
StepTest4all: Improving the Prediction of Cardiovascular Capacity Assessment in Young Adults

1
Department of Sports Sciences, Instituto Politécnico de Bragança, 5301-856 Bragança, Portugal
2
Research Center in Sports, Health and Human Development (CIDESD), 6201-001 Covilhã, Portugal
3
Research Centre for Active Living and Wellbeing (LiveWell), Instituto Politécnico de Bragança, 5301-856 Bragança, Portugal
*
Author to whom correspondence should be addressed.
J. Funct. Morphol. Kinesiol. 2024, 9(1), 30; https://doi.org/10.3390/jfmk9010030
Submission received: 28 December 2023
/
Revised: 31 January 2024
/
Accepted: 6 February 2024
/
Published: 8 February 2024
(This article belongs to the Special Issue Advances in Physiology of Training)
Abstract
:Cardiovascular capacity, expressed as maximal oxygen uptake (VO2max), is a strong predictor of health and fitness and is considered a key measure of physiological function in the healthy adult population. The aim of this study was to investigate the influence of the physical activity levels (PAlevel) of participants in the StepTest4all (validated protocol for the estimation of VO2max in adults). The sample consisted of 69 participants, including 27 women (age 21.7 ± 3.6 years; body mass = 63.5 ± 14.8 kg; height = 1.64 ± 0.06 m; body mass index = 23.7 ± 5.3 kg/m2) and 42 men (aged 21.7 ± 3.4 years; body mass = 72.0 ± 7.3 kg; height = 1.77 ± 0.07 m; body mass index = 23.1 ± 2.1 kg/m2). The participants were assigned to one of the two groups: (i) the VO2max prediction group and (ii) the prediction model validation group. In the multiple linear regression, the following predictors of VO2max remained significant: sex (p < 0.001), physical activity level (p = 0.014), and HRR60 (p = 0.020). The prediction equation (R2 = 74.0%, SEE = 4.78) showed a close and strong relationship between the measurements and can be expressed as follows: VO2max = 17.105 + 0.260·(HRR60) + 8.563·(sex) + 4.097·(PAlevel), in which HRR60 is the magnitude of the HR decrease (bpm) in one minute immediately after stopping the step, and sex: men = 1, women = 0, and PAlevel is level 1 (low), level 2 (moderate), and level 3 (high). The StepTest4all was shown to be a suitable method for estimating cardiovascular capacity, expressed as VO2max, in young adults. Retaining PAlevel as a significant predictor allows us to better individualize the participants’ VO2max.
1. Introduction
Cardiorespiratory capacity is the ability of the circulatory, respiratory, and muscular systems to deliver and use oxygen during prolonged physical exercise [1]. Expressed as maximal oxygen uptake (VO2max), it has emerged over the years as a strong predictor of overall fitness and a key physiological metric in the healthy adult population [2,3,4,5]. Given the abundance of data supporting the importance of cardiorespiratory capacity, the American Heart Association (AHA) issued a scientific statement in 2016 recommending that cardiorespiratory capacity be considered a clinical vital sign [6]. As such, maintaining and assessing cardiorespiratory fitness plays a critical role in preventing health decline in the general population [7].
Exercise testing, a valuable tool for estimating cardiovascular fitness, diagnosing cardiovascular disease, and predicting mortality, involves the assessment of an individual’s physiological response to physical exertion [8,9]. This is especially true when focusing on functional capacity and heart rate dynamics, such as heart rate recovery (HRR) [10,11]. Heart rate recovery is defined as the reduction in heart rate from peak exercise during a stress test to the rate one minute after stopping exercise [12]. This can also be determined at various time points beyond one minute (HRR60). These additional time points, such as heart rate recovery at 2 min and 5 min, can provide valuable insight into the longer recovery process [13]. The heart rate (HR) response to increased exercise intensity involves complex regulatory mechanisms. This increase in HR is tightly regulated by the action of central and peripheral mechanisms that project afferent inputs to medullary centers in the brain. These afferent inputs result in an appropriate efferent response of the autonomic nervous system branches, i.e., a decrease in parasympathetic and an increase in sympathetic activity [12]. A delayed decline in HR after exercise is a strong predictor of overall mortality [2,12]. Maximal heart rate (HRmax) is another critical parameter commonly used in exercise physiology. It represents the highest heart rate that an individual can achieve during intense physical effort and is a key component in several prescription exercise models [14].
