
“I Just Want You to Hear That Term”: Characterizing Language Used in Fetal Cardiology Consultations

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
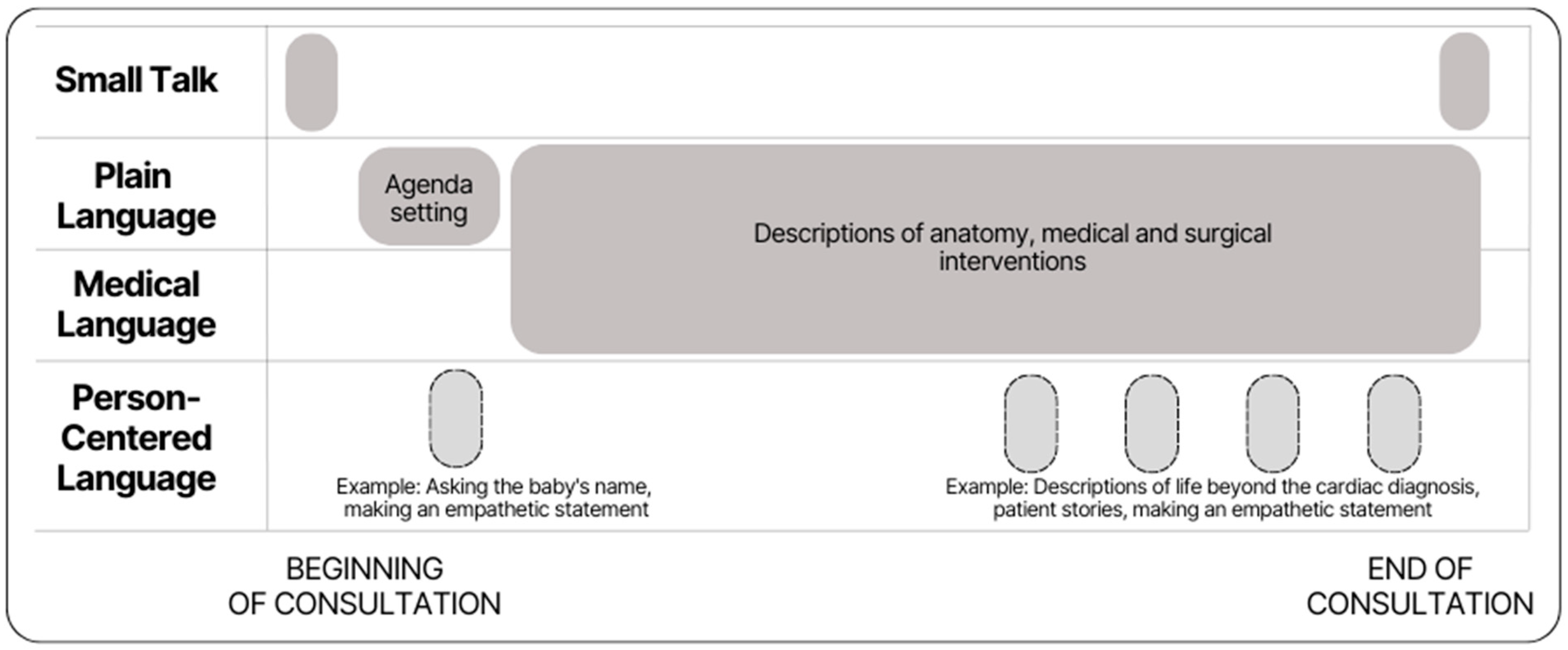
2.1. Design and Setting
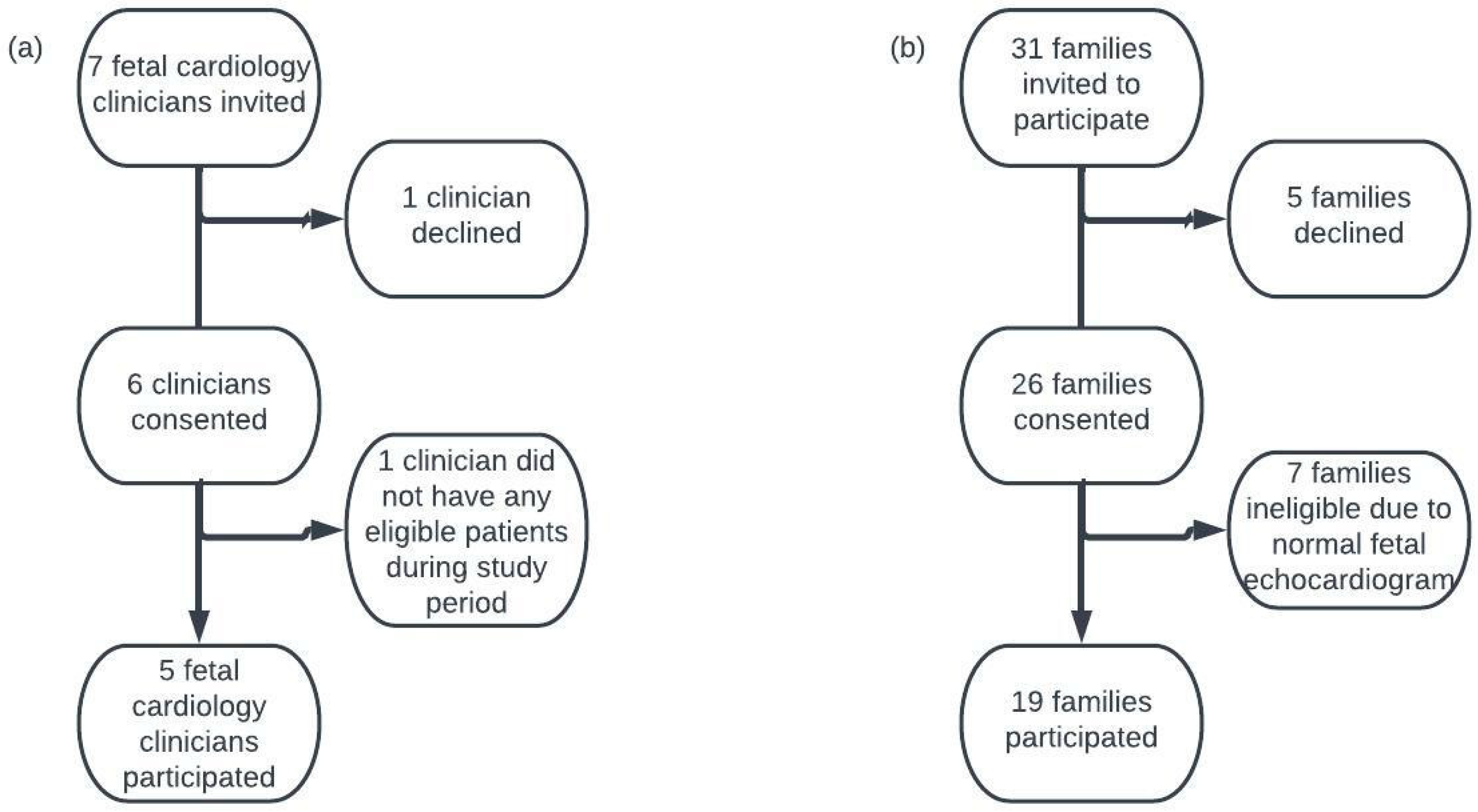
2.2. Participant Recruitment and Data Collection
2.3. Data Analysis
3. Results
3.1. Use of Plain Language to Define and Explain Medical Terms
3.2. Use of Plain Language as a Substitute for Medical Language
Mother: Okay. Can I just tell you how good it feels that you’re calling it a ‘difference’ and not a ‘defect’ because I had that issue with the twins. Doctors sometimes don’t choose their words very well and it makes you feel bad. So, I love that it’s called a ‘difference’.
Clinician: That’s what we call them here, but it’s good to know that that’s a better word for you to hear as well because we’re all different. Everybody’s different, and so just because your heart is formed differently doesn’t mean you’re defective. (C5, F4)
3.3. Use of Person-Centered Language
3.4. Use of Stories as a Person-Centered Language Strategy
Clinician: Do you guys watch winter Olympics at all?
Mother: Oh, we have, yeah.
Clinician: Do you know who Shaun White is, the snowboarder?
Mother: Oh, yeah.
Clinician: He has Tetralogy of Fallot.
Mother: I did not know that.
