1. Introduction
“
Keep your shoulders back, chest out, back straight!” This is a sentence that is constantly repeated to children; but straight compared to what? And how? The fear that deviations of the spine can interfere with the development of children, becomes an exasperation for parents who berate them because they maintain a bad posture [
1]. Especially during school age, the percentage of children that develop spine disorders increases more and more. Bad posture during study, at home or at school, the backpack, the load of books, are all factors that slowly force the child to assume a bad posture [
1]. It has been confirmed by another study [
2] that a heavy backpack determines a forward head posture, a rounded shoulder posture, or even an increased lateral tilting of the shoulders. But what is being done in this regard? Little or nothing. Only a small percentage of parents are seriously concerned about the posture of their children; and the outcome is that when these children reach adolescence, they show paramorphisms and dysmorphisms that are difficult to correct. The high percentage of adolescents with a poor posture may derive from a lack of postural education at home or at school [
3]. Modulation of postural tone is managed by a complex system that can regulate and adapt itself, the so-called
tonic postural system. The reflexes collaborate in the maintenance of the posture, among them stretch reflex, vestibular, and neck reflexes coordinating the movements of the head and the upper limbs. The postural chains represent a contiguous muscle circuit through which they propagate the forces of the body. The standard posture in the upright position is given by a vertical line which, on the sagittal plane, must pass through the apex of the skull, the spinous process of the second cervical vertebra (C2), the vertebral body of the third lombar vertebra (L3), the calcaneo-cuboid joint that is projected on the support polygon. The
postural evaluation of a subject starts with the past medical history of physical traumas and surgery, daily activities, physical activity and work. In the latter field, nowadays work, especially office work, can mean a long period behind a computer screen, which can provoke postural disorders [
4]. Then a static evaluation on the three planes is performed by analyzing the existing symmetries. The task of the
postural tests is to verify the presence of certain dysfunctions, asymmetries, or problems of the receptors. Some of the most common tests are: dominant eye test, examination of dysmorphic facial features, Romberg test for balance and vestibular apparatus, Bernard Autet test which measures the internal rotation of the foot, and others. The kinesiologist has a main role in prevention and motor re-education. The kinesiatric intervention during adolescence, could improve the quality of adult life, preventing diseases related to postural defects [
5,
6].
The aim of this study was to investigate the prevalence of untreated structural alterations, ascribed to a bad posture (paramorphisms or dysmorphisms), in the adolescent growth phase of Italian high school students.
3. Results
In our group of students (
Table 1), the majority of subjects, 77.50% (62/80), both male and female, had normal weight. There was still a percentage of students, 10% (8/80), who had a BMI lower than the value of 18.5 and were therefore underweight; there were also overweight students 11.25% (9/80), whose BMI was between 25 and 30. Only 26.25% (21/80) of subjects showed a malocclusion: 8.75% type 1 (7/80), 10% type 2 (8/80), and 7.50% type 3 (6/80). Ninety-one percent (73/80) of the students showed excellent skin condition; only a minority, 4%, had a lower elasticity of skin (3/80), and scars or tattoos 5% (4/80), although the presence of these had not proved to be a point of tension for the muscle chains. Only 14% (11/80) showed a lower-trophism of muscles, this condition was confirmed by the subjects themselves who declared they did not play sports or engage in physical activity. The presence of scoliotic deviations was ascertained in 36% (29/80) of students, all had a hump, for 62% of them it was positioned to the right (18/80) and for 38% to the left (11/80). Almost half of the subjects, 47.50% (38/80), showed a non-physiological curve of the cervical and lumbar spine. Exactly 10% (8/80) had a pathological condition of the cervical spine, such as the presence of the typical swan neck where the curve is accentuated, or a situation of the plate neck, namely a reduced cervical curve. The remaining 37.50% (30/80) showed a pathologic condition of the lumbar spine, most frequently a flat or excessive lumbar curvature (hyperlordosis). The latter was prevalent in women who practiced artistic gymnastics during the growth phase. Of the examined sample, 33.75% (27/80) showed a pathologic kyphosis, 17.50% (14/80) hyperkyphosis, and 16.25% (13/80) hypokyphosis.