Scientific evidence supports the association between HRR and cardiovascular disease prognosis, highlighting the importance of routine HRR recording in clinical practice [15,16]. Among the various testing modalities available, step testing is of particular importance because of its accessibility to the general population and its ability to assess cardiovascular capacity and HR dynamics during exertion and recovery [17,18,19]. However, existing step tests often have limitations, such as pre-determined durations, efforts that exceed recommended levels for certain demographics, and fixed step heights that are inappropriate for certain individuals [20]. For example, the Harvard Step Test [21] and the YMCA Step Test [22] are commonly used, but their fixed protocols may not account for the varying physical abilities and characteristics of individuals. In addition, the Queen’s College Step Test [23] is limited by a fixed duration, which can be challenging for participants with varying fitness levels.
To address these concerns, Bragada et al. [24] introduced the StepTest4all, a cardiovascular capacity assessment protocol that involves participants in a continuous progressive test on a stable step ranging from 15 to 40 cm, alternating between ascending and descending, with a maximum duration of 10 min. The StepTest4all is distinguished for being adaptable, suitable for people with different physical abilities, with a personalized step height and adjustable difficulty to help participants easily reach the target effort level (80% of HRmax) in a short period of 4 to 10 min. This study retained a significant relationship between VO2max, sex and HRR60 [24]. However, the authors noted that the lack of a variable related to the amount and intensity of the physical activity of participants could be a limitation [24]. A study conducted by Dyrstad et al. [25] emphasized the effect of physical activity level (PAlevel) on cardiorespiratory capacity. This was accomplished by examining the associations between cardiorespiratory fitness and PAlevel, as measured by both the IPAQ (International Physical Activity Questionnaire) and accelerometers, in a large national sample. Key findings showed that individuals, regardless of sex, who met the physical activity recommendations had 5–13% higher VO2max compared to those who did not meet the recommendations. Similarly, a study by Sharma et al. [26] found a significant increase in VO2max after a program of structured and unstructured physical activity in both female and male participants. Therefore, it is important to recognize the role of PAlevel as it plays a pivotal role in influencing cardiorespiratory capacity.
In this context, the aim of this study was to build on the foundation laid by Bragada et al. [24] by refining and validating the StepTest4all protocol. By addressing the limitations identified in the previous research, this study seeks to improve the utility of the protocol in assessing cardiovascular capacity in young adults, possibly through a larger sample size and careful inclusion of physical activity variables in the analysis. Therefore, the aim of this study was to investigate the influence of the PAlevel of participants in the StepTest4all (validated protocol for the estimation of VO2max in adults). Based on the previous assumptions addressed about the importance of PAlevel, it was hypothesized that the PAlevel would be added as a significant predictor of the VO2 concurrently with sex and HRR60.
2. Materials and Methods
2.1. Participants
The sample consisted of 69 participants, including 27 women (age 21.7 ± 3.6 years; body mass = 63.5 ± 14.8 kg; height = 1.64 ± 0.06 m; body mass index = 23.7 ± 5.3 kg/m2) and 42 men (age 21.7 ± 3.4 years; body mass = 72.0 ± 7.3 kg; height = 1.77 ± 0.07 m; body mass index = 23.1 ± 2.1 kg/m2). Those with physical limitations that prevented them from ascending or descending the step or those with medical conditions that prevented them from performing moderate physical exertion were not included in the sample recruitment. All participants signed an informed consent form. All protocols were in accordance with the Declaration of Helsinki regarding human research, and the research design was approved by the Polytechnic Ethics Board.
The groups were randomized and consisted of the following: (i) the VO2max prediction equation group and (ii) the prediction model validation group. The characteristics of the participants are shown in Table 1.
2.2. Physical Activity Level (PAlevel)
The International Physical Activity Questionnaire, in its short form, was used to assess physical activity. This was carried out in accordance with the official IPAQ classification procedure [27], which divides people into three levels of physical activity and is consistent with the categorization shown in several studies [28,29,30]. These values are determined by multiplying the total PA completed during the week by a weighted approximation and then multiplying the result by the duration (minutes), frequency (per week), and MET intensity (MET-min/week) [30].
The official IPAQ scoring system classifies individuals into three PAlevels:
- -
- Low Level: Participants whose energy expenditure does not reach PAlevel.
- -
- Moderate Level: (a) Three or more days of vigorous physical activity for at least 20 min per day; or (b) five or more days of moderate, vigorous, or walking for at least 30 min per day; or (c) five or more days of PA per week (moderate, vigorous, walking, or the sum of PA) for at least 600 MET min each week.
- -
- High Level: At least (a) three days of vigorous physical activity with an energy expenditure of 1500 MET-min/week, or (b) complete at least seven days of physical activity that includes walking, moderate PA, and vigorous PA with an energy expenditure of at least 3000 MET-min/week.
This questionnaire was chosen because of its short form. Extended versions have been shown to overestimate the PAlevel [30]. In addition, it has been developed and tested specifically to determine PAlevels in the adult population, particularly in the 15–69 age group [31].
