
Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis

Abstract
:1. Introduction
2. The Tests
3. The Performance
- (1)
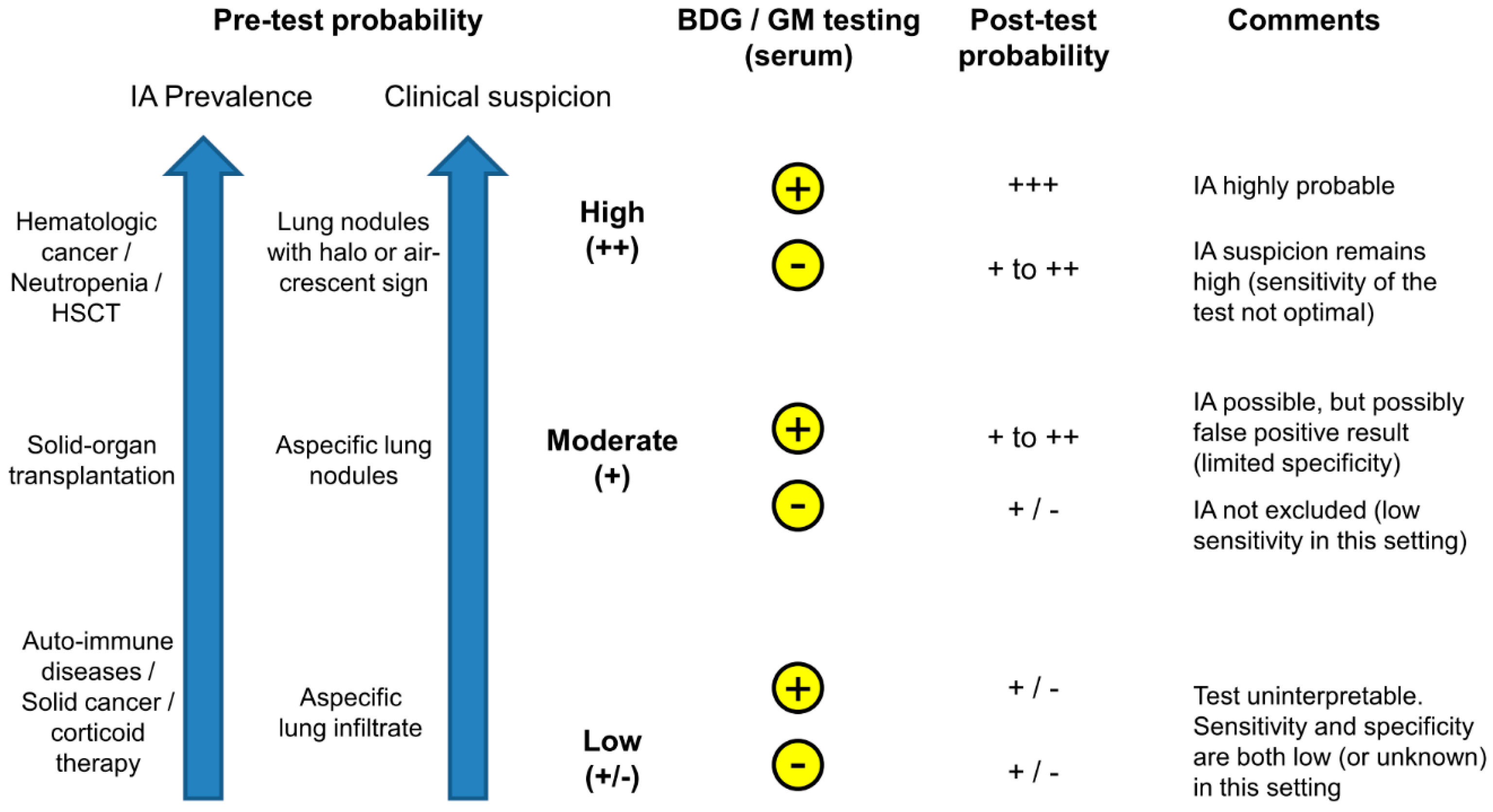
- Among high-risk patients with hematological malignancies and chemotherapy-induced neutropenia or allogeneic HSCT, both tests have a similar performance with a limited sensitivity (60%–80%) and a specificity ≥90%.
- (2)
- The requirement of two consecutive positive tests results in a high specificity (95%–99%), with a slight loss of sensitivity.
