
Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
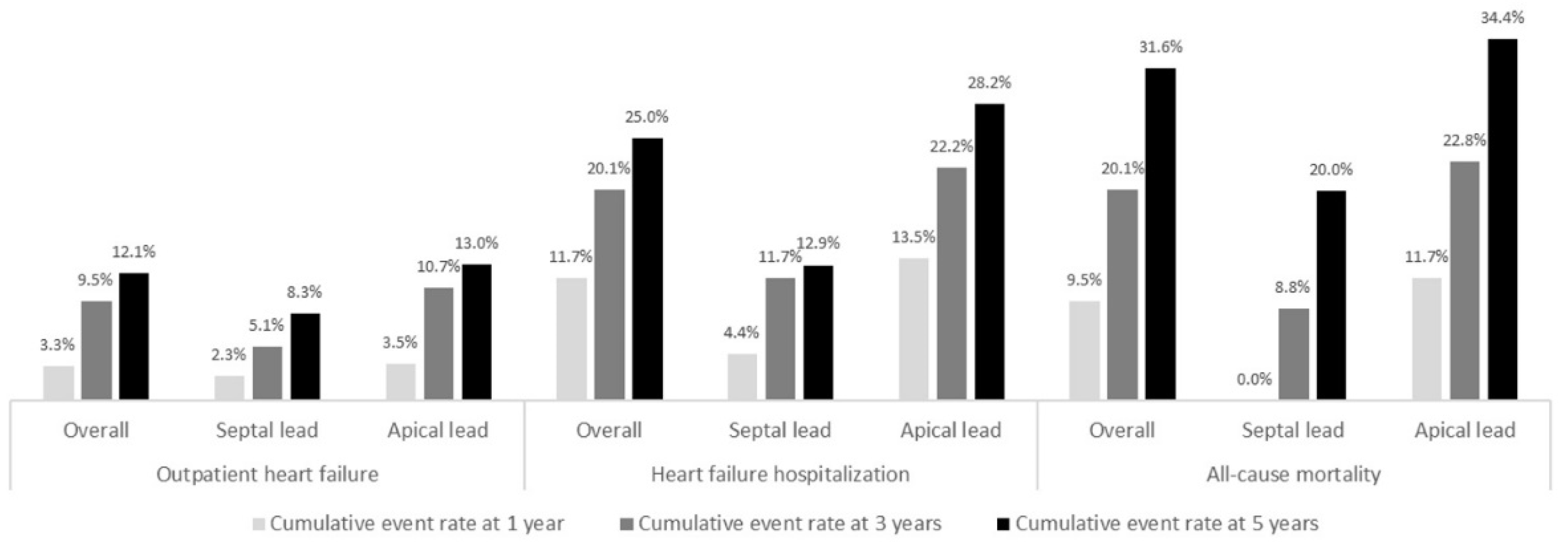
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mond, H.G.; Proclemer, A. The 11th World Survey of Cardiac Pacing and Implantable Cardioverter-Defibrillators: Calendar Year 2009—A World Society of Arrhythmia’s Project. Pacing Clin. Electrophysiol. 2011, 34, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Tayal, B.; Fruelund, P.; Sogaard, P.; Riahi, S.; Polcwiartek, C.; Atwater, B.D.; Gislason, G.; Risum, N.; Torp-Pedersen, C.; Kober, L.; et al. Incidence of heart failure after pacemaker implantation: A nationwide Danish Registry-based follow-up study. Eur. Heart J. 2019, 40, 3641–3648. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, S.; Epstein, A.E.; Verdino, R.J.; Lin, D.; Goldberg, L.R.; Marchlinski, F.E.; Frankel, D.S. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm 2014, 11, 1619–1625. [Google Scholar] [CrossRef]
- Kiehl, E.L.; Makki, T.; Kumar, R.; Gumber, D.; Kwon, D.H.; Rickard, J.W.; Kanj, M.; Wazni, O.M.; Saliba, W.I.; Varma, N.; et al. Incidence and predictors of right ventricular pac-ing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm 2016, 13, 2272–2278. [Google Scholar] [CrossRef] [Green Version]
- Vijayaraman, P.; Bordachar, P.; Ellenbogen, K.A. The Continued Search for Physiological Pacing: Where Are We Now? J. Am. Coll. Cardiol. 2017, 69, 3099–3114. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Li, Q.; Jiang, G.; Zhang, L.; Wang, T.; Zhang, Z. Comparison of effectiveness of right ventricular mid-septal pacing vs. apical pacing: A randomized-controlled trials. Eur. Heart J. Suppl. 2016, 18, F12–F18. [Google Scholar] [CrossRef] [Green Version]
- Saito, M.; Kaye, G.; Negishi, K.; Linker, N.; Gammage, M.; Kosmala, W.; Marwick, T.H. Dyssynchrony, contraction efficiency and regional function with apical and non-apical RV pacing. Heart 2015, 101, 600–608. [Google Scholar] [CrossRef]
- Choudhary, D.; Chaurasia, A.K.; Kumar, S.M.; Arulkumar, A.; Thajudeen, A.; Namboodiri, N.; Sanjay, G.; Abhilash, S.; Ajitkumar, V.; Ja, T. Radial left ventricular dyssynchrony by speckle tracking in apical versus non apical right ventricular pacing- evidence of dyssynchrony on medium term follow up. J. Cardiovasc. Thorac. Res. 2016, 8, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Zou, C.; Song, J.; Li, H.; Huang, X.; Liu, Y.; Zhao, C.; Shi, X.; Yang, X. Right Ventricular Outflow Tract Septal Pacing Is Superior to Right Ventricular Apical Pacing. J. Am. Heart Assoc. 2015, 4, e001777. [Google Scholar] [CrossRef] [Green Version]