Clinician: So there you go … And they didn’t know, exactly, before he was born … But look at how well Shaun White, how athletic he is. (C3, F11)
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tacy, T.A.; Kasparian, N.A.; Karnik, R.; Geiger, M.; Sood, E. Opportunities to enhance parental well-being during prenatal counseling for congenital heart disease. Semin. Perinatol. 2022, 46, 151587. [Google Scholar] [CrossRef]
- Simpson, M.; Buckman, R.; Stewart, M.; Maguire, P.; Lipkin, M.; Novack, D.; Till, J. Doctor-patient communication: The Toronto consensus statement. BMJ 1991, 303, 1385–1387. [Google Scholar] [CrossRef]
- Franklin, R.C.; Jacobs, J.P.; Krogmann, O.N.; Béland, M.J.; Aiello, V.D.; Colan, S.D.; Elliott, M.J.; Gaynor, J.W.; Kurosawa, H.; Maruszewski, B.; et al. Nomenclature for congenital and paediatric cardiac disease: Historical perspectives and The International Pediatric and Congenital Cardiac Code. Cardiol. Young 2008, 18 (Suppl. S2), 70–80. [Google Scholar] [CrossRef] [PubMed]
- Weiss, B. Health literacy and patient safety: Help patients understand. In Manual for Clinicians; American Medical Association: Chicago, IL, USA, 2007. [Google Scholar]
- Brega, A.G.B.J.; Barnard, J.; Mabachi, N.M.; Weiss, B.; DeWalt, D.; Brach, C.; Cifuentes, M.; Albright, K.; West, D. AHRQ Health Literacy Universal Precautions Toolkit; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- US General Services Administration. Federal Plain Language Guidelines. May 2011. Available online: https://www.plainlanguage.gov/guidelines/ (accessed on 24 April 2023).
- Farrell, M.; Deuster, L.; Donovan, J.; Christopher, S. Pediatric Residents’ Use of Jargon During Counseling About Newborn Genetic Screening Results. Pediatrics 2008, 122, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Tallman, K.; Janisse, T.; Frankel, R.M.; Sung, S.H.; Krupat, E.; Hsu, J.T. Communication practices of physicians with high patient-satisfaction ratings. Perm. J. 2007, 11, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Street, R.L.; Makoul, G.; Arora, N.K.; Epstein, R.M. How does communication heal? Pathways linking clinician–patient communication to health outcomes. Patient Educ. Couns. 2009, 74, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.W.; Brelsford, K.M.; Kavanaugh-McHugh, A.; Clayton, E.W. Uncertainty of Prenatally Diagnosed Congenital Heart Disease: A Qualitative Study. JAMA Netw. Open 2020, 3, e204082. [Google Scholar] [CrossRef]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice; Sage Publications: Los Angeles, CA, USA, 2014. [Google Scholar]
- Harris, K.W.; Schweiberger, K.; Kavanaugh-McHugh, A.; Arnold, R.M.; Merlin, J.; Kasparian, N.A.; Chang, J.C. Introducing Uncertainty: An Observational Study of Conversations on Prenatal Diagnosis of Complex Congenital Heart Disease (Sci238). J. Pain Symptom Manag. 2023, 65, e660–e661. [Google Scholar] [CrossRef]
- Schweiberger, K.; Harris, K.W.; Chang, J.C.; Kavanaugh-McHugh, A.; Arnold, R.M.; Merlin, J.S.; Kasparian, N.A. Conversation Structure of Initial Fetal Cardiology Consultations. In International Conference on Communication in Healthcare; Patient Education and Counseling: Rio del Mar, Puerto Rico, 2023. [Google Scholar]
- Allan, L.D.; Huggon, I.C. Counseling following a diagnosis of congenital heart disease. Prenat. Diagn. 2004, 24, 1136–1142. [Google Scholar] [CrossRef]
- “Small Talk, n”. OED Online, Oxford University Press, June 2023. Available online: www.oed.com (accessed on 28 June 2023).
