Automated Analysis of Spatially Resolved X-ray Scattering and Micro Computed Tomography of Artificial and Natural Enamel Carious Lesions



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Sample Preparation
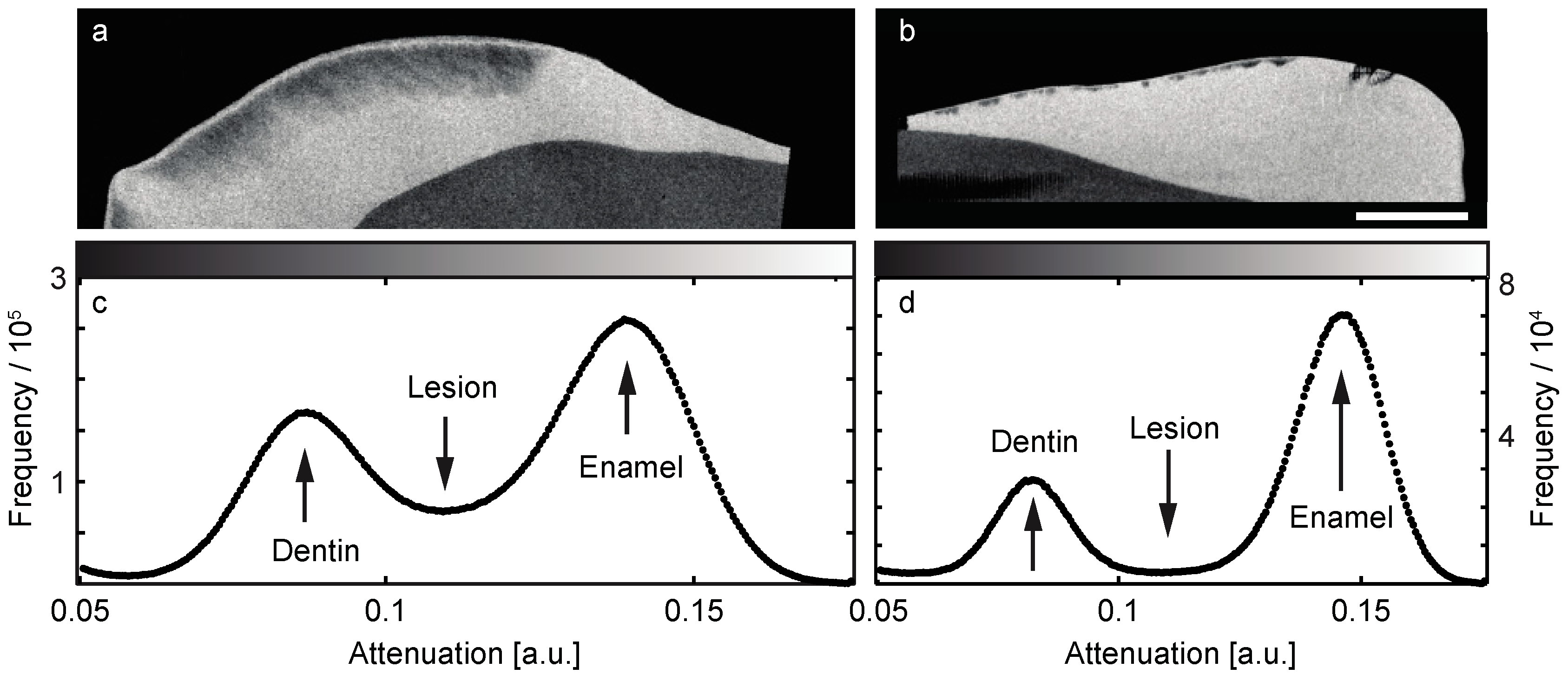
2.3. Micro Computed Tomography
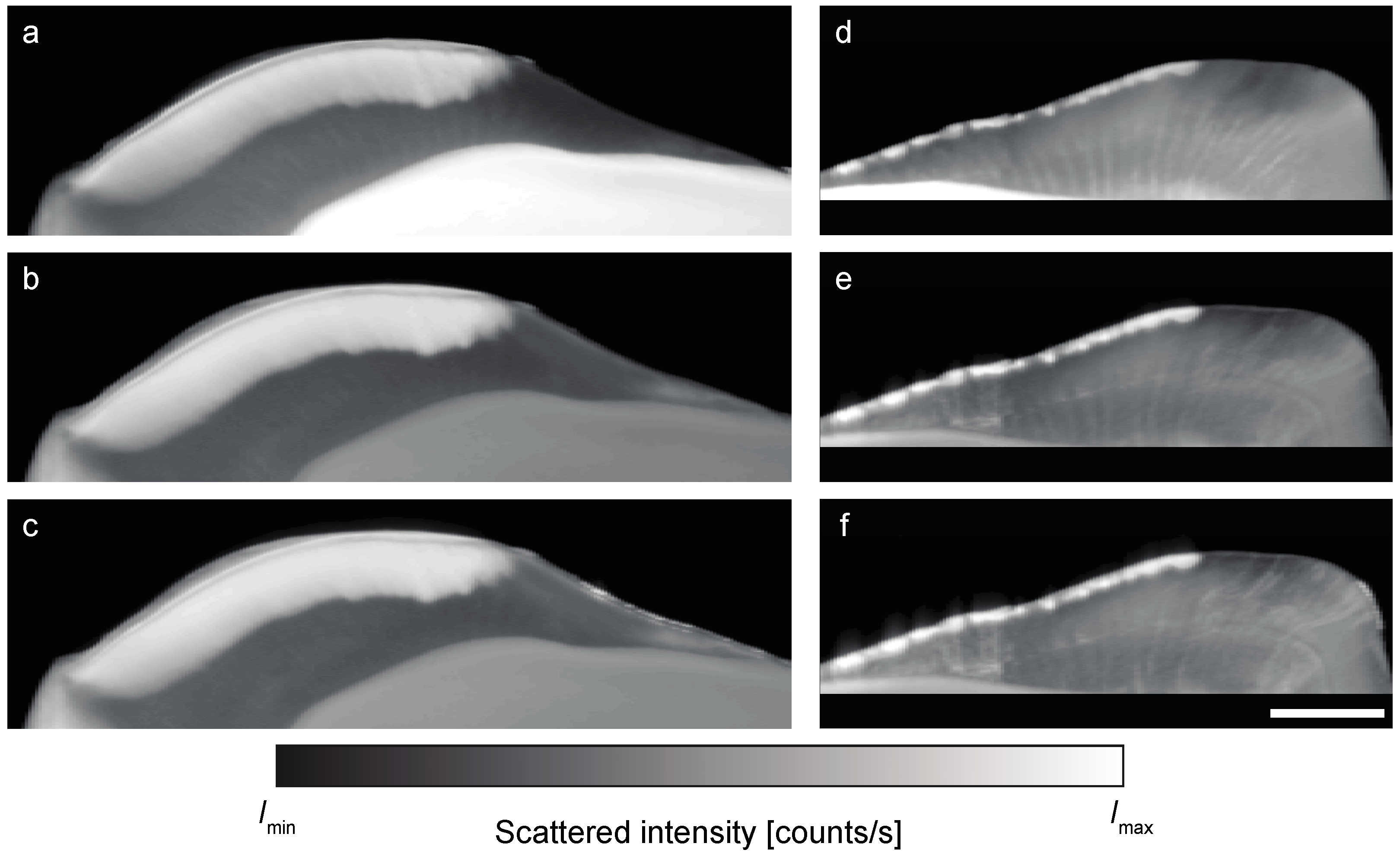
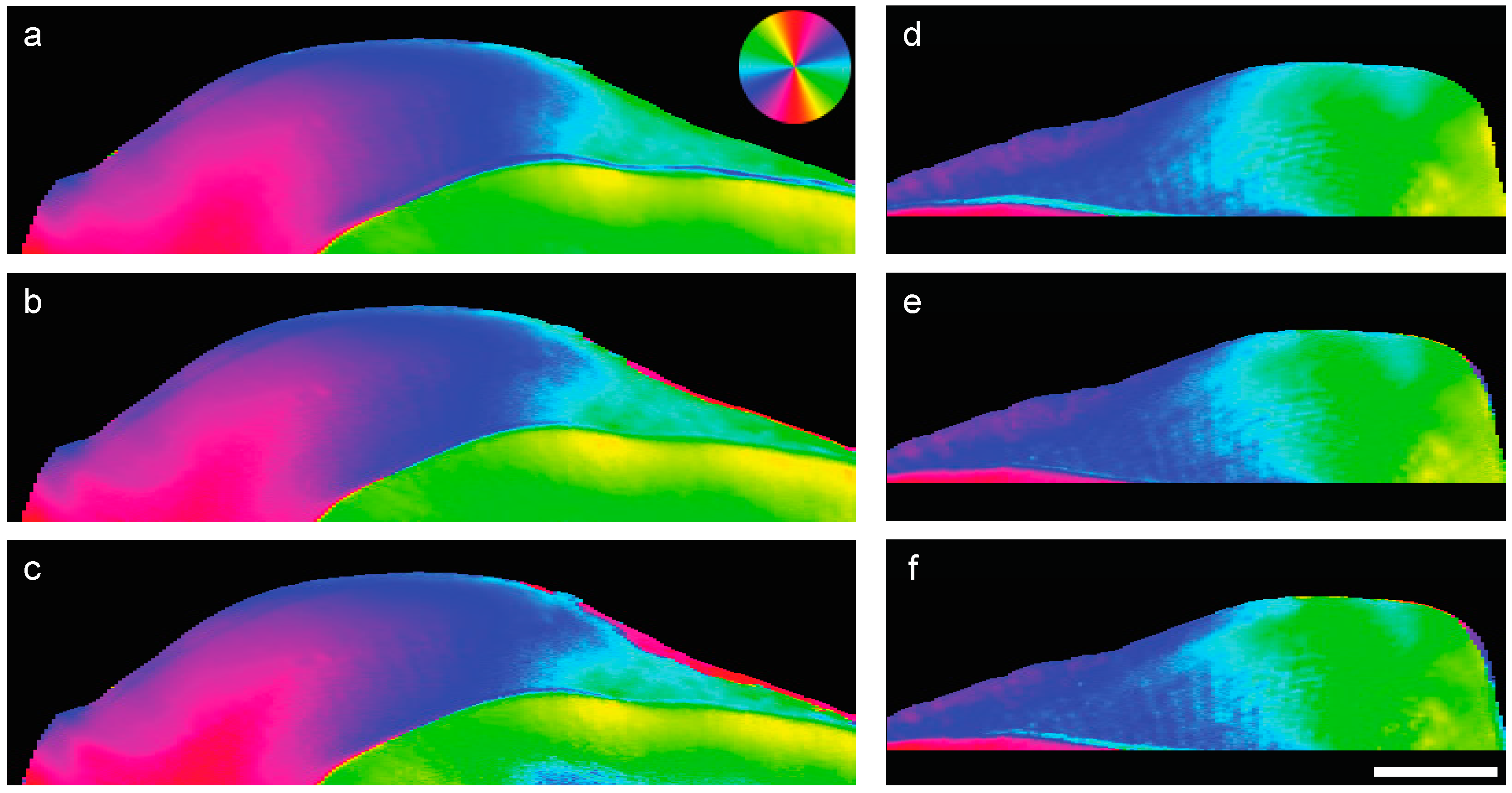
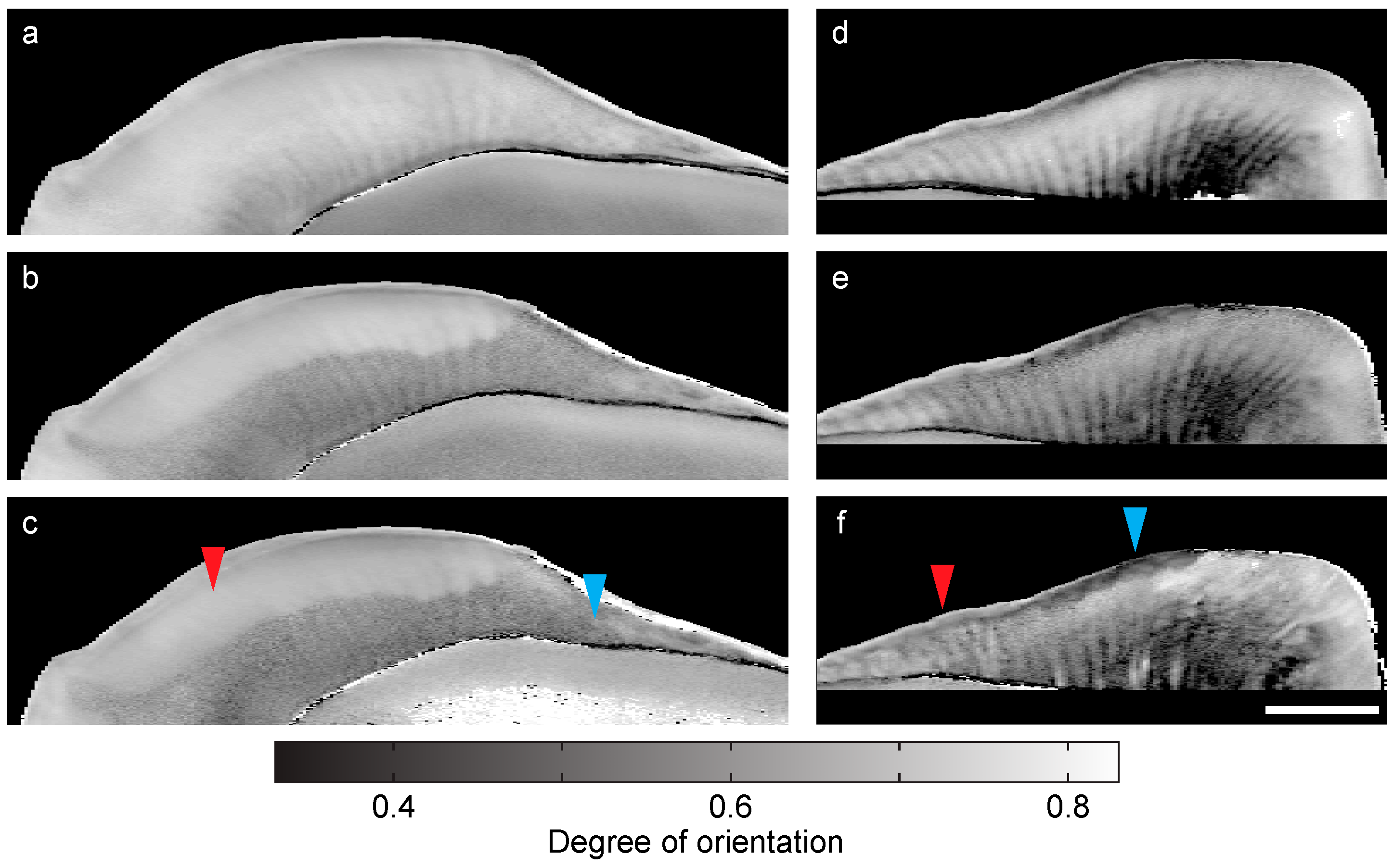
2.4. Small-Angle X-ray Scattering Data Acquisition
2.5. Segmentation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J.L. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Magitot, E. Treatise on Dental Caries. Experimental and Therapeutic Investigations; Houghton, Osgood and Company: Boston, MA, USA, 1878. [Google Scholar]
- Miller, W.D. Agency of micro-organisms in decay of human teeth. Dent. Cosmos 1883, 25, 1–12. [Google Scholar]
- Braga, M.M.; Mendes, F.M.; Martignon, S.; Ricketts, D.N.J.; Ekstrand, K.R. In vitro Comparison of Nyvad’s System and ICDAS-II with Lesion Activity Assessment for Evaluation of Severity and Activity of Occlusal Caries Lesions in Primary Teeth. Caries Res. 2009, 43, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, K.W.; Rodrigues, J.A.; Hug, I.; Stich, H.; Lussi, A. Performance of laser fluorescence devices, visual and radiographic examination for the detection of occlusal caries in primary molars. Clin. Oral Investig. 2011, 15, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Bozdemir, E.; Aktan, A.M.; Ozsevik, A.; Kararslan, E.S.; Ciftci, M.E.; Cebe, M.A. Comparison of different caries detectors for approximal caries detection. J. Dent. Sci. 2016, 11, 293–298. [Google Scholar] [CrossRef]