- Rimbas, R.C.; Margulescu, A.D.; Siliste, C.; Vinereanu, D. Left ventricular strain analysis reveals better synchrony and diastolic function for septal versus apical right ventricular permanent pacing. Maedica 2014, 9, 232–241. [Google Scholar]
- Kaye, G.C.; Linker, N.J.; Marwick, T.H.; Pollock, L.; Graham, L.; Pouliot, E.; Poloniecki, J.; Gammage, M.; Martin, P.; Pepper, C.; et al. Effect of right ventricular pacing lead site on left ventricular function in patients with high-grade atrioventricular block: Results of the Protect-Pace study. Eur. Heart J. 2015, 36, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Spath, N.B.; Wang, K.; Venkatasumbramanian, S.; Fersia, O.; E Newby, D.; Lang, C.C.; Grubb, N.R.; Dweck, M.R. Complications and prognosis of patients undergoing apical or septal right ventricular pacing. Open Heart 2019, 6, e000962. [Google Scholar] [CrossRef] [Green Version]
- Mizukami, A.; Matsue, Y.; Naruse, Y.; Kowase, S.; Kurosaki, K.; Suzuki, M.; Matsumura, A.; Nogami, A.; Aonuma, K.; Hashimoto, Y. Implications of right ventricular septal pacing for medium-term prognosis: Propensity-matched analysis. Int. J. Cardiol. 2016, 220, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.-A.; Cleland, J.G.F.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and re-synchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Parakh, N.; Gupta, A.; Juneja, R.; Naik, N.; Yadav, R.; Sharma, G.; Roy, A.; Verma, S.K.; Bahl, V.K. Incidence and predictors of pacemaker-induced cardiomyopathy with comparison between apical and non-apical right ventricular pacing sites. J. Interv. Card. Electrophysiol. 2019, 56, 63–70. [Google Scholar] [CrossRef]
- Molina, L.; Sutton, R.; Gandoy, W.; Reyes, N.; Lara, S.; Limón, F.; Gómez, S.; Orihuela, C.; Salame, L.; Moreno, G. Medium-Term Effects of Septal and Apical Pacing in Pacemaker-Dependent Patients: A Double-Blind Prospective Randomized Study. Pacing Clin. Electrophysiol. 2014, 37, 207–214. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Docherty, K.F.; Jhund, P.S.; Anand, I.; Bengtsson, O.; Böhm, M.; De Boer, R.A.; DeMets, D.L.; Desai, A.S.; Drozdz, J.; Howlett, J.; et al. Effect of Dapagliflozin on Outpatient Worsening of Patients with Heart Failure and Reduced Ejection Fraction: A Prespecified Analysis of DAPA-HF. Circulation 2020, 142, 1623–1632. [Google Scholar] [CrossRef]
- Yusu, S.; Mera, H.; Hoshida, K.; Miyakoshi, M.; Miwa, Y.; Tsukada, T.; Yoshino, H.; Ikeda, T. Selective site pacing from the right ventricular mid-septum: Follow-up of lead performance and procedure technique. Int. Heart J. 2012, 53, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamagata, K.; Ishibashi, K.; Wakamiya, A.; Shimamoto, K.; Ueda, N.; Kamakura, T.; Wada, M.; Inoue, Y.; Miyamoto, K.; Noda, T.; et al. Comparison Between Septal Pacing With the Catheter Delivery System and Apical Pacing With the Stylet Delivery System for Ventricular Lead Placement: A Randomized Controlled Trial. Circ. Arrhythmia Electrophysiol. 