
Prevalence and Species Distribution of Candida Clinical Isolates in a Tertiary Care Hospital in Ecuador Tested from January 2019 to February 2020
 , , and
, , and 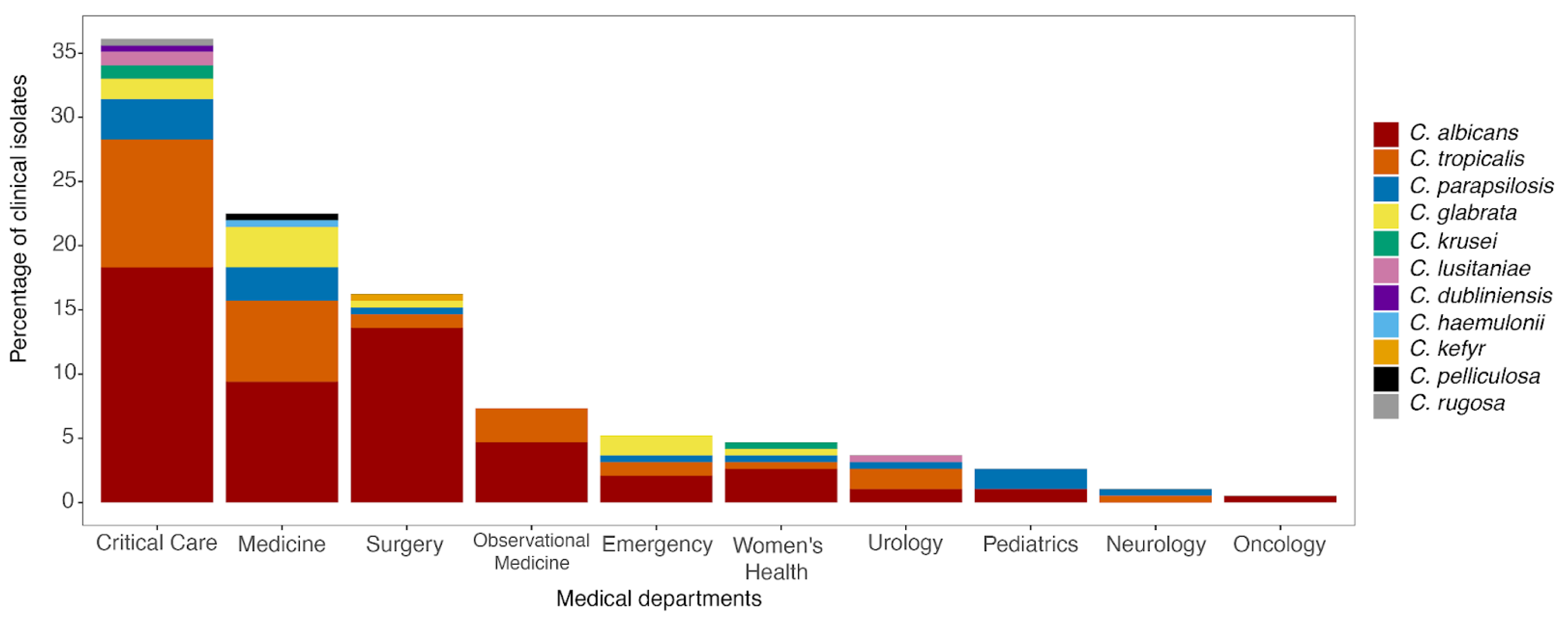{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples and Yeast Isolation Culture
2.2. DNA Extraction
2.3. Molecular Characterization of Candida Clinical Isolates by ITS Regions
3. Results
3.1. Origin of Candida Strains
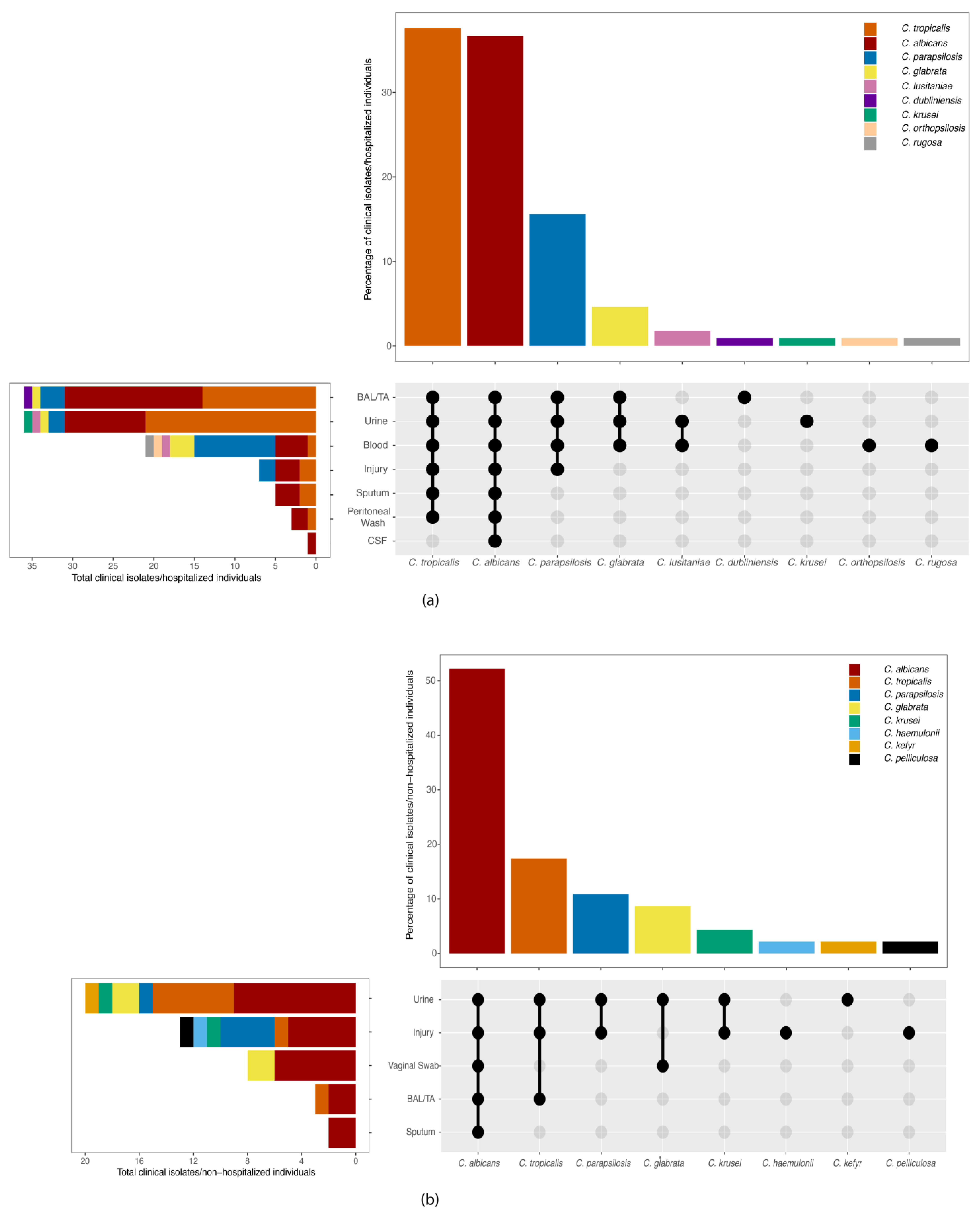
3.2. Molecular Characterization of Candida Strains and Source Distribution
3.3. Comparison of VITEK 2 System and ITS Sequencing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, G.D.; Denning, D.W.; Gow, N.A.R.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden Killers: Human Fungal Infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A. Therapeutic Options for the Management of Oropharyngeal and Esophageal Candidiasis in HIV/AIDS Patients. HIV Clin. Trials 2000, 1, 47–59. [Google Scholar] [CrossRef]
- Sandven, P.; Bevanger, L.; Digranes, A.; Haukland, H.H.; Mannsåker, T.; Gaustad, P.; the Norwegian Yeast Study Group. Candidemia in Norway (1991 to 2003): Results from a Nationwide Study. J. Clin. Microbiol. 2006, 44, 1977–1981. [Google Scholar] [CrossRef] [PubMed]