In this way, 23.75% (19/80) of the subjects studied showed a pathological spine condition involving both lordosis and kyphosis. Ten percent (8/80) of subjects showed a non-physiological condition of the right shoulder; 12.5% (10/80) of the left shoulder, and 5% (4/80) of both shoulders. Usually an asymmetry regarding the height of the shoulders was present; when both shoulders were involved, the forward- or backward-shift of both shoulders was observed. More than half of the examined subjects showed a pathologic condition of the scapulas; 23.75% (19/80) concerned the left scapula, 22.50% (18/80) the right scapula, and 13.75% (11/80) both scapulas. The most frequent situation was that one scapula was shifted forward or backward compared to the other one, and this was observable even when both shoulders had a pathological condition. We also observed the presence, although minimal, of winged scapulas. Almost half of the subjects had a pathological pelvis, the rotation of the pelvis, such as the anteversion or the retroversion, or the possible asymmetry of posterior superior iliac spine or anterior superior iliac spine. Of the examined subjects, 36.25% (29/80) showed an asymmetry of the hips. One more prominent malleolus was observed in 17.5% (14/80), while 6.25% (5/80) of students had an asymmetry between the ankles. Of the studied subjects, 18.75% (15/80) had a foot deformity; in particular 15% (12/80) of those had flat feet, while the remaining 3.75% (3/80) had hollow feet. Three subjects had been operated on because of flat feet, but on examining those subjects, the feet were normal. Only 20% (16/80) of the analyzed subjects showed appreciable fluctuations that could be recorded as positive in the Romberg test.
Table 1.
Anatomical and morphological characteristics of the studied sample.
Table 1.
Anatomical and morphological characteristics of the studied sample.
| Parameters | Total (n = 80) | Female (n = 49) | Male (n = 31) |
|---|
| General examination | | | |
| Underweight | 8 (10%) | 6 (7.5%) | 2 (2.5%) |
| Healthy | 62 (77.5%) | 39 (48.75%) | 23 (28.75%) |
| Overweight | 9 (11.25%) | 4 (5%) | 5 (6.25%) |
| Obese | 1 (1.25%) | 0 (0%) | 1 (1.25%) |
| 1st Degree malocclusion | 7 (8.75%) | 5 (6.25%) | 2 (2.5%) |
