
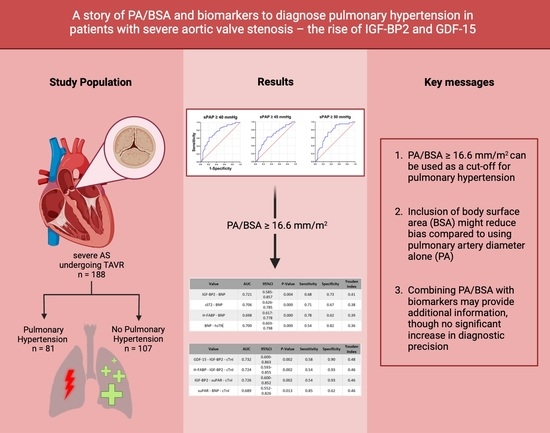
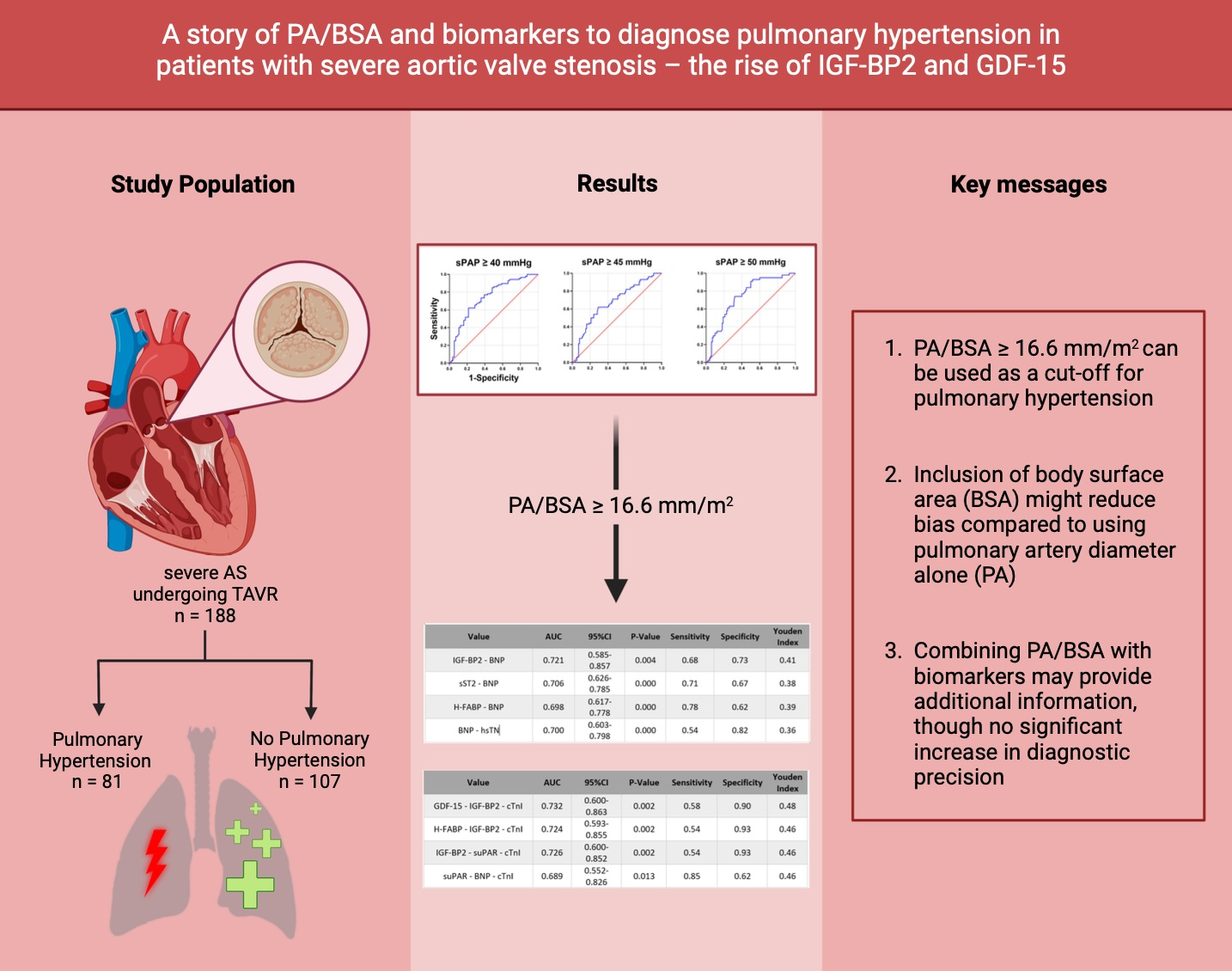
A Story of PA/BSA and Biomarkers to Diagnose Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—The Rise of IGF-BP2 and GDF-15
 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Transthoracic Echocardiography
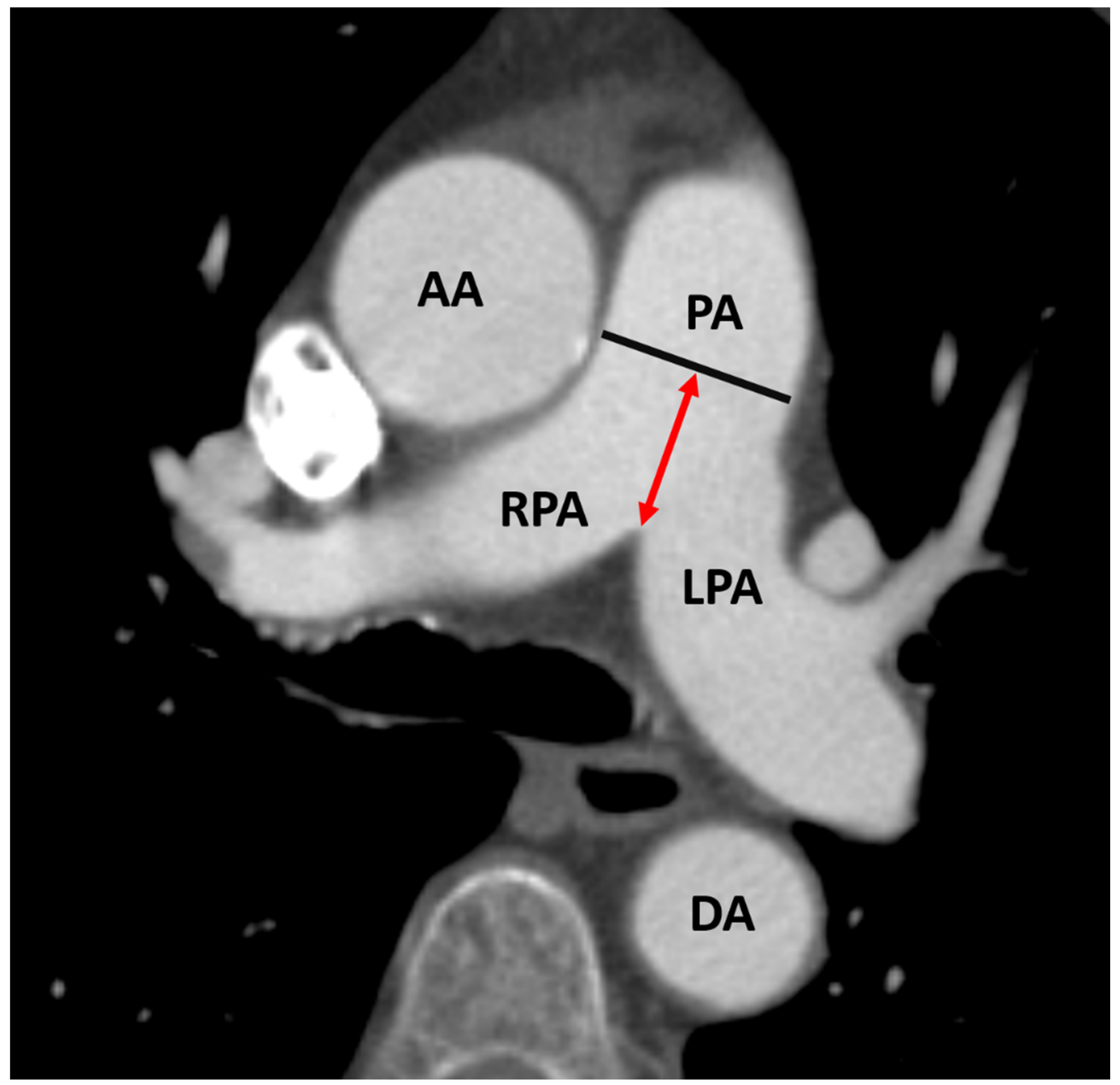
2.3. CTA Protocol and Measurement of PA Diameter for PH Assessment
2.4. Biomarker Analysis
2.5. Statistical Analysis
3. Results
3.1. Sample Size Calculation
3.2. Study Cohort
3.3. Baseline Characteristics
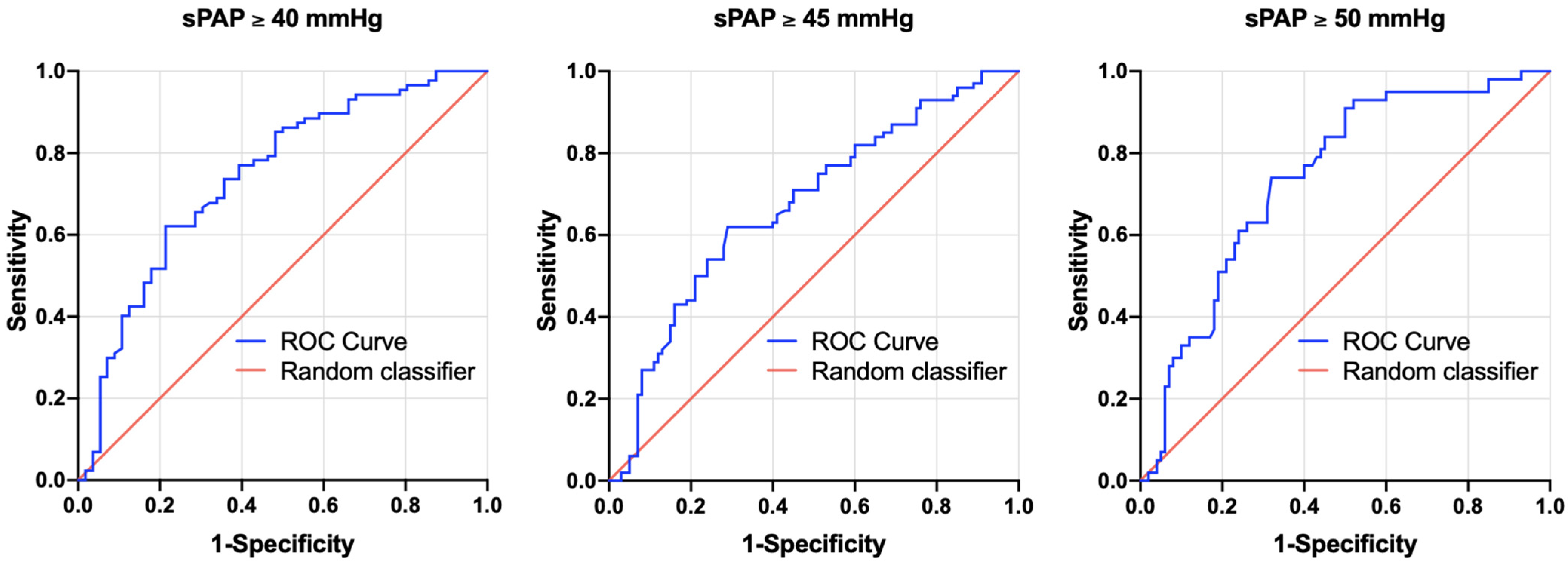
3.4. AUROC Results—sPAP vs. PA/BSA Ratio
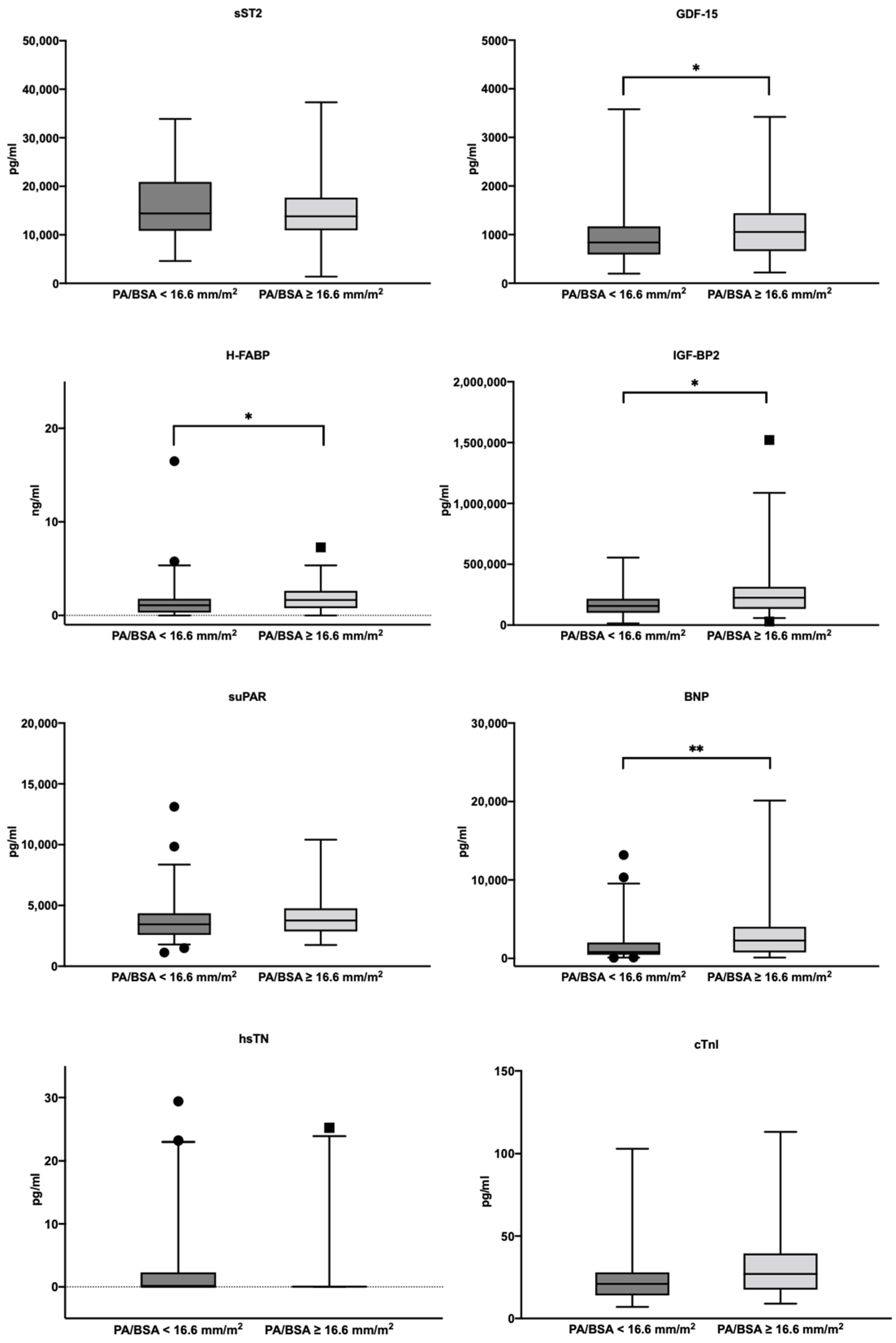
3.5. Biomarker Concentrations in the Study Cohort
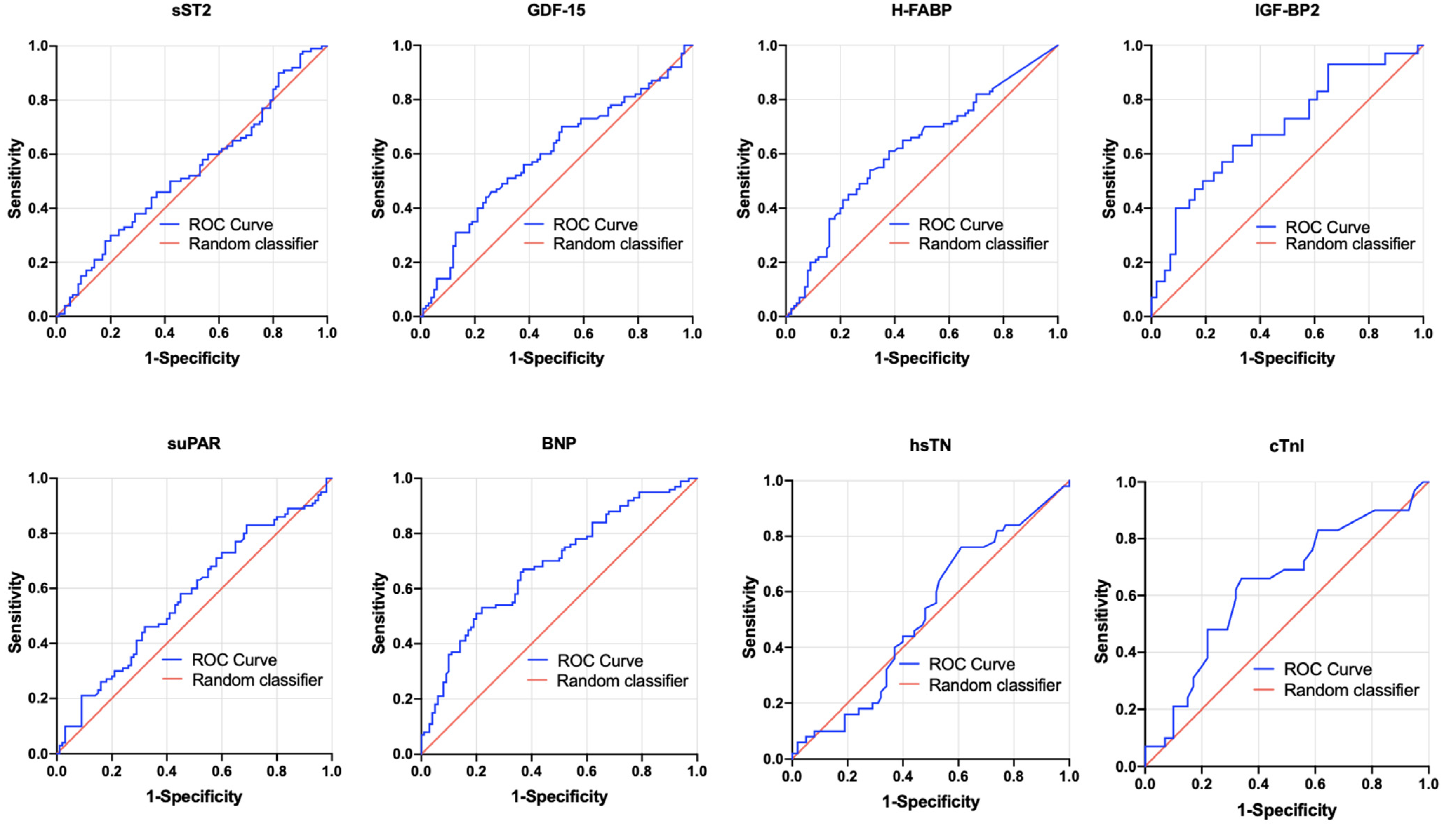
3.6. AUROC Results—PA/BSA vs. Singular Biomarkers
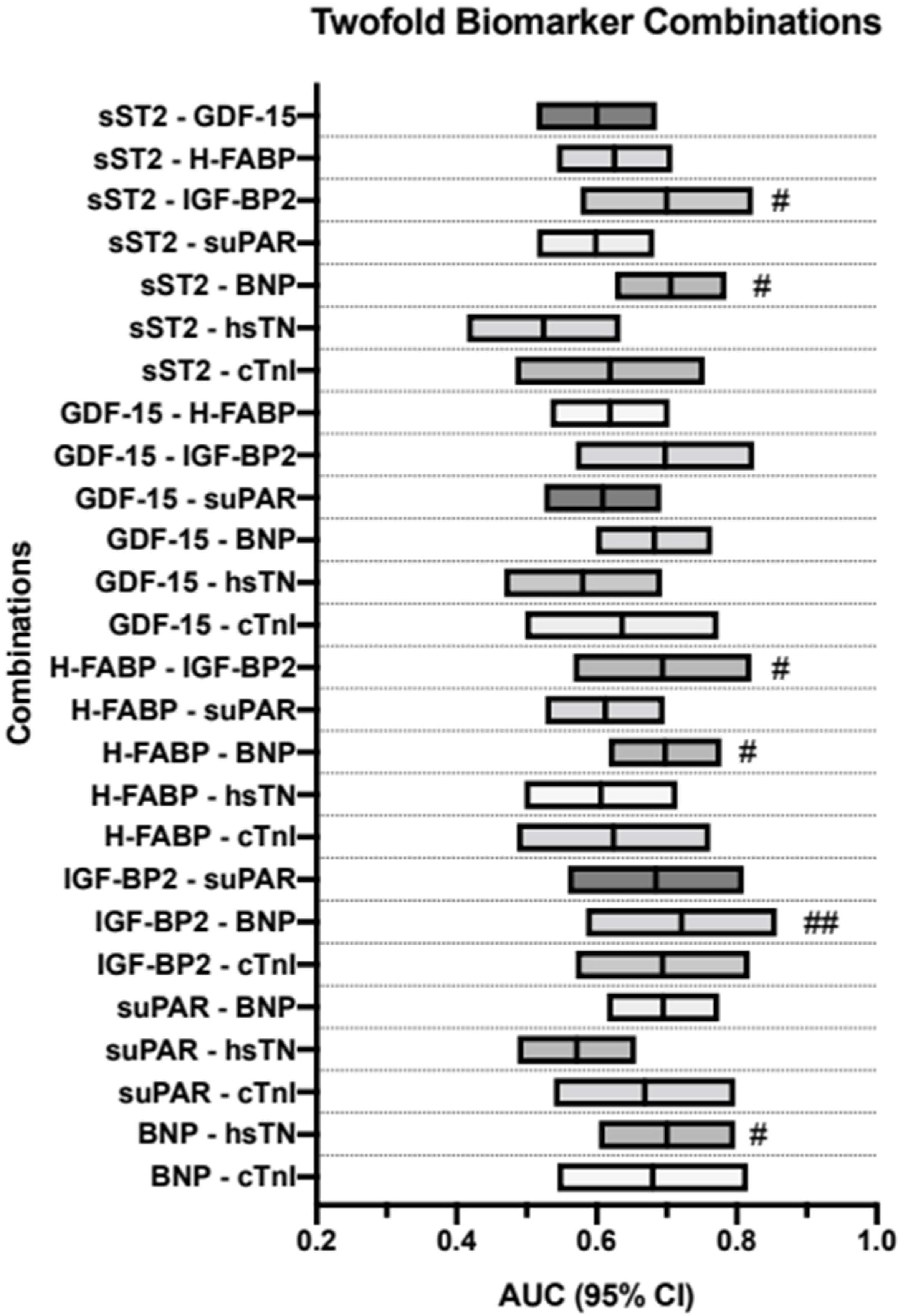
3.7. AUROC Results—PA/BSA vs. Dual-Biomarker Combinations
3.8. AUROC Results—PA/BSA vs. Triple-Biomarker Combinations
3.9. Kaplan–Meier Analysis
4. Discussion
4.1. Can a PA/BSA ≥ 16.6 mm/m2 Be Used as Evidence for PH?
4.2. Can a PA/BSA ≥ 16.6 mm/m2 Be Used as a Prognostic Factor?
4.3. Can a PA/BSA ≥ 16.6 mm/m2 Be Used Together with Biomarkers to Gain Additional Information?
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | aortic stenosis |
| AUC | area under the curve |
| AUROC | area under the receiver operator characteristics |
| BNP | brain natriuretic peptide |
| BSA | body surface area |
| cTnI | cardiac troponin I |
| ESC | European Society of Cardiology |
| GDF-15 | growth/differentiation factor-15 |
| H-FABP | heart-type fatty acid-binding protein |
| hsTN | high-sensitive troponin |
| IGF-BP2 | insulin-like growth factor binding protein 2 |
| IQR | interquartile range |
| IVC | inferior vena cava |
| LVEF | left ventricular ejection fraction |
| PA | pulmonary artery |
| PA/BSA | pulmonary artery diameter/body surface area |
| PH | pulmonary hypertension |
| RAP | right atrial pressure |
| SD | standard deviation |
| sPAP | systolic pulmonary artery pressure |
| sST2 | soluble suppression of tumorigenesis-2 |
| suPAR | soluble urokinase-type plasminogen activator receptor |
| TRV | tricuspid regurgitant jet velocity |
| YI | Youden Index |
References
- Masri, A.; Gleason, T.G.; Lee, J.S.; Cavalcante, J.L. Pulmonary Hypertension Persistency in Severe Aortic Stenosis Patients Treated With TAVR. JACC Cardiovasc. Imaging 2019, 12, 1293–1294. [Google Scholar] [CrossRef] [PubMed]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Stähli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; Maisano, F.; et al. Pulmonary Hypertension in Patients With Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR. JACC Cardiovasc. Imaging 2018, 12, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Schewel, J.; Schlüter, M.; Schmidt, T.; Kuck, K.; Frerker, C.; Schewel, D. Correlation between Doppler echocardiography and right heart catheterization assessment of systolic pulmonary artery pressure in patients with severe aortic stenosis. Echocardiography 2020, 37, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, R.M.; Matsumura, Y.; Yamano, T.; Greenberg, N.; Thomas, J.D.; Shiota, T. Relation of Left Atrial Dysfunction to Pulmonary Artery Hypertension in Patients With Aortic Stenosis and Left Ventricular Systolic Dysfunction. Am. J. Cardiol. 2010, 106, 409–416. [Google Scholar] [CrossRef]
