
Electroporation Parameters for Human Cardiomyocyte Ablation In Vitro

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Immunocytochemistry and Staining
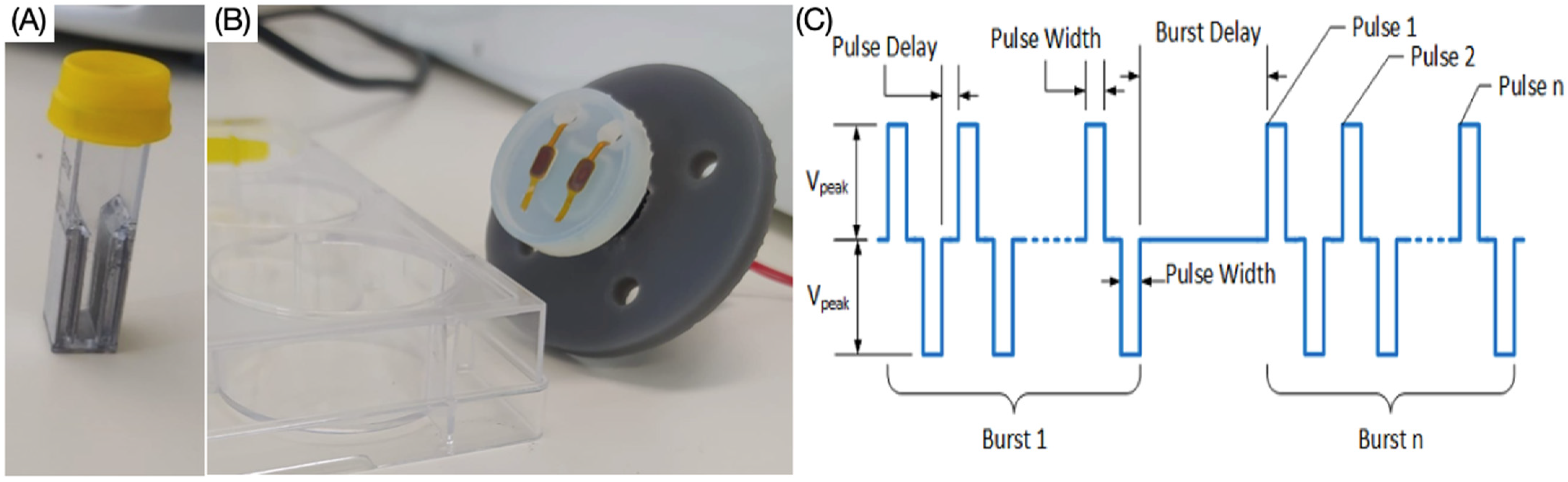
2.3. Electroporation Protocols
2.4. Live-Dead Assay
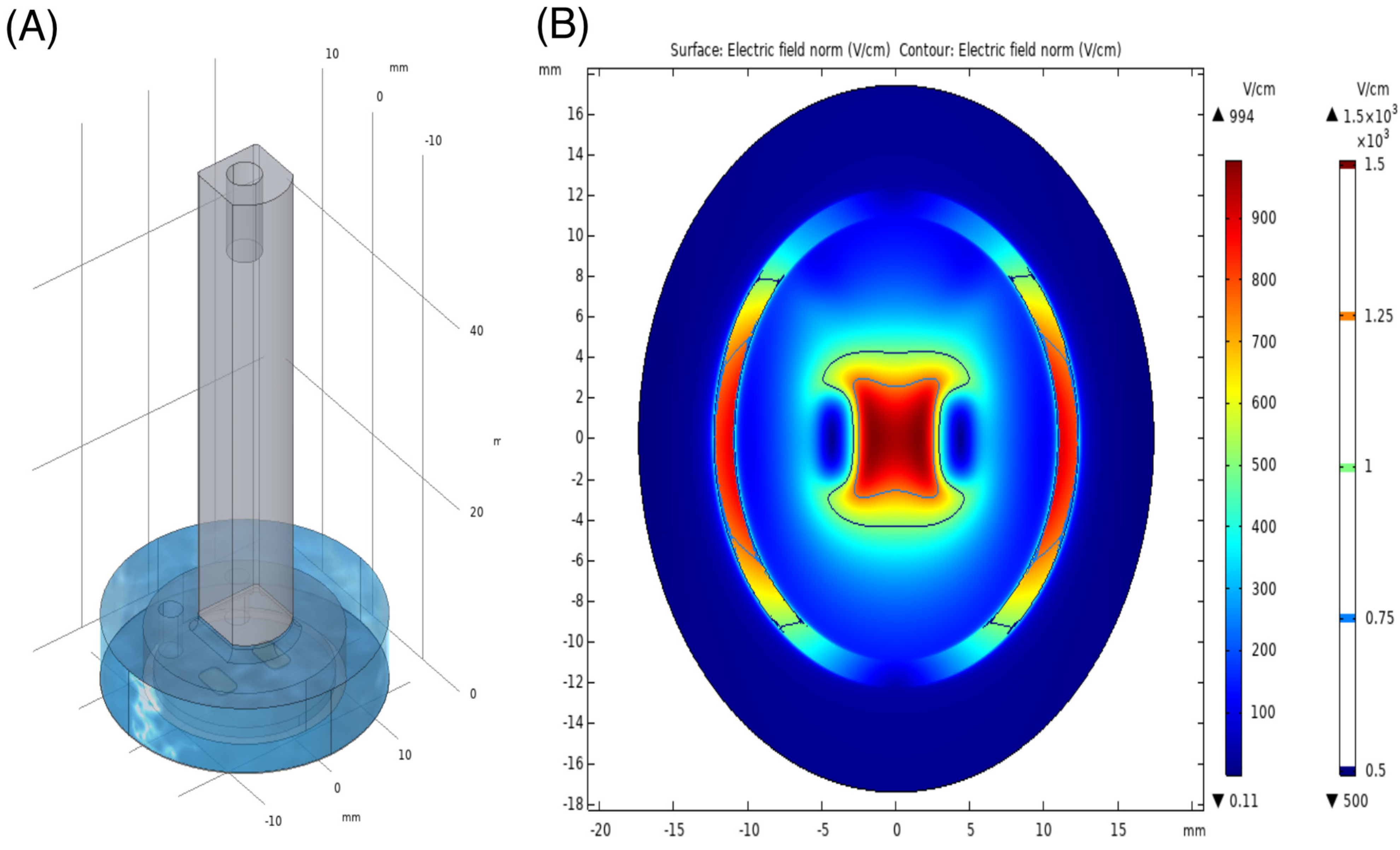
2.5. Numerical Modelling of 2D Ablation Parameters
2.6. Statistical Analysis
3. Results
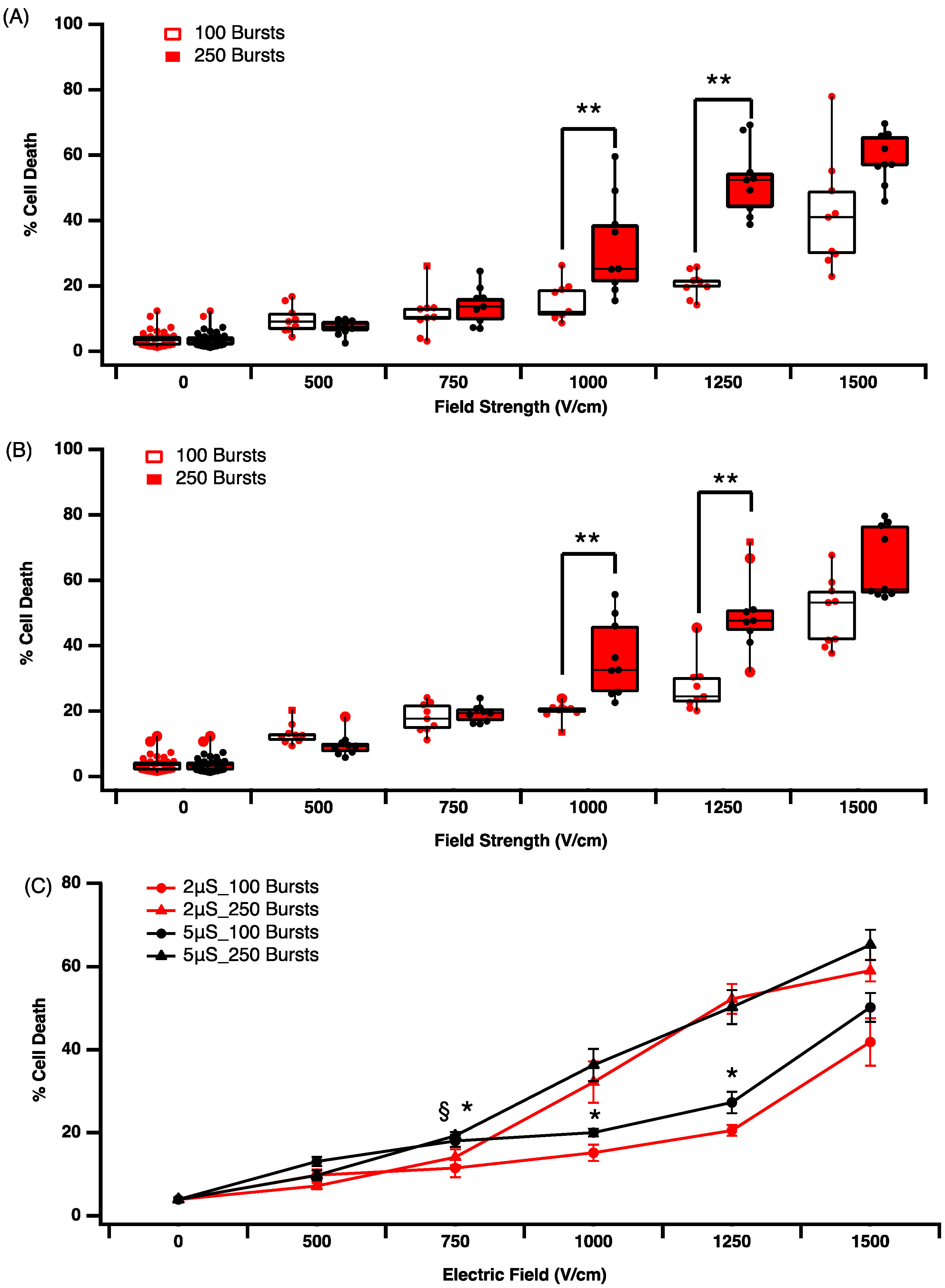
3.1. Effect of Electric Field Parameters on Cell Death in Suspension Culture
3.2. Effect of Time on Cell Death and Lesion Size in a 2D Culture Model
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krijthe, B.P.; Kunst, A.; Benjamin, E.; Lip, G.Y.; Franco, O.; Hofman, A.; Witteman, J.C.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, D.P.; Bernard, M.L.; Madias, C.; Rogers, P.A.; Thihalolipavan, S.; Estes, N.A.M. The State of the Art. Mayo Clin. Proc. 2016, 91, 1778–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gawałko, M.; Kapłon-Cieślicka, A.; Hohl, M.; Dobrev, D.; Linz, D. COVID-19 associated atrial fibrillation: Incidence, putative mechanisms and potential clinical implications. IJC Heart Amp. Vasc. 2020, 30, 100631. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar]
- Morillo, C.A.; Banerjee, A.; Perel, P.; Wood, D. Atrial fibrillation: The current epidemic. J. Geriatr. 2017, 14, 195–203. [Google Scholar]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Avazzadeh, S.; McBride, S.; O’Brien, B.; Coffey, K.; Elahi, A.; O’Halloran, M.; Soo, A.; Quinlan, L.R. Ganglionated plexi ablation for the treatment of atrial fibrillation. J. Clin. Med. 2020, 9, 3081. [Google Scholar] [CrossRef]
- Wu, T.J.; Liang, K.W.; Ting, C.T. Relation Between the Rapid Focal Activation in the Pulmonary Vein and the Maintenance of Paroxysmal Atrial Fibrillation. Pacing Clin. Electrophysiol. 2001, 24, 902–905. [Google Scholar] [CrossRef]
