

A Proposal for a Multidisciplinary Integrated Oral Health Network for Patients Undergoing Major Orthopaedic Surgery (IOHN-OS)

 ,
,  ,
, 
 , and
, and 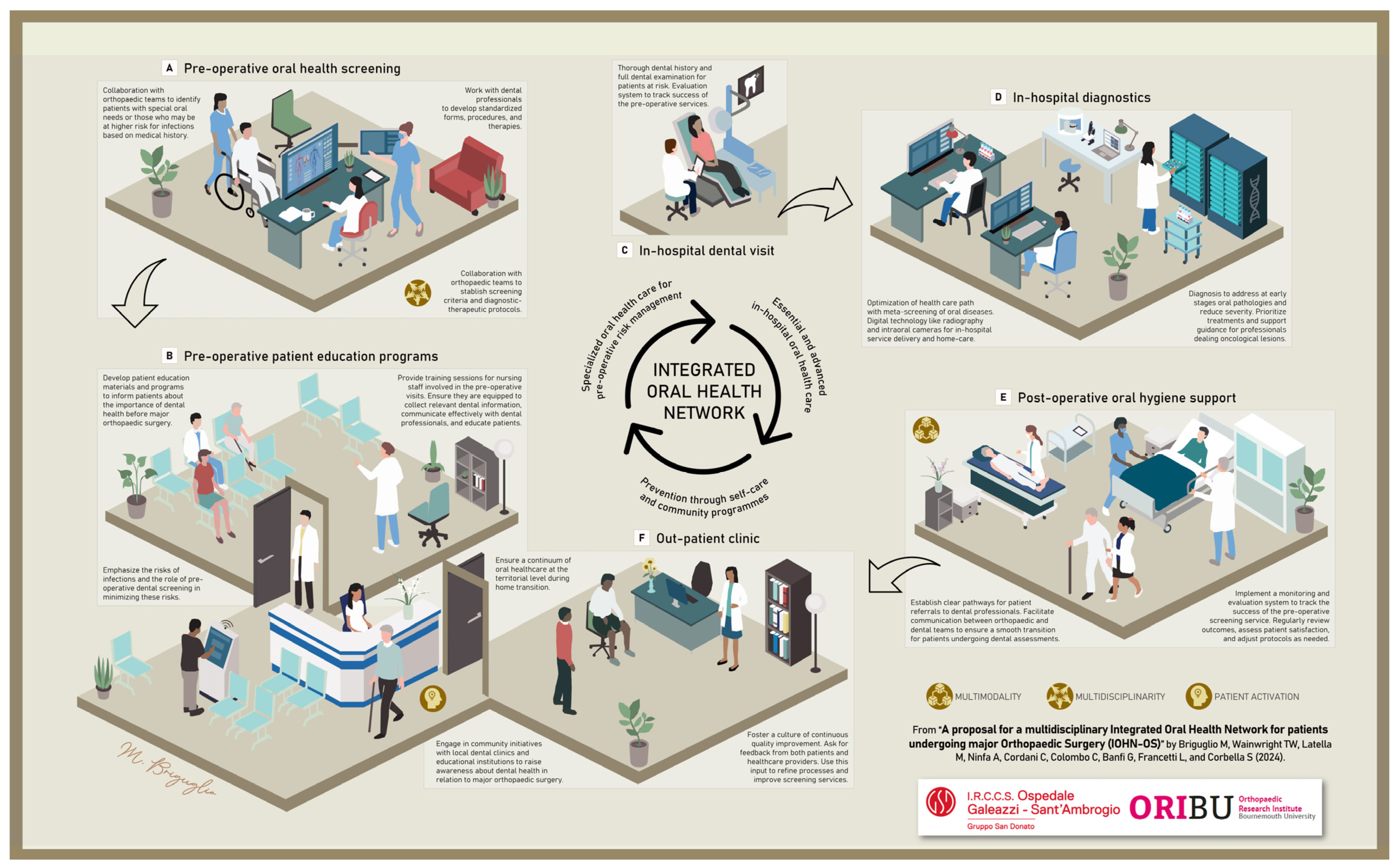{kind=link}
Abstract
:1. Introduction
2. Ageing Poses a Risk to the Oral Cavity of Older Individuals
3. Impact of Medications and Illnesses on the Oral Health of Older Patients
4. The Vicious Cycle between Oral Health and Nutrition in Older Adults
5. Unhealthy Oral Health Conditions Might Pose a Risk to Recovery after Surgery
6. The Integrated Oral Health Network Applied to Orthopaedic Surgery (IOHN-OS)
Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdeen, A.; Della Valle, C.J.; Kendoff, D.; Chen, A.F. The Paradox of Prosthetic Joint Infection and the Microbiome: Are Some Bacteria Actually Helpful? Arthroplast. Today 2022, 13, 116–119. [Google Scholar] [CrossRef]
- Patel, R. Periprosthetic Joint Infection. N. Engl. J. Med. 2023, 388, 251–262. [Google Scholar] [CrossRef]
- Kappenschneider, T.; Maderbacher, G.; Weber, M.; Greimel, F.; Holzapfel, D.; Parik, L.; Schwarz, T.; Leiss, F.; Knebl, M.; Reinhard, J.; et al. Special orthopaedic geriatrics (SOG)—A new multiprofessional care model for elderly patients in elective orthopaedic surgery: A study protocol for a prospective randomized controlled trial of a multimodal intervention in frail patients with hip and knee replacement. BMC Musculoskelet. Disord. 2022, 23, 1079. [Google Scholar] [CrossRef]
- Briguglio, M.; Wainwright, T.W. Nutritional and Physical Prehabilitation in Elective Orthopedic Surgery: Rationale and Proposal for Implementation. Ther. Clin. Risk Manag. 2022, 18, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, N.; de Souto Barreto, P.; Berbon, C.; Mathieu, C.; de Kerimel, J.; Lafont, C.; Takeda, C.; Carrie, I.; Piau, A.; Jouffrey, T.; et al. Implementation of the WHO integrated care for older people (ICOPE) programme in clinical practice: A prospective study. Lancet Healthy Longev. 2022, 3, e394–e404. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 363. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M. The Burdens of Orthopedic Patients and the Value of the HEPAS Approach (Healthy Eating, Physical Activity, and Sleep Hygiene). Front. Med. 2021, 8, 650947. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M.; Cordani, C.; Langella, F.; Perazzo, P.; Pregliasco, F.E.; Banfi, G.; Wainwright, T.W. Why Treat Patients with a Major Orthopaedic Surgery Only to Send Them Back to the Vulnerable Conditions That Made Them Sick in the First Place? A Conceptual Scenario to Improve Patient’s Journey. Int. J. Gen. Med. 2023, 16, 4729–4735. [Google Scholar] [CrossRef] [PubMed]
