
Arrhythmias in Patients with Cardiac Amyloidosis: A Comprehensive Review on Clinical Management and Devices
 , , ,
, , ,
Abstract
:1. Introduction
2. Cardiac Amyloidosis and Arrhythmias
3. Types of Arrhythmias
3.1. Atrial Fibrillation and Atrial Flutter
3.2. Ventricular Arrhythmias
3.3. Conduction System Disorders
3.4. Sudden Cardiac Death
4. Prognostic Significance of Arrhythmias
5. Treatment
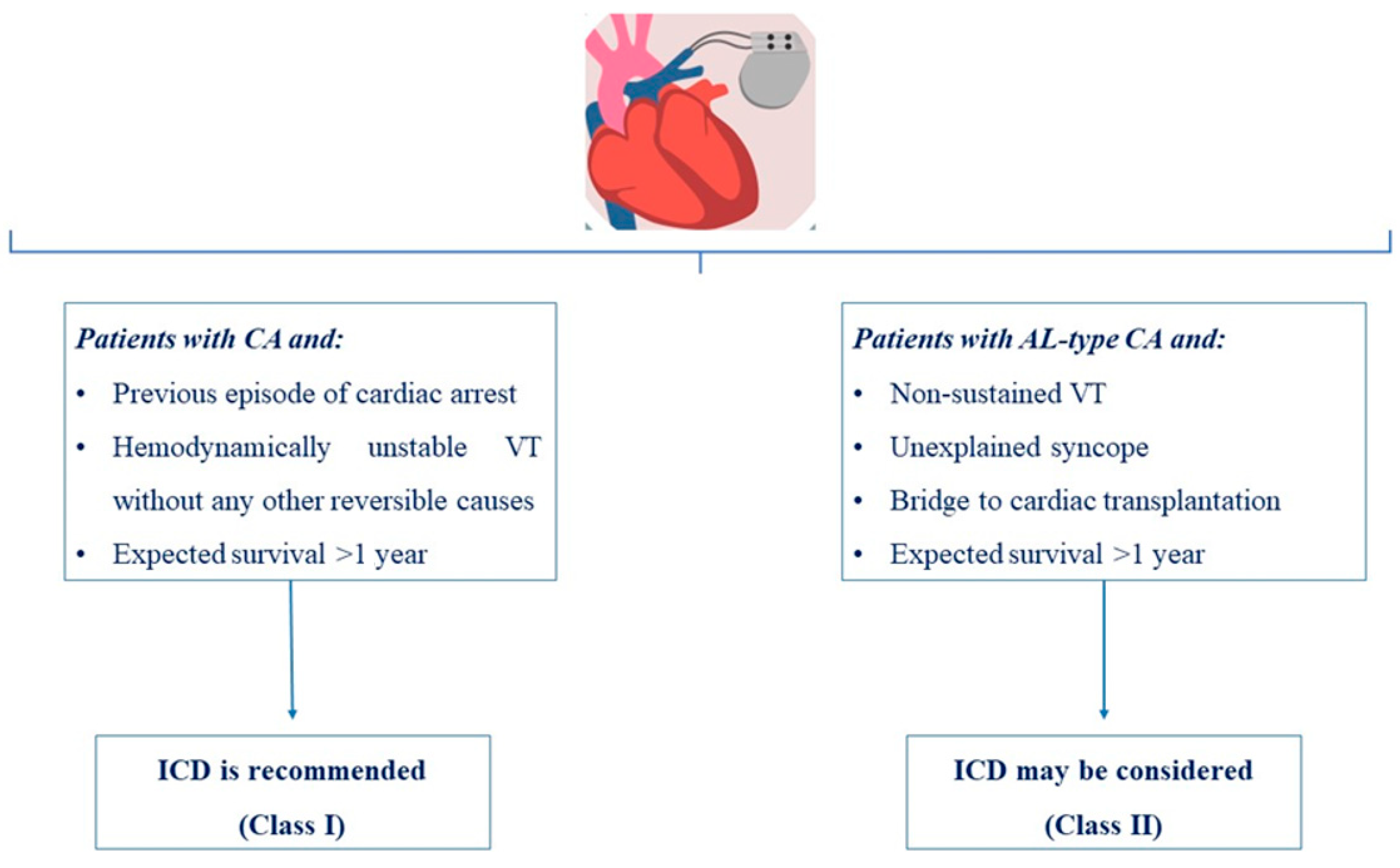
6. Device Therapy in Cardiac Amyloidosis
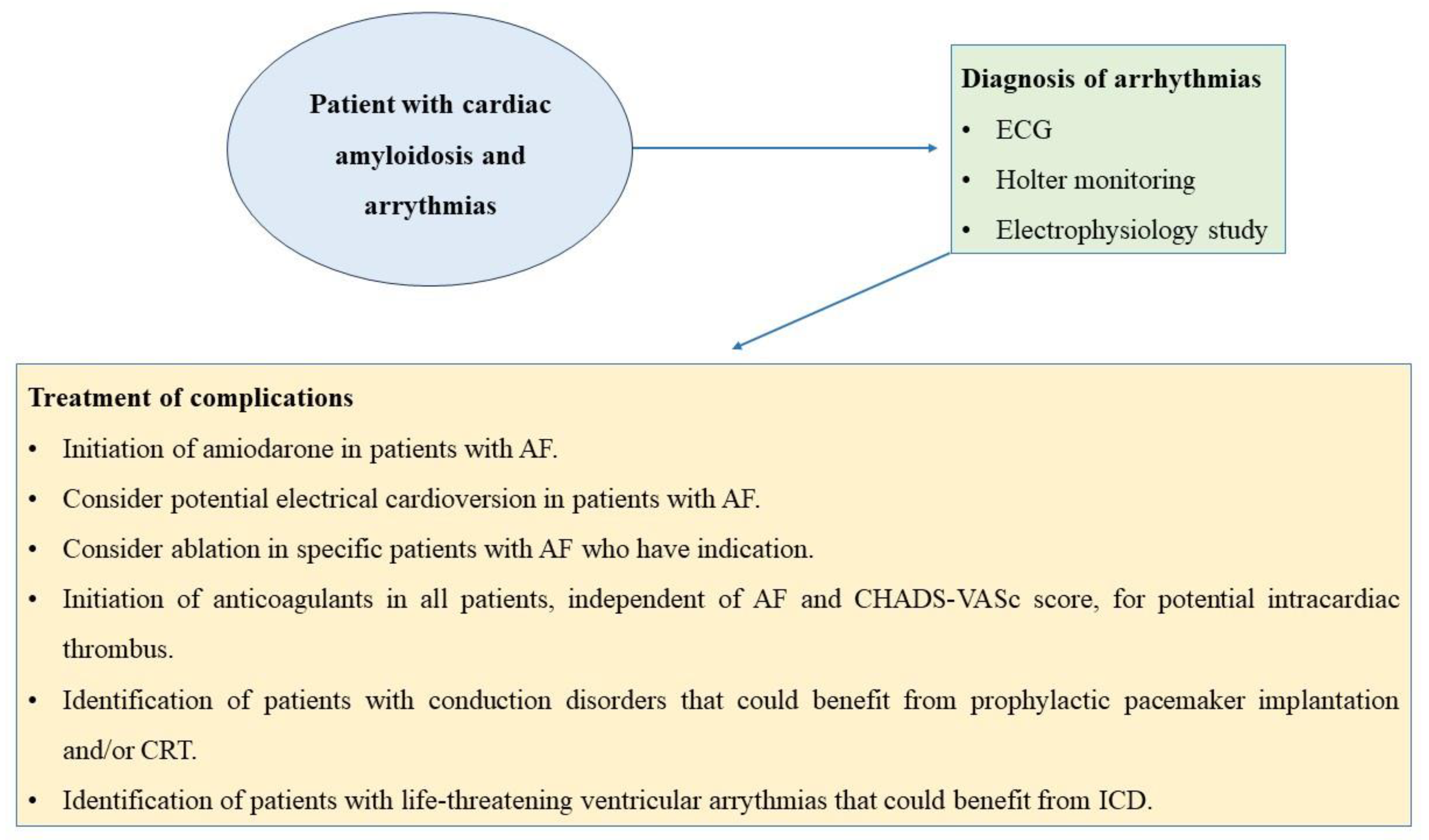
7. Clinical Management
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kristen, A.V.; Dengler, T.J.; Hegenbart, U.; Schönland, S.O.; Goldschmidt, H.; Breunig, F. Prophylactic implantation of cardioverter-defibrillator in patients with severe cardiac amyloidosis and high risk for sudden cardiac death. Heart Rhythm 2008, 5, 1425–1429. [Google Scholar] [CrossRef]
- Dubrey, S.W.; Hawkins, P.N.; Falk, R.H. Amyloid diseases of the heart: Assessment, diagnosis, and referral. Heart 2011, 97, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.; Lo, P.; Cho, K.; Subbiah, R. Ventricular Arrhythmias in Cardiac Amyloidosis: A Review of Current Literature. Clin. Med. Insights Cardiol. 2020, 14, 1179546820963055. [Google Scholar] [CrossRef]
- Ng, P.L.F.; Lim, Y.C.; Evangelista, L.K.M.; Wong, R.C.C.; Chai, P.; Sia, C.H.; Loi, H.Y.; Yeo, T.C.; Lin, W. Utility and pitfalls of the electrocardiogram in the evaluation of cardiac amyloidosis. Ann. Noninvasive Electrocardiol. 2022, 27, e12967. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, S.; Patel, H.P.; Chowdhury, M.; Patel, K.; Kumar, A.; Arora, S.; Zahid, S.; Goel, M.; Barssoum, K.; Jain, V.; et al. Impact of Arrhythmias on Hospitalizations in Patients With Cardiac Amyloidosis. Am. J. Cardiol. 2021, 143, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Argirò, A.; Del Franco, A.; Mazzoni, C.; Allinovi, M.; Tomberli, A.; Tarquini, R.; Di Mario, C.; Perfetto, F.; Cappelli, F.; Zampieri, M. Arrhythmic Burden in Cardiac Amyloidosis: What We Know and What We Do Not. Biomedicines 2022, 10, 2888. [Google Scholar] [CrossRef]
- Laptseva, N.; Rossi, V.A.; Sudano, I.; Schwotzer, R.; Ruschitzka, F.; Flammer, A.J.; Duru, F. Arrhythmic Manifestations of Cardiac Amyloidosis: Challenges in Risk Stratification and Clinical Management. J. Clin. Med. 2023, 12, 2581. [Google Scholar] [CrossRef]
