer, M.J.; Curhan, G.C. Diet and Lifestyle Risk Factors Associated with Incident Hypertension in Women. JAMA 2009, 302, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R.; Evans, N.S.; Church, T.S.; Lewis, C.E.; Schreiner, P.J.; Jacobs, D.R., Jr.; Sternfeld, B.; Sidney, S. Joint Associations of Physical Activity and Aerobic Fitness on the Development of Incident Hypertension. Hypertension 2010, 56, 49–55. [Google Scholar] [CrossRef]
- Maeda, T.; Mimori, K.; Suzuki, S.; Horiuchi, T.; Makino, N. Preventive and promotive effects of habitual hot spa-bathing on the elderly in Japan. Sci. Rep. 2018, 8, 133. [Google Scholar] [CrossRef]
- Wang, P.-C.; Song, Q.-C.; Chen, C.-Y.; Su, T.-C. Cardiovascular physiological effects of balneotherapy: Focused on seasonal differences. Hypertens. Res. 2023, 46, 1650–1661. [Google Scholar] [CrossRef]
- Ojima, S.; Ohishi, M. Effects of hot spring bathing on cardiac and vascular function. Hypertens. Res. 2023, 46, 1705–1706. [Google Scholar] [CrossRef]
- Birger, M.; Kaldjian, A.S.; Roth, G.A.; Moran, A.E.; Dieleman, J.L.; Bellows, B.K. Spending on Cardiovascular Disease and Cardiovascular Risk Factors in the United States: 1996 to 2016. Circulation 2021, 144, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Rohleder, N. Stress and inflammation—The need to address the gap in the transition between acute and chronic stress effects. Psychoneuroendocrinology 2019, 105, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Rozanski, A.; Blumenthal, J.A.; Kaplan, J. Impact of Psychological Factors on the Pathogenesis of Cardiovascular Disease and Implications for Therapy. Circulation 1999, 99, 2192–2217. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, S.; Tokunou, T.; Maeda, T.; Horiuchi, T. Hot spring bathing is associated with a lower prevalence of hyper-tension among Japanese older adults: A cross-sectional study in Beppu. Sci. Rep. 2022, 12, 19462. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Tai, Y.; Saeki, K.; Yamagami, Y.; Yoshimoto, K.; Kurumatani, N.; Nishio, K.; Obayashi, K. Association between timing of hot water bathing before bedtime and night-/sleep-time blood pressure and dipping in the elderly: A longitudinal analysis for repeated measurements in home settings. Chrono Int. 2019, 36, 1714–1722. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, J.; Yoshino, Y.; Watanabe, S.; Harada, K. Reduction in central blood pressure after bathing in hot water. Blood Press. Monit. 2016, 21, 80–86. [Google Scholar] [CrossRef]
- Kawano, Y. Diurnal blood pressure variation and related behavioral factors. Hypertens. Res. 2010, 34, 281–285. [Google Scholar] [CrossRef]
- Obara, T.; the J-HOME Study Group; Ito, K.; Ohkubo, T.; Shibamiya, T.; Shinki, T.; Nakashita, M.; Hara, A.; Metoki, H.; Inoue, R.; et al. Uncontrolled hypertension based on morning and evening home blood pressure measurements from the J-HOME study. Hypertens. Res. 2009, 32, 1072–1078. [Google Scholar] [CrossRef]
- Franklin, S.S.; Jacobs, M.J.; Wong, N.D.; L’italien, G.J.; Lapuerta, P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: Analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension 2001, 37, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Franklin, S.S.; Larson, M.G.; Khan, S.A.; Wong, N.D.; Leip, E.P.; Kannel, W.B.; Levy, D. Does the Relation of Blood Pressure to Coronary Heart Disease Risk Change with Aging? Circulation 2001, 103, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V. Isolated Systolic Hypertension in the Elderly. N. Engl. J. Med. 2007, 357, 789–796. [Google Scholar] [CrossRef]
- A Staessen, J.; Gasowski, J.; Wang, J.G.; Thijs, L.; Hond, E.D.; Boissel, J.-P.; Coope, J.; Ekbom, T.; Gueyffier, F.; Liu, L.; et al. Risks of untreated and treated isolated systolic hypertension in the elderly: Meta-analysis of outcome trials. Lancet 2000, 355, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Barriuso, R.; Banegas, J.R.; Damin, J.; Appel, L.J.; Guallar, E. Systolic blood pressure, diastolic blood pressure, and pulse pressure: An evaluation of their joint effect on mortality. Ann. Intern. Med. 2003, 139, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Protogerou, A.D.; Safar, M.E.; Iaria, P.; Safar, H.; Le Dudal, K.; Filipovsky, J.; Henry, O.; Ducimetière, P.; Blacher, J. Diastolic Blood Pressure and Mortality in the Elderly with Cardiovascular Disease. Hypertension 2007, 50, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, T.; Aoyama, Y.; Sakoda, A.; Nakagawa, S.; Yamaoka, K. Basic study on biochemical mechanism of thoron and thermal therapy. Physiol. Chem. Phys. Med. 2006, 38, 85–92. [Google Scholar]