- Boca, C.; Truyen, B.; Henin, L.; Schulte, A.G.; Stachniss, V.; De Clerck, N.; Cornelis, J.; Bottenberg, P. Comparison of micro-CT imaging and histology for approximal caries detection. Sci. Rep. 2017, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, R.X.; Shao, J.J.; Gao, X.X.; Tao, C.; Ge, J.Y.; Liu, X.J. Noninvasive Assessment of Early Dental Lesion Using a Dual-Contrast Photoacoustic Tomography. Sci. Rep. 2016, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Fratzl, P.; Jakob, J.F.; Rinnerthaler, S.; Roschger, P.; Klaushofer, K. Position-resolved small-angle X-ray scattering of complex biological materials. J. Appl. Crystallogr. 1997, 30, 765–769. [Google Scholar] [CrossRef]
- Gupta, H.S.; Roschger, P.; Zizak, I.; Fratzl-Zelman, N.; Nader, A.; Klaushofer, K.; Fratzl, P. Mineralized microstructure of calcified avian tendons: A scanning small angle X-ray scattering study. Calcif. Tissue Int. 2003, 72, 567–576. [Google Scholar] [PubMed]
- Paris, O. From diffraction to imaging: New avenues in studying hierarchical biological tissues with X-ray microbeams (Review). Biointerphases 2008, 3, FB16–FB26. [Google Scholar] [CrossRef] [PubMed]
- Zizak, I.; Roschger, P.; Paris, O.; Misof, B.M.; Berzlanovich, A.; Brenstorff, S.; Amenitsch, H.; Klaushofer, K.; Fratzl, P. Characteristics of mineral particles in the human bone/cartilage interface. J. Struct. Biol. 2003, 141, 208–217. [Google Scholar] [CrossRef]
- Gutierrez, P.; Piña, C.; Lara, V.H.; Bosch, P. Characterization of enamel with variable caries risk. Arch. Oral. Biol. 2005, 50, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawad, M.; Streuwer, A.; Kilconey, S.H.; Shore, R.C.; Cywinski, R.; Wood, D.J. 2D mapping of texture and lattice parameters of dental enamel. Biomaterials 2007, 28, 2908–2914. [Google Scholar] [CrossRef] [PubMed]