- Sanders, P.; Morton, J.B.; Davidson, N.C.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrical Remodeling of the Atria in Congestive Heart Failure. Circulation 2003, 108, 1461–1468. [Google Scholar] [CrossRef] [Green Version]
- Mahida, S.; Sacher, F.; Derval, N.; Berte, B.; Yamashita, S.; Hooks, D.; Denis, A.; Amraoui, S.; Hocini, M.; Haissaguerre, M.; et al. Science Linking Pulmonary Veins and Atrial Fibrillation. Arrhythm. Amp. Electrophysiol. Rev. 2015, 4, 40. [Google Scholar] [CrossRef] [Green Version]
- Grimaldi, M.; Di Monaco, A.; Gomez, T.; Berman, D.; Datta, K.; Sharma, T.; Govari, A.; Altman, A.; Di Biase, L. Time Course of Irreversible Electroporation Lesion Development Through Short- and Long-Term Follow-Up in Pulsed-Field Ablation–Treated Hearts. Circ. Arrhythm. Electrophysiol. 2022, 15, e010661. [Google Scholar] [CrossRef] [PubMed]
- Maan, A.; Koruth, J. Pulsed Field Ablation: A New Paradigm for Catheter Ablation of Arrhythm. Curr. Cardiol. Rep. 2022, 24, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Yamane, T. Catheter ablation of atrial fibrillation: Current status and near future. J. Cardiol. 2022, 80, 22–27. [Google Scholar] [CrossRef]
- van Es, R.; Konings, M.K.; Du Pré, B.C.; Neven, K.; van Wessel, H.; van Driel, V.J.H.M.; Westra, A.H.; Doevendans, P.A.F.; Wittkampf, F.H.M. High-frequency irreversible electroporation for cardiac ablation using an asymmetrical waveform. Biomed. Eng. Online 2019, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittkampf, F.H.M.; van Es, R.; Neven, K. Electroporation and its Relevance for Cardiac Catheter Ablation. JACC Clin. Electrophysiol. 2018, 4, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Lavee, J.; Onik, G.; Mikus, P.; Rubinsky, B. A Novel Nonthermal Energy Source for Surgical Epicardial Atrial Ablation: Irreversible Electroporation. Heart Surg. Forum 2007, 10, 96. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Neuzil, P.; Koruth, J.S.; Petru, J.; Funosako, M.; Cochet, H.; Sediva, L.; Chovanec, M.; Dukkipati, S.R.; Jais, P. Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation. J. Am. Coll Cardiol. 2019, 74, 315–326. [Google Scholar] [CrossRef] [PubMed]
