
Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- Patients affected by Transthyretin Cardiac Amyloidosis (ATTR), caused either by genetic mutation or wild type, diagnosed in accordance with the 2021 European Society of Cardiology (ESC) position statement [8]—using imaging criteria (transthoracic echocardiography [TTE] or cardiac magnetic resonance [CMR]) and total body 99mTc-PYP, DPD, or HMDP bone scintigraphy with SPECT (Perugini 2 or 3), after ruling out light chains amyloidosis (AL).
- Patients diagnosed with Sarcomeric Hypertrophic Cardiomyopathies (HCMs), in line with the ESC 2014 guidelines [13], featuring TTE criteria: maximum wall thickness ≥15 mm (or ≥13 mm for family members), irrespective of the identification of the genetic mutation. Patients presenting with Obstructive HCM and LVOT gradient >30 mmHg were excluded from the analysis.
2.2. Echocardiography
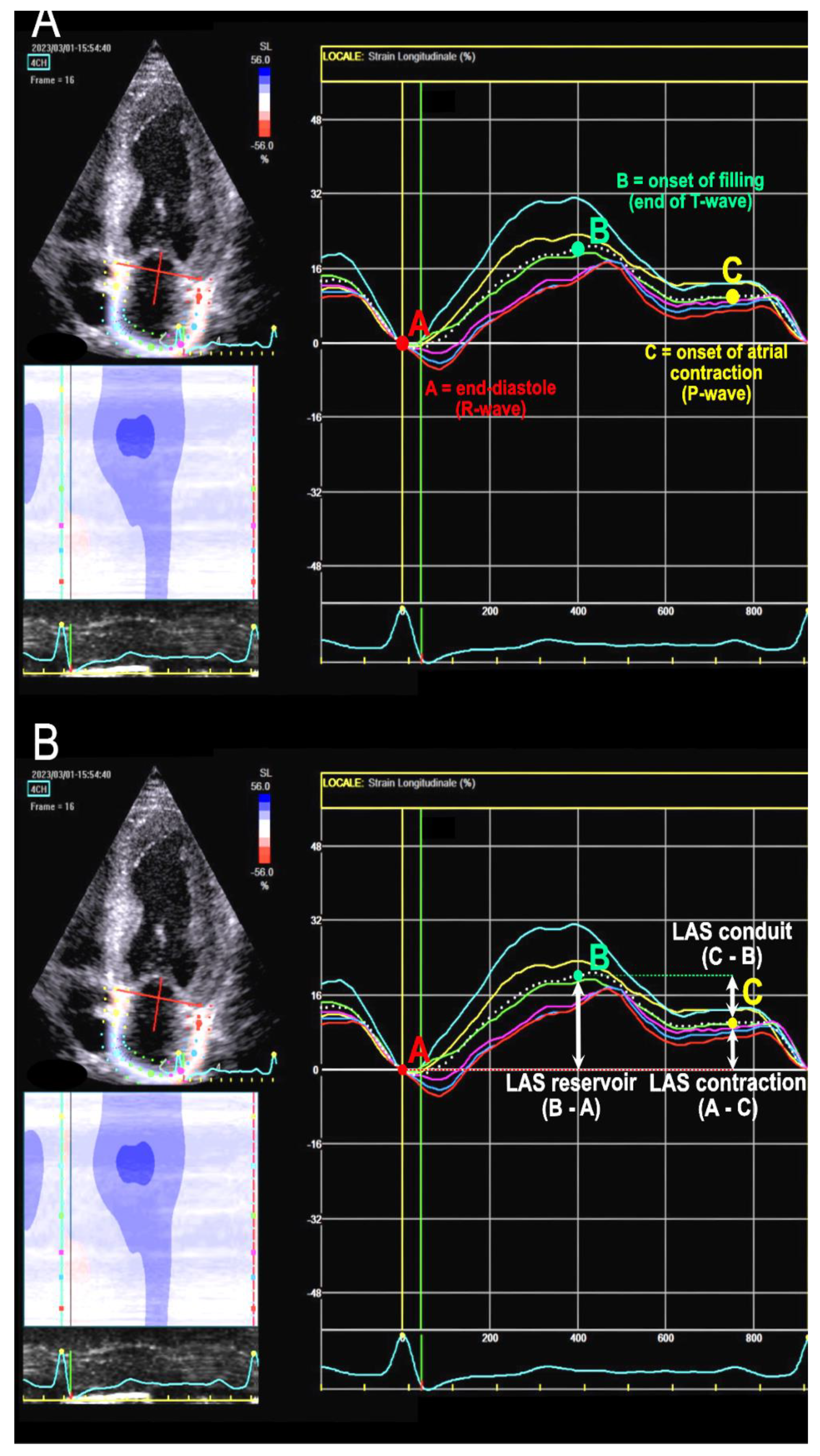
2.3. LA Strain Assessment
2.4. Clinical Outcomes Assessment
2.5. Ethical Considerations
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. LA Strain: Prognostic Value
4.2. Insights about Cut-Off Values from Literature
4.3. Strengths and Clinical—Practical Implications
4.4. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prioli, A.; Marino, P.; Lanzoni, L.; Zardini, P. Increasing degrees of left ventricular filling impairment modulate left atrial function in humans. Am. J. Cardiol. 1998, 82, 756–761. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA Strain for Categorization of LV Diastolic Dysfunction. JACC Cardiovasc. Imaging 2017, 10, 735–743. [Google Scholar] [CrossRef]
- Bisbal, F.; Baranchuk, A.; Braunwald, E.; Bayés de Luna, A.; Bayés-Genís, A. Atrial Failure as a Clinical Entity: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 222–232. [Google Scholar] [CrossRef]
- Faro, D.C.; Losi, V.; Rodolico, M.S.; Licciardi, S.; Monte, I.P. Speckle tracking echocardiography-derived parameters as new prognostic markers in hypertrophic cardiomyopathies. Eur. Heart J. Open 2023, 3, oead014. [Google Scholar] [CrossRef]
- Fujimoto, K.; Inoue, K.; Saito, M.; Higashi, H.; Kono, T.; Uetani, T.; Aono, J.; Nagai, T.; Nishimura, K.; Suzuki, J.; et al. Incremental value of left atrial active function measured by speckle tracking echocardiography in patients with hypertrophic cardiomyopathy. Echocardiography 2018, 35, 1138–1148. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Versteylen, M.O.; Brons, M.; Teske, A.J.; Oerlemans, M. Restrictive Atrial Dysfunction in Cardiac Amyloidosis: Differences between Immunoglobulin Light Chain and Transthyretin Cardiac Amyloidosis Patients. Biomedicines 2022, 10, 1768. [Google Scholar] [CrossRef]