- Deyhle, H.; White, S.N.; Bunk, O.; Beckmann, F.; Müller, B. Nanostructure of the carious tooth enamel lesion. Acta Biomater. 2014, 10, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.; Anderson, P.; Al-Jawad, M. Recovery of Crystallographic Texture in Remineralized Dental Enamel. PLoS ONE 2014, 9, e108879. [Google Scholar] [CrossRef] [PubMed]
- Simmons, L.M.; Al Jawad, M.; Kilcoyne, S.H.; Wood, D.J. Distribution of enamel crystallite orientation through an entire tooth crown studied using synchrotron X-ray diffraction. Eur. J. Oral Sci. 2011, 119, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Yagi, N.; Ohta, T.; Matsuo, Y.; Terada, H.; Kamasaka, K.; To-o, K.; Kometani, T.; Kuriki, T. Evaluation of the distribution and orientation of remineralized enamel crystallites in subsurface lesions by X-ray diffraction. Car. Res. 2010, 44, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Yagi, N.; Ohta, T.; Matsuo, T.; Tanaka, T.; Terada, Y.; Kamasaka, H.; To-o, K.; Kometani, T.; Kuriki, T. Evaluation of enamel crystallites in subsurface lesion by microbeam X-ray diffraction. J. Synchrotron Radiat. 2009, 16, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Shahmoradi, M.; Swain, M.V. Quantitative characterization and micro-CT mineral mapping of natural fissural enamel lesions. J. Dent. 2016, 46, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Rovaris, K.; Matos Ferreira, L.; Oliveira Sousa, T.; Vieira Peroni, L.; Queiroz Freitas, D.; Wenzel, A.; Haiter-Neto, F. Feasibility of micro-computed tomography to detect and classify proximal caries lesions in vitro. Dent. Res. J. 2018, 15, 123–129. [Google Scholar]
- Yagi, N.; Ohta, T.; Matsuo, T.; Tanaka, T.; Terada, Y.; Kamasaka, H.; Kometani, T. A microbeam small-angle X-ray scattering study on enamel crystallites in subsurface lesion. J. Phys. Conf. Ser. 2010, 247, 012024. [Google Scholar] [CrossRef]