- du Pré, B.C.; van Driel, V.J.; van Wessel, H.; Loh, P.; Doevendans, P.A.; Goldschmeding, R.; Wittkampf, F.H.; Vink, A. Minimal coronary artery damage by myocardial electroporation ablation. EP Eur. 2013, 15, 144–149. [Google Scholar] [CrossRef]
- Tan, N.Y.; Ladas, T.P.; Christopoulos, G.; Sugrue, A.M.; van Zyl, M.; Ladejobi, A.O.; Lodhi, F.K.; Hu, T.Y.; Ezzeddine, F.M.; Agboola, K.; et al. Ventricular nanosecond pulsed electric field delivery using active fixation leads: A proof-of-concept preclinical study. J. Interv. Card. Electrophysiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Varghese, F.; Philpott, J.M.; Neuber, J.U.; Hargrave, B.; Zemlin, C.W. Surgical Ablation of Cardiac Tissue with Nanosecond Pulsed Electric Fields in Swine. Cardiovasc. Eng. Technol. 2022. [Google Scholar] [CrossRef]
- Avazzadeh, S.; O’Brien, B.; Coffey, K.; O’Halloran, M.; Keane, D.; Quinlan, L.R. Establishing Irreversible Electroporation Electric Field Potential Threshold in A Suspension In Vitro Model for Cardiac and Neuronal Cells. J. Clin. Med. 2021, 10, 5443. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.W.; Kostecki, G.; Fish, J.M.; Jensen, J.A.; Tandri, H. In Vitro Cell Selectivity of Reversible and Irreversible: Electroporation in Cardiac Tissue. Circ. Arrhythm. Electrophysiol. 2021, 14, e008817. [Google Scholar] [CrossRef]
- Vu, T.D.; Kofidis, T. Biomaterials and cells for cardiac tissue engineering. In Cardiac Regeneration and Repair; Woodhead Publishing: Sawston, UK, 2014; Volume 1, pp. 127–179. [Google Scholar]
- Prieto, J.L.; Su, H.-W.; Hou, H.W.; Pinilla-Vera, M.; Levy, B.D.; Baron, R.M.; Han, J.; Voldman, J. Monitoring sepsis using electrical cell profiling. Lab. Chip. 2016, 16, 4333–4340. [Google Scholar] [CrossRef] [Green Version]
