

Neurocognitive Effects of an Online Brain Health Program and Weekly Telehealth Support Group in Older Adults with Subjective Memory Loss: A Pilot Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Intervention
2.3. Outcomes
2.4. Statistical Analysis
3. Results
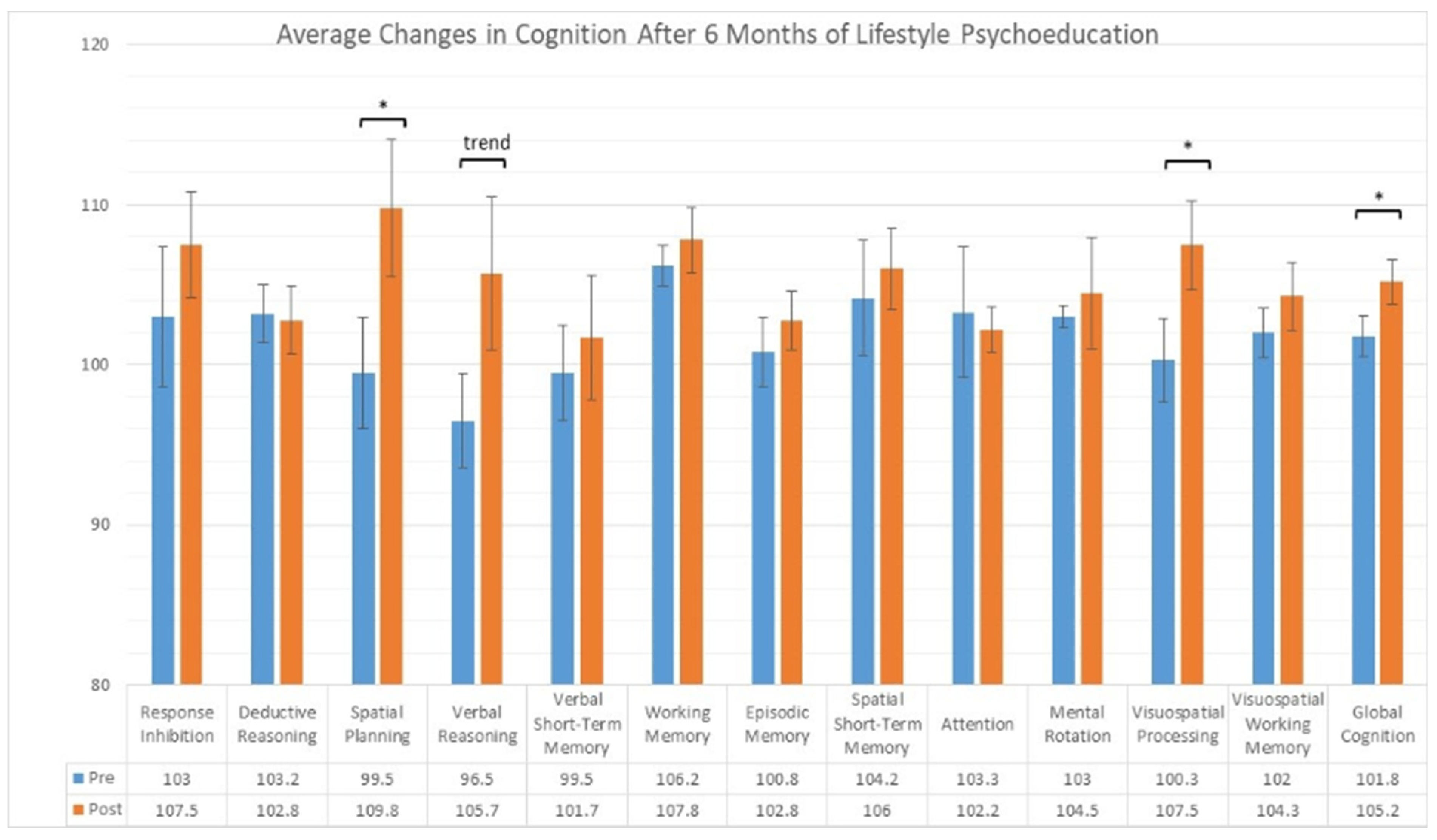
3.1. Cognitive Outcome Measures
3.2. Subjective Reports
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.; Demnitz, N.; Yamamoto, S.; Yaffe, K.; Lawlor, B.; Leroi, I. Defining brain health: A concept analysis. Int. J. Geriatr. Psychiatry 2022, 37. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, Y.; Li, H. What is brain health and why is it important? BMJ 2020, 371, m3683. [Google Scholar] [CrossRef] [PubMed]
- Randolph, J.J.; Strober, L.; Arnett, P.A. Assessment of Lifestyle Factors Associated with Brain Health. In Positive Neuropsychology: Evidence-Based Perspectives on Promoting Brain and Cognitive Health; Randolph, J.J., Ed.; Springer International Publishing: Cham, Switzerland, 2022; pp. 141–160. [Google Scholar]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Hodes, J.F.; Oakley, C.I.; O’Keefe, J.H.; Lu, P.; Galvin, J.E.; Saif, N.; Bellara, S.; Rahman, A.; Kaufman, Y.; Hristov, H.; et al. Alzheimer’s “Prevention” vs. “Risk Reduction”: Transcending Semantics for Clinical Practice. Front. Neurol. 2019, 9, 425076. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Stern, Y.; Gu, Y. Modifiable lifestyle factors and cognitive reserve: A systematic review of current evidence. Ageing Res. Rev. 2022, 74, 101551. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, R.F.; Seshadri, S. Risk Factors, Lifestyle Behaviors, and Vascular Brain Health. Stroke 2022, 53, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Merrill, D.A.; Siddarth, P.; Kepe, V.; Raja, P.V.; Saito, N.; Ercoli, L.M.; Miller, K.J.; Lavretsky, H.; Bookheimer, S.Y.; Barrio, J.R.; et al. Vascular risk and FDDNP-PET influence cognitive performance. J. Alzheimers Dis. 2013, 35, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, G.; Bartrés-Faz, D.; Morris, T.P.; Solana Sánchez, J.; Macià, D.; Tormos, J.M.; Pascual-Leone, A. The Barcelona Brain Health Initiative: Cohort description and first follow-up. PLoS ONE 2020, 15, e0228754. [Google Scholar] [CrossRef]
- Cattaneo, G.; Bartrés-Faz, D.; Morris, T.P.; Sánchez, J.S.; Macià, D.; Tarrero, C.; Tormos, J.M.; Pascual-Leone, A. The Barcelona Brain Health Initiative: A Cohort Study to Define and Promote Determinants of Brain Health. Front. Aging Neurosci. 2018, 10, 321. [Google Scholar] [CrossRef]
- Huffman, M. Health coaching: A new and exciting technique to enhance patient self-management and improve outcomes. Home Healthc. Nurse 2007, 25, 271–274, quiz 275–276. [Google Scholar] [CrossRef]
