Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
2. Lowering CVD Risk: Will Only Weight Loss Do?
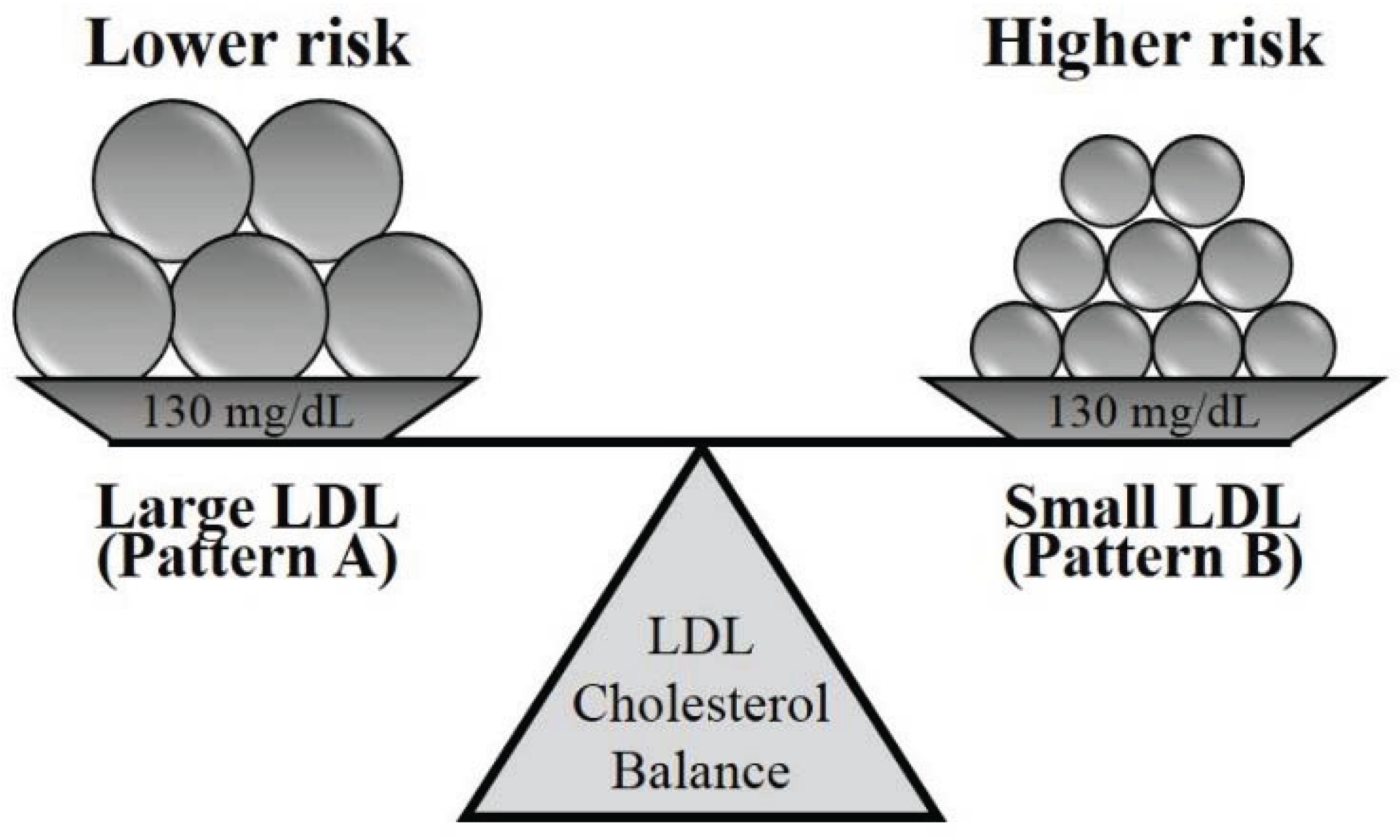