- Deorukhkar, S.C.; Saini, S.; Mathew, S. Non- Albicans Candida Infection: An Emerging Threat. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A.; Candida auris Incident Management Team; Manuel, R.; Brown, C.S. Candida Auris: A Review of the Literature. Clin. Microbiol. Rev. 2018, 31, e00029-17. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.; Queiroz-Telles, F.; Alvarado-Matute, T.; Tiraboschi, I.N.; Cortes, J.; Zurita, J.; Guzman-Blanco, M.; Santolaya, M.E.; Thompson, L.; Sifuentes-Osornio, J.; et al. Epidemiology of Candidemia in Latin America: A Laboratory-Based Survey. PLoS ONE 2013, 8, e59373. [Google Scholar] [CrossRef]
- Colombo, A.L.; Nucci, M.; Park, B.J.; Nouér, S.A.; Arthington-Skaggs, B.; Da Matta, D.A.; Warnock, D.; Morgan, J. Epidemiology of Candidemia in Brazil: A Nationwide Sentinel Surveillance of Candidemia in Eleven Medical Centers. J. Clin. Microbiol. 2006, 44, 2816–2823. [Google Scholar] [CrossRef]
- Sadeghi, G.; Ebrahimi-Rad, M.; Mousavi, S.F.; Shams-Ghahfarokhi, M.; Razzaghi-Abyaneh, M. Emergence of Non-Candida Albicans Species: Epidemiology, Phylogeny and Fluconazole Susceptibility Profile. J. Mycol. Méd. 2018, 28, 51–58. [Google Scholar] [CrossRef]
- Silva, S.; Negri, M.; Henriques, M.; Oliveira, R.; Williams, D.W.; Azeredo, J. Candida Glabrata, Candida Parapsilosis and Candida Tropicalis: Biology, Epidemiology, Pathogenicity and Antifungal Resistance. FEMS Microbiol. Rev. 2012, 36, 288–305. [Google Scholar] [CrossRef]
- Snydman, D.R. Shifting Patterns in the Epidemiology of Nosocomial Candida Infections*. Chest 2003, 123 (Suppl. S5), 500S–503S. [Google Scholar] [CrossRef]