- Boldrini, M.; Salinaro, F.; Mussinelli, R.; Raimondi, A.; Alogna, A.; Musca, F.; Palladini, G.; Merlini, G.; Perlini, S. Prevalence and prognostic value of conduction disturbances at the time of diagnosis of cardiac AL amyloidosis. Ann. Noninvasive Electrocardiol. 2013, 18, 327–335. [Google Scholar] [CrossRef]
- Cappelli, F.; Vignini, E.; Martone, R.; Perlini, S.; Mussinelli, R.; Sabena, A.; Morini, S.; Gabriele, M.; Taborchi, G.; Bartolini, S.; et al. Baseline ECG Features and Arrhythmic Profile in Transthyretin Versus Light Chain Cardiac Amyloidosis. Circ. Heart Fail. 2020, 13, e006619. [Google Scholar] [CrossRef]
- Longhi, S.; Quarta, C.C.; Milandri, A.; Lorenzini, M.; Gagliardi, C.; Manuzzi, L.; Bacchi-Reggiani, M.L.; Leone, O.; Ferlini, A.; Russo, A.; et al. Atrial fibrillation in amyloidotic cardiomyopathy: Prevalence, incidence, risk factors and prognostic role. Amyloid 2015, 22, 147–155. [Google Scholar] [CrossRef]
- Giancaterino, S.; Urey, M.A.; Darden, D.; Hsu, J.C. Management of Arrhythmias in Cardiac Amyloidosis. JACC Clin. Electrophysiol. 2020, 6, 351–361. [Google Scholar] [CrossRef] [PubMed]
- John, R.M. Arrhythmias in Cardiac Amyloidosis. J. Innov. Card. Rhythm Manag. 2018, 9, 3051–3057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis, K.; Cariou, E.; Colombat, M.; Ribes, D.; Huart, A.; Cintas, P.; Fournier, P.; Rollin, A.; Carrié, D.; Galinier, M.; et al. Atrial fibrillation and subtype of atrial fibrillation in cardiac amyloidosis: Clinical and echocardiographic features, impact on mortality. Amyloid 2019, 26, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Assaf, A.; Mekhael, M.; Noujaim, C.; Chouman, N.; Younes, H.; Kreidieh, O.; Marrouche, N.; Donnellan, E. Conduction system disease in cardiac amyloidosis. Trends Cardiovasc. Med. 2023, in press. [CrossRef]
- Donnellan, E.; Wazni, O.M.; Hanna, M.; Elshazly, M.B.; Puri, R.; Saliba, W.; Kanj, M.; Vakamudi, S.; Patel, D.R.; Baranowski, B.; et al. Atrial Fibrillation in Transthyretin Cardiac Amyloidosis: Predictors, Prevalence, and Efficacy of Rhythm Control Strategies. JACC Clin. Electrophysiol. 2020, 6, 1118–1127. [Google Scholar] [CrossRef]
- Barbhaiya, C.R.; Kumar, S.; Baldinger, S.H.; Michaud, G.F.; Stevenson, W.G.; Falk, R.; John, R.M. Electrophysiologic assessment of conduction abnormalities and atrial arrhythmias associated with amyloid cardiomyopathy. Heart Rhythm 2016, 13, 383–390. [Google Scholar] [CrossRef]