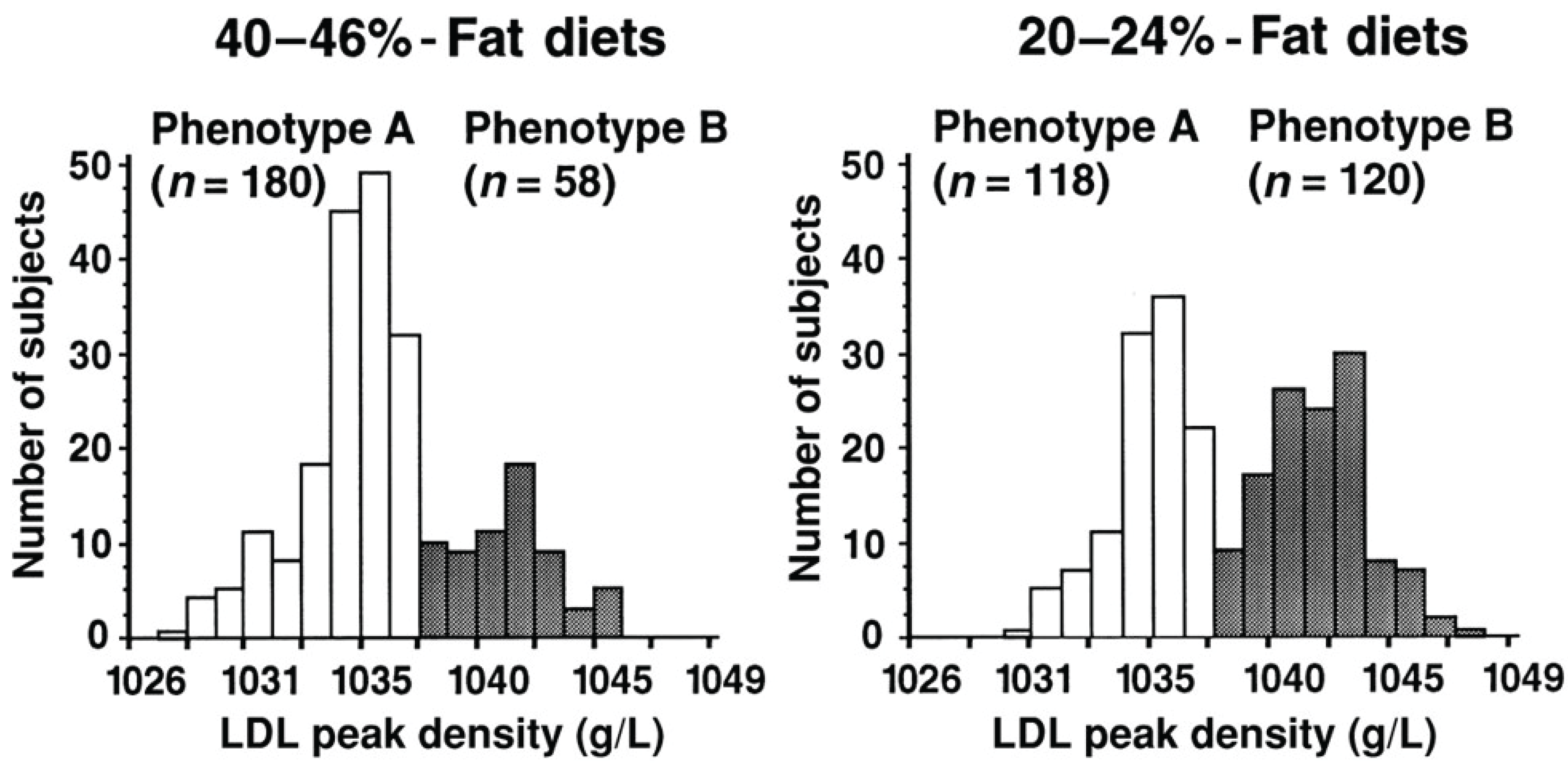
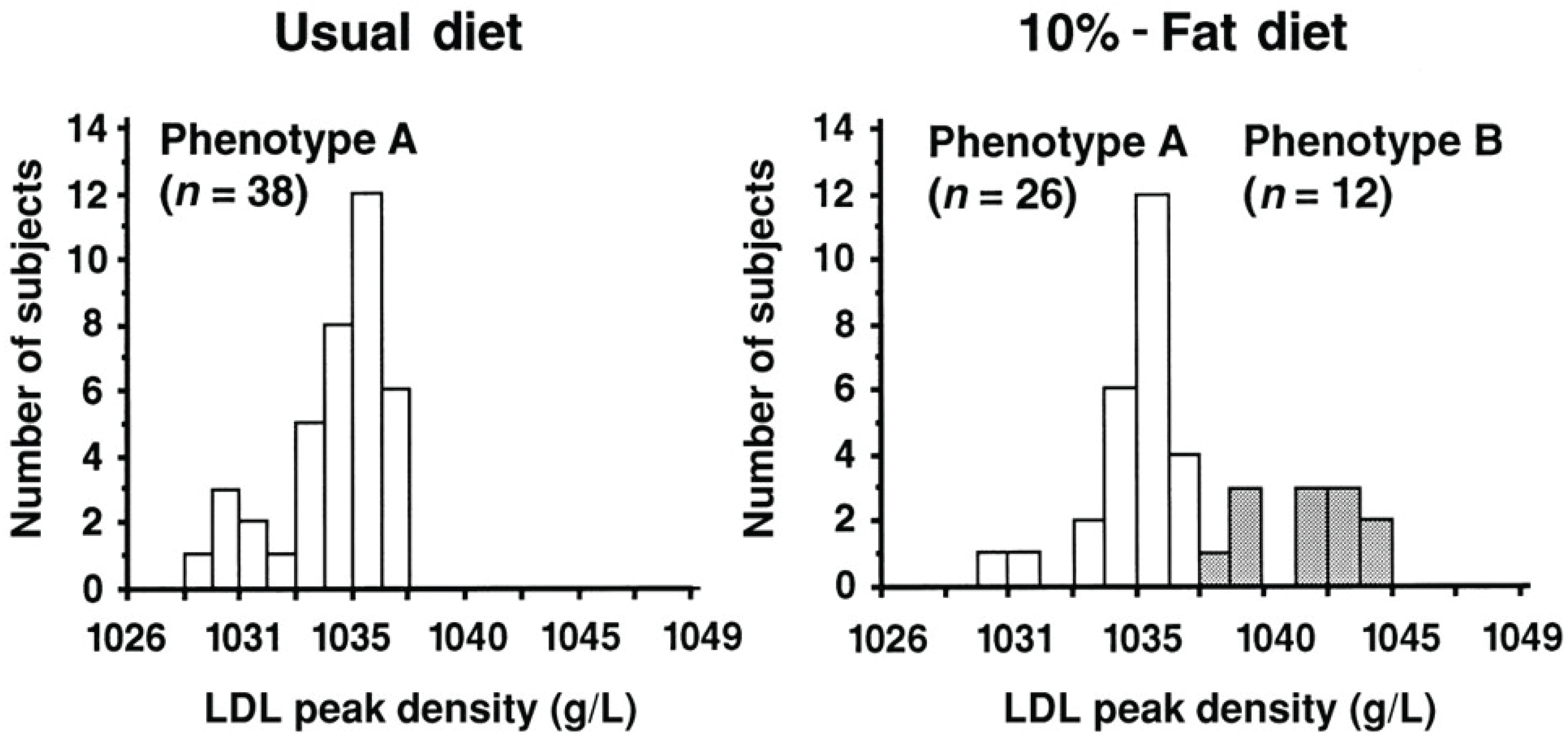
3. Lipid Profile Patterns



4. Saturated Fat
5. Protein Content
6. Literature Shortcomings
7. Conclusion
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011.