- Chien, Y.C.; Burwell, A.K.; Saeki, K.; Fernandez-Martinez, A.; Pugach, M.K.; Nonomura, G.; Habelitz, S.; Ho, S.P.; Rapozo-Hilo, M.; Featherstone, J.D.; et al. Distinct decalcification process of dentin by different cariogenic organic acids: Kinetics, ultrastructure and mechanical properties. Arch. Oral Biol. 2016, 63, 93–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannini, C.; Siliqi, D.; Ladisa, M.; Altamura, D.; Diaz, A.; Beraudi, A.; Sibillano, T.; De Caro, L.; Stea, S.; Baruffaldi, F.; et al. Scanning SAXS-WAXS microscopy on osteoarthritis-affected bone—An age-related study. J. Appl. Crystallogr. 2014, 47, 110–117. [Google Scholar] [CrossRef]
- Lewis, R.A.; Rogers, K.D.; Hall, C.J.; Towns-Andrews, E.; Slawson, S.; Evans, A.; Pinder, S.E.; Ellis, I.O.; Boggis, C.R.M.; Hufton, A.P.; et al. Breast cancer diagnosis using scattered X-rays. J. Synchrotron Radiat. 2000, 7, 348–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falzon, G.; Pearson, S.; Murison, R.; Hall, C.; Siu, K.; Round, A.; Schultke, E.; Kaye, A.H.; Lewis, R. Myelin structure is a key difference in the X-ray scattering signature between meningioma, schwannoma and glioblastoma multiforme. Phys. Med. Biol. 2007, 52, 6543–6553. [Google Scholar] [CrossRef] [PubMed]
- Botta, L.-M.; White, S.N.; Deyhle, H.; Dziadowiec, I.; Schulz, G.; Thalmann, P.; Müller, B. Comparing natural and artificial carious lesions in human crowns by means of conventional hard X-ray micro-tomography and two-dimensional X-ray scattering with synchrotron radiation. Proc. SPIE 2016, 9967, 99670S. [Google Scholar]