| 2nd Degree malocclusion | 8 (10%) | 5 (6.25%) | 3 (3.75%) |
| 3rd Degree malocclusion | 6 (7.5%) | 4 (5%) | 2 (2.5%) |
| Hypoelastic skin | 3 (3.75%) | 1 (1.25%) | 2 (2.5%) |
| Scars or Tattoo | 4 (5%) | 3 (3.75%) | 1 (1.25%) |
| Low muscle trophism | 11 (13.75%) | 9 (11.25%) | 2 (2.5%) |
| Muscoloskeletal and joint system | | | |
| Scoliosis | 29 (36.25%) | 18 (22.5%) | 11 (13.75%) |
| Right hump | 18 (22.5%) | 12 (15%) | 6 (7.5%) |
| Left hump | 11 (13.75%) | 6 (7.5%) | 5 (6.25%) |
| Pathologic cervical lordosis | 8 (10%) | 5 (6.25%) | 3 (3.75%) |
| Pathologic lumbar lordosis | 30 (37.5%) | 17 (21.25%) | 13 (16.25%) |
| Hyperkyphosis | 14 (17.5%) | 6 (7.5%) | 8 (10%) |
| Hypokyphosis | 13 (16.25%) | 8 (10%) | 5 (6.25%) |
| Pathologic right shoulder | 8 (10%) | 5 (6.25%) | 3 (3.75%) |
| Pathologic left shoulder | 10 (12.5%) | 6 (7.5%) | 4 (5%) |
| Pathologic both shoulders | 4 (5%) | 2 (2.5%) | 2 (2.5%) |
| Pathologic right scapula | 18 (22.5%) | 10 (12.5%) | 8 (10%) |
| Pathologic left scapula | 19 (23.75%) | 14 (17.5%) | 5 (6.25%) |
| Pathologic both scapulas | 11 (13.75%) | 8 (10%) | 3 (3.75%) |
| Pathologic pelvis | 39 (48.75%) | 26 (32.5%) | 13 (16.25%) |
| Asymmetry of hips | 29 (36.25%) | 22 (27.5%) | 7 (8.75%) |
| Prominent malleolus | 14 (17.5%) | 9 (11.25%) | 5 (6.25%) |
| Asymmetry of malleolus | 5 (6.25%) | 3 (3.75%) | 2 (2.5%) |
| Flat feet | 12 (15%) | 6 (7.5%) | 6 (7.5%) |
| Hollow feet | 3 (3.75%) | 2 (2.5%) | 1 (1.25%) |
4. Discussion
Puberty is one of the most important phases in growth, characterized by morphological, physiological, and functional changes. In this period, it is important to pay attention to the musculoskeletal development, in order to allow a correct growth of the locomotor apparatus. The best prevention of paramorphisms is the correct movement. The continuous increase of postural defects and dysmorphic features is closely related to the reduction of the possibility of engaging in physical activity for children. This study was based on the postural analysis of students who are close to concluding the puberty phase; so essentially we observed the presence of dysmorphic features or paramorphisms that with time can become hard to correct. Correcting posture is an important aim for physical therapy since people with postural alteration can have muscular modifications which can cause movement problems or change joint alignment. These impairments can lead to problems in everyday life [