- Huffman, M.H. Advancing the Practice of Health Coaching: Differentiation From Wellness Coaching. Workplace Health Saf. 2016, 64, 400–403. [Google Scholar] [PubMed]
- Kreisberg, J.; Marra, R. Board-certified Health Coaches?What Integrative Physicians Need to Know. Integr. Med. Clin. J. 2017, 16, 22–24. [Google Scholar]
- Campitelli, A.; Gills, J.L.; Jones, M.D.; Paulson, S.; Myers, J.; Bryk, K.; Madero, E.N.; Glenn, J.M.; Rodgers, C.H.; Kempkes, J.A.; et al. The effect of a digital health coaching and health education protocol on cognition in adults at-risk for Alzheimer’s. GeroScience 2023, 45, 1147–1159. [Google Scholar] [CrossRef]
- Salazar, S.R.; Krivanek, T.; McFeeley, B.; Nicastri, C.; Babazadeh, D.; Daffner, K.; Gale, S. The Brain Health Champion Study: A Health Coaching Intervention with Mobile Technology in Older Adults with Mild Cognitive Impairment or Risk Factors for Dementia (P13-3.004). Neurology 2022, 98. [Google Scholar] [CrossRef]
- Wesselman, L.M.; Hooghiemstra, A.M.; Schoonmade, L.J.; Wit MC de Flier WM van der Sikkes, S.A. Web-Based Multidomain Lifestyle Programs for Brain Health: Comprehensive Overview and Meta-Analysis. JMIR Ment. Health 2019, 6, e12104. [Google Scholar] [CrossRef]
- Markert, C.; Sasangohar, F.; Mortazavi, B.J.; Fields, S. The Use of Telehealth Technology to Support Health Coaching for Older Adults: Literature Review. JMIR Hum. Factors 2021, 8, e23796. [Google Scholar] [CrossRef]
- Strafella, C.; Caputo, V.; Galota, M.R.; Zampatti, S.; Marella, G.; Mauriello, S.; Cascella, R.; Giardina, E. Application of Precision Medicine in Neurodegenerative Diseases. Front. Neurol. 2018, 9, 407937. [Google Scholar] [CrossRef] [PubMed]
- Ryan, L.; Hay, M.; Huentelman, M.J.; Duarte, A.; Rundek, T.; Levin, B.; Soldan, A.; Pettigrew, C.; Mehl, M.R.; Barnes, C.A. Precision Aging: Applying Precision Medicine to the Field of Cognitive Aging. Front. Aging Neurosci. 2019, 11, 128. [Google Scholar] [CrossRef]
- Toups, K.; Hathaway, A.; Gordon, D.; Chung, H.; Raji, C.; Boyd, A.; Hill, B.D.; Hausman-Cohen, S.; Attarha, M.; Chwa, W.J.; et al. Precision Medicine Approach to Alzheimer’s Disease: Successful Pilot Project. J. Alzheimers Dis. 2022, 88, 1411–1421. [Google Scholar] [CrossRef]
- Chenoweth, L.; Stein-Parbury, J.; White, D.; McNeill, G.; Jeon, Y.-H.; Zaratan, B. Coaching in self-efficacy improves care responses, health and well-being in dementia carers: A pre/post-test/follow-up study. BMC Health Serv. Res. 2016, 16, 166. [Google Scholar] [CrossRef]