- Röcken, C.; Peters, B.; Juenemann, G.; Saeger, W.; Klein, H.U.; Huth, C.; Roessner, A.; Goette, A. Atrial amyloidosis: An arrhythmogenic substrate for persistent atrial fibrillation. Circulation 2002, 106, 2091–2097. [Google Scholar] [CrossRef] [Green Version]
- Ashraf, I.; Peck, M.M.; Maram, R.; Mohamed, A.; Ochoa Crespo, D.; Kaur, G.; Malik, B.H. Association of Arrhythmias in Cardiac Amyloidosis and Cardiac Sarcoidosis. Cureus 2020, 12, e9842. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Donnellan, E.; Elshazly, M.B.; Vakamudi, S.; Wazni, O.M.; Cohen, J.A.; Kanj, M.; Hanna, M.; Baranowski, B.; Saliba, W.; Jaber, W. No Association Between CHADS-VASc Score and Left Atrial Appendage Thrombus in Patients with Transthyretin Amyloidosis. JACC Clin. Electrophysiol. 2019, 5, 1473–1474. [Google Scholar] [CrossRef]
- Dumont, C.A.; Liprandi, M.I.S. Ventricular Arrythmias in Cardiac Amyloidosis: It is Possible to Prevent Sudden Death? ABC Heart Fail. Cardiomyop. 2021, 1, 103–111. [Google Scholar] [CrossRef]
- Palladini, G.; Malamani, G.; Cò, F.; Pistorio, A.; Recusani, F.; Anesi, E.; Garini, P.; Merlini, G. Holter monitoring in AL amyloidosis: Prognostic implications. Pacing Clin. Electrophysiol. 2001, 24, 1228–1233. [Google Scholar] [CrossRef]
- Goldsmith, Y.B.; Liu, J.; Chou, J.; Hoffman, J.; Comenzo, R.L.; Steingart, R.M. Frequencies and types of arrhythmias in patients with systemic light-chain amyloidosis with cardiac involvement undergoing stem cell transplantation on telemetry monitoring. Am. J. Cardiol. 2009, 104, 990–994. [Google Scholar] [CrossRef]
- Martini, N.; Sinigiani, G.; De Michieli, L.; Mussinelli, R.; Perazzolo Marra, M.; Iliceto, S.; Zorzi, A.; Perlini, S.; Corrado, D.; Cipriani, A. Electrocardiographic features and rhythm disorders in cardiac amyloidosis. Trends Cardiovasc. Med. 2023, in press. [CrossRef]
- Dubrey, S.W.; Cha, K.; Anderson, J.; Chamarthi, B.; Reisinger, J.; Skinner, M.; Falk, R.H. The clinical features of immunoglobulin light-chain (AL) amyloidosis with heart involvement. QJM 1998, 91, 141–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dale, Z.; Chandrashekar, P.; Al-Rashdan, L.; Kim, M.; Masri, A.; Nazer, B. Management Strategies for Atrial Fibrillation and Flutter in Patients with Transthyretin Cardiac Amyloidosis. Am. J. Cardiol. 