7]. The lack of convergence movements can be determined by a cervical trauma, spinal fractures, or malocclusions. These deficits can lead to headaches, instability, and motor incoordination. There are a lot of correlations between the motor and the visual systems, indeed the importance of visual function in motor coordination, maintenance of posture, and ambulation has been widely demonstrated [
8,
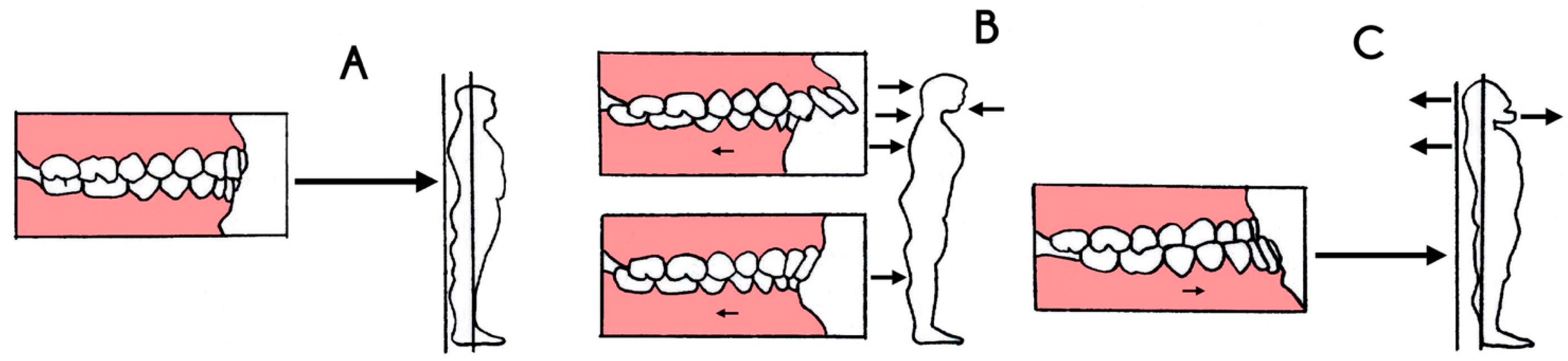
9]. According to some posturology studies, the stomatognathic system plays a particular role. It has been shown that the body creates a posture apparently “correct” according to the occlusal class present. The situation in which the dental arches have no anomalies is called normal occlusion (
Figure 3A). The condition in which the upper teeth are not perfectly aligned with the lower ones is called malocclusion. The tension created by the malocclusion, determines a muscle contraction which leads to postural modifications. In the literature, the correlation between the incidence of malocclusion and orthopedic problems has an increasingly high percentage [
8]. So cooperation between orthodontics and orthopedics becomes crucial in order to determine a correct development of the stomatognathic system and the upper cervical spine [
10]. Moreover, good condition of the skin is a symptom of physical wellness and proper nutrition. Authors showed how the presence of post burn scars causes a lateral cervical flexion contracture [
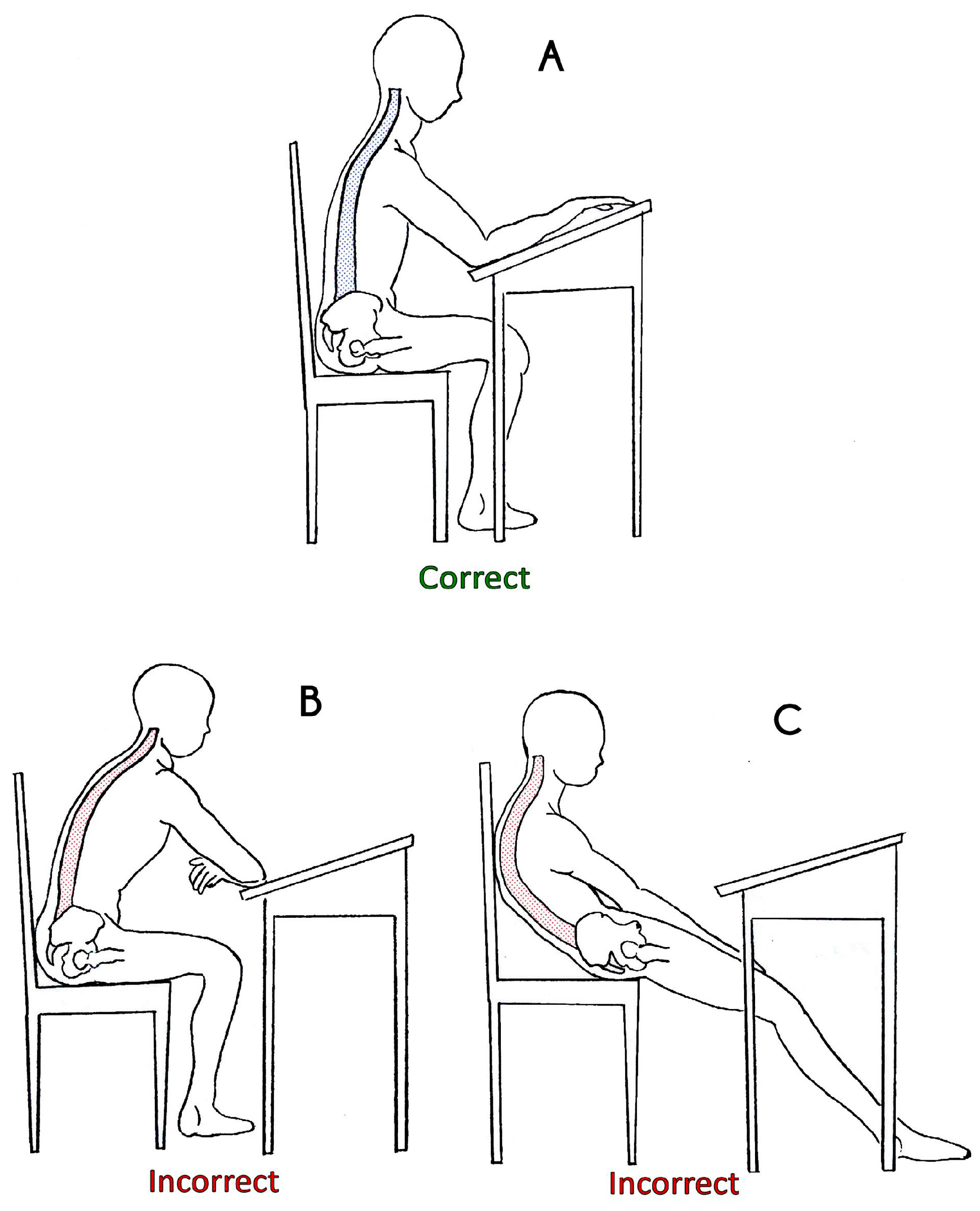
11]. In our study the observation of the classrooms provided relatively negative results, since the percentage of students with a correct posture was low (data not shown). The school desk, defined by Descovich like “the mold of paramorphisms”, had a significant importance (
Figure 4). Obviously not all the students sitting at the desks are predisposed to develop paramorphisms, but the percentage is quite high. The long time spent sitting at the school desk can cause frequent pain, resulting from a wrong sitting posture or static body posture [
12].