- Sobel, J.D. The Emergence of Non-Albicans Candida Species as Causes of Invasive Candidiasis and Candidemia. Curr. Infect. Dis. Rep. 2006, 8, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Seyoum, E.; Bitew, A.; Mihret, A. Distribution of Candida Albicans and Non-Albicans Candida Species Isolated in Different Clinical Samples and Their in Vitro Antifungal Susceptibility Profile in Ethiopia. BMC Infect. Dis. 2020, 20, 231. [Google Scholar] [CrossRef] [PubMed]
- Boonsilp, S.; Homkaew, A.; Phumisantiphong, U.; Nutalai, D.; Wongsuk, T. Species Distribution, Antifungal Susceptibility, and Molecular Epidemiology of Candida Species Causing Candidemia in a Tertiary Care Hospital in Bangkok, Thailand. J. Fungi 2021, 7, 577. [Google Scholar] [CrossRef] [PubMed]
- Bedout, C.D.; Tabares, A.M.; Restrepo, Á.; Arango, M.; Zuluaga, Á. Especies de Candida aisladas de lesiones ungueales y su sensibilidad in vitro al fluconazol (1999–2001). Rev. Asoc. Colomb. Dermatol. Cirugía Dermatol. 2003, 11, 325–331. [Google Scholar]
- Yánez Domínguez, D.D. Caracterización Molecular de las Especies de Candida Almacenadas en el Laboratorio de Micología Clínica de la Carrera de Bioquímica Clínica, Facultad de Medicina de la Pontificia Universidad Católica del Ecuador en la Ciudad de Quito Correspondientes al Período de Enero 2000 a Agosto 2007. Bachelor Thesis, PUCE—Quito. 2020. Available online: http://repositorio.puce.edu.ec:80/handle/22000/17478 (accessed on 19 January 2024).