2021, 157, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Shimizu, W.; Albert, C.M. The spectrum of epidemiology underlying sudden cardiac death. Circ. Res. 2015, 116, 1887–1906. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, B.; Patel, N.; Ho, K.; Amgai, B.; Okada, D.R.; Bandyopadhyay, D.; Krittanawong, C.; Wu, L.; Bhatia, K.; Shah, R.; et al. Incidence and Predictors of Sudden Cardiac Arrest in Sarcoidosis: A Nationwide Analysis. JACC Clin. Electrophysiol. 2021, 7, 1087–1095. [Google Scholar] [CrossRef]
- Lindow, T.; Lindqvist, P. The Prevalence of Advanced Interatrial Block and Its Relationship to Left Atrial Function in Patients with Transthyretin Cardiac Amyloidosis. J. Clin. Med. 2021, 10, 2764. [Google Scholar] [CrossRef]
- Reisinger, J.; Dubrey, S.W.; Lavalley, M.; Skinner, M.; Falk, R.H. Electrophysiologic abnormalities in AL (primary) amyloidosis with cardiac involvement. J. Am. Coll. Cardiol. 1997, 30, 1046–1051. [Google Scholar] [CrossRef] [Green Version]
- Roberts, W.C.; Waller, B.F. Cardiac amyloidosis causing cardiac dysfunction: Analysis of 54 necropsy patients. Am. J. Cardiol. 1983, 52, 137–146. [Google Scholar] [CrossRef]
- D’Errico, S.; Mazzanti, A.; Baldari, B.; Maiese, A.; Frati, P.; Fineschi, V. Sudden death in lambda light chain AL cardiac amyloidosis: A review of literature and update for clinicians and pathologists. Int. J. Clin. Exp. Pathol. 2020, 13, 1474–1482. [Google Scholar]
- Cheung, C.C.; Roston, T.M.; Andrade, J.G.; Bennett, M.T.; Davis, M.K. Arrhythmias in Cardiac Amyloidosis: Challenges in Risk Stratification and Treatment. Can. J. Cardiol. 2020, 36, 416–423. [Google Scholar] [CrossRef] [PubMed]
- El-Am, E.A.; Dispenzieri, A.; Melduni, R.M.; Ammash, N.M.; White, R.D.; Hodge, D.O.; Noseworthy, P.A.; Lin, G.; Pislaru, S.V.; Egbe, A.C.; et al. Direct Current Cardioversion of Atrial Arrhythmias in Adults with Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2019, 73, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Grogan, M.; Scott, C.G.; Kyle, R.A.; Zeldenrust, S.R.; Gertz, M.A.; Lin, G.; Klarich, K.W.; Miller, W.L.; Maleszewski, J.J.; Dispenzieri, A. Natural History of Wild-Type Transthyretin Cardiac Amyloidosis and Risk Stratification Using a Novel Staging System. J. Am. Coll. Cardiol. 2016, 68, 1014–1020. [Google Scholar] [CrossRef]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2018, 138, e210–e271. [Google Scholar] [CrossRef] [Green Version]
