
The Role of Cardiovascular Magnetic Resonance in Patients with Mitral Regurgitation
 , ,
, ,  , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. How to “MRI” a Mitral Valve?
1.1. Mitral Valve Apparatus Assessment
1.2. Ventricular Volume and Function
1.3. Tissue Characterization
1.4. Mitral Regurgitation Quantification
1.4.1. 2D Phase Contrast (PC) Velocity Mapping
1.4.2. Quantitative Assessment of MR with CMR
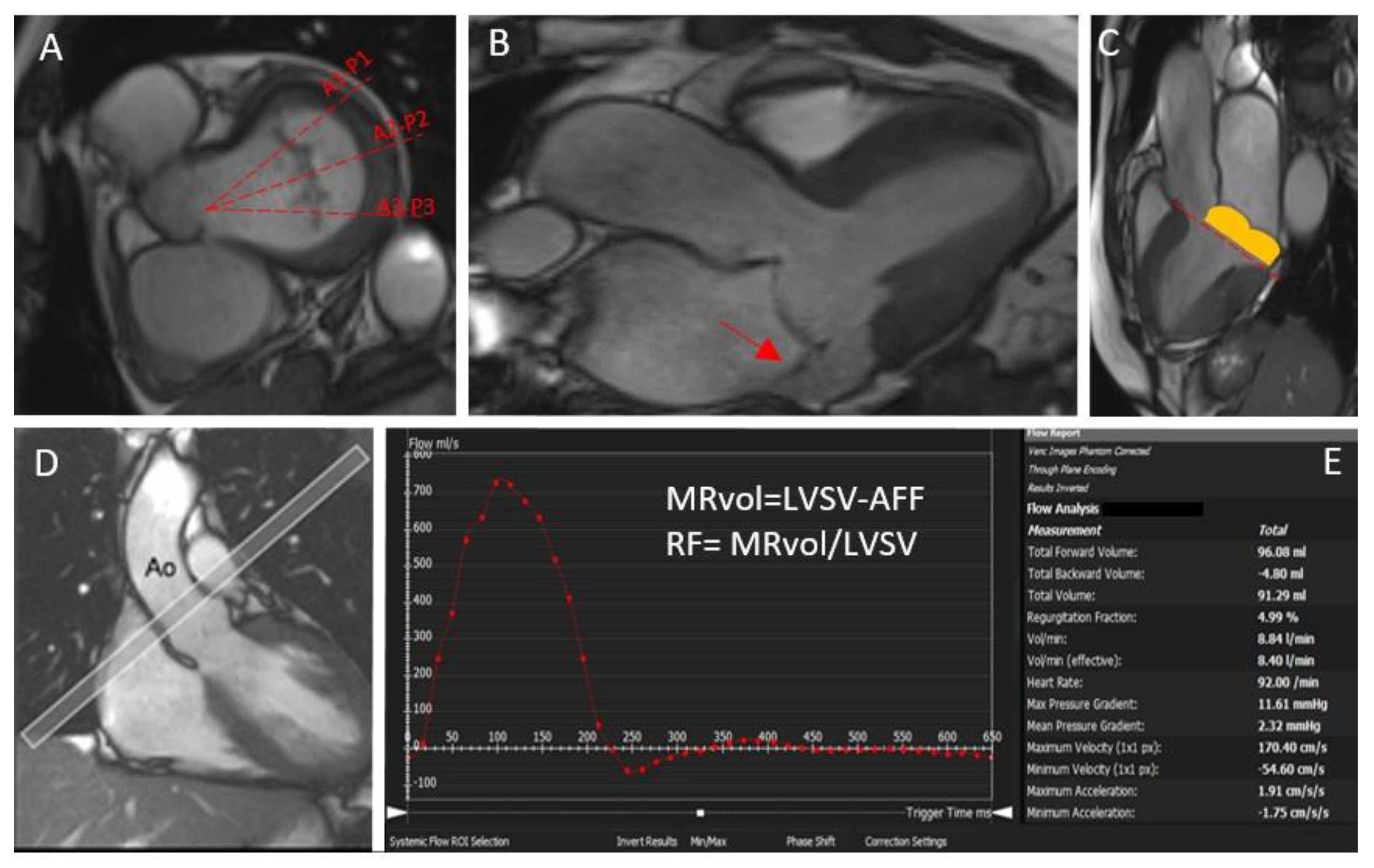
- The standard approach implies the quantification of MRvol and MR RF considering the difference between the LV stroke volume calculated using the planimetry of SSFP images and the aortic (systolic) forward volume obtained by phase-contrast images (AoPC).