- Ambiado-Lillo, M.M. Presbyphagia: A Conceptual Analysis of Contemporary Proposals and Their Influences on Clinical Diagnosis. Dysphagia 2024, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kazarina, A.; Kuzmicka, J.; Bortkevica, S.; Zayakin, P.; Kimsis, J.; Igumnova, V.; Sadovska, D.; Freimane, L.; Kivrane, A.; Namina, A.; et al. Oral microbiome variations related to ageing: Possible implications beyond oral health. Arch. Microbiol. 2023, 205, 116. [Google Scholar] [CrossRef]
- Jacobson, A.; Green, E.; Murphy, C. Age-related functional changes in gustatory and reward processing regions: An fMRI study. Neuroimage 2010, 53, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C.; Pedersen, A.M.; Villa, A.; Ekström, J.; Proctor, G.B.; Vissink, A.; Aframian, D.; McGowan, R.; Aliko, A.; Narayana, N.; et al. The functions of human saliva: A review sponsored by the World Workshop on Oral Medicine VI. Arch. Oral. Biol. 2015, 60, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Müller, F.; Chebib, N.; Maniewicz, S.; Genton, L. The Impact of Xerostomia on Food Choices—A Review with Clinical Recommendations. J. Clin. Med. 2023, 12, 4592. [Google Scholar] [CrossRef] [PubMed]
- Ulm, C.; Kneissel, M.; Schedle, A.; Solar, P.; Matejka, M.; Schneider, B.; Donath, K. Characteristic features of trabecular bone in edentulous maxillae. Clin. Oral Implant. Res. 1999, 10, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Zihni Korkmaz, M.; Yemenoğlu, H.; Günaçar, D.N.; Ustaoğlu, G.; Ateş Yildirim, E. The effects of vitamin D deficiency on mandibular bone structure: A retrospective radiological study. Oral Radiol. 2023, 39, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Walczak, A.; Krenz-Niedbała, M.; Łukasik, S. Insight into age-related changes of the human facial skeleton based on medieval European osteological collection. Sci. Rep. 2023, 13, 20564. [Google Scholar] [CrossRef] [PubMed]
- Boven, G.C.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J. Improving masticatory performance, bite force, nutritional state and patient’s satisfaction with implant overdentures: A systematic review of the literature. J. Oral Rehabil. 2015, 42, 220–233. [Google Scholar] [CrossRef]
- N’gom, P.I.; Woda, A. Influence of impaired mastication on nutrition. J. Prosthet. Dent. 2002, 87, 667–673. [Google Scholar] [CrossRef]
- Rohani, B. Oral manifestations in patients with diabetes mellitus. World J. Diabetes 2019, 10, 485–489. [Google Scholar] [CrossRef]
- Ito, K.; Izumi, N.; Funayama, S.; Nohno, K.; Katsura, K.; Kaneko, N.; Inoue, M. Characteristics of medication-induced xerostomia and effect of treatment. PLoS ONE 2023, 18, e0280224. [Google Scholar] [CrossRef]
- Chandna, S.; Bathla, M. Oral manifestations of thyroid disorders and its management. Indian J. Endocrinol. Metab. 2011, 15, S113–S116. [Google Scholar] [CrossRef]
- Panebianco, M.; Marchese-Ragona, R.; Masiero, S.; Restivo, D.A. Dysphagia in neurological diseases: A literature review. Neurol. Sci. 2020, 41, 3067–3073. [Google Scholar] [CrossRef]