- White, T.J.; Bruns, T.; Lee, S.J.W.T.; Taylor, J. Amplification and direct sequencing of fungal ribosomal RNA genes for phylogenetics. In PCR Protocols: A Guide to Methods and Applications; Academic Press: Cambridge, MA, USA, 1990; pp. 315–322. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis. 2016. Available online: https://ggplot2.tidyverse.org/ (accessed on 25 March 2024).
- Conde-Rosa, A.; Amador, R.; Perez-Torres, D.; Colón, E.; Sánchez-Rivera, C.; Nieves-Plaza, M.; González-Ramos, M.; Bertrán-Pasarell, J. Candidemia Distribution, Associated Risk Factors, and Attributed Mortality at a University-Based Medical Center. P. R. Health Sci. J. 2010, 29, 26–29. [Google Scholar] [PubMed]
- Ortíz Ruiz, G.; Osorio, J.; Valderrama, S.; Álvarez, D.; Elías Díaz, R.; Calderón, J.; Ballesteros, D.; Franco, A. Risk Factors for Candidemia in Non-Neutropenic Critical Patients in Colombia. Med. Intensiv. 2016, 40, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Doi, A.M.; Pignatari, A.C.C.; Edmond, M.B.; Marra, A.R.; Camargo, L.F.A.; Siqueira, R.A.; da Mota, V.P.; Colombo, A.L. Epidemiology and Microbiologic Characterization of Nosocomial Candidemia from a Brazilian National Surveillance Program. PLoS ONE 2016, 11, e0146909. [Google Scholar] [CrossRef] [PubMed]
- Rodero, L.; Davel, G.; Soria, M.; Vivot, W.; Córdoba, S.; Canteros, C.E.; Saporiti, A.; EMIFN. Multicenter study of fungemia due to yeasts in Argentina. Rev. Argent. Microbiol. 2005, 37, 189–195. [Google Scholar] [PubMed]
- Yang, Z.-T.; Wu, L.; Liu, X.-Y.; Zhou, M.; Li, J.; Wu, J.-Y.; Cai, Y.; Mao, E.-Q.; Chen, E.-Z.; Lortholary, O. Epidemiology, Species Distribution and Outcome of Nosocomial Candida Spp.Bloodstream Infection in Shanghai. BMC Infect. Dis. 2014, 14, 241. [Google Scholar] [CrossRef]
- Awad, L.; Tamim, H.; Abdallah, D.; Salameh, M.; Mugharbil, A.; Jisr, T.; Zahran, K.; Droubi, N.; Ibrahim, A.; Moghnieh, R. Correlation between Antifungal Consumption and the Distribution of Candida Species in Different Hospital Departments of a Lebanese Medical Centre. BMC Infect. Dis. 2018, 18, 589. [Google Scholar] [CrossRef]
- Caggiano, G.; Coretti, C.; Bartolomeo, N.; Lovero, G.; De Giglio, O.; Montagna, M.T. Candida Bloodstream Infections in Italy: Changing Epidemiology during 16 Years of Surveillance. BioMed Res. Int. 2015, 2015, e256580. [Google Scholar] [CrossRef]
- da Costa, V.G.; Quesada, R.M.B.; Abe, A.T.S.; Furlaneto-Maia, L.; Furlaneto, M.C. Nosocomial Bloodstream Candida Infections in a Tertiary-Care Hospital in South Brazil: A 4-Year Survey. Mycopathologia 2014, 178, 243–250. [Google Scholar] [CrossRef]
- Bedout, C.; Gómez, B. Candida and Candidiasis: The Challenge Continues for an Early Diagnosis. Infectio 2010, 14, s159–s171. [Google Scholar] [CrossRef]
- Da Matta, D.A.; Souza, A.C.R.; Colombo, A.L. Revisiting Species Distribution and Antifungal Susceptibility of Candida Bloodstream Isolates from Latin American Medical Centers. J. Fungi 2017, 3, 24. [Google Scholar] [CrossRef]