- Centers for Disease Control and Prevention. Heart Disease and Stroke Prevention: Addressing the Nation’s Leading Killers. 2011. Available online: http://www.cdc.gov/chronicdisease/resources/publications/aag/pdf/2011/heart-disease-and-stroke-aag-2011.pdf (accessed on 13 January 2014). [Google Scholar]
- Health Canada. Canada’s Food Guide. 2011. Available online: http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php (accessed on 28 November 2013).
- The American Heart Association’s Diet and Lifestyle Recommendations. Available online: http://www.heart.org/HEARTORG/GettingHealthy/Diet-and-Lifestyle-Recommendations_UCM_305855_Article.jsp (accessed on 20 November 2013).
- Austin, M.A. Epidemiology of hypertriglyceridemia and cardiovascular disease. Am. J. Cardiol. 1999, 83, 13–16. [Google Scholar] [CrossRef]
- Hokanson, J.E.; Austin, M.A. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: A metaanalysis of population-based prospective studies. Eur. J. Prev. Cardiol. 1996, 3, 213–219. [Google Scholar] [CrossRef]
- Shankar, A.; Mitchell, P.; Rochtchina, E.; Wang, J.J. The association between circulating while blood cell count, triglyceride level and cardiovascular and all-cause mortality: Population-based cohort study. Atherosclerosis 2007, 192, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Gould, A.L.; Davies, G.M.; Alemao, E.; Yin, D.D.; Cook, J.R. Cholesterol reduction yields clinical benefits: meta-analysis including recent trials. Clin. Therapeut. 2007, 29, 778–794. [Google Scholar] [CrossRef]
- Manninen, V.; Tenkanen, L.; Koskinen, P.; Huttunen, J.K.; Manttari, M.; Heinonen, O.P.; Frick, M.H. Joint effects of serum triglyceride and ldl cholesterol and hdl cholesterol concentrations on coronary heart disease risk in the Helsinki heart study. Implications for treatment. Circulation 1992, 85, 37–45. [Google Scholar] [CrossRef]
- Briel, M.; Ferreira-Gonzalez, I.; You, J.J.; Karanicolas, P.J.; Akl, E.A.; Wu, P.; Blechacz, B.; Bassler, D.; Wei, X.; Sharman, A.; et al. Association between change in high density lipoprotein cholesterol and cardiovascular disease morbidity and mortality: Systematic review and meta-regression analysis. Brit. Med. J. 2009, 338. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Alaupovic, P.; Moye, L.A.; Cole, T.G.; Sussex, B.; Stampfer, M.J.; Pfeffer, M.A.; Braunwald, E. Vldl, Apolipoproteins v, cIII, and e, and risk of recurrent coronary events in the cholesterol and recurrent events (care) trial. Circulation 2000, 102, 1186–1892. [Google Scholar] [CrossRef]
- Van Gaal, L.F.; Wauters, M.A.; De Leeuw, I.H. The beneficial effects of modest weight loss on cardiovascular risk factors. Int. J. Obes. Relat. Metab. Disorders 1997, 21, S5–S9. [Google Scholar]
- Hu, T.; Mills, K.T.; Yao, L.; Demanelis, K.; Eloustaz, M.; Yancy, W.S.; Kelly, T.N., Jr.; Bazzano, L.A.; et al. Effects of low-carbohydrate diets versus low-fat diets on metabolic risk factors: A meta-analysis of randomized controlled clinical trials. Am. J. Epidemiol. 2012, 176, S44–S54. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; McManus, K.; Champagne, C.M.; Bishop, L.M.; Laranjo, N. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. New England J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. New England J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef]
- Bueno, N.B.; Vieira de Melo, I.S.; Lima de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Brit. J. Nutr. 2013, 1178, 1178–1187. [Google Scholar] [CrossRef]