- Tran, B.Q.; Sweeny, K. Correlates of Physicians’ and Patients’ Language Use during Surgical Consultations. Health Commun. 2020, 35, 1248–1255. [Google Scholar] [CrossRef]
- Bagley, C.; Hunter, A.; Bacarese-Hamilton, I. Patients’ misunderstanding of common orthopaedic terminology: The need for clarity. Ann. R. Coll. Surg. Engl. 2011, 93, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Gotlieb, R.; Praska, C.; Hendrickson, M.A.; Marmet, J.; Charpentier, V.; Hause, E.; Allen, K.A.; Lunos, S.; Pitt, M.B. Accuracy in Patient Understanding of Common Medical Phrases. JAMA Netw. Open 2022, 5, e2242972. [Google Scholar] [CrossRef]
- Stableford, S.; Mettger, W. Plain language: A strategic response to the health literacy challenge. J. Public Health Policy 2007, 28, 71–93. [Google Scholar] [CrossRef] [PubMed]
- Ogden, J.; Branson, R.; Bryett, A.; Campbell, A.; Febles, A.; Ferguson, I.; Lavender, H.; Mizan, J.; Simpson, R.; Tayler, M. What’s in a name? An experimental study of patients’ views of the impact and function of a diagnosis. Fam. Pract. 2003, 20, 248–253. [Google Scholar] [CrossRef]
- Wiener, R.S.; Gould, M.K.; Woloshin, S.; Schwartz, L.M.; Clark, J.A. What do you mean, a spot?: A qualitative analysis of patients’ reactions to discussions with their physicians about pulmonary nodules. Chest 2013, 143, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Weis, B. Health Literacy: A Manual for Clinicians; American Medical Association, American Medical Foundation: Chicago, IL, USA, 2003. [Google Scholar]
- Bottema-Beutel, K.; Kapp, S.K.; Lester, J.N.; Sasson, N.J.; Hand, B.N. Avoiding Ableist Language: Suggestions for Autism Researchers. Autism Adulthood 2020, 3, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Bury, S.M.; Jellett, R.; Spoor, J.R.; Hedley, D. “It Defines Who I Am” or “It’s Something I Have”: What Language Do [Autistic] Australian Adults [on the Autism Spectrum] Prefer? J. Autism Dev. Disord. 2023, 53, 677–687. [Google Scholar] [CrossRef] [PubMed]
- National Association of the Deaf. Community and Culture-Frequently Asked Questions. 2023. Available online: https://www.nad.org/resources/american-sign-language/community-and-culture-frequently-asked-questions/ (accessed on 4 May 2023).
- Garza, I.V.; Cox, J.; Sadat, B.; De la Garza, B.; Chatila, K.F. #Wordsmatter: Patient Perception on Heart Failure Disease and Terminology Preference. J. Am. Coll. Cardiol. 2023, 81 (Suppl. S8), 362. [Google Scholar]
- Puhl, R.; Peterson, J.L.; Luedicke, J. Motivating or stigmatizing? Public perceptions of weight-related language used by health providers. Int. J. Obes. 2013, 37, 612–619. [Google Scholar] [CrossRef]
- Hashim, M.J. Patient-Centered Communication: Basic Skills. Am. Fam. Physician 2017, 95, 29–34. [Google Scholar]
- de Crespigny, L. Words matter: Nomenclature and communication in perinatal medicine. Clin. Perinatol. 2003, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Charon, R.; Montello, M. Stories Matter: The Role of Narrative in Medical Ethics; Routledge: New York, NY, USA, 2004. [Google Scholar]
- Kulish, N. The Power of Stories. J. Am. Psychoanal. Assoc. 2022, 70, 829–844. [Google Scholar] [CrossRef] [PubMed]
- Hilton-Kamm, D.; Sklansky, M.; Chang, R.-K. How not to tell parents about their child’s new diagnosis of congenital heart disease: An internet survey of 841 parents. Pediatr. Cardiol. 2014, 35, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Alkazaleh, F.; Thomas, M.; Grebenyuk, J.; Glaude, L.; Savage, D.; Johannesen, J.; Caetano, M.; Windrim, R. What women want: Women’s preferences of caregiver behavior when prenatal sonography findings are abnormal. Ultrasound Obstet. Gynecol. 2004, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, A.; Wacker-Gussmann, A.; Bär, S.; Elsässer, M.; Mohammadi Motlagh, A.; Ostermayer, E.; Oberhoffer-Fritz, R.; Ewert, P.; Gorenflo, M.; Starystach, S. Parents’ Perspectives on Counseling for Fetal Heart Disease: What Matters Most? J. Clin. Med. 2022, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.; Gaskin, K. Parents’ experiences of receiving an antenatal versus postnatal diagnosis of complex congenital heart disease. Nurs. Child. Young People 2018, 30, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Bertaud, S.; Lloyd, D.F.A.; Sharland, G.; Razavi, R.; Bluebond-Langner, M. The impact of prenatal counselling on mothers of surviving children with hypoplastic left heart syndrome: A qualitative interview study. Health Expect. 2020, 23, 1224–1230. [Google Scholar] [CrossRef]