- Mathew, V.; Olson, L.J.; Gertz, M.A.; Hayes, D.L. Symptomatic conduction system disease in cardiac amyloidosis. Am. J. Cardiol. 1997, 80, 1491–1492. [Google Scholar] [CrossRef]
- Donnellan, E.; Wazni, O.; Kanj, M.; Elshazly, M.B.; Hussein, A.; Baranowski, B.; Hanna, M.; Patel, D.; Trulock, K.; Martyn, M.; et al. Atrial fibrillation ablation in patients with transthyretin cardiac amyloidosis. Europace 2020, 22, 259–264. [Google Scholar] [CrossRef]
- Maurer, M.S.; Hanna, M.; Grogan, M.; Dispenzieri, A.; Witteles, R.; Drachman, B.; Judge, D.P.; Lenihan, D.J.; Gottlieb, S.S.; Shah, S.J.; et al. Genotype and Phenotype of Transthyretin Cardiac Amyloidosis: THAOS (Transthyretin Amyloid Outcome Survey). J. Am. Coll. Cardiol. 2016, 68, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Dale, Z.; Chandrashekar, P.; Al-Rashdan, L.; Gill, S.; Elman, M.; Fischer, K.L.; Nazer, B.; Masri, A. Routine ambulatory heart rhythm monitoring for detection of atrial arrhythmias in transthyretin cardiac amyloidosis. Int. J. Cardiol. 2022, 358, 65–71. [Google Scholar] [CrossRef]
- Nicol, M.; Siguret, V.; Vergaro, G.; Aimo, A.; Emdin, M.; Dillinger, J.G.; Baudet, M.; Cohen-Solal, A.; Villesuzanne, C.; Harel, S.; et al. Thromboembolism and bleeding in systemic amyloidosis: A review. ESC Heart Fail. 2022, 9, 11–20. [Google Scholar] [CrossRef]
- Halligan, C.S.; Lacy, M.Q.; Vincent Rajkumar, S.; Dispenzieri, A.; Witzig, T.E.; Lust, J.A.; Fonseca, R.; Gertz, M.A.; Kyle, R.A.; Pruthi, R.K. Natural history of thromboembolism in AL amyloidosis. Amyloid 2006, 13, 31–36. [Google Scholar] [CrossRef]
- Cariou, E.; Sanchis, K.; Rguez, K.; Blanchard, V.; Cazalbou, S.; Fournier, P.; Huart, A.; Roussel, M.; Cintas, P.; Galinier, M.; et al. New Oral Anticoagulants vs. Vitamin K Antagonists Among Patients with Cardiac Amyloidosis: Prognostic Impact. Front. Cardiovasc. Med. 2021, 8, 742428. [Google Scholar] [CrossRef]
- Alkhawam, H.; Patel, D.; Nguyen, J.; Easaw, S.M.; Al-Sadawi, M.; Syed, U.; Zaiem, F.; Homsi, M.; Vittorio, T.J. Cardiac amyloidosis: Pathogenesis, clinical context, diagnosis and management options. Acta Cardiol. 2017, 72, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Nagarakanti, R.; Sankaramangalam, K.; Nagarakanti, S.; Moin, D.; Dulnuan, K.; Iyer, D.B. Cardiac Amyloidosis Wild Type (ATTR-CAwt) and Associated Cardiac Arrhythmias: A Case Report and Literature Review. Indian J. Clin. Cardiol. 2021, 2, 80–85. [Google Scholar] [CrossRef]