2021, 14, e010362. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.M.; Lenz, C.J.; Shih, H.H.; Ebrille, E.; Rosenbaum, A.N.; Van Zyl, M.; Aung, H.; Manocha, K.K.; Deshmukh, A.J.; Ms, D.O.H.; et al. Right ventricular pacemaker lead position is associated with differences in long-term outcomes and complications. J. Cardiovasc. Electrophysiol. 2017, 28, 924–930. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | Overall (n = 251) | Septal (n = 47) | Apical (n = 204) | p Value |
|---|---|---|---|---|
| Age (years), mean (SD) | 76.5 (11.3) | 72.2 (11.4) | 77.4 (11.1) | 0.004 |
| Men | 129 (51.4%) | 32 (68.1%) | 97 (47.5%) | 0.008 |
| BMI (Kg/m2), mean (SD) | 28.0 (5.2) | 26.6 (4.3) | 28.4 (5.4) | 0.01 |
| Hypertension | 190 (75.7%) | 31 (66.0%) | 159 (77.9%) | 0.07 |
| Dyslipidemia | 131 (52.2%) | 27 (57.4%) | 104 (51.0%) | 0.26 |
| Diabetes mellitus | 80 (32.0%) | 16 (34.0%) | 64 (31.5%) | 0.43 |
| Insulin-treated | 23 (9.3%) | 2 (4.5%) | 21 (10.3%) | 0.23 |
| Smoker | 53 (21.1%) | 11 (23.4%) | 42 (20.6%) | 0.40 |
| Coronary artery disease | 48 (19.1%) | 14 (29.8%) | 34 (16.7%) | 0.04 |
| Heart failure | 92 (36.7%) | 15 (31.9%) | 77 (37.7%) | 0.28 |
| Atrial fibrillation | 101 (40.2%) | 26 (55.3%) | 75 (36.8%) | 0.02 |
| Peripheral artery disease | 9 (3.6%) | 2 (4.3%) | 7 (3.4%) | 0.78 |
| Chronic kidney disease | 66 (26.3%) | 9 (19.1%) | 57 (27.9%) | 0.15 |
| Hemoglobin (g/dL), mean (SD) | 12.9 (1.8) | 13.5 (1.8) | 12.7 (1.7) | 0.01 |
| Serum creatinine, median (IQR) | 0.98 (0.80–1.34) | 0.90 (0.78–1.22) | 1.00 (0.80–1.40) | 0.14 |
| Medication prior to pacemaker implantation | ||||
| Antiplatelet | 89 (36.0) | 10 (22.7%) | 79 (38.9%) | 0.03 |
| Vitamin K antagonist | 49 (19.8) | 13 (29.5%) | 36 (17.7%) | 0.06 |
| Novel oral anticoagulant | 27 (10.9) | 8 (18.2%) | 19 (9.4%) | 0.09 |
| Beta-blocker | 59 (23.8) | 9 (20.5%) | 50 (24.5%) | 0.36 |
| Ivabradine | 1 (0.4) | 1 (2.3%) | 0 | 0.18 |
| Cardiac glycoside | 7 (2.8%) | 2 (4.5%) | 5 (2.5%) | 0.45 |
| ACE-I/ARB | 142 (57.3%) | 21 (47.7%) | 121 (59.3%) | 0.38 |
| MRA | 10 (4.0%) | 0 | 10 (4.9%) | 0.13 |
| Loop diuretic | 88 (35.5%) | 12 (27.3%) | 76 (37.3%) | 0.14 |
| LVEF (%), mean (SD) | 54.1 (7.5) | 53.7 (7.5) | 54.2 (7.6) | 0.71 |
| LVEF < 50% | 36 (17.0%) | 10 (24.4%) | 26 (15.2%) | 0.12 |
| RV systolic dysfunction | 12 (5.7%) | 2 (5.0%) | 10 (5.8%) | 0.84 |
| Severe LVH | 6 (2.8%) | 0 | 6 (3.5%) | 0.23 |
| Large pericardial effusion | 2 (1.0%) | 0 | 2 (1.2%) | 0.49 |