- Sampaio Camargo, T.Z.; Marra, A.R.; Silva, C.V.; Cardoso, M.F.S.; Martino, M.D.V.; Camargo, L.F.A.; Correa, L. Secular Trends of Candidemia in a Tertiary Care Hospital. Am. J. Infect. Control 2010, 38, 546–551. [Google Scholar] [CrossRef] [PubMed]
- González, G.M.; Elizondo, M.; Ayala, J. Trends in Species Distribution and Susceptibility of Bloodstream Isolates of Candida Collected in Monterrey, Mexico, to Seven Antifungal Agents: Results of a 3-Year (2004 to 2007) Surveillance Study. J. Clin. Microbiol. 2008, 46, 2902–2905. [Google Scholar] [CrossRef] [PubMed]
- Corzo-Leon, D.E.; Alvarado-Matute, T.; Colombo, A.L.; Cornejo-Juarez, P.; Cortes, J.; Echevarria, J.I.; Guzman-Blanco, M.; Macias, A.E.; Nucci, M.; Ostrosky-Zeichner, L.; et al. Surveillance of Candida Spp Bloodstream Infections: Epidemiological Trends and Risk Factors of Death in Two Mexican Tertiary Care Hospitals. PLoS ONE 2014, 9, e97325. [Google Scholar] [CrossRef]
- Bustamante, B.; Martins, M.A.; Bonfietti, L.X.; Szeszs, M.W.; Jacobs, J.; Garcia, C.; Melhem, M.S.C. Species Distribution and Antifungal Susceptibility Profile of Candida Isolates from Bloodstream Infections in Lima, Peru. J. Med. Microbiol. 2014, 63, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Riera, F.; Medeot, M.; Sartori, L.; Bergallo, C.; Minoli, J.; Vilchez, V.; Sánchez, P.; Abiega, C.; Pincheira, C.; Correa, S.; et al. Candidemia epidemiology in Córdoba Argentina. Surveillance study of five institutions. Rev. Fac. Cien. Med. Univ. Nac. Cordoba 2014, 71, 89–93. [Google Scholar]
- Martí-Carrizosa, M.; Sánchez-Reus, F.; March, F.; Coll, P. Fungemia in a Spanish Hospital: The Role of Candida Parapsilosis over a 15-Year Period. Scand. J. Infect. Dis. 2014, 46, 454–461. [Google Scholar] [CrossRef]
- Girão, E.; Levin, A.S.; Basso, M.; Gobara, S.; Gomes, L.B.; Medeiros, E.A.S.; Costa, S.F. Seven-Year Trend Analysis of Nosocomial Candidemia and Antifungal (Fluconazole and Caspofungin) Use in Intensive Care Units at a Brazilian University Hospital. Med. Mycol. 2008, 46, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Asmundsdottir, L.R.; Erlendsdottir, H.; Gottfredsson, M. Nationwide Study of Candidemia, Antifungal Use, and Antifungal Drug Resistance in Iceland, 2000 to 2011. J. Clin. Microbiol. 2020, 51, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Guinea, J. Global Trends in the Distribution of Candida Species Causing Candidemia. Clin. Microbiol. Infect. 2014, 20, 5–10. [Google Scholar] [CrossRef]
- Nishikaku, A.S.; Melo, A.S.A.; Colombo, A.L. Geographic Trends in Invasive Candidiasis. Curr. Fungal Infect. Rep. 2010, 4, 210–218. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of Invasive Candidiasis: A Persistent Public Health Problem. Clin. Microbiol. Rev. 2007, 20, 133–163. [Google Scholar] [CrossRef]