- De Gregorio, C.; Dattilo, G.; Casale, M.; Terrizzi, A.; Donato, R.; Di Bella, G. Left Atrial Morphology, Size and Function in Patients With Transthyretin Cardiac Amyloidosis and Primary Hypertrophic Cardiomyopathy–Comparative Strain Imaging Study. Circ. J. 2016, 80, 1830–1837. [Google Scholar] [CrossRef]
- Mohty, D.; Pibarot, P.; Dumesnil, J.G.; Darodes, N.; Lavergne, D.; Echahidi, N.; Virot, P.; Bordessoule, D.; Jaccard, A. Left atrial size is an independent predictor of overall survival in patients with primary systemic amyloidosis. Arch. Cardiovasc. Dis. 2011, 104, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Nochioka, K.; Quarta, C.C.; Claggett, B.; Roca, G.Q.; Rapezzi, C.; Falk, R.H.; Solomon, S.D. Left atrial structure and function in cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [PubMed]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1301–1310. [Google Scholar] [PubMed]
- Voigt, J.U.; Mălăescu, G.G.; Haugaa, K.; Badano, L. How to do LA strain. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Koyama, J.; Ray-Sequin, P.A.; Falk, R.H. Longitudinal myocardial function assessed by tissue velocity, strain, and strain rate tissue Doppler echocardiography in patients with AL (primary) cardiac amyloidosis. Circulation 2003, 107, 2446–2452. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Duchenne, J.; Mirea, O.; Vovas, G.; Van Cleemput, J.; Delforge, M.; Kuznetsova, T.; Bogaert, J.; Voigt, J.-U. The Relation of Ejection Fraction and Global Longitudinal Strain in Amyloidosis: Implications for Differential Diagnosis. JACC Cardiovasc. Imaging 2016, 9, 1358–1359. [Google Scholar] [CrossRef]
- Ternacle, J.; Bodez, D.; Guellich, A.; Audureau, E.; Rappeneau, S.; Lim, P.; Radu, C.; Guendouz, S.; Couetil, J.-P.; Benhaiem, N.; et al. Causes and Consequences of Longitudinal LV Dysfunction Assessed by 2D Strain Echocardiography in Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2016, 9, 126–138. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Mirea, O.; Duchenne, J.; Van Cleemput, J.; Delforge, M.; Bogaert, J.; Kuznetsova, T.; Voigt, J.U. Echo Parameters for Differential Diagnosis in Cardiac Amyloidosis: A Head-to-Head Comparison of Deformation and Nondeformation Parameters. Circ. Cardiovasc. Imaging 2017, 10, e005588. [Google Scholar] [CrossRef]
- Inoue, K.; Kawakami, H.; Akazawa, Y.; Higashi, H.; Higaki, T.; Yamaguchi, O. Echocardiographic Assessment of Atrial Function: From Basic Mechanics to Specific Cardiac Diseases. J. Cardiovasc. Dev. Dis. 2022, 9, 68. [Google Scholar] [CrossRef]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; García-Izquierdo, E.; Chetrit, M.; Moñivas-Palomero, V.; Mingo-Santos, S.; Andersen, Ø.S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Heart J. Cardiovasc. Imaging 2021, 23, 61–70. [Google Scholar] [CrossRef]