- Krieger, J.W.; Sitren, H.S.; Daniels, M.J.; Langkamp-Henken, B. Effects of variation in protein and carbohydrate intake on body mass and composition during restriction: A meta-regression. Am. J. Clin. Nutr. 2006, 83, 260–274. [Google Scholar]
- Volek, J.S.; Sharman, M.J.; Gómez, A.L.; DiPasquale, C.; Roti, M.; Pumerantz, A.; Kraemer, W.J. Comparison of a very low-carbohydrate and low-fat diet on fasting lipids, ldl subclasses, insulin resistance, and postprandial lipemic responses in overweight women. J. Am. College Nutr. 2004, 23, 177–184. [Google Scholar] [CrossRef]
- Howard, B.V.; Van Horn, L.; Hsia, J.; Manson, J.E.; Stefanick, M.L.; Wassertheil-Smoller, S.; Kotchen, J.M. Low-fat dietary pattern and risk of cardiovascular disease: The women’s health initiative randomized controlled modification trial. J. Am. Med. Assoc. 2006, 295, 655–666. [Google Scholar] [CrossRef]
- Brehm, B.J.; Seeley, R.J.; Daniels, S.R.; D’Alessio, D.A. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J. Clin. Endocrinol. Metab. 2003, 88, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Ruth, M.R.; Port, A.M.; Shah, M.; Bourland, A.C.; Istfan, N.W.; Nelson, K.P.; Gokce, N.; Apovian, C.M. Consuming a hypocaloric high fat low carbohydrate diet for 12 weeks lowers c-reactive protein, and raises serum adiponectin and high density lipoprotein-cholesterol in obese subjects. Metabolism 2013, 62, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Comparison of effects of long-term low-fat vs. high-fat diets on blood lipid levels in overweight or obese patients: A systematic review and meta-analysis. J. Acad. Nutr. Diet. 2013, 113, 1640–1661. [Google Scholar] [PubMed]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a dash-style diet and risk of coronary heart disease and stroke in women. Arch. Inter. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Obarzanek, E.; Sacks, F.M.; Vollmer, W.M.; Bray, G.A.; Miller, E.R., III; Lin, P.-H.; Karanja, N.M.; Most-Windhauser, M.M.; Moore, T.J.; Swain, J.F.; Bales, C.W.; Proschan, M.A.; DASH Research Group. Effects on blood lipids of a blood pressure-lowering diet; the dietary approaches to stop hypertension (dash) trial. Am. J. Clin. Nutr. 2001, 74, 80–89. [Google Scholar]
- Howard, B.V.; Curb, J.D.; Eaton, C.B.; Kooperberg, C.; Ockene, J.; Kostis, J.B.; Pettinger, M.; Rajkovic, A.; Robinson, J.G.; Rossouw, J.; Sarto, G.; Shikany, J.M.; Van Horn, L. Low-fat dietary pattern and lipoprotein risk factors: The women’s health initiative dietary modification trial. Am. J. Clin. Nutr. 2010, 91, 860–874. [Google Scholar]
- Dreon, D.M.; Fernstrom, H.A.; Williams, P.T.; Krauss, R.M. A very-low-fat diet is not associated with improved lipoprotein profiles in men with a predominance of large, low-density lipoproteins. Am. J. Clin. Nutr. 1999, 69, 411–418. [Google Scholar]
- Gardner, C.D.; Kiazand, A.; Alhassan, S.; Stafford, R.S.; Balise, R.R.; Kraemer, H.C.; King, A.C. Comparison of the atkins, zone, ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women. J. Am. Med. Assoc. 2007, 297, 969–976. [Google Scholar] [CrossRef]
- Austin, M.A.; Breslow, J.L.; Hennekens, C.H.; Buring, J.E.; Willet, W.C.; Krauss, R.M. Low-density lipoprotein subclass patterns and risk of myocardial infarction. J. Am. Med. Assoc. 1988, 260, 1917–1921. [Google Scholar] [CrossRef]