- Wasson, E.M.; Alinezhadbalalami, N.; Brock, R.M.; Allen, I.C.; Verbridge, S.S.; Davalos, R.V. Understanding the role of calcium-mediated cell death in high-frequency irreversible electroporation. Bioelectrochemistry 2020, 131, 107369. [Google Scholar] [CrossRef] [PubMed]
- McBride, S.; Avazzadeh, S.; Wheatley, A.; O’Brien, B.; Coffey, K.; Elahi, A.; O’Halloran, M.; Quinlan, L. Ablation Modalities for Therapeutic Intervention in Arrhythmia-Related Cardiovascular Disease: Focus on Electroporation. J. Clin. Med. 2021, 10, 2657. [Google Scholar] [CrossRef]
- Weaver, J. Electroporation of cells and tissues. Trans. Plasma Sci. 2000, 28, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Kaminska, I.; Kotulska, M.; Stecka, A.; Saczko, J. Electroporation-induced changes in normal immature rat myoblasts (H9C2). Gen. Physiol. Biophys. 2012, 31, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Sugrue, A.; Maor, E.; Ivorra, A.; Vaidya, V.; Witt, C.; Kapa, S.; Asirvatham, S. Irreversible electroporation for the treatment of cardiac arrhythmias. Expert Rev. Cardiovasc. Ther. 2018, 16, 349–360. [Google Scholar] [CrossRef]
- Mercadal, B.; Beitel-White, N.; Aycock, K.N.; Castellví, Q.; Davalos, R.V.; Ivorra, A. Dynamics of Cell Death After Conventional IRE and H-FIRE Treatments. Ann. Biomed. Eng. 2020, 48, 1451–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, F.; Varghese, F.; Pakhomov, A.G.; Semenov, I.; Xiao, S.; Philpott, J.; Zemlin, C. Ablation of Myocardial Tissue With Nanosecond Pulsed Electric Fields. PLoS ONE 2015, 10, e0144833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, Q.; Xiong, Z.-A.; Liu, Y.; Yao, C.-G.; Zhou, W.; Hua, Y.-Y.; Wang, Z.-L. Effects of irreversible electroporation on cervical cancer cell lines in vitro. Mol. Med. Rep. 2016, 14, 2187–2193. [Google Scholar] [CrossRef] [Green Version]