- If no other valve regurgitation or haemodynamically significant shunt are present, the MRvol can be derived by the difference between the LV stroke volume and the RV stroke volume calculated using the planimetry of SSFP images. It must be noted that, given the relatively lower precision with which the RV stroke volume is quantified compared with the LV stroke volume, intra- and inter-observed variability is lower compared with other methods [11].
- The difference between the mitral inflow stroke volume and the AoPC. If this method is suitable for patients with multiple valve regurgitations, the fact that 2D phase-contrast CMR requires static imaging planes and cannot adapt to valve motion may result in some inaccuracy [12].
- Finally, if 4D-flow is available, a direct quantification of the MR flow with retrospective mitral valve tracking can also be performed. MR jets are quantified by defining a systolic reformatted plane perpendicular to the single jet or individually for multiple jets. Otherwise, a reconstructed aortic plane using the retrospective valve-tracking method can be used to quantify AoPC. This measurement can then be used to quantify the MR volume or fraction using the standard LVSV–AoPC method.
1.4.3. 4D Flow
2. Echocardiography and Cardiovascular Magnetic Resonance: Friends or Foes?
3. What Is the Role of CMR in Primary Mitral Regurgitation?
Arrhythmic Mitral Valve Prolapse
4. What Is the Role of MRI in Secondary Mitral Regurgitation?
5. Future Steps
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Doherty, J.U.; Kort, S.; Mehran, R.; Schoenhagen, P.; Soman, P. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate Use Criteria for Multimodality Imaging in Valvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardio-vascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2017, 70, 1647–1672. [Google Scholar] [CrossRef] [PubMed]
- Landi, A.; Faletra, F.F.; Pavon, A.G.; Pedrazzini, G.; Valgimigli, M. From secondary to tertiary mitral regurgitation: The paradigm shifts, but uncertainties remain. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Swift, A.J.; Zhong, L.; Carlhäll, C.-J.; Ebbers, T.; Westenberg, J.; Hope, M.D.; Bucciarelli-Ducci, C.; Bax, J.J.; Myerson, S.G. Assessment of mitral valve regurgitation by cardiovascular magnetic resonance imaging. Nat. Rev. Cardiol. 2019, 17, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef]
- Le Goffic, C.; Toledano, M.; Ennezat, P.-V.; Binda, C.; Castel, A.-L.; Delelis, F.; Graux, P.; Tribouilloy, C.; Maréchaux, S. Quantitative Evaluation of Mitral Regurgitation Secondary to Mitral Valve Prolapse by Magnetic Resonance Imaging and Echocardiography. Am. J. Cardiol. 2015, 116, 1405–1410. [Google Scholar] [CrossRef]
- Topilsky, Y.; Michelena, H.; Bichara, V.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Mitral valve prolapse with mid-late systolic mitral regurgitation: Pitfalls of evaluation and clinical outcome compared with holosystolic regurgitation. Circulation 2012, 125, 1643–1651. [Google Scholar] [CrossRef] [Green Version]
- Vincenti, G.; Masci, P.G.; Rutz, T.; De Blois, J.; Prša, M.; Jeanrenaud, X.; Schwitter, J.; Monney, P. Impact of bileaflet mitral valve prolapse on quantification of mitral regurgitation with cardiac magnetic resonance: A single-center study. J. Cardiovasc. Magn. Reson. 2017, 19, 56. [Google Scholar] [CrossRef] [Green Version]
- Pelc, N.J.; Herfkens, R.J.; Shimakawa, A.; Enzmann, D.R. Phase contrast cine magnetic resonance imaging. Magn. Reson. Q. 1991, 7, 229–254. [Google Scholar]