- Austin, M.A.; King, M.C.; Vranizan, K.M.; Krauss, R.M. Atherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease risk. Circulation 1990, 82, 495–506. [Google Scholar] [CrossRef]
- Williams, P.T.; Krauss, R.M. Associations of age, adiposity, menopause, and alcohol intake with low-density lipoprotein subclasses. Arterioscl. Thromb. Vascul. Biol. 1997, 17, 1082–1090. [Google Scholar]
- Dreon, D.M.; Fernstrom, H.A.; Miller, B.; Krauss, R.M. Low-density lipoprotein subclass patterns and lipoprotein response to a reduced-fat diet in men. J. Fed. Am. Soc. Exper. Biol. 1994, 8, 121–126. [Google Scholar]
- Carmena, R.; Duriez, P.; Fruchart, J.-C. Atherogenic lipoprotein particles in atherosclerosis. Circulation 2004, 109 (23 Suppl 1), III2–III7. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Campos, H.; Moye, L.A.; Sacks, F.M. Ldl containing Apolipoprotein cIII is an independent risk factor for coronary events in diabetic patients. Atheroscl. Thromb. Vascul. Biol. 2003, 23, 853–858. [Google Scholar] [CrossRef]
- Krauss, R.M.; Blanche, P.J.; Rawlings, R.S.; Fernstrom, H.S.; Williams, P.T. Separate effects of reduced carbohydrate intake and weight loss on atherogenic dyslipidemia. Am. J. Clin. Nutr. 2006, 83, 1025–1031. [Google Scholar] [PubMed]
- Faghihnia, N.; Mangravite, L.M.; Chiu, S.; Bergeron, N.; Krauss, R.M. Effects of dietary saturated fat on ldl subclasses and Apolipoprotein cIII in men. Eur. J. Clin. Nutr. 2012, 66, 1229–1233. [Google Scholar] [CrossRef] [PubMed]
- Scholl, J. Traditional dietary recommendations for the prevention of cardiovascular disease: Do they meet the needs of our patients? Cholesterol 2012. [Google Scholar] [CrossRef]
- Jakobsen, M.U.; Overvad, K.; Dyerberg, J.; Schroll, M.; Heitmann, B.L. Dietary fat and risk of coronary heart disease: Possible effect modification by gender and age. Am. J. Epidemiol. 2004, 160, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Rimm, E.; Colditz, G.A.; Rosner, B.A.; Willett, W.C. Dietary fat intake and the risk of coronary heart disease in women. New England J. Med. 1997, 337, 1491–1499. [Google Scholar] [CrossRef]
- Jakobsen, M.U.; O’Reilly, E.J.; Heitmann, B.L.; Pereira, M.A.; Bälter, K.; Fraser, G.E.; Ascherio, A. Major types of dietary fat and risk of coronary heart disease: A pooled analysis of 11 cohort studies. Am. J. Clin. Nutr. 2009, 89, 1425–1432. [Google Scholar]
- Cuchel, M.; Schwab, U.S.; Jones, J.H.; Vogel, S.; Lammi-Keefe, C.; Li, Z.; Lichtenstein, A.H. Impact of hydrogenated fat consumption on endogenous cholesterol synthesis of low-density lipoprotein to oxidation in moderately hypercholesterolemic individuals. Metabolism 1996, 45, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Mensink, R.P.; Zock, P.L.; Kester, A.D.M.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to hdl cholesterol and on serum lipids and Apolipoproteins: A meta-analysis of 60 controlled trials. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am. J. Clin. Nutr. 2010, 91, 535–546. [Google Scholar] [CrossRef]
- Frantz, I.D.; Dawson, E.A., Jr.; Ashman, P.L.; Gatewood, L.C.; Bartsch, G.E.; Kuba, K.; Brewer, E.R. Test of effect of lipid lowering by diet on cardiovascular risk. The Minnesota coronary survey. Arterioscl. Thromb. Vascul. Biol. 1989, 9, 129–135. [Google Scholar] [CrossRef]
- Appel, L.J.; Sacks, F.M.; Obarzanek, E.; Swain, J.F.; Miller, E.R.; Conlin, P.R.; Erlinger, T.P.; Rosner, B.A.; Laranjo, N.M.; Charleston, J.; McCarron, P.; Bishop, L.M.; OmniHeart Collaborative Research Group. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: Results of the omniheart randomized trial. J. Am. Med. Assoc. 2005, 294, 2455–2464. [Google Scholar] [CrossRef]