Figure 4.
Graphic design of correct or incorrected posture at the school desk. (A) Correct posture while sitting on the school desk; (B) Wrong posture at the school desk; and (C) Wrong posture on the chair.
Figure 4.
Graphic design of correct or incorrected posture at the school desk. (A) Correct posture while sitting on the school desk; (B) Wrong posture at the school desk; and (C) Wrong posture on the chair.
In the correct sitting posture (
Figure 4A) the subject is placed with the spine slightly inclined forward with the load on the hip joint instead of the spine, which must remain straight, supported by the arms resting over the school desk. Most of students tended to be lying on the chair (
Figure 4C) or even lying on the school desk (
Figure 4B). To avoid this problem, some useful tips have been proposed to the teacher to improve this condition, such as letting the students periodically change their place in the classroom; planning some free minutes to let the students relax for a while at the beginning of every lesson; arranging the desks in an amphitheater shape. Moreover, the backpack plays a negative role in posture. Nowadays the students tend to carry it with one shoulder instead of two, creating a posture of compensation from the attempt to rebalance the center of gravity of the body. When the backpack’s load is heavy, this tends to bend the backs of the students; for this fact, literature recommends using backpacks with wheels, thus avoiding carrying it on the shoulders. Pathological deviations that affect the spine are divided between congenital and acquired. The deviations are due to a formation or segmentation congenital defect, and often are associated with scoliosis. When the vertebrae bodies are fused together there is a kyphotic deformity; while we talk about lordotic deformity when the fusion refers to vertebral arches. Acquired deviations are pathological conditions of increase or decrease of the curvature over the physiological limits, such as dorsal hyperkyphosis, lumbar hyperlordosis, and thoracolumbar kyphosis. The
structural shapes are the idiopathic rounding spine and Scheuermann's disease, which is a form of osteochondrosis of the spine with structural deformity of the vertebral elements and increased posterior rounding of the thoracic spine [
13].