- Papadimitriou-Olivgeris, M.; Spiliopoulou, A.; Kolonitsiou, F.; Bartzavali, C.; Lambropoulou, A.; Xaplanteri, P.; Anastassiou, E.D.; Marangos, M.; Spiliopoulou, I.; Christofidou, M. Increasing Incidence of Candidaemia and Shifting Epidemiology in Favor of Candida Non-Albicans in a 9-Year Period (2009–2017) in a University Greek Hospital. Infection 2019, 47, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Yapar, N. Epidemiology and Risk Factors for Invasive Candidiasis. TCRM 2014, 10, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Motoa, G.; Muñoz, J.S.; Oñate, J.; Pallares, C.J.; Hernández, C.; Villegas, M.V. Epidemiology of Candida isolates from Intensive Care Units in Colombia from 2010 to 2013. Rev. Iberoam. Micol. 2017, 34, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ami, R.; Olshtain-Pops, K.; Krieger, M.; Oren, I.; Bishara, J.; Dan, M.; Wiener-Well, Y.; Weinberger, M.; Zimhony, O.; Chowers, M.; et al. Antibiotic Exposure as a Risk Factor for Fluconazole-Resistant Candida Bloodstream Infection. Antimicrob. Agents Chemother. 2012, 56, 2518–2523. [Google Scholar] [CrossRef]
- Lortholary, O.; Renaudat, C.; Sitbon, K.; Madec, Y.; Denoeud-Ndam, L.; Wolff, M.; Fontanet, A.; Bretagne, S.; Dromer, F.; French Mycosis Study Group. Worrisome Trends in Incidence and Mortality of Candidemia in Intensive Care Units (Paris Area, 2002–2010). Intensive Care Med. 2014, 40, 1303–1312. [Google Scholar] [CrossRef]
- Colombo, A.L.; Garnica, M.; Aranha Camargo, L.F.; Da Cunha, C.A.; Bandeira, A.C.; Borghi, D.; Campos, T.; Senna, A.L.; Valias Didier, M.E.; Dias, V.C.; et al. Candida Glabrata: An Emerging Pathogen in Brazilian Tertiary Care Hospitals. Med. Mycol. 2013, 51, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Hinrichsen, S.L.; Falcão, E.; Vilella, T.A.S.; Colombo, A.L.; Nucci, M.; Moura, L.; Rêgo, L.; Lira, C.; Almeida, L. Candidemia in a tertiary hospital in northeastern Brazil. Rev. Soc. Bras. Med. Trop. 2008, 41, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Santolaya, M.E.; Thompson, L.; Benadof, D.; Tapia, C.; Legarraga, P.; Cortés, C.; Rabello, M.; Valenzuela, R.; Rojas, P.; Rabagliati, R. A Prospective, Multi-Center Study of Candida Bloodstream Infections in Chile. PLoS ONE 2019, 14, e0212924. [Google Scholar] [CrossRef] [PubMed]
- Tortorano, A.M.; Prigitano, A.; Morroni, G.; Brescini, L.; Barchiesi, F. Candidemia: Evolution of Drug Resistance and Novel Therapeutic Approaches. IDR 2021, 14, 5543–5553. [Google Scholar] [CrossRef] [PubMed]
- Ngouana, T.K.; Toghueo, R.M.K.; Kenfack, I.F.; Lachaud, L.; Nana, A.K.; Tadjou, L.; Kouanfack, C.; Boyom, F.F.; Bertout, S. Epidemiology and Antifungal Susceptibility Testing of Non-Albicans Candida Species Colonizing Mucosae of HIV-Infected Patients in Yaoundé (Cameroon). J. Mycol. Méd. 2019, 29, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Won, E.J.; Choi, M.J.; Kim, M.-N.; Yong, D.; Lee, W.G.; Uh, Y.; Kim, T.S.; Byeon, S.A.; Lee, S.Y.; Kim, S.H.; et al. Fluconazole-Resistant Candida Glabrata Bloodstream Isolates, South Korea, 2008–2018. Emerg. Infect. Dis. 2021, 27, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Maraki, S.; Mavromanolaki, V.E.; Stafylaki, D.; Nioti, E.; Hamilos, G.; Kasimati, A. Epidemiology and Antifungal Susceptibility Patterns of Candida Isolates from Greek Women with Vulvovaginal Candidiasis. Mycoses 2019, 62, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Dunaiski, C.M.; Kock, M.M.; Chan, W.Y.; Ismail, A.; Peters, R.P.H. Molecular Epidemiology and Antimicrobial Resistance of Vaginal Candida Glabrata Isolates in Namibia. Med. Mycol. 2024, 62, myae009. [Google Scholar] [CrossRef] [PubMed]