Table 2 shows the PAlevels of the participants categorized based on the IPAQ scores. The scores were translated into Low (Level 1), Moderate (Level 2), and High (Level 3).
2.3. Data Collection
An electronic scale (Seca 884, Hamburg, Germany) and a digital stadiometer (Seca 242, Hamburg, Germany) were used to measure anthropometric characteristics. A stationary breath-by-breath electronic metabolic device (Cortex, Model MetaLyzer 3B, Leipzig, Germany) was used to monitor HR and VO2. A heart rate transmitter (Polar Electro Oy, Kempele, Finland) is part of the device. The device was calibrated with standard gases prior to each test. The standard error for oxygen and carbon dioxide sensors is 0.1%, according to the manufacturer’s handbook.
Each participant’s VO2 and HR were continuously monitored as they performed the activities in the following order: rest, StepTest4all protocol, and recovery. The HR and VO2 values obtained were used for further analysis: resting values (average of the last minute of rest), values obtained during StepTest4all (average of the last 5 s of each intensity level), and recovery phase (average of the last 5 s of the first minute of recovery). Resting heart rate (HR) and resting VO2 were continuously measured while sitting in a quiet, dimly lit room for ten minutes. The participants were not allowed to nap. The last minute values were used for data analysis. In the recovery phase, although HR values were recorded after the first two minutes, only the value from the first minute was considered. The one-minute recovery period was chosen because it has a higher reproducibility [13].
2.4. StepTest4all Protocol
Figure 1 shows an infogram of the StepTest4all specificities. Each participant completed a continuous progressive test that involved stepping up and down on a steady step. After the step-up phase, the participant stood vertically, supported by both legs, and the opposite leg also stepped up to the platform. This was followed by the step-down phase. The step-down phase ended when the participant returned to the starting point, where he or she stood vertically again, supported by both legs. It began with the same leg as the previous phase.
Using data on each participant’s cardiovascular capacity, step height was determined for each participant. The variables selected were sex, age, physical fitness, height, body mass index (BMI), and smoking status. Each variable was assigned a numerical value as follows: (i) sex (women = 0.5; men = 1), (ii) age (senior = 0, adult = 0.5, young = 1), (iii) physical fitness (insufficiently active = 0, moderately active = 0.5, vigorously active = 1), (iv) body mass index (BMI < 25 = 0.5, BMI < 30 = 0, BMI ≥ 30 = −0.5), and (v) smoking status (smoker = 0, nonsmoker = 0.5). From these data, the step height was calculated using the formula: step height (cm) = 4 × sum of these variables + 15, and it could range from 15 to 40 cm. These ponderation factors were only used to calculate the step’s height.
This formula is the result of many tests conducted on individuals with varying physical abilities and characteristics. Although the step height is important, it can vary somewhat because the adjustment of the ascent and descent speed is mostly used to control the intensity of the load progression until the appropriate value (80% of the HRmax) is reached.
In the current study, a step height of 40 cm and a fast pace resulted in an intensity that reached 80% of the estimated maximum heart rate (HRmax) in 5–10 min. This occurs even in subjects with good physical fitness and tall stature. A height of 40 to 45 cm has been used previously in other protocols, such as the Harvard step [32].
Depending on the metronome control, the test began at a rate of 15 cycles per minute (0.25 Hz). In each cycle, the participant walked up and down the step so that the cycle ended at the same time the second leg reached the ground. The cadence was increased by 2.5 cycles per minute. The test should take no more than ten minutes. Anyone can perform the very slow ascent and descent at the lower limit of 15 cycles per minute, which also serves as a warm-up. The maximum speed of 37.5 cycles per minute is limited to subjects with high physical capacity. A visual representation of the StepTest4all is shown in Figure 2.
The test ended when one of the following criteria was met: (i) when the HR reached 80% of HRmax, (ii) when the subject felt uncomfortable with the exertion, or (iii) when the subject was unable to complete the exercise at the correct cadence. In this case, all participants met the first criterion, i.e., they reached 80% of HRmax. The participants were instructed to stand for two minutes after completion of the test. While standing, participants were asked not to talk, grab, or hold onto anything. Instead, they were encouraged to relax in order to recover as much as possible.
The step height and rhythm increments, together with the intensity threshold of the test (80% of HRmax), allowed for the effective assessment of cardiorespiratory capacity in a manageable length of time (5 to 10 min) on a wide range of subjects. HR was continuously collected during the recovery period using the Garmin Fenix 6 and its HR belt (Garmin International, Inc., Olathe, KS, USA).
HRmax and VO2max were estimated as follows: HRmax was estimated using the formula: HRmax = 208 − 0.7·age [33].