- Vogel, J.A.; van Veldhuisen, E.; Agnass, P.; Crezee, J.; Dijk, F.; Verheij, J.; van Gulik, T.M.; Meijerink, M.R.; Vroomen, L.G.; van Lienden, K.P.; et al. Time-Dependent Impact of Irreversible Electroporation on Pancreas, Liver, Blood Vessels and Nerves: A Systematic Review of Experimental Studies. PLoS ONE 2017, 10, e0174018. [Google Scholar]
- Beebe, S.J. Regulated and apoptotic cell death after nanosecond electroporation. In Handbook of Electroporation; Miklavčič, D., Ed.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Yatim, N.; Cullen, S.; Albert, M.L. Dying cells actively regulate adaptive immune responses. Nat. Rev. Immunol. 2017, 17, 262–275. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ablation Protocol | Pulse Width (μs) | Pulse Number | Burst Number | On-Time (ms) |
|---|---|---|---|---|
| 1 | 100 | 5 | 10 | 3 |
| 2 | 100 | 5 | 60 | 60 |
| 3 | 2 | 60 | 100 | 24 |
| 4 | 2 | 60 | 250 | 60 |
| 5 | 5 | 60 | 100 | 30 |
| 6 | 5 | 60 | 250 | 75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baena-Montes, J.M.; O’Halloran, T.; Clarke, C.; Donaghey, K.; Dunne, E.; O’Halloran, M.; Quinlan, L.R. Electroporation Parameters for Human Cardiomyocyte Ablation In Vitro. J. Cardiovasc. Dev. Dis. 2022, 9, 240. https://doi.org/10.3390/jcdd9080240
Baena-Montes JM, O’Halloran T, Clarke C, Donaghey K, Dunne E, O’Halloran M, Quinlan LR. Electroporation Parameters for Human Cardiomyocyte Ablation In Vitro. Journal of Cardiovascular Development and Disease. 2022; 9(8):240. https://doi.org/10.3390/jcdd9080240
Chicago/Turabian StyleBaena-Montes, Jara M., Tony O’Halloran, Cormac Clarke, Kevin Donaghey, Eoghan Dunne, Martin O’Halloran, and Leo R. Quinlan. 2022. "Electroporation Parameters for Human Cardiomyocyte Ablation In Vitro" Journal of Cardiovascular Development and Disease 9, no. 8: 240. https://doi.org/10.3390/jcdd9080240