- Furtado, J.D.; Campos, H.; Appel, L.J.; Miller, E.R.; Laranjo, N.; Carey, V.J.; Sacks, F.M. Effect of protein, unsaturated fat, and carbohydrate intakes on plasma Apolipoprotein b and vldl and ldl containing Apolipoprotein c-III: Results from the omniheart trial. Am. J. Clin. Nutr. 2008, 87, 1623–1630. [Google Scholar]
- Noakes, M.; Keogh, J.B.; Foster, P.R.; Clifton, P.M. Effect of an energy-restricted, high-protein, low-fat diet relative to a conventional high-carbohydrate, low-fat diet on weight loss, body composition, nutritional status, and markers of cardiovascular health in obese women. Am. J. Clin. Nutr. 2005, 81, 1298–1306. [Google Scholar] [PubMed]
- St Sachiko, T.J.; Howard, B.V.; Prewitt, E.; Bovee, V.; Bazzarre, T.; Eckel, R.H.; Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Dietary protein and weight reduction: A statement for healthcare professionals from the nutrition committee of the council on nutrition, physical activity, and metabolism of the American heart association. Circulation 2001, 104, 1869–1874. [Google Scholar]
- Fung, T.T.; van Dam, R.M.; Hankinson, S.E.; Willett, W.C. Low-carbohydrate diets and all-cause and cause-specific mortality: Two cohort studies. Ann. Inter. Med. 2010, 153, 289–298. [Google Scholar] [CrossRef]
- Kipnis, V.; Midthune, D.; Freedman, L.; Bingham, S.; Day, N.E.; Riboli, E.; Ferrari, P.; Carroll, R.J. Part E. New statistical approaches to dealing with bias associated with dietary data: Bias in dietary-report instruments and its implications for nutritional epidemiology. Public Health Nutr. 2002, 5, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, V.; Subar, A.F.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Carroll, R.J. Structure of dietary measurement error: Results of the open biomarker study. Am. J. Epidemiol. 2003, 158, 14–21. [Google Scholar] [CrossRef]
- Siebelink, E.; Geelen, A.; de Vries, J.H.M. Self-reported energy intake by FFQ compared with actual energy intake to maintain body weight in 516 adults. Brit. J. Nutr. 2011, 106, 274–281. [Google Scholar] [CrossRef]
- Zheng, C.; Khoo, C.; Ikewaki, K.; Sacks, F.M. Rapid turnover of Apolipoprotein C-III-containing triglyceride-rich lipoproteins contributing to the formation of ldl subfractions. J. Lipid Res. 2007, 48, 1190–1203. [Google Scholar]
- Campos, H.; Dreon, D.M.; Krauss, R.M. Associations of hepatic and lipoprotein lipase activities with changes in dietary composition and low density lipoprotein subclasses. J. Lipid Res. 1995, 36, 462–472. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daoud, E.; Scheede-Bergdahl, C.; Bergdahl, A. Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease. J. Cardiovasc. Dev. Dis. 2014, 1, 201-213. https://doi.org/10.3390/jcdd1030201
Daoud E, Scheede-Bergdahl C, Bergdahl A. Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease. Journal of Cardiovascular Development and Disease. 2014; 1(3):201-213. https://doi.org/10.3390/jcdd1030201
Chicago/Turabian StyleDaoud, Emilie, Celena Scheede-Bergdahl, and Andreas Bergdahl. 2014. "Effects of Dietary Macronutrients on Plasma Lipid Levels and the Consequence for Cardiovascular Disease" Journal of Cardiovascular Development and Disease 1, no. 3: 201-213. https://doi.org/10.3390/jcdd1030201