Specifically, by determining the value of VO2 corresponding to HRmax, VO2max was estimated using the individual equation of the regression line corresponding to HR–VO2 obtained from the resting data and during three or more steps of StepTest4all [34]. This value was assumed when measuring VO2max. The range of individual linear regressions (R2) was 0.97 to 0.99, indicating an almost perfect relationship. This is a standard and appropriate method for assessing VO2max in those who may find it inconvenient to perform a maximal test to exhaustion.
Submaximal testing has been shown to be an adequate method for estimating VO2max from the HR–VO2 relationship [35,36]. In a systematic review, Evans and colleagues [37] reported non-significant discrepancies between the measured and predicted VO2max in 28 equations. HR (N = 19) was the most commonly used variable in the predictive equations. A submaximal treadmill-based protocol was also reviewed by Bennett and colleagues [38]. The authors found that estimating VO2max from the projection of HRmax provided a more accurate result.
2.5. Statistical Analysis
First, normality and homoscedasticity were assessed using the Kolmogorov–Smirnov and Levene tests, respectively. The means of the descriptive data were computed together with one standard deviation (1 SD). Stepwise regression (backward elimination) was used to predict VO2max based on the following independent variables, i.e., sex, body mass, height, BMI, PAlevel, and HRR60. Only significant predictors were retained (p < 0.05) in the final model.
The validation procedure between measured and predicted VO2max was based on the following: (i) a comparison of the mean data, (ii) intraclass correlation coefficient (ICC), and (iii) Bland–Altman analysis. The paired samples t-test (p < 0.05) was used to compare the mean data between the estimated and measured VO2max. The effect size index used was Cohen’s d, along with the mean difference and 95% confidence intervals. Cohen’s d was considered to be (i) trivial (<0.20), (ii) small (0.20–0.59), (iii) moderate (0.6–1.19), (iv) large (1.2–1.99), and (v) very large (≥2.0) [39]. The two-way mixed model with an “absolute agreement” definition was used for the ICC [40]. The qualitative interpretation was performed as follows: (i) poor, if ICC < 0.5; (ii) moderate, if 0.5 ≤ ICC < 0.75; (iii) good, if 0.75 ≤ ICC < 0.90; and (iv), excellent, if ICC > 0.90 [40]. Bland–Altman plots showing the mean and difference between the measured and predicted VO2max were analyzed [41]. At least 80% of the plots were considered to be within the ±1.96 standard deviation of the difference (95%CI) for qualitative assessment.
3. Results
In the multiple linear regression, the following predictors of VO2max remained significant: sex (p < 0.001), PAlevel (p = 0.014) and HRR60 (p = 0.020). Age, body mass, height, and BMI were not significant in this model. The prediction equation (R2 = 74.0%, SEE = 4.78) showed a close relationship between the measurements and can be expressed as follows:
VO2max = 17.105 + 0.260·(HRR60) + 8.563·(sex) + 4.097·(PAlevel)
In which VO2max is the maximum oxygen uptake (mL·kg−1·min−1), HRR60 is the heart rate recovery (beats per minute) for one minute immediately after the end of the step test, sex is zero for women and 1 for men, and PAlevel is level 1 (low), level 2 (moderate), and level 3 (high).
Table 3 shows the comparison between measured and estimated VO2max. The results showed nonsignificant differences with a trivial effect size.
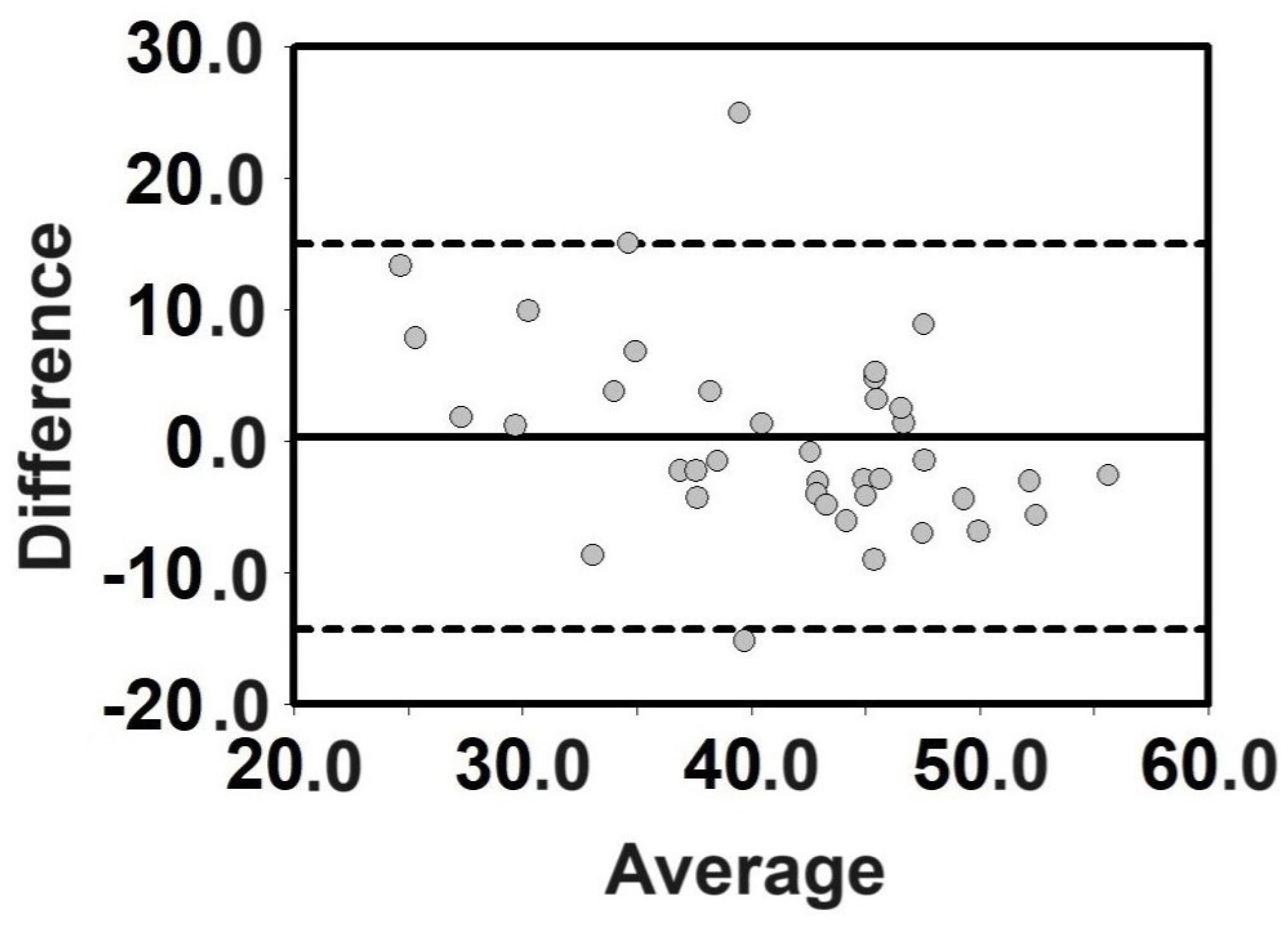
The ICC between measured and predicted VO2max showed good agreement between the measurements (ICC = 0.759, p < 0.001). Figure 3 shows the Bland–Altman plots. This analysis also met the agreement criteria with more than 80% of the plots within the 95% CI.
4. Discussion
The aim of this study was to investigate the influence of the PAlevel of participants in the StepTest4all (validated protocol for estimating VO2max in adults). The study retained the PAlevel as a significant predictor of VO2max simultaneously with the previous predictors (sex, HRR60) of the young adult population. In addition, these results show that the magnitude of the heart rate decrease that occurs immediately after exercise is a useful indicator of cardiovascular capacity. This suggests that StepTest4all can be used to assess cardiovascular capacity for individualized, longitudinal monitoring of cardiovascular fitness. Regular use of the StepTest4all facilitates tracking of cardiovascular fitness progression over time. However, comparing VO2max results between different populations should be carried out with caution. The same VO2max value may indicate different physical capabilities for different demographic variables, including age and sex. Therefore, individual VO2max values should be compared with benchmark tables available in the literature to verify compliance with the proposed standards [42].
An attenuated HRR, defined as an insufficient decrease in HR immediately after exercise, indicates decreased parasympathetic nervous system activity [43,44]. The decrease in HR during recovery is mostly caused by the reactivation of the parasympathetic nervous system, which occurs primarily in the initial phase of recovery [45]. Measurement of the post-exercise HR decline also provides an indication of neural system function [46]. Research has shown that a small drop in heart rate in the minutes following the end of exercise is associated with a higher risk of cardiovascular problems [47] and may even be the cause of early mortality [12]. Conversely, a faster decline in HR after exercise is correlated with improved cardiovascular capacity [13]. A study also found that sedentary healthy individuals can improve heart rate recovery (HRR60 and HRR120) by engaging in moderate-intensity exercise [48].