- Nijenhuis, V.; Huitema, M.; Vorselaars, V.; Swaans, M.; de Kroon, T.; van der Heyden, J.; Rensing, B.; Heijmen, R.; Berg, J.T.; Post, M. Echocardiographic pulmonary hypertension probability is associated with clinical outcomes after transcatheter aortic valve implantation. Int. J. Cardiol. 2016, 225, 218–225. [Google Scholar] [CrossRef]
- Bishu, K.; Suri, R.M.; Nkomo, V.T.; Kane, G.C.; Greason, K.L.; Reeder, G.S.; Mathew, V.; Holmes, D.R.; Rihal, C.S.; Melduni, R.M. Prognostic Impact of Pulmonary Artery Systolic Pressure in Patients Undergoing Transcatheter Aortic Valve Replacement for Aortic Stenosis. Am. J. Cardiol. 2014, 114, 1562–1567. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; Conrotto, F.; Salizzoni, S.; Rossi, M.L.; Nijhoff, F.; Gasparetto, V.; Barbanti, M.; Mennuni, M.; Omedè, P.; Marra, W.G.; et al. Incidence, predictors, and impact on prognosis of systolic pulmonary artery pressure and its improvement after transcatheter aortic valve implantation: A multicenter registry. J. Am. Coll. Cardiol. 2015, 27, 114–119. [Google Scholar]
- Lancellotti, P.; Magne, J.; Donal, E.; O’Connor, K.; Dulgheru, R.; Rosca, M.; Pierard, L.A. Determinants and Prognostic Significance of Exercise Pulmonary Hypertension in Asymptomatic Severe Aortic Stenosis. Circulation 2012, 126, 851–859. [Google Scholar] [CrossRef] [Green Version]
- Durmaz, T.; Ayhan, H.; Keleş, T.; Aslan, A.N.; Kasapkara, H.A.; Sari, C.; Bilen, E.; Bayram, N.A.; Akçay, M.; Bozkurt, E. The Effect of Transcatheter Aortic Valve Implantation on Pulmonary Hypertension. Echocardiography 2014, 32, 1057–1063. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Hear. J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef]
- O’Sullivan, C.J.; Montalbetti, M.; Zbinden, R.; Kurz, D.J.; Bernheim, A.M.; Liew, A.; Meyer, M.R.; Tuller, D.; Eberli, F.R. Screening For Pulmonary Hypertension With Multidetector Computed Tomography Among Patients With Severe Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation. Front. Cardiovasc. Med. 2018, 5, 63. [Google Scholar] [CrossRef]
- Turner, V.L.; Jubran, A.; Kim, J.B.; Maret, E.; Moneghetti, K.J.; Haddad, F.; Amsallem, M.; Codari, M.; Hinostroza, V.; Mastrodicasa, D.; et al. CTA pulmonary artery enlargement in patients with severe aortic stenosis: Prognostic impact after TAVR. J. Cardiovasc. Comput. Tomogr. 2021, 15, 431–440. [Google Scholar] [CrossRef]
- Wu, Y.; Pan, N.; An, Y.; Xu, M.; Tan, L.; Zhang, L. Diagnostic and Prognostic Biomarkers for Myocardial Infarction. Front. Cardiovasc. Med. 2021, 7, 617277. [Google Scholar] [CrossRef]
- Wang, X.-Y.; Zhang, F.; Zhang, C.; Zheng, L.-R.; Yang, J. The Biomarkers for Acute Myocardial Infarction and Heart Failure. BioMed Res. Int. 2020, 2020, 14. [Google Scholar] [CrossRef] [Green Version]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Hear. Fail. Rev. 2021, 27, 625–643. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; Januzzi, J.L., Jr. Established and Emerging Roles of Biomarkers in Heart Failure. Circ. Res. 2018, 123, 614–629. [Google Scholar] [CrossRef]
- Boxhammer, E.; Mirna, M.; Bäz, L.; Bacher, N.; Topf, A.; Sipos, B.; Franz, M.; Kretzschmar, D.; Hoppe, U.C.; Lauten, A.; et al. Soluble ST2 as a Potential Biomarker for Risk Assessment of Pulmonary Hypertension in Patients Undergoing TAVR? Life 2022, 12, 389. [Google Scholar] [CrossRef]