- Spencer, H.; Kramer, L.; Norris, C.; Osis, D. Effect of small doses of aluminum-containing antacids on calcium and phosphorus metabolism. Am. J. Clin. Nutr. 1982, 36, 32–40. [Google Scholar] [CrossRef]
- Bell, V.; Rodrigues, A.R.; Antoniadou, M.; Peponis, M.; Varzakas, T.; Fernandes, T. An Update on Drug-Nutrient Interactions and Dental Decay in Older Adults. Nutrients 2023, 15, 4900. [Google Scholar] [CrossRef]
- Beth-Tasdogan, N.H.; Mayer, B.; Hussein, H.; Zolk, O.; Peter, J.U. Interventions for managing medication-related osteonecrosis of the jaw. Cochrane Database Syst. Rev. 2022, 7, CD012432. [Google Scholar] [CrossRef]
- Sheiham, A.; Steele, J. Does the condition of the mouth and teeth affect the ability to eat certain foods, nutrient and dietary intake and nutritional status amongst older people? Public Health Nutr. 2001, 4, 797–803. [Google Scholar] [CrossRef]
- Saleedaeng, P.; Korwanich, N.; Muangpaisan, W.; Korwanich, K. Effect of Dysphagia on the Older Adults’ Nutritional Status and Meal Pattern. J. Prim. Care Community Health 2023, 14, 21501319231158280. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Choi, Y.; Jeong, H.S.; Lee, J.; Sung, J. Effect of different cooking methods on the content of vitamins and true retention in selected vegetables. Food Sci. Biotechnol. 2018, 27, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.S.; Chen, T.C.; Verhoeff, M.C.; Lobbezoo, F.; Trulsson, M.; Fuh, J.L. An umbrella review on the association between factors of oral health and cognitive dysfunction. Ageing Res. Rev. 2023, 93, 102128. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, Y.; Egami, Y.; Matsubara, T.; Koike, G.; Akifusa, S.; Jingu, S.; Yamashita, Y. Relationship between obesity and physical fitness and periodontitis. J. Periodontol. 2010, 81, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Inui, A.; Takahashi, I.; Sawada, K.; Naoki, A.; Oyama, T.; Tamura, Y.; Osanai, T.; Satake, A.; Nakaji, S.; Kobayashi, W. Teeth and physical fitness in a community-dwelling 40 to 79-year-old Japanese population. Clin. Interv. Aging 2016, 11, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Anne Marie, U.; Murererehe, J.; Rehman, M.; Chittilla, M.; Uwambaye, P.; Razzaque, M.S. Oral manifestations of iron imbalance. Front. Nutr. 2023, 10, 1272902. [Google Scholar] [CrossRef] [PubMed]
- Tada, A.; Miura, H. The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 2472. [Google Scholar] [CrossRef]