| Severe AS | 9 (4.3%) | 2 (5.0%) | 7 (4.1%) | 0.80 |
| Significant MS | 2 (0.9%) | 0 | 2 (1.2%) | 0.49 |
| Severe MR | 1 (0.5%) | 0 | 1 (0.6%) | 0.63 |
| Severe TR | 3 (1.4%) | 1 (2.5%) | 2 (1.2%) | 0.52 |
| Pacemaker indication | ||||
| Sinus node disease | 38 (15.1%) | 3 (6.4%) | 35 (17.2%) | 0.04 |
| Atrioventricular block | 174 (69.3%) | 40 (85.1%) | 134 (65.7%) | 0.006 |
| Tachycardia-bradycardia syndrome | 39 (15.5%) | 4 (8.5%) | 35 (17.2%) | 0.10 |
| QRS duration (milliseconds), mean (SD) | 116.0 (25.8) | 112.5 (22.6) | 116.6 (26.4) | 0.36 |
| Dual-chamber pacemaker | 170 (67.7%) | 25 (53.2%) | 145 (71.1%) | 0.02 |
| Radiation time, median (IQR) | 3.2 (1.6–5.5) | 3.3 (2.3–5.5) | 3.1 (1.6–5.5) | 0.53 |
| In-hospital mortality | 7 (2.8%) | 1 (2.1%) | 6 (2.9%) | 0.76 |
| Follow-Up | Overall (n = 244) | Septal (n = 46) | Apical (n = 198) | p Value |
|---|---|---|---|---|
| Follow-up time, median (IQR) | 5.2 (3.0–5.5) | 5.3 (5.1–5.5) | 5.1 (2.6–5.4) | 0.01 |
| QRS duration during RV pacing (milliseconds), mean (SD) | 171.1 (21.1) | 159.0 (13.3) | 173.9 (21.6) | <0.001 |
| Pacemaker complications | ||||
| Pocket infection | 2 (0.8%) | 1 (2.1%) | 1 (0.5%) | 0.26 |
| Pocket hematoma | 2 (0.8%) | 1 (2.1%) | 1 (0.5%) | 0.26 |
| Subclavian vein thrombosis | 1 (0.4%) | 0 | 1 (0.5%) | 0.63 |
| Diaphragm stimulation requiring lead repositioning | 1 (0.4%) | 1 (2.1%) | 0 | 0.19 |
| Pacemaker related endocarditis | 1 (0.4%) | 1 (2.1%) | 0 | 0.19 |
| Heart failure | 89 (37.1%) | 11 (23.9%) | 78 (40.2%) | 0.03 |
| Outpatient | 29 (12.1%) | 4 (8.7%) | 25 (12.9%) | 0.31 |
| Hospitalization | 60 (25.0%) | 7 (15.2%) | 53 (27.3%) | 0.06 |
| Time-to-heart failure, median (IQR) | 1.5 (0.6–3.3) | 2.9 (0.9–4.5) | 1.5 (0.6–3.2) | 0.16 |
| All-cause mortality | 83 (34.2%) | 9 (19.6%) | 74 (37.6%) | 0.01 |
| Time-to-death, median (IQR) | 2.6 (0.9–4.2) | 3.1 (2.0–4.4) | 2.3 (0.8–4.3) | 0.31 |
| RV pacing percentage | 84 (16–99) | 85 (18–98) | 84 (16–99) | 0.99 |
| RV pacing percentage ≥ 40% | 139 (66.5%) | 29 (70.7%) | 110 (65.5%) | 0.33 |
| LVEF (%), mean (SD) | 50.9 (9.9) | 50.1 (9.2) | 51.2 (10.2) | 0.56 |
| LVEF < 50% | 48 (35.6%) | 15 (45.5%) | 33 (32.4%) | 0.12 |
| Upgrade to CRT | 6 (2.5%) | 3 (6.5%) | 3 (1.5%) | 0.05 |
| Medication during follow-up | ||||
| Antiplatelet | 76 (32.3%) | 11 (25.0%) | 65 (34.0%) | 0.17 |
| Vitamin K antagonist | 41 (17.4%) | 13 (29.5%) | 28 (14.7%) | 0.02 |
| Novel oral anticoagulant | 55 (23.4%) | 14 (31.8%) | 41 (21.5%) | 0.11 |
| Beta-blocker | 96 (40.9%) | 19 (43.2%) | 77 (40.3%) | 0.43 |
| Ivabradine | 4 (1.7%) | 2 (4.5%) | 2 (1.0%) | 0.11 |
| Cardiac glycoside | 18 (7.7%) | 3 (6.8%) | 15 (7.9%) | 0.82 |