- Muessig, J.M.; Lichtenauer, M.; Wernly, B.; Kelm, M.; Franz, M.; Bäz, L.; Schulze, P.C.; Racher, V.; Zimmermann, G.; Figulla, H.-R.; et al. Insulin like growth factor binding protein 2 (IGFBP-2) for risk prediction in patients with severe aortic stenosis undergoing Transcatheter Aortic Valve Implantation (TAVI). Int. J. Cardiol. 2018, 277, 54–59. [Google Scholar] [CrossRef]
- Hodges, G.W.; Bang, C.; Eugen-Olsen, J.; Olsen, M.H.; Boman, K.; Ray, S.; Kesäniemi, A.Y.; Jeppesen, J.L.; Wachtell, K. SuPAR predicts postoperative complications and mortality in patients with asymptomatic aortic stenosis. Open Hear. 2018, 5, e000743. [Google Scholar] [CrossRef]
- Kim, J.B.; Kobayashi, Y.; Moneghetti, K.J.; Brenner, D.A.; O’Malley, R.; Schnittger, I.; Wu, J.C.; Murtagh, G.; Beshiri, A.; Fischbein, M.; et al. GDF-15 (Growth Differentiation Factor 15) Is Associated With Lack of Ventricular Recovery and Mortality After Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2017, 10, e005594. [Google Scholar] [CrossRef]
- Mirna, M.; Wernly, B.; Paar, V.; Jung, C.; Jirak, P.; Figulla, H.R.; Kretzschmar, D.; Franz, M.; Hoppe, U.C.; Lichtenauer, M.; et al. Multi-biomarker analysis in patients after transcatheter aortic valve implantation (TAVI). Biomarkers: Biochemical indicators of exposure, response, and susceptibility to chemicals. Biomarkers 2018, 23, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Sudo, M.; Sugiura, A.; Treiling, L.; Al-Kassou, B.; Shamekhi, J.; Kütting, D.; Wilde, N.; Weber, M.; Zimmer, S.; Nickenig, G.; et al. Baseline PA/BSA ratio in patients undergoing transcatheter aortic valve replacement–A novel CT-based marker for the prediction of pulmonary hypertension and outcome. Int. J. Cardiol. 2021, 348, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Eberhard, M.; Mastalerz, M.; Pavicevic, J.; Frauenfelder, T.; Nietlispach, F.; Maisano, F.; Tanner, F.C.; Nguyen-Kim, T. Value of CT signs and measurements as a predictor of pulmonary hypertension and mortality in symptomatic se-vere aortic valve stenosis. The international journal of cardiovascular imaging. Int. J. Cardiovasc. Imag. 2017, 33, 1637–1651. [Google Scholar] [CrossRef] [PubMed]
- Luçon, A.; Oger, E.; Bedossa, M.; Boulmier, D.; Verhoye, J.P.; Eltchaninoff, H.; Iung, B.; Leguerrier, A.; Laskar, M.; Leprince, P.; et al. Prognostic Implications of Pulmonary Hypertension in Patients With Severe Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation: Study from the FRANCE 2 Registry. Circ. Cardiovasc. Interv. 2014, 7, 240–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumauskiene, B.; Padervinskiene, L.; Vaskelyte, J.J.; Vaitiekiene, A.; Lapinskas, T.; Hoppenot, D.; Miliauskas, S.; Galnaitiene, G.; Simkus, P.; Ereminiene, E. Left Ventricular Morphology and Function as a Determinant of Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Cardiovascular Magnetic Resonance Imaging Study. Medicina 2019, 55, 711. [Google Scholar] [CrossRef] [Green Version]
- Maeder, M.T.; Weber, L.; Ammann, P.; Buser, M.; Ehl, N.F.; Gerhard, M.; Brenner, R.; Haager, P.K.; Maisano, F.; Rickli, H. Relationship between B-type natriuretic peptide and invasive haemodynamics in patients with severe aortic valve stenosis. ESC Hear. Fail. 2020, 7, 577–587. [Google Scholar] [CrossRef] [Green Version]