Adabag and Pierpont’s [49] findings on the recovery of heart rate during exercise are consistent with the current study and emphasize that in recent years, assessments have been used more frequently to evaluate risk and functional autonomic state in both healthy individuals and those with a variety of disorders. HR is usually calculated as the difference (HRR60 and HRR120, respectively) between the maximum heart rate and the heart rate one to two minutes after stopping exercise. Other measures, including HRR180, HRR240, and HRR300, have also been provided. Short-term reproducibility is demonstrated by these results, and validation has been established for HRR60 and HRR120. For example, HRR values of 12–13 bpm in 1 min are referred to as threshold levels in a review by Adabag et al. [49]. However, due to the wide variety of tests used and the level of demand, care must be taken when setting cut-off values (between normal and abnormal). It is known that healthy athletes can recover 60 bpm or more in one minute, which is the ideal recovery number. Therefore, values between 12 and 60 bpm can be used to measure the quality of recovery. Increasingly higher values indicate very good cardiovascular capacity and good autonomic nervous system function; values close to 12 bpm may indicate a higher risk of cardiovascular disease or parasympathetic nervous system dysfunction [49,50]. The average HRR60 value found in the participants of the present study was 37 ± 11 bpm. This value is well above the minimum values mentioned earlier. In addition, a study by Carnethon et al. [51] found that participants who self-reported a high level of physical activity had a significantly higher HRR (but in this case measured after 2 min of exercise cessation) than participants in the lowest group (corresponding to the lowest level of physical activity). Thus, physical activity was associated with a faster HRR in a treadmill exercise test. Therefore, the participants in the current study seem to be consistent with their age group and active lifestyle [51].
The range of HRR variation (19 to 63 bpm of recovery over one minute) commonly found in these individuals was divided, and four categories were developed to provide a qualitative description of cardiovascular capacity in this population group (young adults). The cardiovascular capacity categorization, the reference VO2max values for the participants in the present study aged between 18 and 29 years, and the values of comparable categories proposed by McArdle et al. [52] are shown in Table 4. This finding may indicate that there is no difference between the VO2max values calculated by Equation (1) and other estimates. Using the StepTest4all, it has been observed that values below 25 are typically associated with a sedentary lifestyle and the presence of additional risk factors such as obesity and smoking, while values above 55 are typically found in individuals who lead a healthy lifestyle and engage in high levels of daily physical activity. Table 4 shows the VO2max values predicted by Equation (1) (from our study) and the values proposed by McArdle et al. [52] for similar categories. Similar values can also be found in a company of world-renowned body composition assessment company (Tanita: https://tanita.eu/blog/could-improving-your-vo2-max-be-the-secret-of-success (accessed on 28 July 2022)) [53].
The assessment of physical activity as a predictor of VO2max is consistent with previous research, such as the study conducted by Dyrstad et al. [25]. The aim of this study was to investigate how different levels of self-reported and objectively measured physical activity, including sedentary time, correlated with variations in VO2max. This study included a sample of 759 participants (366 women and 393 men) with a mean age of 48.5 years (SD of 14.4) who completed the cardiopulmonary exercise test 5–8 months after completing the IPAQ questionnaire. The article by Dyrstad et al. [25] examines the relationship between physical activity and cardiorespiratory fitness, both of which are inversely associated with disease and all-cause mortality. Their results indicate that individuals classified as highly active by the IPAQ had higher cardiorespiratory fitness than those who reported low levels of physical activity. In addition, meeting the physical activity recommendation of 150 min per week of daily moderate-intensity physical activity was associated with higher cardiorespiratory fitness. The study highlights the variation in cardiorespiratory fitness and underscores the central role of physical activity in maintaining good health and reducing the risk of disease and mortality. Indeed, our results showed that the PAlevel was retained as a significant predictor of VO2max. In comparison to the study of Bragada et al. [24], our modeling allowed us to increase the prediction output (R2 from 63% to 74%). This reinforces the importance of PAlevel in the assessment of cardiorespiratory capacity.
Because of its unique characteristics, the StepTest4all demonstrates adaptability to individuals with different physical abilities and varying somatic characteristics. While not the first step test to incorporate multiple characteristics in determining step height, this protocol refines this approach. This refined calculation allows for a primary adjustment that prevents the test from becoming too challenging or too easy. Further precision is achieved through careful control of the pace and its incremental adjustments throughout the test to ensure that the desired intensity of effort associated with 80% of HRmax (upper limit) is achieved within an appropriate time frame of 5 to 10 min for all participants. This updated protocol builds on the foundation laid by Bragada et al. [24], contributing advancements to the methodology and enhancing its effectiveness in assessing cardiovascular capacity among individuals with varying physical characteristics.
In the current study, age was excluded as a predictor of VO2max via stepwise regression modeling. This exclusion was influenced by the homogeneity of the sample, which consisted predominantly of young adults. It is plausible that in studies with a more diverse age range, age could become an important factor in the predictive equation for VO2max. Expanding the age spectrum in future investigations may shed light on the potential impact of age on the predictive accuracy of the model.