- Ashtiani, S.; Makela, N.; Carrion, P.; Austin, J. Parents’ experiences of receiving their child’s genetic diagnosis: A qualitative study to inform clinical genetics practice. Am. J. Med. Genet. Part A 2014, 164, 1496–1502. [Google Scholar] [CrossRef]
- Arya, B.; Glickstein, J.S.; Levasseur, S.M.; Williams, I.A. Parents of Children with Congenital Heart Disease Prefer More Information than Cardiologists Provide. Congenit. Heart Dis. 2013, 8, 78–85. [Google Scholar] [CrossRef]
- Lalor, J.G.; Begley, C.M.; Galavan, E. A grounded theory study of information preference and coping styles following antenatal diagnosis of foetal abnormality. J. Adv. Nurs. 2008, 64, 185–194. [Google Scholar] [CrossRef]
- Sood, E.; Karpyn, A.; Demianczyk, A.C.; Ryan, J.; Delaplane, E.A.; Neely, T.; Frazier, A.H.; Kazak, A.E. Mothers and Fathers Experience Stress of Congenital Heart Disease Differently: Recommendations for Pediatric Critical Care. Pediatr. Crit. Care Med. 2018, 19, 626. [Google Scholar] [CrossRef]
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. Diagnosis and Treatment of Fetal Cardiac Disease. Circulation 2014, 129, 2183–2242. [Google Scholar] [CrossRef]
- Keelan, J.A.; Moon Grady, A.J.; Arya, B.; Donofrio, M.T.; Schidlow, D.N.; Tacy, T.A.; Stern, K.W.; Geiger, M.K. Current State of Fetal Heart Disease Counseling and Training: Room for Improvement? Pediatr. Cardiol. 2022, 43, 1548–1558. [Google Scholar] [CrossRef]
- Bellander, T.; Karlsson, A.-M. Patient participation and learning in medical consultations about congenital heart defects. PLoS ONE 2019, 14, e0220136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | n | % | |
|---|---|---|---|
| Clinicians (n = 5) | Institutions trained at for residency and fellowship, n | 5 | |
| Time practicing at current institution median (IQR), years | 10 (2) | ||
| Initial Fetal Cardiology Consultations (n = 19) | Duration of counselling, median (IQR), minutes | 37 (25) | |
| Partner(s) present | 14 | 74 | |
| Other children present | 3 | 16 | |
| Language interpreter present | 1 | 5 | |
| Pregnant Persons (n = 19) | Gestation at first visit, median (IQR), weeks | 26 (7) | |
| Native language | |||
| English | 15 | 79 | |
| Spanish | 1 | 5 | |
| Arabic | 1 | 5 | |
| Kurdish | 1 | 5 | |
| Unspecified African Dialect | 1 | 5 | |
| Race/Ethnicity | |||
| White (European) | 14 | 74 | |
| White (Middle Eastern) | 2 | 11 | |
| Black/African American | 2 | 11 | |
| Hispanic/Latina | 1 | 5 | |
| Family history of CHD | 5 | 26 | |
| Self-identify as a “mother” | 19 | 100 | |
| CHD Diagnoses (n = 19) | Lower risk of mortality 1 | ||
| Coarctation of the Aorta | 2 | 11 | |
| Tetralogy of Fallot | 2 | 11 | |
| Transposition of the Great Arteries (simple) | 1 | 5 | |
| Pulmonary Stenosis | 2 | 11 | |
| Atrioventricular Septal Defect | 1 | 5 | |
| Vessel aneurysm | 2 | 11 | |
| Higher risk of mortality 1 | |||
| Ebstein Anomaly (severe) | 1 | 5 | |
| Hypoplastic Left Heart Syndrome | 2 | 11 | |
| Hypoplastic Right Heart Syndrome | 2 | 11 | |
| Transposition of the Great Arteries (complex) | 1 | 5 | |
| Pulmonary Atresia | 1 | 5 | |
| Double outlet right ventricle and other anomalies | 1 | 5 | |
| Autoimmune complete heart block | 1 | 5 | |
| Discourse Style | Definition | Use | Examples |
|---|---|---|---|
| Medical Language | Medical terminology or jargon | Used to describe anatomy, procedures, and medications. Also used to familiarize families with the terms | “She might actually be what we call “balanced” because of the difference, which is the pulmonary stenosis”. (Clinician 4 to Family 4) “This is one of the heart lesions that we do see intrauterine fetal demise in”. (Clinician 2 to Family 2) |