- Calin, A.; Mateescu, A.D.; Rosca, M.; Beladan, C.C.; Enache, R.; Botezatu, S.; Cosei, I.; Calin, C.; Simion, M.; Ginghina, C.; et al. Left atrial dysfunction as a determinant of pulmonary hypertension in patients with severe aortic stenosis and preserved left ventricular ejection fraction. Int. J. Cardiovasc. Imaging 2017, 33, 1939–1947. [Google Scholar] [CrossRef]
- Gumauskienė, B.; Krivickienė, A.; Jonkaitienė, R.; Vaškelytė, J.J.; Siudikas, A.; Ereminienė, E. Impact of Left Ventricular Diastolic Dysfunction and Biomarkers on Pulmonary Hypertension in Patients with Severe Aortic Stenosis. Medicina 2018, 54, 63. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.; Jia, Y.; Zhu, B. BNP and NT-proBNP as Diagnostic Biomarkers for Cardiac Dysfunction in Both Clinical and Forensic Medicine. Int. J. Mol. Sci. 2019, 20, 1820. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.-D.; He, Y.; Wang, S.; Wong, G.T.; Irwin, M.; Xia, Z. Heart-type fatty acid binding protein (H-FABP) as a biomarker for acute myocardial injury and long-term post-ischemic prognosis. Acta Pharmacol. Sin. 2018, 39, 1155–1163. [Google Scholar] [CrossRef]
- Boxhammer, E.; Köller, C.; Paar, V.; Fejzic, D.; Rezar, R.; Reiter, C.; Kammler, J.; Kellermair, J.; Hammerer, M.; Blessberger, H.; et al. Systolic Pulmonary Artery Pressure and Cardiovascular Biomarkers—New Non-Invasive Ways to Detect Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis Undergoing TAVR? Rev. Cardiovasc. Med. 2022, 23, 224. [Google Scholar] [CrossRef]
- Boxhammer, E.; Paar, V.; Jirak, P.; Köller, C.; Demirel, O.; Eder, S.; Reiter, C.; Kammler, J.; Kellermair, J.; Hammerer, M.; et al. Main pulmonary artery diameter in combination with cardiovascular biomarkers. New possibilities to identify pulmonary hypertension in patients with severe aortic valve stenosis? Minerva Medica 2022. [Google Scholar] [CrossRef]
- Verhamme, F.M.; Freeman, C.M.; Brusselle, G.G.; Bracke, K.R.; Curtis, J.L. GDF-15 in Pulmonary and Critical Care Medicine. Am. J. Respiratory Cell Mol. Biol. 2019, 60, 621–628. [Google Scholar] [CrossRef]
- Larissi, K.; Politou, M.; Margeli, A.; Poziopoulos, C.; Flevari, P.; Terpos, E.; Papassotiriou, I.; Voskaridou, E. The Growth Differentiation Factor-15 (GDF-15) levels are increased in patients with compound heterozygous sickle cell and beta-thalassemia (HbS/βthal), correlate with markers of hemolysis, iron burden, coagulation, endothelial dysfunction and pulmonary hypertension. Blood Cells Mol. Dis. 2019, 77, 137–141. [Google Scholar] [CrossRef]
- Griffiths, M.; Yang, J.; Nies, M.; Vaidya, D.; Brandal, S.; Williams, M.; Matsui, E.C.; Grant, T.; Damico, R.; Ivy, D.; et al. Pediatric pulmonary hypertension: Insulin-like growth factor-binding protein 2 is a novel marker associated with disease severity and survival. Pediatr. Res. 2020, 88, 850–856. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IVC Diameter | Respiratory Caliber Fluctuation | RAP |
|---|---|---|
| ≥21 mm | <50% | 15 mmHg |
| Not corresponding to these constellations | 8 mmHg | |
| <21 mm | ≥50% | 3 mmHg |
| Overall Cohort n = 188 | PA/BSA < 16.6 mm/m2 n = 107 | PA/BSA ≥ 16.6 mm/m2 n = 81 | |||||
|---|---|---|---|---|---|---|---|
| Clinical Data | p-value | ||||||
| Age (years)—mean ± SD | 82.8 | 4.9 | 82.0 | 5.0 | 83.0 | 4.5 | 0.139 |
| Gender (male)—% | 52.7 | 60.7 | 42.0 | 0.011 | |||
| Weight (kg)—mean ± SD | 74.2 | 14.6 | 76.0 | 15.5 | 71.0 | 12.8 | 0.021 |
| Height (cm)—mean ± SD | 166.9 | 9.1 | 168.6 | 8.7 | 164.7 | 9.0 | 0.003 |
| BMI (kg/m2)—mean ± SD | 26.6 | 5.3 | 26.8 | 5.7 | 26.3 | 4.6 | 0.517 |