- (3)
- Insufficient data are available to assess the performance of these tests in solid-organ transplant recipients and other populations of immunocompromised patients at low or moderate risk of IA. However, sensitivity appears to be markedly decreased in this setting (40% or less), which can be explained by the limited angio-invasion in patients with better immune defenses compared to those with neutropenia. Concerns about poor specificity have also been raised, in particular for BDG testing in lung transplant recipients in one study [12].
- (4)
4. The Clinical Utility
4.1. Which Patient Should Be Tested?
4.2. When and How the Test Should Be Performed?
5. Conclusions
References
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Garbino, J.; Fluckiger, U.; Elzi, L.; Imhof, A.; Bille, J.; Zimmerli, S. Survey of aspergillosis in non-neutropenic patients in Swiss teaching hospitals. Clin. Microbiol. Infect. 2011, 17, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive fungal infections among organ transplant recipients: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [PubMed]
- Marchetti, O.; Lamoth, F.; Mikulska, M.; Viscoli, C.; Verweij, P.; Bretagne, S. ECIL recommendations for the use of biological markers for the diagnosis of invasive fungal diseases in leukemic patients and hematopoietic SCT recipients. Bone Marrow Transplant. 2012, 47, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Karageorgopoulos, D.E.; Vouloumanou, E.K.; Ntziora, F.; Michalopoulos, A.; Rafailidis, P.I.; Falagas, M.E. β-d-glucan assay for the diagnosis of invasive fungal infections: A meta-analysis. Clin. Infect. Dis. 2011, 52, 750–770. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Cruciani, M.; Mengoli, C.; Castagnola, E.; Lortholary, O.; Richardson, M.; Marchetti, O. β-Glucan antigenemia assay for the diagnosis of invasive fungal infections in patients with hematological malignancies: A systematic review and meta-analysis of cohort studies from the Third European Conference on Infections in Leukemia (ECIL-3). Clin. Infect. Dis. 2012, 54, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Leeflang, M.M.; Debets-Ossenkopp, Y.J.; Visser, C.E.; Scholten, R.J.; Hooft, L.; Bijlmer, H.A.; Reitsma, J.B.; Bossuyt, P.M.; Vandenbroucke-Grauls, C.M. Galactomannan detection for invasive aspergillosis in immunocompromized patients. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Lu, Y.; Chen, Y.Q.; Guo, Y.L.; Qin, S.M.; Wu, C.; Wang, K. Diagnosis of invasive fungal disease using serum 1,3-β-d-glucan: A bivariate meta-analysis. Intern. Med. 2011, 50, 2783–2791. [Google Scholar] [CrossRef] [PubMed]
- Onishi, A.; Sugiyama, D.; Kogata, Y.; Saegusa, J.; Sugimoto, T.; Kawano, S.; Morinobu, A.; Nishimura, K.; Kumagai, S. Diagnostic accuracy of serum 1,3-β-d-glucan for Pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: Systematic review and meta-analysis. J. Clin. Microbiol. 2012, 50, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.D.; Fine, J.P.; Safdar, N. Diagnosis of invasive aspergillosis using a galactomannan assay: A meta-analysis. Clin. Infect. Dis. 2006, 42, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.D.; Smith, P.B.; Davis, R.D.; Perfect, J.R.; Reller, L.B. The 1,3-β-d-glucan test as an aid to early diagnosis of invasive fungal infections following lung transplantation. J. Clin. Microbiol. 2010, 48, 4083–4088. [Google Scholar] [CrossRef] [PubMed]
- Herbrecht, R.; Letscher-Bru, V.; Oprea, C.; Lioure, B.; Waller, J.; Campos, F.; Villard, O.; Liu, K.L.; Natarajan-Ame, S.; Lutz, P.; et al. Aspergillus galactomannan detection in the diagnosis of invasive aspergillosis in cancer patients. J. Clin. Oncol. 2002, 20, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.B.; Benjamin, D.K., Jr.; Alexander, B.D.; Johnson, M.D.; Finkelman, M.A.; Steinbach, W.J. Quantification of 1,3-β-d-glucan levels in children: Preliminary data for diagnostic use of the β-glucan assay in a pediatric setting. Clin. Vaccine Immunol. 2007, 14, 924–925. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.L.; Chen, Y.Q.; Wang, K.; Qin, S.M.; Wu, C.; Kong, J.L. Accuracy of BAL galactomannan in diagnosing invasive aspergillosis: A bivariate metaanalysis and systematic review. Chest 2010, 138, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Zou, M.; Tang, L.; Zhao, S.; Zhao, Z.; Chen, L.; Chen, P.; Huang, Z.; Li, J.; Fan, X. Systematic review and meta-analysis of detecting galactomannan in bronchoalveolar lavage fluid for diagnosing invasive aspergillosis. PLoS ONE 2012, 7, e43347. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.J.; Jaber, R.A.; Leather, H.L.; Wingard, J.R.; Staley, B.; Wheat, L.J.; Cline, C.L.; Rand, K.H.; Schain, D.; Baz, M.; et al. Bronchoalveolar lavage galactomannan in diagnosis of invasive pulmonary aspergillosis among solid-organ transplant recipients. J. Clin. Microbiol. 2007, 45, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Luong, M.L.; Clancy, C.J.; Vadnerkar, A.; Kwak, E.J.; Silveira, F.P.; Wissel, M.C.; Grantham, K.J.; Shields, R.K.; Crespo, M.; Pilewski, J.; et al. Comparison of an Aspergillus real-time polymerase chain reaction assay with galactomannan testing of bronchoalvelolar lavage fluid for the diagnosis of invasive pulmonary aspergillosis in lung transplant recipients. Clin. Infect. Dis. 2011, 52, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Avni, T.; Levy, I.; Sprecher, H.; Yahav, D.; Leibovici, L.; Paul, M. Diagnostic accuracy of PCR alone compared to galactomannan in bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis: A systematic review. J. Clin. Microbiol. 2012, 50, 3652–3658. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.M.; Maertens, J.A.; Lagrou, K.; Driessen, G.J.; Cornelissen, J.J.; Rijnders, B.J. diagnostic performance of galactomannan antigen testing in cerebrospinal fluid. J. Clin. Microbiol. 2016, 54, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Alexander, B.D. Nonmolecular methods for the diagnosis of respiratory fungal infections. Clin. Lab. Med. 2014, 34, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Sulahian, A.; Touratier, S.; Ribaud, P. False positive test for aspergillus antigenemia related to concomitant administration of piperacillin and tazobactam. N. Engl. J. Med. 2003, 349, 2366–2367. [Google Scholar] [CrossRef] [PubMed]
- Mikulska, M.; Furfaro, E.; Del Bono, V.; Raiola, A.M.; Ratto, S.; Bacigalupo, A.; Viscoli, C. Piperacillin/tazobactam (Tazocin) seems to be no longer responsible for false-positive results of the galactomannan assay. J. Antimicrob. Chemother. 2012, 67, 1746–1748. [Google Scholar] [CrossRef] [PubMed]
- Vergidis, P.; Razonable, R.R.; Wheat, L.J.; Estes, L.; Caliendo, A.M.; Baden, L.R.; Wingard, J.R.; Baddley, J.; Assi, M.; Norris, S.; et al. Reduction in false-positive Aspergillus serum galactomannan enzyme immunoassay results associated with use of piperacillin-tazobactam in the United States. J. Clin. Microbiol. 2014, 52, 2199–2201. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.; Van Eldere, J.; Verhaegen, J.; Verbeken, E.; Verschakelen, J.; Boogaerts, M. Use of circulating galactomannan screening for early diagnosis of invasive aspergillosis in allogeneic stem cell transplant recipients. J. Infect. Dis. 2002, 186, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Senn, L.; Robinson, J.O.; Schmidt, S.; Knaup, M.; Asahi, N.; Satomura, S.; Matsuura, S.; Duvoisin, B.; Bille, J.; Calandra, T.; et al. 1,3-β-d-glucan antigenemia for early diagnosis of invasive fungal infections in neutropenic patients with acute leukemia. Clin. Infect. Dis. 2008, 46, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Weisser, M.; Rausch, C.; Droll, A.; Simcock, M.; Sendi, P.; Steffen, I.; Buitrago, C.; Sonnet, S.; Gratwohl, A.; Passweg, J.; et al. Galactomannan does not precede major signs on a pulmonary computerized tomographic scan suggestive of invasive aspergillosis in patients with hematological malignancies. Clin. Infect. Dis. 2005, 41, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, A.; Porcher, R.; Menotti, J.; Poirot, J.L.; Chagnon, K.; Vekhoff, A.; Cornet, M.; Isnard, F.; Raffoux, E.; Brethon, B.; et al. Prospective evaluation of clinical and biological markers to predict the outcome of invasive pulmonary aspergillosis in hematological patients. J. Clin. Microbiol. 