In addition to this, the use of step tests, coupled with the above-mentioned advantages, remains favorable due to their simplicity, minimal space requirements, and ability to be performed by individuals at home. As demonstrated on the StepTest4all Facebook page (https://www.facebook.com/StepTest4all, accessed on 28 July 2022) [54], the accessibility of the protocol enhances its practicality and convenience, making it an attractive option for widespread participation in cardiovascular fitness assessments.
The current study has several limitations that need to be considered. First, the research was conducted with young adults only. Therefore, further studies with a broader demographic representation are needed to generalize the findings to different age groups. Second, it is important to note that both VO2 and HRmax values were estimated rather than directly measured. However, these estimates were derived from the evolution of actual individual values of VO2max and HR, both at rest and at different intensity levels. It is important to emphasize that this estimation method is consistent with standard procedures commonly used in non-athletic participants or special populations where it is not advisable to subject individuals to maximal tests to exhaustion. Finally, the reliability of the test was not measured in this particular sample. Thus, further studies could address this issue. Despite these limitations, the findings of this study provide a foundation for future research efforts aimed at addressing these limitations and expanding the applicability of the StepTest4all protocol.
5. Conclusions
The StepTest4all was shown to be a suitable method for estimating cardiovascular capacity, expressed as VO2max, in young adults. The validation procedure showed a high degree of agreement between measured and estimated VO2. Additionally, it is possible to determine the qualitative level of cardiovascular capacity (PAlevel) from the HRR60, more specifically, poor: <25 bpm, moderate: 25 to 39 bpm, good: 40 to 55 bpm, and excellent: ≥55 bpm. This method is easy to use and accessible to everyone, so it can be used at home without the need for specialized supervision.
Author Contributions
Conceptualization, J.E.M. and J.A.B.; methodology, T.S., J.E.M. and J.A.B.; data curation, T.S. and J.E.M.; writing—original draft preparation, T.S., J.A.B. and J.E.M. The paper and data have not been published before, are not under consideration for publication elsewhere, and have been approved by all co-authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Portuguese Foundation for Science and Technology, I. P. (project UIDB/DTP/04045/2020).
Institutional Review Board Statement
All procedures were in accordance with the Declaration of Helsinki regarding human research, and the Polytechnic Ethics Board approved the research design (Nº 43/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request to the contact author.
Acknowledgments
The authors acknowledge the cooperation of all subjects who voluntarily participated in the collection procedures.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lee, D.; Artero, E.G.; Sui, X.; Blair, S.N. Mortality Trends in the General Population: The Importance of Cardiorespiratory Fitness. J. Psychopharmacol. 2010, 24, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Cole, C.R.; Blackstone, E.H.; Pashkow, F.J.; Snader, C.E.; Lauer, M.S. Heart-Rate Recovery Immediately after Exercise as a Predictor of Mortality. N. Engl. J. Med. 1999, 341, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.A.; Fleenor, B.S.; Kaminsky, L.A. The Influence of Change in Cardiorespiratory Fitness with Short-Term Exercise Training on Mortality Risk from The Ball State Adult Fitness Longitudinal Lifestyle Study. Mayo Clin. Proc. 2019, 94, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Giacomantonio, N.; Morrison, P.; Rasmussen, R.; MacKay-Lyons, M.J. Reliability and Validity of the 6-Minute Step Test for Clinical Assessment of Cardiorespiratory Fitness in People at Risk of Cardiovascular Disease. J. Strength Cond. Res. 2020, 34, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Harber, M.P.; Kaminsky, L.A.; Arena, R.; Blair, S.N.; Franklin, B.A.; Myers, J.; Ross, R. Impact of Cardiorespiratory Fitness on All-Cause and Disease-Specific Mortality: Advances Since 2009. Prog. Cardiovasc. Dis. 2017, 60, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S. Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and Women: A Meta-Analysis. Clin. Rev. 2009, 301, 2024. [Google Scholar] [CrossRef]