| NYHA—median ± IQR | 3.0 | 1.0 | 3.0 | 1.0 | 3.0 | 1.0 | 0.277 |
| STSScore—mean ± SD | 2.9 | 1.6 | 2.4 | 1.0 | 3.5 | 1.8 | 0.005 |
| Concomitant Disease | p-value | ||||||
| Diabetes mellitus—% | 21.8 | 23.4 | 19.8 | 0.553 | |||
| Hypertension—% | 79.3 | 82.2 | 75.3 | 0.246 | |||
| CVD-% | 73.4 | 80.4 | 64.2 | 0.025 | |||
| CVD-1 vessel—% | 22.3 | 25.2 | 18.5 | 0.399 | |||
| CVD-2 vessels—% | 9.0 | 8.4 | 9.9 | 0.610 | |||
| CVD-3 vessels—% | 9.6 | 11.2 | 7.4 | 0.469 | |||
| Myocardial infarction—% | 3.2 | 2.8 | 3.7 | 0.737 | |||
| Atrial fibrillation—% | 33.5 | 29.0 | 39.5 | 0.130 | |||
| Pacemaker—% | 7.4 | 6.5 | 8.6 | 0.587 | |||
| Malignancy—% | 21.3 | 24.3 | 17.3 | 0.244 | |||
| Stroke—% | 4.8 | 3.7 | 6.2 | 0.436 | |||
| PAD—% | 5.3 | 4.7 | 6.2 | 0.650 | |||
| COPD—% | 9.0 | 8.4 | 9.9 | 0.729 | |||
| Echocardiography | p-value | ||||||
| LVEF (%)—mean ± SD | 55.8 | 11.0 | 57.5 | 9.4 | 53.4 | 12.4 | 0.015 |
| LVEDD (mm)—mean ± SD | 46.0 | 6.1 | 4.5 | 0.5 | 4.6 | 0.7 | 0.277 |
| IVSd (mm)—mean ± SD | 15.2 | 2.9 | 15.0 | 2.8 | 15.5 | 3.2 | 0.377 |
| AV Vmax (m/s)—mean ± SD | 4.3 | 0.6 | 4.3 | 0.5 | 4.3 | 0.6 | 0.678 |
| AVdPmean (mmHg)—mean ± SD | 48.6 | 12.5 | 48.6 | 12.0 | 48.7 | 13.3 | 0.949 |
| AVdPmax (mmHg)—mean ± SD | 77.8 | 19.2 | 77.9 | 18.3 | 77.7 | 20.4 | 0.950 |
| TAPSE (mm)—mean ± SD | 22.1 | 3.9 | 22.7 | 4.1 | 21.1 | 3.6 | 0.077 |
| sPAP (mmHg)—mean ± SD | 43.3 | 15.4 | 38.5 | 14.3 | 49.0 | 14.8 | <0.001 |
| AVI ≥ II°—% | 16.0 | 11.2 | 22.2 | 0.053 | |||
| MVI ≥ II°—% | 19.7 | 15.9 | 24.7 | 0.147 | |||
| TVI ≥ II°—% | 12.2 | 9.3 | 16.0 | 0.154 | |||
| Laboratory data | p-value | ||||||
| Creatinine (mg/dL)—median ± IQR | 1.0 | 0.4 | 1.0 | 0.3 | 1.0 | 0.5 | 0.694 |
| BNP (pg/mL)—median ± IQR | 1174.0 | 2094.4 | 823.1 | 1557.3 | 2270.5 | 3263.7 | <0.001 |
| cTnI (pg/mL)—median ± IQR | 23.5 | 19.0 | 21.0 | 14.0 | 27.0 | 22.0 | 0.055 |
| hsTN (pg/mL)—median ± IQR | 2.5 | 2.3 | 2.4 | 2.3 | 2.7 | 1.3 | 0.747 |
| Hkt (%)—median ± IQR | 38.4 | 6.2 | 39.1 | 5.3 | 37.4 | 7.7 | 0.013 |
| Hb (g/dL)—median ± IQR | 12.8 | 2.3 | 13.1 | 2.4 | 12.6 | 2.9 | 0.011 |
| CK (U/L)—median ± IQR | 79.0 | 68.0 | 86.5 | 78.0 | 75.0 | 66.0 | 0.218 |
| sST2 (pg/mL)—median ± IQR | 13,947.3 | 9073.6 | 14,399.6 | 10,086.8 | 13,806.6 | 6727.2 | 0.323 |
| GDF-15 (pg/mL)—median ± IQR | 922.8 | 707.5 | 840.1 | 577.7 | 1055.2 | 778.9 | 0.040 |
| H-FABP (ng/mL)—median ± IQR | 1.3 | 1.8 | 1.1 | 1.5 | 1.6 | 1.9 | 0.007 |
| IGF-BP2 (pg/mL)—median ± IQR | 178,153.7 | 134,892.6 | 156,947.6 | 115,637.5 | 225,232.1 | 180,916.1 | 0.005 |
| suPAR (pg/mL)—median ± IQR | 3524.1 | 1740.2 | 3449.2 | 1775.6 | 3767.5 | 1895.8 | 0.097 |
| Value | Prediction | AUC | 95%CI | p-Value | Cut-Off | Sensitivity | Specificity | Youden Index |
|---|---|---|---|---|---|---|---|---|
| PA/BSA (mm/m2) | sPAP ≥ 40 mmHg | 0.741 | 0.656–0.826 | <0.001 | 16.53 | 0.62 | 0.79 | 0.41 |
| PA/BSA (mm/m2) | sPAP ≥ 45 mmHg | 0.642 | 0.584–0.761 | <0.001 | 16.65 | 0.62 | 0.71 | 0.33 |
| PA/BSA (mm/m2) | sPAP ≥ 50 mmHg | 0.742 | 0.658–0.826 | <0.001 | 16.65 | 0.74 | 0.68 | 0.42 |
| Value | Prediction | AUC | 95%CI | p-Value | Cut-Off | Sensitivity | Specificity | Youden Index |
|---|---|---|---|---|---|---|---|---|
| sST2 (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.466 | 0.382–0.550 | 0.433 | 11,545.5 | 0.72 | 0.33 | 0.05 |
| GDF-15 (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.595 | 0.509–0.680 | 0.029 | 1172.0 | 0.44 | 0.76 | 0.20 |