- Kristen, A.V. Amyloid cardiomyopathy. Herz 2020, 45, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Dispenzieri, A.; Kyle, R.; Grogan, M.; Brady, P.A. Implantable cardioverter defibrillators in patients with cardiac amyloidosis. J. Cardiovasc. Electrophysiol. 2013, 24, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, E.; Wazni, O.M.; Saliba, W.I.; Hanna, M.; Kanj, M.; Patel, D.R.; Wilner, B.; Kochar, A.; Jaber, W.A. Prevalence, incidence, and impact on mortality of conduction system disease in transthyretin cardiac amyloidosis. Am. J. Cardiol. 2020, 128, 140–146. [Google Scholar] [CrossRef]
- Donnellan, E.; Wazni, O.M.; Saliba, W.I.; Baranowski, B.; Hanna, M.; Martyn, M.; Patel, D.; Trulock, K.; Menon, V.; Hussein, A.; et al. Cardiac devices in patients with transthyretin amyloidosis: Impact on functional class, left ventricular function, mitral regurgitation, and mortality. J. Cardiovasc. Electrophysiol. 2019, 30, 2427–2432. [Google Scholar] [CrossRef]
- Algalarrondo, V.; Dinanian, S.; Juin, C.; Chemla, D.; Bennani, S.L.; Sebag, C.; Planté, V.; Le Guludec, D.; Samuel, D.; Adams, D.; et al. Prophylactic pacemaker implantation in familial amyloid polyneuropathy. Heart Rhythm 2012, 9, 1069–1075. [Google Scholar] [CrossRef]
- Adam, R.D.; Coriu, D.; Jercan, A.; Bădeliţă, S.; Popescu, B.A.; Damy, T.; Jurcuţ, R. Progress and challenges in the treatment of cardiac amyloidosis: A review of the literature. ESC Heart Fail. 2021, 8, 2380–2396. [Google Scholar] [CrossRef]
- Sayed, R.H.; Rogers, D.; Khan, F.; Wechalekar, A.D.; Lachmann, H.J.; Fontana, M.; Mahmood, S.; Sachchithanantham, S.; Patel, K.; Hawkins, P.N.; et al. A study of implanted cardiac rhythm recorders in advanced cardiac AL amyloidosis. Eur. Heart J. 2015, 36, 1098–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, R.M.; Stern, D.L. Use of Implantable Electronic Devices in Patients With Cardiac Amyloidosis. Can. J. Cardiol. 2020, 36, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Hamon, D.; Algalarrondo, V.; Gandjbakhch, E.; Extramiana, F.; Marijon, E.; Elbaz, N.; Selhane, D.; Dubois-Rande, J.L.; Teiger, E.; Plante-Bordeneuve, V.; et al. Outcome and incidence of appropriate implantable cardioverter-defibrillator therapy in patients with cardiac amyloidosis. Int. J. Cardiol. 2016, 222, 562–568. [Google Scholar] [CrossRef]