- Bredesen, D. The End of Alzheimer’s: The First Program to Prevent and Reverse Cognitive Decline; Penguin: New York, NY, USA, 2017. [Google Scholar]
- Bredesen, D.E. Reversal of cognitive decline: A novel therapeutic program. Aging 2014, 6, 707–717. [Google Scholar] [CrossRef]
- Bredesen, D. The End of Alzheimer’s Program: The First Protocol to Enhance Cognition and Reverse Decline at Any Age; Avery: Shinagawa, Tokyo, 2020. [Google Scholar]
- Norwitz, N.G.; Saif, N.; Ariza, I.E.; Isaacson, R.S. Precision Nutrition for Alzheimer’s Prevention in ApoE4 Carriers. Nutrients 2021, 13, 1362. [Google Scholar] [CrossRef]
- Isaacson, R.S.; Hristov, H.; Saif, N.; Hackett, K.; Hendrix, S.; Melendez, J.; Safdieh, J.; Fink, M.; Thambisetty, M.; Sadek, G.; et al. Individualized clinical management of patients at risk for Alzheimer’s dementia. Alzheimers Dement. J. Alzheimers Assoc. 2019, 15, 1588–1602. [Google Scholar] [CrossRef]
- Krivanek, T.; McFeeley, B.; Nicastri, C.M.; Babazadeh, D.; Daffner, K.R.; Gale, S.A. The Brain Health Champion study: A health coaching intervention with mobile technology in older adults with mild cognitive impairment or risk factors for dementia. Alzheimers Dement. 2021, 17, e054068. [Google Scholar] [CrossRef]
- Brenkel, M.; Shulman, K.; Hazan, E.; Herrmann, N.; Owen, A.M. Assessing Capacity in the Elderly: Comparing the MoCA with a Novel Computerized Battery of Executive Function. Dement. Geriatr. Cogn. Disord. Extra 2017, 7, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Gregory, M.A.; Gill, D.P.; Shellington, E.M.; Liu-Ambrose, T.; Shigematsu, R.; Zou, G.; Shoemaker, K.; Owen, A.M.; Hachinski, V.; Stuckey, M.; et al. Group-based exercise and cognitive-physical training in older adults with self-reported cognitive complaints: The Multiple-Modality, Mind-Motor (M4) study protocol. BMC Geriatr. 2016, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Sternin, A.; Burns, A.; Owen, A.M. Thirty-Five Years of Computerized Cognitive Assessment of Aging—Where Are We Now? Diagnostics 2019, 9, 114. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.M.; Nesbitt, B.J. Health Coaching to Improve Healthy Lifestyle Behaviors: An Integrative Review. Am. J. Health Promot. 2010, 25, e1–e12. [Google Scholar] [CrossRef] [PubMed]
- Serio, C.; Gabarda, A.; Uyar-Morency, F.; Silfee, V.; Ludwig, J.; Szigethy, E.; Butterworth, S. Strengthening the Impact of Digital Cognitive Behavioral Interventions Through a Dual Intervention: Proficient Motivational Interviewing—Based Health Coaching Plus In-Application Techniques. JMIR Form. Res. 2022, 6, e34552. [Google Scholar] [CrossRef]