| H-FABP (ng/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.616 | 0.533–0.700 | 0.080 | 1.6 | 0.54 | 0.69 | 0.23 |
| IGF-BP2 (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.694 | 0.570–0.818 | 0.050 | 198,440.4 | 0.63 | 0.70 | 0.33 |
| suPAR (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.572 | 0.487–0.656 | 0.097 | 2753.9 | 0.83 | 0.31 | 0.14 |
| BNP (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.684 | 0.604–0.764 | <0.001 | 2194.0 | 0.51 | 0.80 | 0.32 |
| hsTN (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.518 | 0.410–0.626 | 0.748 | 2.0 | 0.76 | 0.39 | 0.15 |
| cTNI (pg/mL) | PA/BSA ≥ 16.6 mm/m2 | 0.635 | 0.501–0.770 | 0.055 | 24.5 | 0.66 | 0.66 | 0.31 |
| Values | Prediction | AUC | 95%CI | p-Value | Sensitivity | Specificity | Youden Index |
|---|---|---|---|---|---|---|---|
| sST2—GDF-15 | PA/BSA ≥ 16.6 mm/m2 | 0.600 | 0.514–0.686 | 0.022 | 0.34 | 0.88 | 0.22 |
| sST2—H-FABP | PA/BSA ≥ 16.6 mm/m2 | 0.625 | 0.543–0.708 | 0.004 | 0.67 | 0.56 | 0.23 |
| sST2—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.700 | 0.577–0.823 | 0.004 | 0.53 | 0.81 | 0.35 |
| sST2—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.599 | 0.515–0.682 | 0.220 | 0.30 | 0.93 | 0.22 |
| sST2—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.706 | 0.626–0.785 | < 0.001 | 0.71 | 0.67 | 0.38 |
| sST2—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.524 | 0.415–0.634 | 0.056 | 0.77 | 0.38 | 0.14 |
| sST2—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.619 | 0.484–0.754 | 0.092 | 0.59 | 0.66 | 0.25 |
| GDF-15—H-FABP | PA/BSA ≥ 16.6 mm/m2 | 0.619 | 0.534–0.704 | 0.006 | 0.67 | 0.62 | 0.29 |
| GDF-15—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.698 | 0.570–0.825 | 0.005 | 0.64 | 0.72 | 0.36 |
| GDF-15—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.609 | 0.525–0.692 | 0.013 | 0.49 | 0.74 | 0.22 |
| GDF-15—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.682 | 0.599–0.765 | <0.001 | 0.76 | 0.58 | 0.34 |
| GDF-15—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.580 | 0.468–0.693 | 0.153 | 0.51 | 0.74 | 0.25 |
| GDF-15—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.636 | 0.498–0.774 | 0.059 | 0.48 | 0.83 | 0.31 |
| H-FABP—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.694 | 0.567–0.821 | 0.006 | 0.46 | 0.88 | 0.35 |
| H-FABP—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.612 | 0.527–0.697 | 0.010 | 0.51 | 0.74 | 0.25 |
| H-FABP—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.698 | 0.617–0.778 | <0.001 | 0.78 | 0.62 | 0.39 |
| H-FABP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.606 | 0.497–0.715 | 0.056 | 0.45 | 0.77 | 0.22 |
| H-FABP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.624 | 0.486–0.762 | 0.086 | 0.59 | 0.68 | 0.28 |
| IGF-BP2—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.684 | 0.559–0.810 | 0.008 | 0.43 | 0.88 | 0.32 |
| IGF-BP2—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.721 | 0.585–0.857 | 0.004 | 0.68 | 0.73 | 0.41 |
| IGF-BP2—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.694 | 0.570–0.818 | 0.005 | 0.63 | 0.70 | 0.33 |
| suPAR—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.695 | 0.615–0.775 | <0.001 | 0.47 | 0.84 | 0.31 |
| suPAR—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.572 | 0.487–0.656 | 0.097 | 0.83 | 0.31 | 0.14 |