- Kind, L.; Stevanovic, S.; Wuttig, S.; Wimberger, S.; Hofer, J.; Müller, B.; Pieles, U. Biomimetic remineralization of carious lesions by self-assembling peptide. J. Dent. Res. 2017, 96, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Deyhle, H.; Schulz, G.; Khimchenko, A.; Bikis, C.N.; Hieber, S.E.; Jaquiery, C.; Kunz, C.; Müller-Gerbl, M.; Hoechel, S.; Saxer, T.; et al. Imaging tissues for biomedical research using the high-resolution micro-tomography system nanotom® m. Proc. SPIE 2016, 9967, 99670Q. [Google Scholar]
- Dziadowiec, I.; Beckmann, F.; Schulz, G.; Deyhle, H.; Müller, B. Characterization of a human tooth with carious lesions using conventional and synchrotron radiation-based micro computed tomography. Proc. SPIE 2014, 9212, 92120W. [Google Scholar]
- Bunk, O.; Bech, M.; Jensen, T.H.; Feidenhans’l, R.; Binderup, T.; Menzel, A.; Pfeiffer, F. Multimodal X-ray scatter imaging. New J. Phys. 2009, 11, 123016. [Google Scholar] [CrossRef]
- Lloyd, S.P. Least square quantization in PCM. IEEE Trans. Inf. Theory 1982, 28, 129–137. [Google Scholar] [CrossRef]
- Müller, B.; Beckmann, F.; Huser, M.; Maspero, F.; Szekely, G.; Ruffieux, K.; Thurner, P.; Wintermantel, E. Non-destructive three-dimensional evaluation of a polymer sponge by micro-tomography using synchrotron radiation. Biomol. Eng. 2002, 19, 73–78. [Google Scholar] [CrossRef]
- Deyhle, H.; Bunk, O.; Müller, B. Nanostructure of healthy and caries-affected human teeth. Nanomed. Nanotechnol. Biol. Med. 2011, 7, 694–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sui, T.; Sandholzer, M.A.; Baimpas, N.; Dolbnya, I.P.; Landini, G.; Korsunsky, A.M. Hierarchical modelling of elastic behaviour of human enamel based on synchrotron diffraction characterisation. J. Struct. Biol. 2013, 184, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Schulz, G.; Waschkies, C.; Pfeiffer, F.; Zanette, I.; Weitkamp, T.; David, C.; Müller, B. Multimodal imaging of human cerebellum—Merging X-ray phase microtomography, magnetic resonance microscopy and histology. Sci. Rep. 2012, 2, 826. [Google Scholar] [CrossRef] [PubMed]