| ACE-I/ARB | 113 (48.3%) | 25 (56.8%) | 88 (46.3%) | 0.14 |
| ARNI | 5 (2.1%) | 2 (4.5%) | 3 (1.6%) | 0.22 |
| MRA | 17 (7.2%) | 4 (9.1%) | 13 (6.8%) | 0.60 |
| Loop diuretic | 120 (51.0%) | 19 (43.2%) | 101 (52.9%) | 0.16 |
| SGLT2 inhibitor | 10 (4.3%) | 4 (9.1%) | 6 (3.1%) | 0.08 |
| GLP-1 receptor agonist | 2 (0.9%) | 1 (2.3%) | 1 (0.5%) | 0.26 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR 95% CI | p Value | HR 95% CI | p Value | |
| Age (years) | 1.04 (1.01–1.06) | 0.002 | 1.01 (0.99–1.04) | 0.46 |
| Men | 1.25 (0.82–1.89) | 0.30 | 1.59 (0.95–2.65) | 0.08 |
| Hypertension | 1.53 (0.89–2.63) | 0.12 | - | - |
| Dyslipidemia | 1.65 (1.07–2.55) | 0.02 | - | - |
| Diabetes mellitus | 1.57 (1.03–2.40) | 0.04 | - | - |
| Smoker | 1.62 (1.03–2.56) | 0.04 | - | - |
| Coronary artery disease | 1.97 (1.23–3.15) | 0.005 | 1.66 (0.95–2.91) | 0.08 |
| Heart failure | 3.84 (2.50–5.89) | <0.001 | 3.22 (1.88–5.5) | <0.001 |
| Atrial fibrillation | 1.60 (1.05–2.42) | 0.03 | - | - |
| Chronic kidney disease | 1.97 (1.25–3.09) | 0.003 | - | - |
| Hemoglobin (g/dL) | 0.85 (0.76–0.96) | 0.008 | - | - |
| Serum creatinine (mg/dL) | 1.13 (0.97–1.31) | 0.11 | - | - |
| LVEF < 50% | 2.55 (1.55–4.22) | <0.001 | 1.46 (0.76–2.79) | 0.26 |
| RV systolic disfunction | 1.26 (0.46–3.46) | 0.65 | - | - |
| Severe AS | 6.20 (2.66–14.42) | <0.001 | 10.88 (3.25–36.44) | <0.001 |
| Significant MS | 1.71 (0.24–12.35) | 0.60 | - | - |
| Severe MR | 4.35 (0.60–31.64) | 0.15 | - | - |
| Severe TR | 1.68 (0.41–6.86) | 0.47 | - | - |
| RVA pacing | 2.08 (1.11–4.00) | 0.02 | 3.32 (1.48–7.46) | 0.004 |
| RV pacing percentage | 1.00 (0.99–1.01) | 0.90 | 1.00 (0.99–1.01) | 0.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias-Frias, A.; Costa, R.; Campinas, A.; Alexandre, A.; Sá-Couto, D.; Sousa, M.J.; Roque, C.; Vieira, P.; Lagarto, V.; Reis, H.; et al. Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival. J. Cardiovasc. Dev. Dis. 2022, 9, 444. https://doi.org/10.3390/jcdd9120444
Dias-Frias A, Costa R, Campinas A, Alexandre A, Sá-Couto D, Sousa MJ, Roque C, Vieira P, Lagarto V, Reis H, et al. Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival. Journal of Cardiovascular Development and Disease. 2022; 9(12):444. https://doi.org/10.3390/jcdd9120444
Chicago/Turabian StyleDias-Frias, André, Ricardo Costa, Andreia Campinas, André Alexandre, David Sá-Couto, Maria João Sousa, Carla Roque, Pinheiro Vieira, Vitor Lagarto, Hipólito Reis, and et al. 2022. "Right Ventricular Septal Versus Apical Pacing: Long-Term Incidence of Heart Failure and Survival" Journal of Cardiovascular Development and Disease 9, no. 12: 444. https://doi.org/10.3390/jcdd9120444