- Rezk, T.; Whelan, C.J.; Lachmann, H.J.; Fontana, M.; Sachchithanantham, S.; Mahmood, S.; Khan, F.; Khiani, R.; Tomson, J.; Youngstein, T.; et al. Role of implantable intracardiac defibrillators in patients with cardiac immunoglobulin light chain amyloidosis. Br. J. Haematol. 2018, 182, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Varr, B.C.; Zarafshar, S.; Coakley, T.; Liedtke, M.; Lafayette, R.A.; Arai, S.; Schrier, S.L.; Witteles, R.M. Implantable cardioverter-defibrillator placement in patients with cardiac amyloidosis. Heart Rhythm 2014, 11, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.; Eriksson, P.; Olofsson, B.O.; Thornell, L.E. The sinoatrial node in familial amyloidosis with polyneuropathy. A clinico-pathological study of nine cases from northern Sweden. Virchows Arch. A. Pathol. Anat. Histopathol. 1984, 402, 239–246. [Google Scholar] [CrossRef]
- Eriksson, P.; Olofsson, B.O. Pacemaker treatment in familial amyloidosis with polyneuropathy. Pacing Clin. Electrophysiol. 1984, 7, 702–706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briasoulis, A.; Kourek, C.; Papamichail, A.; Loritis, K.; Bampatsias, D.; Repasos, E.; Xanthopoulos, A.; Tsougos, E.; Paraskevaidis, I. Arrhythmias in Patients with Cardiac Amyloidosis: A Comprehensive Review on Clinical Management and Devices. J. Cardiovasc. Dev. Dis. 2023, 10, 337. https://doi.org/10.3390/jcdd10080337
Briasoulis A, Kourek C, Papamichail A, Loritis K, Bampatsias D, Repasos E, Xanthopoulos A, Tsougos E, Paraskevaidis I. Arrhythmias in Patients with Cardiac Amyloidosis: A Comprehensive Review on Clinical Management and Devices. Journal of Cardiovascular Development and Disease. 2023; 10(8):337. https://doi.org/10.3390/jcdd10080337
Chicago/Turabian StyleBriasoulis, Alexandros, Christos Kourek, Adamantia Papamichail, Konstantinos Loritis, Dimitrios Bampatsias, Evangelos Repasos, Andrew Xanthopoulos, Elias Tsougos, and Ioannis Paraskevaidis. 2023. "Arrhythmias in Patients with Cardiac Amyloidosis: A Comprehensive Review on Clinical Management and Devices" Journal of Cardiovascular Development and Disease 10, no. 8: 337. https://doi.org/10.3390/jcdd10080337