The non-structural shapes are reversible postures presenting just a condition of flexion of the vertebral bodies, and not a physiological modification of them. The
mixed shapes are situations in which both modifications may be present. Spinal deformity in addition to modifying the shapes of the trunk, changes the relation between muscles, bones, and the whole structure of the body [
14]. S
coliosis is an alteration of the spine with an unknown etiology, characterized by a deflection on the three-dimensional plane [
15]. A distinction is made between unstructural scoliosis defined as “attitude”, and a structural scoliosis which is the real one in the strict sense. The scoliotic posture is characterized by a lateral deviation of the spine not associated with a rotation of the vertebrae. While the proper scoliosis with a rotation on the three-dimensional plane is divided in idiopathic, secondary, and congenital. When the scoliosis regards the thoracic spine, the ribs attached to the transverse processes follow the direction of the apophyses and form the typical overhang called hump. The presence of the hump is essential for the diagnosis of scoliosis (except congenital scoliosis), and is indicative of vertebrae rotation. Idiopathic scoliosis can occur throughout life, although the higher percentage of occurrence is during growth. Obviously scoliosis interferes with other skeletal elements like the scapulas or the pelvis. A study [
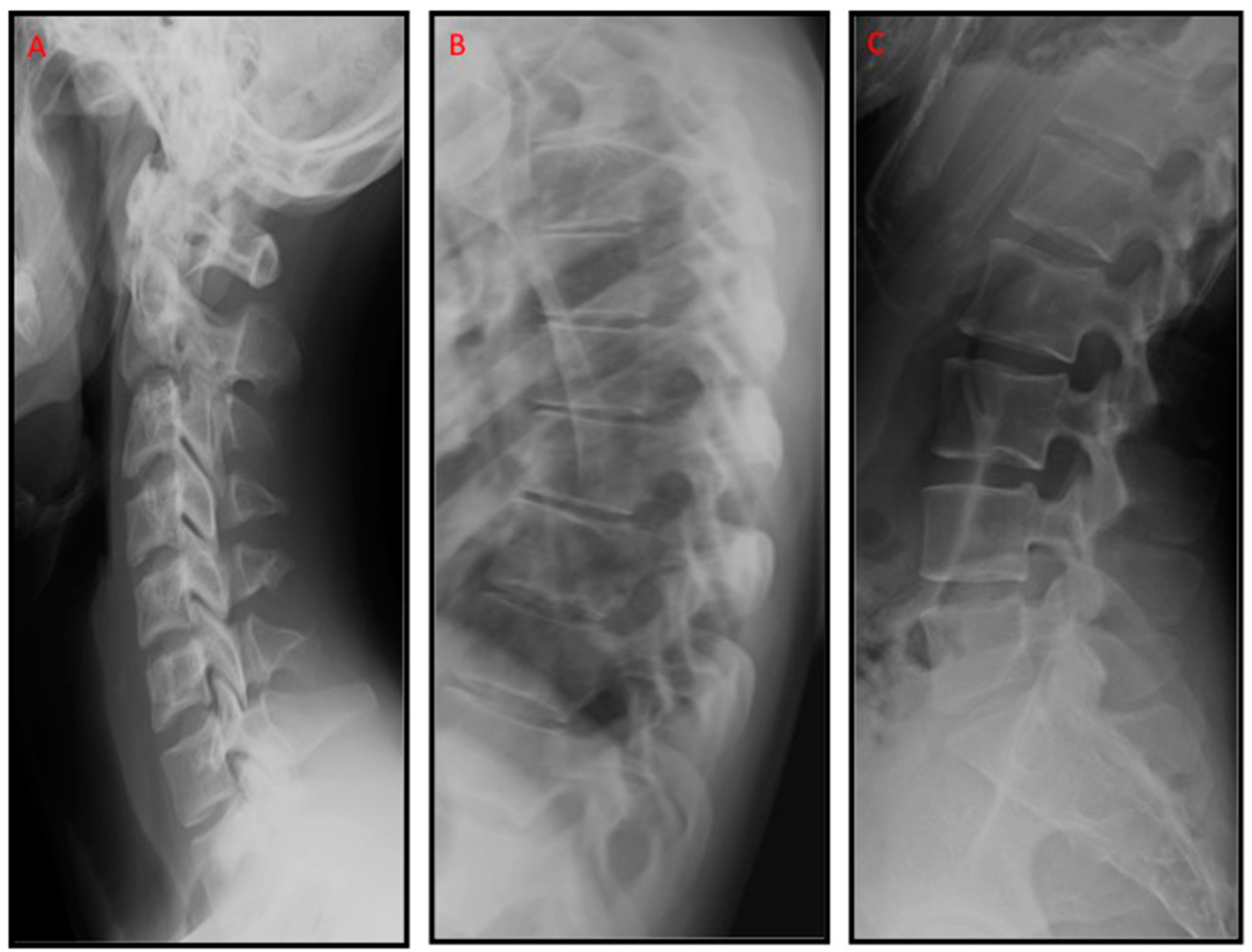
16] has already proven the relationship between the scapulas, the pelvis, and the structural deviations during quiet standing. The different curvatures of idiopathic scoliosis can be observed through
radiological examination; the most prominent features are in the transverse plane for the right thoracic scoliosis, in the frontal plane for the left thoracolumbar one, and in the frontal and transverse plane for the right thoracic-left lumbar one [
17].