- Nayak, K.S.; Hu, B.S.; Nishimura, D.G. Rapid quantitation of high-speed flow jets. Magn. Reson. Med. 2003, 50, 366–372. [Google Scholar] [CrossRef] [Green Version]
- Kon, M.W.S.; Myerson, S.; Moat, N.E.; Pennell, D.J. Quantification of regurgitant fraction in mitral regurgitation by cardiovascular magnetic resonance: Comparison of techniques. J. Heart Valve Dis. 2004, 13, 600–607. [Google Scholar] [PubMed]
- Calkoen, E.E.; Roest, A.A.; Kroft, L.J.; van der Geest, R.J.; Jongbloed, M.R.; Bsc, P.J.V.D.B.; Blom, N.A.; Hazekamp, M.G.; De Roos, A.; Westenberg, J.J. Characterization and improved quantification of left ventricular inflow using streamline visualization with 4DFlow MRI in healthy controls and patients after atrioventricular septal defect correction. J. Magn. Reson. Imaging 2014, 41, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Dyverfeldt, P.; Bissell, M.; Barker, A.J.; Bolger, A.F.; Carlhäll, C.-J.; Ebbers, T.; Francios, C.J.; Frydrychowicz, A.; Geiger, J.; Giese, D.; et al. 4D flow cardiovascular magnetic resonance consensus statement. J. Cardiovasc. Magn. Reson. 2015, 17, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.N.; Avery, R.; Soulat, G.; Allen, B.D.; Collins, J.D.; Choudhury, L.; Bonow, R.O.; Carr, J.; Markl, M.; Elbaz, M.S.M. Direct mitral regurgitation quantification in hypertrophic cardiomyopathy using 4D flow CMR jet tracking: Evaluation in comparison to conventional CMR. J. Cardiovasc. Magn. Reson. 2021, 23, 138. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Gupta, A.N.; Ma, L.E.; Scott, M.B.; Mason, O.R.; Wu, E.; Thomas, J.D.; Markl, M. Valvular regurgitation flow jet assessment using in vitro 4D flow MRI: Implication for mitral regurgitation. Magn. Reson. Med. 2021, 87, 1923–1937. [Google Scholar] [CrossRef]
- Fidock, B.; Archer, G.; Barker, N.; Elhawaz, A.; Al-Mohammad, A.; Rothman, A.; Hose, R.; Hall, I.R.; Grech, E.; Briffa, N.; et al. Standard and emerging CMR methods for mitral regurgitation quantification. Int. J. Cardiol. 2021, 331, 316–321. [Google Scholar] [CrossRef]
- Blanken, C.P.S.; Westenberg, J.J.M.; Aben, J.-P.; Bijvoet, G.P.; Chamuleau, S.A.J.; Boekholdt, S.M.; Nederveen, A.J.; Leiner, T.; Van Ooij, P.; Planken, R.N. Quantification of Mitral Valve Regurgitation from 4D Flow MRI Using Semiautomated Flow Tracking. Radiol. Cardiothorac. Imaging 2020, 2, e200004. [Google Scholar] [CrossRef]
- Ma, L.E.; Yerly, J.; Piccini, D.; Di Sopra, L.; Roy, C.W.; Carr, J.C.; Rigsby, C.K.; Kim, D.; Stuber, M.; Markl, M. 5D Flow MRI: A Fully Self-gated, Free-running Framework for Cardiac and Respiratory Motion–resolved 3D Hemodynamics. Radiol. Cardiothorac. Imaging 2020, 2, e200219. [Google Scholar] [CrossRef]
- Falcão, M.B.L.; Di Sopra, L.; Ma, L.; Bacher, M.; Yerly, J.; Speier, P.; Rutz, T.; Prša, M.; Markl, M.; Stuber, M.; et al. Pilot tone navigation for respiratory and cardiac motion-resolved free-running 5D flow MRI. Magn. Reson. Med. 2021, 87, 718–732. [Google Scholar] [CrossRef]
- Uretsky, S.; Gillam, L.; Lang, R.; Chaudhry, F.A.; Argulian, E.; Supariwala, A.; Gurram, S.; Jain, K.; Subero, M.; Jang, J.J.; et al. Discordance between echocardiography and MRI in the assessment of mitral regurgitation severity: A prospective multicenter trial. J. Am. Coll. Cardiol. 2015, 65, 1078–1088. [Google Scholar] [CrossRef] [Green Version]