- Schwartz, H.E.M.; Bay, C.P.; McFeeley, B.M.; Krivanek, T.J.; Daffner, K.R.; Gale, S.A. The Brain Health Champion study: Health coaching changes behaviors in patients with cognitive impairment. Alzheimers Dement. Transl. Res. Clin. Intervig. 2019, 5, 771–779. [Google Scholar] [CrossRef]
- Gale, S.; Schwartz, H.; Daffner, K. The Brain Health Champion Study: Promoting Non-Pharmacological Interventions in Cognitive Disorders (S9.003). Neurology 2019, 92. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Felici, E.; Cucchieri, G.; Amabili, G.; Margaritini, A.; Franceschetti, C.; Barboni, I.; Paolini, S.; Civerchia, P.; Raccichini, A.; et al. Results of the Italian RESILIEN-T Pilot Study: A Mobile Health Tool to Support Older People with Mild Cognitive Impairment. J. Clin. Med. 2023, 12, 6129. [Google Scholar] [CrossRef] [PubMed]
- McFeeley, B.; Krivanek, T.; Nicastri, C.M.; Daffner, K.R.; Gale, S.A. The Brain Health Champion (BHC) Study, COVID-19 sub-study: The impact of COVID-19 on behaviors adopted following interventions to promote brain-healthy activities. Alzheimers Dement. 2021, 17, e056392. [Google Scholar] [CrossRef]
- Amabili, G.; Maranesi, E.; Margaritini, A.; Benadduci, M.; Barbarossa, F.; Casaccia, S.; Nap, H.H.; Bevilacqua, R. Usability and Feasibility Assessment of a Social Assistive Robot for the Older People: Results from the GUARDIAN Project. Bioengineering 2024, 11, 20. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (years) | 72 (62–76) |
| Biological Sex | 5 Female, 1 Male |
| Years of Education | 18 (15–20) |
| MoCA $ | 28 (26–30) |
| BMI & | 21 (18–27) |
| APOE-4 risk | 3/4 (n = 5), 3/3 (n = 1) |
| Family history of dementia | Yes (n = 3), No (n = 3) |
| Amyloid status | Positive (n = 1), Negative (n = 5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glatt, R.M.; Amos, A.; Merrill, D.A.; Hodes, J.F.; Wong, C.L.; Miller, K.J.; Siddarth, P. Neurocognitive Effects of an Online Brain Health Program and Weekly Telehealth Support Group in Older Adults with Subjective Memory Loss: A Pilot Study. Geriatrics 2024, 9, 37. https://doi.org/10.3390/geriatrics9020037
Glatt RM, Amos A, Merrill DA, Hodes JF, Wong CL, Miller KJ, Siddarth P. Neurocognitive Effects of an Online Brain Health Program and Weekly Telehealth Support Group in Older Adults with Subjective Memory Loss: A Pilot Study. Geriatrics. 2024; 9(2):37. https://doi.org/10.3390/geriatrics9020037
Chicago/Turabian StyleGlatt, Ryan M., Amylee Amos, David A. Merrill, John F. Hodes, Claudia L. Wong, Karen J. Miller, and Prabha Siddarth. 2024. "Neurocognitive Effects of an Online Brain Health Program and Weekly Telehealth Support Group in Older Adults with Subjective Memory Loss: A Pilot Study" Geriatrics 9, no. 2: 37. https://doi.org/10.3390/geriatrics9020037