- Aimo, A.; Fabiani, I.; Giannoni, A.; Mandoli, G.E.; Pastore, M.C.; Vergaro, G.; Spini, V.; Chubuchny, V.; Pasanisi, E.M.; Petersen, C.; et al. Multi-chamber speckle tracking imaging and diagnostic value of left atrial strain in cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2022, 24, 130–141. [Google Scholar] [CrossRef]
- Aimo, A.; Fabiani, I.; Spini, V.; Chubuchny, V.; Pasanisi, E.M.; Petersen, C.; Poggianti, E.; Taddei, C.; Cameli, M.; E Mandoli, G.; et al. Left atrial strain in cardiac amyloidosis. Eur. Heart J. 2021, 42, ehab724-1794. [Google Scholar] [CrossRef]
- Tayal, B.; Malahfji, M.; Buergler, J.M.; Shah, D.J.; Nagueh, S.F. Hemodynamic determinants of left atrial strain in patients with hypertrophic cardiomyopathy: A combined echocardiography and CMR study. PLoS ONE 2021, 16, e0245934. [Google Scholar] [CrossRef]
- Candan, Ö.; Geçmen, Ç.; Kahyaoğlu, M.; Çelik, M.; Şimşek, Z.; Dindaş, F.; Doğduş, M.; Zehir, R.; Kırma, C. Left Atrial Dysfunction as Marker of Arrhythmic Events in Patients with Hypertrophic Cardiomyopathy. Anatol. J. Cardiol. 2022, 26, 771–777. [Google Scholar] [CrossRef]
- Teixeira, K.L.M.; Correia, E.B.; Tressino, C.G.; Peçanha, M.M.; Melchior, W.A.; Barretto, R.B.D.M.; de Medeiros, B.G.; Le Bihan, D. Echocardiographic assessment of atrial function in patients with hypertrophic cardiomyopathy with and without paroxysmal atrial fibrillation. Rev. Port. Cardiol. 2022, 41, 771–779. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, H.K.; Rhee, T.M.; Choi, Y.-J.; Hwang, I.-C.; Yoon, Y.E.; Park, J.-B.; Lee, S.-P.; Kim, Y.-J.; Cho, G.-Y. Left Atrial Reservoir Strain-Based Left Ventricular Diastolic Function Grading and Incident Heart Failure in Hypertrophic Cardiomyopathy. Circ. Cardiovasc. Imaging 2022, 15, e013556. [Google Scholar] [CrossRef]
- Rausch, K.; Scalia, G.M.; Sato, K.; Edwards, N.; Lam, A.K.-Y.; Platts, D.G.; Chan, J. Left atrial strain imaging differentiates cardiac amyloidosis and hypertensive heart disease. Int. J. Cardiovasc. Imaging 2021, 37, 81–90. [Google Scholar] [CrossRef]
- Iio, C.; Inoue, K.; Nishimura, K.; Fujii, A.; Nagai, T.; Suzuki, J.; Okura, T.; Higaki, J.; Ogimoto, A. Characteristics of Left Atrial Deformation Parameters and Their Prognostic Impact in Patients with Pathological Left Ventricular Hypertrophy: Analysis by Speckle Tracking Echocardiography. Echocardiography 2015, 32, 1821–1830. [Google Scholar] [CrossRef]