- Chesdachai, S.; Yetmar, Z.A.; Ranganath, N.; Everson, J.J.; Wengenack, N.L.; Abu Saleh, O.M. Antifungal Susceptibility Pattern of Candida Glabrata from a Referral Center and Reference Laboratory: 2012–2022. J. Fungi 2023, 9, 821. [Google Scholar] [CrossRef]
- De Oliveira, C.S.; Colombo, A.L.; Francisco, E.C.; de Lima, B.; Gandra, R.F.; de Carvalho, M.C.P.; de Carrilho, C.M.D.M.; Petinelli, R.; Pelison, M.; Helbel, C.; et al. Clinical and Epidemiological Aspects of Candidemia in Eight Medical Centers in the State of Parana, Brazil: Parana Candidemia Network. Braz. J. Infect. Dis. 2021, 25, 101041. [Google Scholar] [CrossRef]
- Kaur, H.; Shankarnarayana, S.A.; Hallur, V.; Muralidharan, J.; Biswal, M.; Ghosh, A.K.; Ray, P.; Chakrabarti, A.; Rudramurthy, S.M. Prolonged Outbreak of Candida Krusei Candidemia in Paediatric Ward of Tertiary Care Hospital. Mycopathologia 2020, 185, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Kothalawala, M.; Jayaweera, J.A.A.S.; Arunan, S.; Jayathilake, A. The Emergence of Non-Albicans Candidemia and Evaluation of HiChrome Candida Differential Agar and VITEK2 YST® Platform for Differentiation of Candida Bloodstream Isolates in Teaching Hospital Kandy, Sri Lanka. BMC Microbiol. 2019, 19, 136. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Abbasi, A.F.; Prakash, S.; Mangat, J.; Hosein, Z.; Haider, N.; Chan, J. Candida Auris: An Overview of the Emerging Drug-Resistant Fungal Infection. Infect. Chemother. 2022, 54, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Peterson, S.W.; Kurtzman, C.P. Ribosomal RNA Sequence Divergence Among Sibling Species of Yeasts. Syst. Appl. Microbiol. 1991, 14, 124–129. [Google Scholar] [CrossRef]
- Alonso-Vargas, R.; Elorduy, L.; Eraso, E.; Cano, F.J.; Guarro, J.; Pontón, J.; Quindós, G. Isolation of Candida Africana, Probable Atypical Strains of Candida Albicans, from a Patient with Vaginitis. Med. Mycol. 2008, 46, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Criseo, G.; Scordino, F.; Romeo, O. Current Methods for Identifying Clinically Important Cryptic Candida Species. J. Microbiol. Methods 2015, 111, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Leguizamón, G.; Fiori, A.; López, L.F.; Gómez, B.L.; Parra-Giraldo, C.M.; Gómez-López, A.; Suárez, C.F.; Ceballos, A.; Van Dijck, P.; Patarroyo, M.A. Characterizing Atypical Candida Albicans Clinical Isolates from Six Third-Level Hospitals in Bogotá, Colombia. BMC Microbiol. 2015, 15, 199. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.F.; Gade, L.; Chow, N.A.; Loparev, V.N.; Juieng, P.; Berkow, E.L.; Farrer, R.A.; Litvintseva, A.P.; Cuomo, C.A. Genomic Insights into Multidrug-Resistance, Mating and Virulence in Candida Auris and Related Emerging Species. Nat. Commun. 2018, 9, 5346. [Google Scholar] [CrossRef] [PubMed]
- Petti, C.A.; Bosshard, P.P.; Brandt, M.E.; Clarridge, J.E.; Feldblyum, T.V.; Foxall, P.; Furtado, M.R.; Pace, N.; Procop, G. Interpretive Criteria for Identification of Bacteria and Fungi by DNA Target Sequencing; Approved Guideline. Clin. Lab. Stand. Inst. (CLSI) Doc. 2008, 28, 19087-1898. [Google Scholar]