- Clarke, R.; Grimley Evans, J.; Schneede, J.; Nexo, E.; Bates, C.; Fletcher, A.; Prentice, A.; Johnston, C.; Ueland, P.M.; Refsum, H.; et al. Vitamin B12 and folate deficiency in later life. Age Ageing 2004, 33, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez Gossweiler, A.; Martinez-Mier, E.A. Chapter 6: Vitamins and Oral Health. Monogr. Oral Sci. 2020, 28, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M.; Sirtori, P.; Mangiavini, L.; Buzzi, S.; Cordani, C.; Zerni, M.F.; Wainwright, T.W.; Ursino, N.; Peretti, G.M.; Banfi, G. How Do Older Patients with End-Stage Osteoarthritis of the Hip Eat Prior to Hip Replacement? A Preliminary Snapshot That Highlights a Poor Diet. Nutrients 2023, 15, 4868. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M.; Crespi, T.; Mazzocchi, M.; Petrillo, S.; Turco, C.; De Vecchi, E.; Riso, P.; Porrini, M.; Banfi, G.; Romagnoli, S.; et al. Oral iron powder for prehabilitation in hip and knee arthroplasty: A randomized controlled trial to optimize hemoglobin concentration. Nutr. Clin. Métabolisme 2023, 37, 241–246. [Google Scholar] [CrossRef]
- Briguglio, M.; Sirtori, P.; Mangiavini, L.; Wainwright, T.; Peretti, G.; Banfi, G. Undernutrition, sarcopenia, sarcopenic obesity, and sarcopenic undernutrition: A cross-sectional view on patients before total joint arthroplasty. Orthop. Nurs. 2024. [Google Scholar]
- WHO. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Schmalz, G.; Reuschel, F.; Bartl, M.; Schmidt, L.; Runge, J.; Haak, R.; Goralski, S.; Roth, A.; Ziebolz, D. One Third of Patients before Endoprosthesis Implantation Show an Oral Focus as Potential Source of Infectious Complication-The Value of Pre-Operative Dental Risk Stratification in a German Cohort. J. Clin. Med. 2022, 11, 3686. [Google Scholar] [CrossRef]
- Rakow, A.; Perka, C.; Trampuz, A.; Renz, N. Origin and characteristics of haematogenous periprosthetic joint infection. Clin. Microbiol. Infect. 2019, 25, 845–850. [Google Scholar] [CrossRef]
- Fenske, F.; Kujat, B.; Krause, L.; Meyer, S.; Sander, A.K.; Repmann, J.; Neuhaus, M.; Haak, R.; Roth, A.; Lethaus, B.; et al. Preoperative dental screening can reduce periprosthetic infections of hip and knee endoprostheses in the first month after surgery: Results of a cohort study. Infection 2023, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Parahitiyawa, N.B.; Jin, L.J.; Leung, W.K.; Yam, W.C.; Samaranayake, L.P. Microbiology of odontogenic bacteremia: Beyond endocarditis. Clin. Microbiol. Rev. 2009, 22, 46–64. [Google Scholar] [CrossRef]
- Kohler, J.G.; Holte, A.J.; Glass, N.A.; Bedard, N.A.; Brown, T.S. Dental Screening in Elective Total Joint Arthroplasty: Risk Factors for Failure. J. Arthroplast. 2021, 36, 1548–1550. [Google Scholar] [CrossRef] [PubMed]
- De Sam Lazaro, S.L.; Nitschke Durben, A.M.; Kline, J.J. Barriers and Opportunities to Support the Oral Health of Older Adults: A Rapid Review of Health Policy and Systems. Int. J. Aging Hum. Dev. 2023, 96, 51–62. [Google Scholar] [CrossRef]
- Kossioni, A.E. Is Europe prepared to meet the oral health needs of older people? Gerodontology 2012, 29, e1230–e1240. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Ziebolz, D. The hypotheses of oral disease-associated perioprosthetic joint infections to understand the role of oral health for endoprostheses—A narrative review. Spec. Care Dentist 2023, 44, 328–338. [Google Scholar] [CrossRef]