- Kado, Y.; Obokata, M.; Nagata, Y.; Ishizu, T.; Addetia, K.; Aonuma, K.; Kurabayashi, M.; Lang, R.M.; Takeuchi, M.; Otsuji, Y. Cumulative Burden of Myocardial Dysfunction in Cardiac Amyloidosis Assessed Using Four-Chamber Cardiac Strain. J. Am. Soc. Echocardiogr. 2016, 29, 1092–1099.e2. [Google Scholar] [CrossRef]
- Lucas, C.; Martel, H.; Ruimy, A.; Fabre, C.; Gardenat, A.; Rique, A.; Michel, N.; Dernys, A.; Jacquier, A.; Habib, G. Multimodal imaging assessment of left atrial strain in cardiac amyloidosis and hypertrophic cardiomyopathies. Eur. Heart J. Cardiovasc. Imaging 2022, 23, jeab289-045. [Google Scholar] [CrossRef]
- Henein, M.Y.; Suhr, O.B.; Arvidsson, S.; Pilebro, B.; Westermark, P.; Hörnsten, R.; Lindqvist, P. Reduced left atrial myocardial deformation irrespective of cavity size: A potential cause for atrial arrhythmia in hereditary transthyretin amyloidosis. Amyloid 2018, 25, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Huntjens, P.R.; Zhang, K.W.; Soyama, Y.; Karmpalioti, M.; Lenihan, D.J.; Gorcsan, J., 3rd. Prognostic Utility of Echocardiographic Atrial and Ventricular Strain Imaging in Patients With Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2021, 14, 1508–1519. [Google Scholar] [CrossRef] [PubMed]
- Oike, F.; Usuku, H.; Yamamoto, E.; Yamada, T.; Egashira, K.; Morioka, M.; Nishi, M.; Komorita, T.; Hirakawa, K.; Tabata, N.; et al. Prognostic value of left atrial strain in patients with wild-type transthyretin amyloid cardiomyopathy. ESC Heart Fail. 2021, 8, 5316–5326. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Naharro, A.; Gonzalez-Lopez, E.; Corovic, A.; Mirelis, J.G.; Baksi, A.J.; Moon, J.C.; Garcia-Pavia, P.; Gillmore, J.D.; Hawkins, P.N.; Fontana, M. High Prevalence of Intracardiac Thrombi in Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2019, 73, 1733–1734. [Google Scholar] [CrossRef]
- Akintoye, E.; Majid, M.; Klein, A.; Hanna, M. Prognostic Utility of Left Atrial Strain to Predict Thrombotic Events and Mortality in Amyloid Cardiomyopathy. J. Am. Coll. Cardiol. Imaging, 2023; in press. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/ SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 1 of 2—Evidence Base and Standardized Methods of Imaging. Circ. Cardiovasc. Imaging 2021, 14, e000029. [Google Scholar]
- Bandera, F.; Martone, R.; Chacko, L.; Ganesananthan, S.; Gilbertson, J.A.; Ponticos, M.; Lane, T.; Martinez-Naharro, A.; Whelan, C.; Quarta, C.; et al. Clinical Importance of Left Atrial Infiltration in Cardiac Transthyretin Amyloidosis. JACC Cardiovasc. Imaging 2022, 15, 17–29. [Google Scholar] [CrossRef]