- Stalder, A.; Ilgenstein, B.; Chicerova, N.; Deyhle, H.; Beckmann, F.; Müller, B.; Hieber, S.E. Combined use of micro computed tomography and histology to evaluate the regenerative capacity of bone grafting materials. Int. J. Mater. Res. 2014, 105, 679–691. [Google Scholar] [CrossRef] [Green Version]
- Deyhle, H.; Dziadowiec, I.; Kind, L.; Thalmann, P.; Schulz, G.; Müller, B. Mineralization of early stage carious lesions in vitro—A quantitative approach. Dent. J. 2015, 3, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, J.M.; Dundon, K.A.; Vernon, P.G.; Damato, F.A.; Huntington, E.; Exterkate, R.A.M.; Wefel, J.S.; Jordan, T.; Stephen, K.W.; Roberts, A.J. Preparation and measurement of artificial enamel lesions, a four-laboratory ring test. Car. Res. 1996, 30, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T. Refraction and Scattering Based X-ray Imaging; University of Copenhagen: Copenhagen, Denmark, 2010. [Google Scholar]
- Lautensack, J.; Rack, A.; Redenbach, C.; Zabler, S.; Fischer, H.; Graber, H.G. In situ demineralisation of human enamel studied by synchrotron-based X-ray microtomography—A descriptive pilot-study. Micron 2013, 44, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Christoffersen, J. The nature of early caries lesions in enamel. J. Dent. Res. 1986, 65, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, F.; Bech, M.; Bunk, O.; Kraft, P.; Eikenberry, E.F.; Brönnimann, C.; Grünzweig, C.; David, C. Hard-X-ray dark-field imaging using a grating interferometer. Nat. Mater. 2008, 7, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Revol, V.; Jerjen, I.; Kottler, C.; Schutz, P.; Kaufmann, R.; Luthi, T.; Sennhauser, U.; Straumann, U.; Urban, C. Sub-pixel porosity revealed by X-ray scatter dark field imaging. J. Appl. Phys. 2011, 110, 5. [Google Scholar] [CrossRef]