- Grayburn, P.A.; Bhella, P. Grading Severity of Mitral Regurgitation by Echocardiography: Science or Art? JACC Cardiovasc. Imaging 2010, 3, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Uretsky, S.; Argulian, E.; Supariwala, A.; Marcoff, L.; Koulogiannis, K.; Aldaia, L.; Chaudhry, F.A.; Wolff, S.D.; Gillam, L.D. A Comparative Assessment of Echocardiographic Parameters for Determining Primary Mitral Regurgitation Severity Using Magnetic Resonance Imaging as a Reference Standard. J. Am. Soc. Echocardiogr. 2018, 31, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Uretsky, S.; Animashaun, I.B.; Sakul, S.; Aldaia, L.; Marcoff, L.; Koulogiannis, K.; Argulian, E.; Rosenthal, M.; Wolff, S.D.; Gillam, L.D. American Society of Echocardiography Algorithm for Degenerative Mitral Regurgitation: Comparison With CMR. JACC Cardiovasc. Imaging 2022, 15, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, V.; Hannoush, H.; Sidenko, S.; Saba, S.G.; Sears-Rogan, P.; Bandettini, W.P.; Brofferio, A.; Shanbhag, S.M.; Brenneman, C.L.; Horvath, K.A.; et al. Are Echocardiography and CMR Really Discordant in Mitral Regurgitation? JACC Cardiovasc. Imaging 2017, 10, 823–824. [Google Scholar] [CrossRef]
- Cawley, P.J.; Hamilton-Craig, C.; Owens, D.S.; Krieger, E.V.; Strugnell, W.E.; Mitsumori, L.; D’Jang, C.L.; Schwaegler, R.G.; Nguyen, K.Q.; Nguyen, B.; et al. Prospective Comparison of Valve Regurgitation Quantitation by Cardiac Magnetic Resonance Imaging and Transthoracic Echocardiography. Circ. Cardiovasc. Imaging 2013, 6, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Myerson, S.G.; D’Arcy, J.; Christiansen, J.P.; Dobson, L.E.; Mohiaddin, R.; Francis, J.M.; Prendergast, B.; Greenwood, J.P.; Karamitsos, T.D.; Neubauer, S. Determination of Clinical Outcome in Mitral Regurgitation with Cardiovascular Magnetic Resonance Quantification. Circulation 2016, 133, 2287–2296. [Google Scholar] [CrossRef]
- Uretsky, S.; Argulian, E.; Narula, J.; Wolff, S.D. Use of Cardiac Magnetic Resonance Imaging in Assessing Mitral Regurgitation: Current Evidence. J. Am. Coll. Cardiol. 2018, 71, 547–563. [Google Scholar] [CrossRef]
- Gorodisky, L.; Agmon, Y.; Porat, M.; Abadi, S.; Lessick, J. Assessment of mitral regurgitation by 3-dimensional proximal flow convergence using magnetic resonance imaging: Comparison with echo-Doppler. Int. J. Cardiovasc. Imaging 2018, 34, 793–802. [Google Scholar] [CrossRef]
- Altes, A.; Levy, F.; Iacuzio, L.; Dumortier, H.; Toledano, M.; Tartar, J.; Tribouilloy, C.; Maréchaux, S. Comparison of Mitral Regurgitant Volume Assessment between Proximal Flow Convergence and Volumetric Methods in Patients with Significant Primary Mitral Regurgitation: An Echocardiographic and Cardiac Magnetic Resonance Imaging Study. J. Am. Soc. Echocardiogr. 2022, 35, 671–681. [Google Scholar] [CrossRef]
- Hutchins, G.M.; Moore, G.W.; Skoog, D.K. The Association of Floppy Mitral Valve with Disjunction of the Mitral Annulus Fibrosus. New Engl. J. Med. 1986, 314, 535–540. [Google Scholar] [CrossRef]
- Pavon, A.; Monney, P.; Schwitter, J. Mitral Valve Prolapse, Arrhythmias, and Sudden Cardiac Death: The Role of Multimodality Imaging to Detect High-Risk Features. Diagnostics 2021, 11, 683. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Peters, D.C.; Salton, C.J.; Bzymek, D.; Nezafat, R.; Goddu, B.; Kissinger, K.V.; Zimetbaum, P.J.; Manning, W.J.; Yeon, S.B. Cardiovascular Magnetic Resonance Characterization of Mitral Valve Prolapse. JACC Cardiovasc. Imaging 2008, 1, 294–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantegazza, V.; Volpato, V.; Gripari, P.; Ali, S.G.; Fusini, L.; Italiano, G.; Muratori, M.; Pontone, G.; Tamborini, G.; Pepi, M. Multimodality imaging assessment of mitral annular disjunction in mitral valve prolapse. Heart 2020, 107, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.P.; Basso, C.; De Lazzari, M.; Rizzo, S.; Cipriani, A.; Giorgi, B.; Lacognata, C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Morphofunctional Abnormalities of Mitral Annulus and Arrhythmic Mitral Valve Prolapse. Circ. Cardiovasc. Imaging 2016, 9, e005030. [Google Scholar] [CrossRef] [Green Version]
- Sriram, C.S.; Syed, F.F.; Ferguson, M.E.; Johnson, J.N.; Enriquez-Sarano, M.; Cetta, F.; Cannon, B.C.; Asirvatham, S.J.; Ackerman, M.J. Malignant Bileaflet Mitral Valve Prolapse Syndrome in Patients With Otherwise Idiopathic Out-of-Hospital Cardiac Arrest. J. Am. Coll. Cardiol. 2013, 62, 222–230. [Google Scholar] [CrossRef] [Green Version]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Yang, L.-T.; Maalouf, J.; Asirvatham, S.; Michelena, H.; Enriquez-Sarano, M. Presentation and Outcome of Arrhythmic Mitral Valve Prolapse. J. Am. Coll. Cardiol. 2020, 76, 637–649. [Google Scholar] [CrossRef]
- Toh, H.; Mori, S.; Izawa, Y.; Fujita, H.; Miwa, K.; Suzuki, M.; Takahashi, Y.; Toba, T.; Watanabe, Y.; Kono, A.K.; et al. Prevalence and extent of mitral annular disjunction in structurally normal hearts: Comprehensive 3D analysis using cardiac computed tomography. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 614–622. [Google Scholar] [CrossRef]
- Zugwitz, D.; Fung, K.; Aung, N.; Rauseo, E.; McCracken, C.; Cooper, J.; El Messaoudi, S.; Anderson, R.H.; Piechnik, S.K.; Neubauer, S.; et al. Mitral Annular Disjunction Assessed Using CMR Imaging: Insights From the UK Biobank Population Study. JACC Cardiovasc. Imaging 2022, 15, 1856–1866. [Google Scholar] [CrossRef]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Schlossbauer, S.A.; Pavon, A.G.; Ho, S.Y.; Maisano, F. Morphology of Mitral Annular Disjunction in Mitral Valve Prolapse. J. Am. Soc. Echocardiogr. 2021, 35, 176–186. [Google Scholar] [CrossRef]
- Basso, C.; Marra, M.P.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic Mitral Valve Prolapse and Sudden Cardiac Death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef] [Green Version]
- Pavon, A.G.; Arangalage, D.; Pascale, P.; Hugelshofer, S.; Rutz, T.; Porretta, A.P.; Le Bloa, M.; Muller, O.; Pruvot, E.; Schwitter, J.; et al. Myocardial extracellular volume by T1 mapping: A new marker of arrhythmia in mitral valve prolapse. J. Cardiovasc. Magn. Reson. 2021, 23, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Figliozzi, S.; Georgiopoulos, G.; Lopes, P.M.; Bauer, K.B.; Moura-Ferreira, S.; Tondi, L.; Mushtaq, S.; Censi, S.; Pavon, A.G.; Bassi, I.; et al. Myocardial Fibrosis at Cardiac MRI Helps Predict Adverse Clinical Outcome in Patients with Mitral Valve Prolapse. Radiology 2022, 220454. [Google Scholar] [CrossRef] [PubMed]
- Beaufils, A.-L.C.D.; Huttin, O.; Jobbe-Duval, A.; Senage, T.; Filippetti, L.; Piriou, N.; Cueff, C.; Venner, C.; Mandry, D.; Sellal, J.-M.; et al. Replacement Myocardial Fibrosis in Patients With Mitral Valve Prolapse: Relation to Mitral Regurgitation, Ventricular Remodeling, and Arrhythmia. Circulation 2021, 143, 1763–1774. [Google Scholar] [CrossRef]