| suPAR—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.669 | 0.539–0.798 | 0.017 | 0.69 | 0.63 | 0.32 |
| BNP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.700 | 0.603–0.798 | <0.001 | 0.54 | 0.82 | 0.36 |
| BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.680 | 0.544–0.816 | 0.018 | 0.89 | 0.44 | 0.33 |
| Values | Prediction | AUC | 95%CI | p-Value | Sensitivity | Specificity | Youden Index |
|---|---|---|---|---|---|---|---|
| sST2—GDF-15—H-FABP | PA/BSA ≥ 16.6 mm/m2 | 0.633 | 0.550–0.717 | 0.002 | 0.55 | 0.71 | 0.26 |
| sST2—GDF-15—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.702 | 0.575–0.829 | 0.004 | 0.82 | 0.53 | 0.36 |
| sST2—GDF-15—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.614 | 0.529–0.699 | 0.009 | 0.40 | 0.87 | 0.26 |
| sST2—GDF-15—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.708 | 0.627–0.788 | <0.001 | 0.75 | 0.62 | 0.36 |
| sST2—GDF-15—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.584 | 0.473–0.695 | 0.136 | 0.36 | 0.85 | 0.21 |
| sST2—GDF-15—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.637 | 0.496–0.778 | 0.058 | 0.48 | 0.85 | 0.33 |
| sST2—H-FABP—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.719 | 0.595–0.844 | 0.002 | 0.68 | 0.72 | 0.40 |
| sST2—H-FABP—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.630 | 0.548–0.712 | 0.003 | 0.61 | 0.61 | 0.22 |
| sST2—H-FABP—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.714 | 0.635–0.793 | <0.001 | 0.73 | 0.65 | 0.38 |
| sST2—H-FABP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.619 | 0.512–0.725 | 0.035 | 0.68 | 0.56 | 0.24 |
| sST2—H-FABP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.626 | 0.487–0.765 | 0.080 | 0.67 | 0.61 | 0.28 |
| sST2—IGF-BP2—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.697 | 0.573–0.821 | 0.004 | 0.53 | 0.81 | 0.35 |
| sST2—IGF-BP2—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.727 | 0.593–0.862 | 0.003 | 0.64 | 0.79 | 0.43 |
| sST2—IGF-BP2—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.731 | 0.605–0.858 | 0.001 | 0.64 | 0.80 | 0.44 |
| sST2—suPAR—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.698 | 0.618–0.778 | <0.001 | 0.60 | 0.74 | 0.34 |
| sST2—suPAR—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.559 | 0.449–0.669 | 0.294 | 0.57 | 0.61 | 0.18 |
| sST2—suPAR—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.699 | 0.574–0.823 | 0.005 | 0.76 | 0.66 | 0.42 |
| sST2—BNP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.708 | 0.609–0.807 | <0.001 | 0.62 | 0.74 | 0.36 |
| sST2—BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.688 | 0.553–0.823 | 0.013 | 0.81 | 0.53 | 0.34 |
| GDF-15—H-FABP—IGF-BP2 | PA/BSA ≥ 16.6 mm/m2 | 0.698 | 0.570–0.825 | 0.005 | 0.57 | 0.79 | 0.36 |
| GDF-15—H-FABP—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.627 | 0.544–0.711 | 0.003 | 0.75 | 0.51 | 0.26 |
| GDF-15—H-FABP—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.699 | 0.619–0.779 | <0.001 | 0.82 | 0.54 | 0.36 |
| GDF-15—H-FABP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.610 | 0.499–0.720 | 0.051 | 0.70 | 0.64 | 0.34 |
| GDF-15—H-FABP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.635 | 0.496–0.774 | 0.061 | 0.48 | 0.83 | 0.31 |
| GDF-15—IGF-BP2—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.695 | 0.567–0.823 | 0.006 | 0.50 | 0.86 | 0.36 |
| GDF-15—IGF-BP2—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.727 | 0.590–0.864 | 0.004 | 0.74 | 0.67 | 0.41 |