- Potter, E.L.; Ramkumar, S.; Kawakami, H.; Yang, H.; Wright, L.; Negishi, T.; Marwick, T.H. Association of Asymptomatic Diastolic Dysfunction Assessed by Left Atrial Strain With Incident Heart Failure. JACC Cardiovasc. Imaging. 2020, 13, 2316–2326. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Khan, S.U. Left Atrial Strain for Assessment of Left Ventricular Diastolic Function: Focus on Populations With Normal LVEF. JACC Cardiovasc. Imaging 2023, 16, 691–707. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CA N = 33 | HCM N = 34 | Co N = 33 | p (All Groups) | CA vs. HCM | CA vs. Co | HCM vs. Co | |
|---|---|---|---|---|---|---|---|
| Age (yo) | 68 (62.5–77.5) | 58.5 (38.7–63.2) | 58 (53–65) | <0.001 | <0.001 | 0.001 | 0.37 |
| M | 24 (72.7%) | 23 (67.6%) | 18 (54.5%) | 0.31 | 0.79 | 0.20 | 0.32 |
| F | 9 (27.3%) | 11 (32.4%) | 15 (45.5%) | 0.31 | 0.79 | 0.20 | 0.32 |
| NYHA 1 | 7 (21.2%) | 18 (52.9%) | <0.001 | 0.01 | <0.001 | <0.001 | |
| NYHA 2 | 23 (69.8%) | 14 (41.2%) | <0.001 | 0.03 | <0.001 | <0.001 | |
| NYHA 3 | 3 (9%) | 2 (5.9%) | 0.28 | 0.38 | 0.06 | 0.49 | |
| NYHA 4 | 0 | 0 | 1 | 1 | 1 | 1 | |
| BSA | 1.8 (1.7–1.9) | 1.9 (1.6–2.0) | 1.9 (1.7–2) | 0.48 | 0.24 | 0.30 | 0.69 |
| BP-sys, mmHg | 125 (112.5–135) | 130 (120–140) | 135 (131–145) | 0.001 | 0.11 | <0.001 | 0.01 |
| BP-dia, mmHg | 80 (75–85) | 80 (70–85) | 85 (80.5–90) | 0.03 | 0.13 | 0.07 | 0.004 |
| HR, bpm | 71 (65–78) | 65 (60–74.7) | 68 (60.5–75) | 0.33 | 0.07 | 0.11 | 0.67 |
| Fam. history SCD | 2 (6.1%) | 9 (26.5%) | 0 | 0.001 | 0.04 | 0.49 | 0.002 |
| Exertional dyspnoea | 29 (87.9%) | 14 (41.2%) | 0 | <0.001 | <0.001 | <0.001 | <0.001 |
| Syncope | 1 (3%) | 2 (5.9%) | 0 | 0.65 | 1 | 1 | 0.49 |
| AF | 6 (18.2%) | 3 (8.8%) | 0 | 0.03 | 0.30 | 0.02 | 0.24 |
| NSVT | 1 (3%) | 8 (23.5%) | 0 | 0.001 | 0.031 | 1 | 0.005 |
| ICD | 1 (3%) | 3 (8.8%) | 0 | 0.31 | 0.61 | 1 | 0.23 |
| CA N = 33 | HCM N = 34 | Co N = 33 | p All Groups | CA vs. HCM | CA vs. Co | HCM vs. Co | |
|---|---|---|---|---|---|---|---|
| EF, % | 53 (40.5–58.5) | 63.5 (58–69) | 60 (56.5–63) | <0.001 | <0.001 | <0.001 | 0.08 |
| LVMi (g/sqm) | 150 (123.5–188.5) | 130.2 (117.2–153) | 79 (68–96.5) | <0.001 | 0.056 | <0.001 | <0.001 |
| E/e’ | 16.3 (11.7–21.4) | 10 (7.2–14.2) | 6.5 (6–8.1) | <0.001 | 0.001 | <0.001 | <0.001 |
| LAVi (mL/sqm) | 43.3 (37.4–53) | 40 (31.5–57.2) | 25.6 (20.6–30.5) | <0.001 | 0.46 | <0.001 | <0.001 |
| TAPSE mm | 18 (15–21) | 23 (20.5–25) | 23 (20–26) | <0.001 | <0.001 | <0.001 | 0.92 |
| LV-GLS, % | −12 (−10, −14.2) | −15 (−11.7, −18) | −19 (−18, −20.5) | <0.001 | 0.005 | <0.001 | <0.001 |
| LAS-reservoir, % | 9 (5.8–16.6) | 14.5 (9.7–25) | 32 (25–38) | <0.001 | 0.009 | <0.001 | <0.001 |