- Briguglio, M.; Crespi, T.; Langella, F.; Riso, P.; Porrini, M.; Scaramuzzo, L.; Bassani, R.; Brayda-Bruno, M.; Berjano, P. Perioperative Anesthesia and Acute Smell Alterations in Spine Surgery: A “Sniffing Impairment” Influencing Refeeding? Front. Surg. 2022, 9, 785676. [Google Scholar] [CrossRef]
- Teramoto, S. The current definition, epidemiology, animal models and a novel therapeutic strategy for aspiration pneumonia. Respir. Investig. 2022, 60, 45–55. [Google Scholar] [CrossRef]
- Schmitter, M.; Essig, M.; Seneadza, V.; Balke, Z.; Schröder, J.; Rammelsberg, P. Prevalence of clinical and radiographic signs of osteoarthrosis of the temporomandibular joint in an older persons community. Dentomaxillofac. Radiol. 2010, 39, 231–234. [Google Scholar] [CrossRef]
- Jockusch, J.; Hahnel, S.; Sobotta, B.B.A.J.; Nitschke, I. The Effect of a Masticatory Muscle Training Program on Chewing Efficiency and Bite Force in People with Dementia. Int. J. Environ. Res. Public Health 2022, 19, 3778. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, I.; Nitschke, S.; Haffner, C.; Sobotta, B.A.J.; Jockusch, J. On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process. Int. J. Environ. Res. Public Health 2022, 19, 6148. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Lenzen, C.; Reuschel, F.; Fenske, F.; Haak, R.; Goralski, S.; Roth, A.; Ziebolz, D. Lack of oral health awareness and interdisciplinary dental care: A survey in patients prior to endoprosthesis and orthopaedic centres in Germany. BMC Oral Health 2023, 23, 92. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mobile Technologies for Oral Health: An Implementation Guide; WHO: Geneva, Switzerland, 2021. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briguglio, M.; Wainwright, T.W.; Latella, M.; Ninfa, A.; Cordani, C.; Colombo, C.; Banfi, G.; Francetti, L.; Corbella, S. A Proposal for a Multidisciplinary Integrated Oral Health Network for Patients Undergoing Major Orthopaedic Surgery (IOHN-OS). Geriatrics 2024, 9, 39. https://doi.org/10.3390/geriatrics9020039
Briguglio M, Wainwright TW, Latella M, Ninfa A, Cordani C, Colombo C, Banfi G, Francetti L, Corbella S. A Proposal for a Multidisciplinary Integrated Oral Health Network for Patients Undergoing Major Orthopaedic Surgery (IOHN-OS). Geriatrics. 2024; 9(2):39. https://doi.org/10.3390/geriatrics9020039
Chicago/Turabian StyleBriguglio, Matteo, Thomas W. Wainwright, Marialetizia Latella, Aurora Ninfa, Claudio Cordani, Cecilia Colombo, Giuseppe Banfi, Luca Francetti, and Stefano Corbella. 2024. "A Proposal for a Multidisciplinary Integrated Oral Health Network for Patients Undergoing Major Orthopaedic Surgery (IOHN-OS)" Geriatrics 9, no. 2: 39. https://doi.org/10.3390/geriatrics9020039