- Chen, Z.; Yang, J.; Zhu, L.; Zhang, A.; Wang, Z.; Liu, P.; Wang, G.; Li, C.; Luo, T.; Zhou, Y. Classification of typical hot springs and their relationship with health in Guizhou, China. Environ. Geochem. Health 2020, 43, 1287–1304. [Google Scholar] [CrossRef]
- Henderson, K.N.; Killen, L.G.; O’Neal, E.K.; Waldman, H.S. The Cardiometabolic Health Benefits of Sauna Exposure in Individuals with High-Stress Occupations. A Mechanistic Review. Int. J. Environ. Res. Public Health 2021, 18, 1105. [Google Scholar] [CrossRef]
- Akerman, A.P.; Notley, S.R.; Sigal, R.J.; Boulay, P.; Ruzicka, M.; Friesen, B.J.; Kenny, G.P. Impact of uncomplicated controlled hypertension on thermoregulation during exercise-heat stress. J. Hum. Hypertens. 2020, 35, 880–883. [Google Scholar] [CrossRef]
- Tai, Y.; Obayashi, K.; Yamagami, Y.; Yoshimoto, K.; Kurumatani, N.; Nishio, K.; Saeki, K. Hot-water bathing before bedtime and shorter sleep onset latency are accompanied by a higher distal-proximal skin temperature gradient in older adults. Sleep Med. 2021, 17, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Sawatari, H.; Nishizaka, M.K.; Miyazono, M.; Ando, S.I.; Inoue, S.; Takemoto, M.; Sakamoto, T.; Goto, D.; Furumoto, T.; Kinugawa, S.; et al. Three nights leg thermal therapy could improve sleep quality in patients with chronic heart failure. Heart Vessel. 2018, 33, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Haghayegh, S.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R.; Castriotta, R.J. Before-bedtime passive body heating by warm shower or bath to improve sleep: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 46, 124–135. [Google Scholar] [CrossRef]
- Pinheiro, L.C.; Oliveira-Paula, G.H. Sources and Effects of Oxidative Stress in Hypertension. Curr. Hypertens. Rev. 2021, 16, 166–180. [Google Scholar] [CrossRef]
- Podstawski, R.; Borysławski, K.; Pomianowski, A.; Krystkiewicz, W.; Żurek, P. Endocrine Effects of Repeated Hot Thermal Stress and Cold Water Immersion in Young Adult Men. Am. J. Mens Health 2021, 15, 15579883211008339. [Google Scholar] [CrossRef]
- Song, W.; Wang, H.; Wu, Q. Atrial natriuretic peptide in cardiovascular biology and disease (NPPA). Gene 2015, 569, 1–6. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Baseline BP | ||||
|---|---|---|---|---|---|
| Characteristics | Noon | Afternoon | Night | SBP | DBP |
| n = 26 | n = 52 | n = 21 | Mean (IQR), mmHg | ||
| Age, mean (IQR), year | 72 (5) | 79 (16) | 78 (14) | ||
| Female (%) | 6 (23) | 29 (56) | 15 (71) | ||
| Comorbidity (%) | |||||
| Hypertension | 9 (35) | 11 (21) | 9 (43) | 114 (15) | 67 (12) |
| Benign cardiac arrhythmia | 0 | 3 (6) | 3 (14) | 112 (2) | 61 (11) |
| Stroke | 3 (12) | 0 | 0 | 132 (10) | 80 (9) |
| Gout | 0 | 3 (6) | 0 | 122 (2) | 66 (5) |
| Diabetes mellitus | 9 (35) | 23 (44) | 9 (43) | 116 (13) | 64 (10) |
| Hyperlipidemia | 6 (23) | 11 (21) | 3 (14) | 120 (14) | 70 (9) |
| Renal disease | 0 | 7 (14) | 2 (10) | 117 (8) | 66 (9) |
| Chronic hepatitis | 3 (12) | 0 | 0 | 92 (2) | 61 (1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamasaki, S.; Tokunou, T.; Maeda, T.; Horiuchi, T. Night-Time Hot Spring Bathing Is Associated with a Lower Systolic Blood Pressure among Japanese Older Adults: A Single-Institution Retrospective Cohort Study. Geriatrics 2024, 9, 2. https://doi.org/10.3390/geriatrics9010002
Yamasaki S, Tokunou T, Maeda T, Horiuchi T. Night-Time Hot Spring Bathing Is Associated with a Lower Systolic Blood Pressure among Japanese Older Adults: A Single-Institution Retrospective Cohort Study. Geriatrics. 2024; 9(1):2. https://doi.org/10.3390/geriatrics9010002
Chicago/Turabian StyleYamasaki, Satoshi, Tomotake Tokunou, Toyoki Maeda, and Takahiko Horiuchi. 2024. "Night-Time Hot Spring Bathing Is Associated with a Lower Systolic Blood Pressure among Japanese Older Adults: A Single-Institution Retrospective Cohort Study" Geriatrics 9, no. 1: 2. https://doi.org/10.3390/geriatrics9010002