| LAS-conduit, % | −6.7 (−4.2, −8.6) | −9 (−4.9, −15.3) | −15 (−12.1, −18.5) | <0.001 | 0.09 | <0.001 | 0.005 |
| LAS-contract., % | −3 (−0.9, −10.5) | −6 (−3, −9.7) | −14.3 (−10.5, −19.5) | <0.001 | 0.14 | <0.001 | <0.001 |
| CArEF N = 13 | CApEF N = 20 | HCM N = 34 | CApEF vs. CArEF | CApEF vs. HCM | |
|---|---|---|---|---|---|
| Age, yo | 75 (66.5–82) | 65.5 (57–72.5) | 58.5 (38.7–63.2) | 0.02 | 0.01 |
| BP-sys, mmHg | 115 (110–131.5) | 130 (123.5–135) | 130 (120–140) | 0.03 | 0.77 |
| BP-dia, mmHg | 82 (77.5–85) | 80 (75–88.7) | 80 (70–85) | 0.78 | 0.28 |
| HR, bpm | 69 (63–75) | 76.5 (65–78.7) | 65 (60–74.7) | 0.23 | 0.06 |
| NYHA 1, n (%) | 2 (15) | 5 (25) | 18 (53) | 0.67 | 0.05 |
| NYHA 2 | 9 (60) | 14 (70) | 14 (41) | 1 | 0.15 |
| NYHA 3 | 2 (15) | 1 (5) | 2 (6) | 0.54 | 1 |
| AF, n (%) | 3 (20) | 3 (15) | 3 (9) | 0.65 | 0.66 |
| EF, % | 37 (34.5–41) | 55.5 (54.2–60) | 63.5 (58–69) | <0.001 | 0.004 |
| LVMi, g/sqm | 165.5 (129.7–206.7) | 147.3 (119.8–176.8) | 130.2 (117.2–153) | 0.25 | 0.24 |
| E/e’ | 16.3 (13.5–22.2) | 15.9 (11.4–19.6) | 10 (7.2–14.2) | 0.43 | 0.001 |
| S’, cm/s | 4 (4–5.7) | 5 (5,6) | 7 (5–8) | 0.06 | 0.002 |
| LAVi, mL/sqm | 47.4 (40.1–60.5) | 41.9 (28.5–50.5) | 40 (31.5–57.2) | 0.08 | 0.85 |
| TAPSE, mm | 19 (11.5–24) | 17.5 (15.7–19.2) | 23 (20.5–25) | 0.82 | <0.001 |
| LV-GLS, % | −10 (−7, −12) | −13 (−10, −15) | −15 (−11.7, −18) | 0.02 | 0.07 |
| LAS-reservoir, % | 6.4 (3.9−13.5) | 9.4 (7–18) | 14.5 (9.7–25) | 0.10 | 0.09 |
| LAS-conduit, % | −5.2 (−3.3, −7.2) | −8 (−5, −9.7) | −9 (−4.9, −15.3) | 0.04 | 0.35 |
| LAS-contract. % | −3.5 (0.4, −10.2) | −3 (−1, −11) | −6 (−3, −9.7) | 0.80 | 0.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monte, I.P.; Faro, D.C.; Trimarchi, G.; de Gaetano, F.; Campisi, M.; Losi, V.; Teresi, L.; Di Bella, G.; Tamburino, C.; de Gregorio, C. Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy. J. Cardiovasc. Dev. Dis. 2023, 10, 261. https://doi.org/10.3390/jcdd10060261
Monte IP, Faro DC, Trimarchi G, de Gaetano F, Campisi M, Losi V, Teresi L, Di Bella G, Tamburino C, de Gregorio C. Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy. Journal of Cardiovascular Development and Disease. 2023; 10(6):261. https://doi.org/10.3390/jcdd10060261
Chicago/Turabian StyleMonte, Ines Paola, Denise Cristiana Faro, Giancarlo Trimarchi, Fabrizio de Gaetano, Mariapaola Campisi, Valentina Losi, Lucio Teresi, Gianluca Di Bella, Corrado Tamburino, and Cesare de Gregorio. 2023. "Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy" Journal of Cardiovascular Development and Disease 10, no. 6: 261. https://doi.org/10.3390/jcdd10060261