| Plain Language | Clear, straight-forward communication using everyday words [6] | Used to define and explain the meaning of medical language | “Once baby’s born, it’s not uncommon that people would hear a murmur from it, which is just a sound that you hear from differences in how blood flow can move, especially if you have something with one of the valves that’s different”. (Clinician 4 to Family 4) “We call this … there’s many names and I’m going to put a bunch of terms on here, hypoplastic, right-heart syndrome, which just means small right heart”. (Clinician 1 to Family 13) “Instead of being this nice small vessel, some people get big baggy blood vessels there. It is called a ductal aneurysm. Okay? And aneurysm sounds like a terrible word, but what it really means is a big baggy thing”. (Clinician 1 to Family 17) |
| Used as a substitute for medical language | “And though one blood vessel itself is small, so we would say hypoplasia or smallness of the pulmonary artery … So the tricuspid valve is small, the pump is small and the way out is small and actually, sealed over”. (Clinician 1 to Family 13) “We agree with the diagnosis of the hole in the heart”. (Clinician 5 to Family 4) | ||
| Person-Centered Language | Emphasized the person prior to the disease (i.e., person-first language), or acknowledged the person’s experience as opposed to talking about them objectively | Used to emphasize the baby as a whole person | “We’re all different. Everybody’s different, and so just because your heart is formed differently doesn’t mean you’re defective”. (Clinician 5 to Family 4) “His pump is different but I know a lot of very neat people who are like him in our world”. (Clinician 1 to Family 13) “We’re all a little different on the outside. We can be a little different on the inside” (Clinician 1 to Family 17) |
| Use of person-first language | “Typically, people with Tetralogy of Fallot lead full lives but they do have extra medical needs that will require checkups”. (Clinician 2 to Family 11) | ||
| Use of stories | “But real stories from patients I’ve taken care of, one young lady who was a gymnast and she said, ‘I can vault, but I can’t do floor exercise. That’s too long.’” (Clinician 1 to Family 13) | ||
| Small Talk | Polite conversation about non-sensitive matters [15] | Used to establish rapport with the family | Clinician: I’ve lived in [redact] for [redact] years. You would think I would know where everything is and I still don’t. So I was just trying to get my head around where you lived. So between here and your house is how far time-wise, when you get in your car? Mother: Hour and a half. Clinician: Still good amount. Mother: Without traffic. (Clinician 1 to Family 1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweiberger, K.; Harris, K.W.; Kavanaugh-McHugh, A.; Soudi, A.; Arnold, R.M.; Merlin, J.S.; Kasparian, N.A.; Chang, J.C. “I Just Want You to Hear That Term”: Characterizing Language Used in Fetal Cardiology Consultations. J. Cardiovasc. Dev. Dis. 2023, 10, 394. https://doi.org/10.3390/jcdd10090394
Schweiberger K, Harris KW, Kavanaugh-McHugh A, Soudi A, Arnold RM, Merlin JS, Kasparian NA, Chang JC. “I Just Want You to Hear That Term”: Characterizing Language Used in Fetal Cardiology Consultations. Journal of Cardiovascular Development and Disease. 2023; 10(9):394. https://doi.org/10.3390/jcdd10090394
Chicago/Turabian StyleSchweiberger, Kelsey, Kelly W. Harris, Ann Kavanaugh-McHugh, Abdesalam Soudi, Robert M. Arnold, Jessica S. Merlin, Nadine A. Kasparian, and Judy C. Chang. 2023. "“I Just Want You to Hear That Term”: Characterizing Language Used in Fetal Cardiology Consultations" Journal of Cardiovascular Development and Disease 10, no. 9: 394. https://doi.org/10.3390/jcdd10090394
APA StyleSchweiberger, K., Harris, K. W., Kavanaugh-McHugh, A., Soudi, A., Arnold, R. M., Merlin, J. S., Kasparian, N. A., & Chang, J. C. (2023). “I Just Want You to Hear That Term”: Characterizing Language Used in Fetal Cardiology Consultations. Journal of Cardiovascular Development and Disease, 10(9), 394. https://doi.org/10.3390/jcdd10090394