From our data, it is possible to observe that only 35% of the subjects showed a good posture or at least the absence of relevant data. Every time we carried out a postural assessment, we asked those students if they practiced sport on a regular basis or if they have ever done it; what is surprising is that only half of them played a sport when young, and a small part of them continued. The absence of movement during the growth phase, resulted in postural defects or aggravation of pre-existing conditions. In addition, several students who had a severe condition of the spine stated that they were not examined by a specialist, since they did not know that they had scoliosis, or that they used a corset as a child, but it was annoying and they left it at that or they did re-educative gymnastics, but it was boring and so they did not do it anymore. What was missing then, is the prevention when aged between 7 and 12 years; it is useful since, with some early corrective intervention, the development of possible anomalies could be prevented [
18]. Moreover, malocclusion [
19] is associated with postural system dysfunctions; like a forward or backward-shift of the shoulder. In 26.25% of students with a malocclusion, it was possible to observe the forward-shift of the shoulder. In accordance with other studies, the protracted and the forward shoulder are common postural disorders among adolescents [
20]. A slouched posture over a long time at the desk could lead to rounded shoulder posture; and the rounded shoulder posture is a factor that can determine upper back pain [
21]. Moreover, observing the lower limbs and the ankles, an asymmetry was often noticed, both by measuring the thigh length and the protruding malleoli. Another important element was the muscular tropism. By asking some questions, it was found again that sport or even just physical activity, was poorly practiced. This condition decreased further in maturity, indeed the percentage of them who still play a sport was really low [
3]. Anyway the ones who showed a reduced tropism represented the minority. Regarding the spine, it was shown that 36% of the examined subjects present a scoliotic deviation. To verify this condition, the spine was initially observed in orthostatism, and some subjects showed a spine with a lateral deviation, not accompanied by a rotation or deformation of the vertebral bodies; so it was clear that this was a scoliotic posture, a paramorphism therefore. The clear difference between scoliosis and scoliotic posture is that the latter is a stance with no anatomical abnormality, since the curve disappears on flexion [
22]. To be sure to deal with a paramorphism and not a dysmorphism, it is crucial to perform a forward bending test, and it was possible to appreciate the presence of a hump. The total absence of an accurate examination during childhood, has led to an increased percentage of subjects with scoliosis. Also on the sagittal plane, the thoracic and lumbar spine showed some pathological conditions, in particular thoracic hyperkyphosis, usually compensated by an accentuated lumbar lordosis. In an interesting study [
23] it was shown that the sagittal configuration of the spine changes during growth; anyway the relation between kyphosis and lordosis becomes more pronounced in men than women. The early approach to a subject with a kyphotic problem includes kinesiatric methods, like aerobic activity and exercise conditioning programs [
24]. Moreover, biofeedback can help to reduce the problems of the spine by fixing the curvatures of it [
25]. Many countries have established school screening programs for scoliosis. The first screening for scoliosis began in 1963 in Minnesota [
26]. In USA 21 States had legislated school screening; 11 states just recommended school screening and the remaining either had volunteer screenings or recommended not to conduct screening in the schools [
27]. While there has been controversy nationally regarding the cost-effectiveness of school screening for scoliosis, most physician groups continue to support the principle of school screening. The American Academy of Pediatrics suggests spinal screening as part of a preventive health visit at 12, 14, and 16 years of age [
27]. In Japan, school-screening program for scoliosis is mandatory by law, but an actual program depends on local educational committees [
27]. The British Orthopaedic Association and the British Scoliosis Society, instead, concluded that it should not be a national policy to routinely screen children for scoliosis throughout the United Kingdom [
28]. In Italy, school screening was introduced sporadically and to a variable extent in most regions and towns. So the school screening programs for scoliosis and other posture alterations remain a subject of considerable controversy.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