- Jensen, T.; Bech, M.; Zanette, I.; Weitkamp, T.; David, C.; Deyhle, H.; Feidenhans’l, R.; Pfeiffer, F. Directional X-ray dark-field imaging of strongly ordered systems. Phys. Rev. B 2010, 82, 214103. [Google Scholar] [CrossRef]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deyhle, H.; White, S.N.; Botta, L.; Liebi, M.; Guizar-Sicairos, M.; Bunk, O.; Müller, B. Automated Analysis of Spatially Resolved X-ray Scattering and Micro Computed Tomography of Artificial and Natural Enamel Carious Lesions. J. Imaging 2018, 4, 81. https://doi.org/10.3390/jimaging4060081
Deyhle H, White SN, Botta L, Liebi M, Guizar-Sicairos M, Bunk O, Müller B. Automated Analysis of Spatially Resolved X-ray Scattering and Micro Computed Tomography of Artificial and Natural Enamel Carious Lesions. Journal of Imaging. 2018; 4(6):81. https://doi.org/10.3390/jimaging4060081
Chicago/Turabian StyleDeyhle, Hans, Shane N. White, Lea Botta, Marianne Liebi, Manuel Guizar-Sicairos, Oliver Bunk, and Bert Müller. 2018. "Automated Analysis of Spatially Resolved X-ray Scattering and Micro Computed Tomography of Artificial and Natural Enamel Carious Lesions" Journal of Imaging 4, no. 6: 81. https://doi.org/10.3390/jimaging4060081
APA StyleDeyhle, H., White, S. N., Botta, L., Liebi, M., Guizar-Sicairos, M., Bunk, O., & Müller, B. (2018). Automated Analysis of Spatially Resolved X-ray Scattering and Micro Computed Tomography of Artificial and Natural Enamel Carious Lesions. Journal of Imaging, 4(6), 81. https://doi.org/10.3390/jimaging4060081