| GDF-15—IGF-BP2—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.732 | 0.600–0.863 | 0.002 | 0.58 | 0.90 | 0.48 |
| GDF-15—suPAR—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.699 | 0.619–0.779 | <0.001 | 0.69 | 0.64 | 0.32 |
| GDF-15—suPAR—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.594 | 0.486–0.702 | 0.095 | 0.72 | 0.49 | 0.21 |
| GDF-15—suPAR—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.653 | 0.516–0.790 | 0.034 | 0.63 | 0.76 | 0.39 |
| GDF-15—BNP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.707 | 0.607–0.806 | <0.001 | 0.51 | 0.85 | 0.36 |
| GDF-15—BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.648 | 0.500–0.797 | 0.056 | 0.71 | 0.65 | 0.36 |
| H-FABP—IGF-BP2—suPAR | PA/BSA ≥ 16.6 mm/m2 | 0.694 | 0.567–0.820 | 0.006 | 0.43 | 0.91 | 0.34 |
| H-FABP—IGF-BP2—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.721 | 0.580–0.861 | 0.005 | 0.52 | 0.91 | 0.43 |
| H-FABP—IGF-BP2—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.724 | 0.593–0.855 | 0.002 | 0.54 | 0.93 | 0.46 |
| H-FABP—suPAR—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.698 | 0.618–0.778 | <0.001 | 0.82 | 0.55 | 0.37 |
| H-FABP—suPAR—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.627 | 0.518–0.737 | 0.024 | 0.68 | 0.62 | 0.30 |
| H-FABP—suPAR—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.668 | 0.536–0.801 | 0.019 | 0.82 | 0.51 | 0.33 |
| H-FABP—BNP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.732 | 0.638–0.826 | <0.001 | 0.87 | 0.56 | 0.43 |
| H-FABP—BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.669 | 0.527–0.811 | 0.029 | 0.75 | 0.65 | 0.40 |
| IGF-BP2—suPAR—BNP | PA/BSA ≥ 16.6 mm/m2 | 0.720 | 0.584–0.856 | 0.004 | 0.52 | 0.88 | 0.40 |
| IGF-BP2—suPAR—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.726 | 0.600–0.852 | 0.002 | 0.54 | 0.93 | 0.46 |
| IGF-BP2—BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.733 | 0.599–0.868 | 0.003 | 0.56 | 0.88 | 0.44 |
| suPAR—BNP—hsTN | PA/BSA ≥ 16.6 mm/m2 | 0.710 | 0.612–0.809 | <0.001 | 0.70 | 0.66 | 0.36 |
| suPAR—BNP—cTnI | PA/BSA ≥ 16.6 mm/m2 | 0.689 | 0.552–0.826 | 0.013 | 0.85 | 0.62 | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kletzer, J.; Hecht, S.; Ramsauer, S.; Scharinger, B.; Kaufmann, R.; Kammler, J.; Kellermair, J.; Akbari, K.; Blessberger, H.; Steinwender, C.; et al. A Story of PA/BSA and Biomarkers to Diagnose Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—The Rise of IGF-BP2 and GDF-15. J. Cardiovasc. Dev. Dis. 2023, 10, 22. https://doi.org/10.3390/jcdd10010022
Kletzer J, Hecht S, Ramsauer S, Scharinger B, Kaufmann R, Kammler J, Kellermair J, Akbari K, Blessberger H, Steinwender C, et al. A Story of PA/BSA and Biomarkers to Diagnose Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—The Rise of IGF-BP2 and GDF-15. Journal of Cardiovascular Development and Disease. 2023; 10(1):22. https://doi.org/10.3390/jcdd10010022
Chicago/Turabian StyleKletzer, Joseph, Stefan Hecht, Susanne Ramsauer, Bernhard Scharinger, Reinhard Kaufmann, Jürgen Kammler, Jörg Kellermair, Kaveh Akbari, Hermann Blessberger, Clemens Steinwender, and et al. 2023. "A Story of PA/BSA and Biomarkers to Diagnose Pulmonary Hypertension in Patients with Severe Aortic Valve Stenosis—The Rise of IGF-BP2 and GDF-15" Journal of Cardiovascular Development and Disease 10, no. 1: 22. https://doi.org/10.3390/jcdd10010022