2012, 50, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Bryar, J.M.; Baden, L.R.; Marty, F.M. Prognostic features of galactomannan antigenemia in galactomannan-positive invasive aspergillosis. J. Clin. Microbiol. 2010, 48, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Miceli, M.H.; Grazziutti, M.L.; Woods, G.; Zhao, W.; Kocoglu, M.H.; Barlogie, B.; Anaissie, E. Strong correlation between serum aspergillus galactomannan index and outcome of aspergillosis in patients with hematological cancer: Clinical and research implications. Clin. Infect. Dis. 2008, 46, 1412–1422. [Google Scholar] [CrossRef] [PubMed]
- Woods, G.; Miceli, M.H.; Grazziutti, M.L.; Zhao, W.; Barlogie, B.; Anaissie, E. Serum Aspergillus galactomannan antigen values strongly correlate with outcome of invasive aspergillosis: A study of 56 patients with hematologic cancer. Cancer 2007, 110, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Baden, L.R.; Marty, F.M. Post-diagnostic kinetics of the 1,3-β-d-glucan assay in invasive aspergillosis, invasive candidiasis and Pneumocystis jirovecii pneumonia. Clin. Microbiol. Infect. 2012, 18, E122–E127. [Google Scholar] [CrossRef] [PubMed]
- Cordonnier, C.; Pautas, C.; Maury, S.; Vekhoff, A.; Farhat, H.; Suarez, F.; Dhedin, N.; Isnard, F.; Ades, L.; Kuhnowski, F.; et al. Empirical versus preemptive antifungal therapy for high-risk, febrile, neutropenic patients: A randomized, controlled trial. Clin. Infect. Dis. 2009, 48, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Girmenia, C.; Micozzi, A.; Gentile, G.; Santilli, S.; Arleo, E.; Cardarelli, L.; Capria, S.; Minotti, C.; Cartoni, C.; Brocchieri, S.; et al. Clinically driven diagnostic antifungal approach in neutropenic patients: A prospective feasibility study. J. Clin. Oncol. 2010, 28, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.; Theunissen, K.; Verhoef, G.; Verschakelen, J.; Lagrou, K.; Verbeken, E.; Wilmer, A.; Verhaegen, J.; Boogaerts, M.; Van Eldere, J. Galactomannan and computed tomography-based preemptive antifungal therapy in neutropenic patients at high risk for invasive fungal infection: A prospective feasibility study. Clin. Infect. Dis. 2005, 41, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Klont, R.; Masson, C.; Theunissen, K.; Meersseman, W.; Lagrou, K.; Heinen, C.; Crepin, B.; Van Eldere, J.; Tabouret, M.; et al. Optimization of the cutoff value for the Aspergillus double-sandwich enzyme immunoassay. Clin. Infect. Dis. 2007, 44, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- D′Haese, J.; Theunissen, K.; Vermeulen, E.; Schoemans, H.; De Vlieger, G.; Lammertijn, L.; Meersseman, P.; Meersseman, W.; Lagrou, K.; Maertens, J. Detection of galactomannan in bronchoalveolar lavage fluid samples of patients at risk for invasive pulmonary aspergillosis: Analytical and clinical validity. J. Clin. Microbiol. 2012, 50, 1258–1263. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Fungal Biomarker | Assay | Indication | Clinical Sample | Recommended Cut-off 3 | Sensitivity/Specificity 6 |
|---|---|---|---|---|---|
| Galactomannan | Platelia Aspergillus EIA (Bio-Rad Laboratories, Marne-La-Coquette, France) | Invasive aspergillosis | Serum BAL CSF | OD 0.5 OD 0.5–1 4 OD 0.5–2 4 | 60%–80%/80%–95% 85%–90%/90%–95% 85%–90%/95%–100% |
| 1,3-β-d-glucan | Fungitell (Associates of Cape Cod Inc. (East Falmouth, MA, USA)) 1 | Invasive aspergillosis Invasive candidiasis Other invasive mycoses 2 | Serum | 60–80 pg/mL 5 | 60%–80%/80%–95% |
© 2016 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamoth, F. Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis. J. Fungi 2016, 2, 22. https://doi.org/10.3390/jof2030022
Lamoth F. Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis. Journal of Fungi. 2016; 2(3):22. https://doi.org/10.3390/jof2030022
Chicago/Turabian StyleLamoth, Frédéric. 2016. "Galactomannan and 1,3-β-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis" Journal of Fungi 2, no. 3: 22. https://doi.org/10.3390/jof2030022