- Guglielmo, M.; Fusini, L.; Muscogiuri, G.; Baessato, F.; Loffreno, A.; Cavaliere, A.; Rizzon, G.; Baggiano, A.; Rabbat, M.G.; Muratori, M.; et al. T1 mapping and cardiac magnetic resonance feature tracking in mitral valve prolapse. Eur. Radiol. 2020, 31, 1100–1109. [Google Scholar] [CrossRef]
- Bui, A.H.; Roujol, S.; Foppa, M.; Kissinger, K.V.; Goddu, B.; Hauser, T.H.; Zimetbaum, P.J.; Ngo, L.H.; Manning, W.J.; Nezafat, R.; et al. Diffuse myocardial fibrosis in patients with mitral valve prolapse and ventricular arrhythmia. Heart 2016, 103, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, D.H.; Kusunose, K.; Obuchowski, N.A.; Cavalcante, J.L.; Popovic, Z.B.; Thomas, J.D.; Desai, M.Y.; Flamm, S.D.; Griffin, B.P. Predictors and Prognostic Impact of Progressive Ischemic Mitral Regurgitation in Patients with Advanced Ischemic Cardiomyopathy: A Multimodality Study. Circ. Cardiovasc. Imaging 2016, 9, e004577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, M.; Curtin, R.; Nowicki, E.R.; Rajeswaran, J.; Flamm, S.D.; Blackstone, E.H.; Mihaljevic, T. Regional wall motion abnormalities and scarring in severe functional ischemic mitral regurgitation: A pilot cardiovascular magnetic resonance imaging study. J. Thorac. Cardiovasc. Surg. 2009, 137, 1063–1070.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spieker, M.; Marpert, J.; Afzal, S.; Scheiber, D.; Bönner, F.; Horn, P.; Kelm, M.; Westenfeld, R. Extent and determinants of left ventricular reverse remodeling in patients with secondary mitral regurgitation undergoing MitraClip implantation. IJC Heart Vasc. 2021, 34, 100804. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-Craig, C.; Strugnell, W.; Gaikwad, N.; Ischenko, M.; Speranza, V.; Chan, J.; Neill, J.; Platts, D.; Scalia, G.M.; Burstow, D.; et al. Quantitation of mitral regurgitation after percutaneous MitraClip repair: Comparison of Doppler echocardiography and cardiac magnetic resonance imaging. Ann. Cardiothorac. Surg. 2015, 4, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.; Crandon, S.; Swoboda, P.P.; Fent, G.J.; Foley, J.R.J.; Chew, P.G.; Brown, L.A.E.; Vijayan, S.; Hassell, M.E.C.J.; Nijveldt, R.; et al. Left ventricular blood flow kinetic energy after myocardial infarction—Insights from 4D flow cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2018, 20, 61. [Google Scholar] [CrossRef] [Green Version]
- van der Geest, R.J.; Garg, P. Advanced Analysis Techniques for Intra-cardiac Flow Evaluation from 4D Flow MRI. Curr. Radiol. Rep. 2016, 4, 38. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavon, A.G.; Guglielmo, M.; Mennilli, P.M.; Falcão, M.B.L.; Bergamaschi, L.; Costantin, D.F.; Vivaldo, M.; Leo, L.A.; Schlossbauer, S.; Roy, C.W.; et al. The Role of Cardiovascular Magnetic Resonance in Patients with Mitral Regurgitation. J. Cardiovasc. Dev. Dis. 2022, 9, 399. https://doi.org/10.3390/jcdd9110399
Pavon AG, Guglielmo M, Mennilli PM, Falcão MBL, Bergamaschi L, Costantin DF, Vivaldo M, Leo LA, Schlossbauer S, Roy CW, et al. The Role of Cardiovascular Magnetic Resonance in Patients with Mitral Regurgitation. Journal of Cardiovascular Development and Disease. 2022; 9(11):399. https://doi.org/10.3390/jcdd9110399
Chicago/Turabian StylePavon, Anna Giulia, Marco Guglielmo, Pierpaolo Mattia Mennilli, Mariana B. L. Falcão, Luca Bergamaschi, David Filip Costantin, Michele Vivaldo, Laura Anna Leo, Susanne Schlossbauer, Christopher W. Roy, and et al. 2022. "The Role of Cardiovascular Magnetic Resonance in Patients with Mitral Regurgitation" Journal of Cardiovascular Development and Disease 9, no. 11: 399. https://doi.org/10.3390/jcdd9110399