- Bosco-Borgeat, M.E.; Taverna, C.G.; Cordoba, S.; Isla, M.G.; Murisengo, O.A.; Szusz, W.; Vivot, W.; Davel, G. Prevalence of Candida Dubliniensis Fungemia in Argentina: Identification by a Novel Multiplex PCR and Comparison of Different Phenotypic Methods. Mycopathologia 2011, 172, 407–414. [Google Scholar] [CrossRef]
- Caceres, D.H.; Forsberg, K.; Welsh, R.M.; Sexton, D.J.; Lockhart, S.R.; Jackson, B.R.; Chiller, T. Candida Auris: A Review of Recommendations for Detection and Control in Healthcare Settings. J. Fungi 2019, 5, 111. [Google Scholar] [CrossRef] [PubMed]
- Who Fungal Priority Pathogens List To Guide Research, Development And Public Health Action, World Health Organization. 2022. Available online: https://www.who.int/publications-detail-redirect/9789240060241 (accessed on 26 January 2024).
- Colombo, A.L.; Cortes, J.A.; Zurita, J.; Guzman-Blanco, M.; Alvarado Matute, T.; De Queiroz Telles, F.; Santolaya, M.E.; Tiraboschi, I.N.; Echevarría, J.; Sifuentes, J.; et al. Recommendations for the Diagnosis of Candidemia in Latin America. Rev. Iberoam. Micol. 2013, 30, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, M.; Anagnostou, T.; Fuchs, B.B.; Caliendo, A.M.; Mylonakis, E. Molecular and Nonmolecular Diagnostic Methods for Invasive Fungal Infections. Clin. Microbiol. Rev. 2014, 27, 490–526. [Google Scholar] [CrossRef] [PubMed]
- Cortés, J.A.; Ruiz, J.F.; Melgarejo-Moreno, L.N.; Lemos, E.V. Candidemia En Colombia. Biomedica 2020, 40, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Camp, I.; Spettel, K.; Willinger, B. Molecular Methods for the Diagnosis of Invasive Candidiasis. J. Fungi 2020, 6, 101. [Google Scholar] [CrossRef]
- Salem-Bango:, Z.; Price, T.K.; Chan, J.L.; Chandrasekaran, S.; Garner, O.B.; Yang, S. Fungal Whole-Genome Sequencing for Species Identification: From Test Development to Clinical Utilization. J. Fungi 2023, 9, 183. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acosta-Mosquera, Y.; Tapia, J.C.; Armas-González, R.; Cáceres-Valdiviezo, M.J.; Fernández-Cadena, J.C.; Andrade-Molina, D. Prevalence and Species Distribution of Candida Clinical Isolates in a Tertiary Care Hospital in Ecuador Tested from January 2019 to February 2020. J. Fungi 2024, 10, 304. https://doi.org/10.3390/jof10050304
Acosta-Mosquera Y, Tapia JC, Armas-González R, Cáceres-Valdiviezo MJ, Fernández-Cadena JC, Andrade-Molina D. Prevalence and Species Distribution of Candida Clinical Isolates in a Tertiary Care Hospital in Ecuador Tested from January 2019 to February 2020. Journal of Fungi. 2024; 10(5):304. https://doi.org/10.3390/jof10050304
Chicago/Turabian StyleAcosta-Mosquera, Yessenia, Juan Carlos Tapia, Rubén Armas-González, María José Cáceres-Valdiviezo, Juan Carlos Fernández-Cadena, and Derly Andrade-Molina. 2024. "Prevalence and Species Distribution of Candida Clinical Isolates in a Tertiary Care Hospital in Ecuador Tested from January 2019 to February 2020" Journal of Fungi 10, no. 5: 304. https://doi.org/10.3390/jof10050304