- Jae, S.Y.; Kurl, S.; Laukkanen, J.A.; Zaccardi, F.; Choi, Y.-H.; Fernhall, B.; Carnethon, M.; Franklin, B.A. Exercise Heart Rate Reserve and Recovery as Predictors of Incident Type 2 Diabetes. Am. J. Med. 2016, 129, 536.e7–536.e12. [Google Scholar] [CrossRef]
- Yu, T.Y.; Jee, J.H.; Bae, J.C.; Hong, W.-J.; Jin, S.-M.; Kim, J.H.; Lee, M.-K. Delayed Heart Rate Recovery after Exercise as a Risk Factor of Incident Type 2 Diabetes Mellitus after Adjusting for Glycometabolic Parameters in Men. Int. J. Cardiol. 2016, 221, 17–22. [Google Scholar] [CrossRef]
- Messinger-Rapport, B.; Pothier Snader, C.E.; Blackstone, E.H.; Yu, D.; Lauer, M.S. Value of Exercise Capacity and Heart Rate Recovery in Older People. J. Am. Geriatr. Soc. 2003, 51, 63–68. [Google Scholar] [CrossRef]
- Kurl, S.; Jae, S.Y.; Voutilainen, A.; Hagnäs, M.; Laukkanen, J.A. Exercise Heart Rate Reserve and Recovery as Risk Factors for Sudden Cardiac Death. Prog. Cardiovasc. Dis. 2021, 68, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Peçanha, T.; Bartels, R.; Brito, L.C.; Paula-Ribeiro, M.; Oliveira, R.S.; Goldberger, J.J. Methods of Assessment of the Post-Exercise Cardiac Autonomic Recovery: A Methodological Review. Int. J. Cardiol. 2017, 227, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Fecchio, R.Y.; Brito, L.; Leicht, A.S.; Forjaz, C.L.M.; Peçanha, T. Reproducibility of Post-Exercise Heart Rate Recovery Indices: A Systematic Review. Auton. Neurosci. 2019, 221, 102582. [Google Scholar] [CrossRef] [PubMed]
- De Abreu Camarda, S.R.; Tebexreni, A.S.; Páfaro, C.N.; Sasai, F.B.; Tambeiro, V.L.; Juliano, Y.; de Barros Neto, T.L. Comparison of Maximal Heart Rate Using the Prediction Equations Proposed by Karvonen and Tanaka. Arq. Bras. Cardiol. 2008, 91, 311–314. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Sun, Z.; Li, L.; Zuegel, M.; Steinacker, J.M.; Schumann, U. Heart Rate Recovery and Risk of Cardiovascular Events and All-Cause Mortality: A Meta-Analysis of Prospective Cohort Studies. J. Am. Heart Assoc. 2017, 6, e005505. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Li, X.; Zhang, Y.; Zhao, Z.; Zhao, Q.; Yan, L.; Duan, A.; Luo, Q.; Liu, Z. Heart Rate Recovery at 1 Min after Exercise Is a Marker of Disease Severity and Prognosis in Chronic Thromboembolic Pulmonary Hypertension. Respiration 2021, 101, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Petrella, R.J.; Koval, J.J.; Cunningham, D.A.; Paterson, D.H. A Self-Paced Step Test to Predict Aerobic Fitness in Older Adults in the Primary Care Clinic. J. Am. Geriatr. Soc. 2001, 49, 632–638. [Google Scholar] [CrossRef]
- Hughes, A.D.; Chaturvedi, N. Estimation of Maximal Oxygen Consumption and Heart Rate Recovery Using the Tecumseh Sub-Maximal Step Test and Their Relationship to Cardiovascular Risk Factors. Artery Res. 2017, 18, 29. [Google Scholar] [CrossRef]
- Pepera, G.; Panagiota, Z. Comparison of Heart Rate Response and Heart Rate Recovery after Step Test among Smoker and Non-Smoker Athletes. Afr. Health Sci. 2021, 21, 105–111. [Google Scholar] [CrossRef]
- Hansen, D.; Jacobs, N.; Bex, S.; D’Haene, G.; Dendale, P.; Claes, N. Are Fixed-Rate Step Tests Medically Safe for Assessing Physical Fitness? Eur. J. Appl. Physiol. 2011, 111, 2593–2599. [Google Scholar] [CrossRef]
- Gallagher, J.R.; Brouha, L.V. A Simple Method of Evaluating Fitness in Boys: The Step Test. Yale J. Biol. Med. 1943, 15, 769–779. [Google Scholar]
- Santo, A.S.; Golding, L.A. Predicting Maximum Oxygen Uptake from a Modified 3-Minute Step Test. Res. Q. Exerc. Sport 2003, 74, 110–115. [Google Scholar] [CrossRef]
- McArdle, W.D.; Katch, F.I.; Pechar, G.S.; Jacobson, L.; Ruck, S. Reliability and Interrelationships between Maximal Oxygen Intake, Physical Work Capacity and Step-Test Scores in College Women. Med. Sci. Sports 1972, 4, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Bragada, J.A.; Bartolomeu, R.F.; Rodrigues, P.M.; Magalhães, P.M.; Bragada, J.P.; Morais, J.E. Validation of StepTest4all for Assessing Cardiovascular Capacity in Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 11274. [Google Scholar] [CrossRef] [PubMed]
- Dyrstad, S.M.; Anderssen, S.A.; Edvardsen, E.; Hansen, B.H. Cardiorespiratory Fitness in Groups with Different Physical Activity Levels. Scand. J. Med. Sci. Sports 2016, 26, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.K.; Subramanian, S.K.; Radhakrishnan, K.; Rajendran, R.; Ravindran, B.S.; Arunachalam, V. Comparison of Structured and Unstructured Physical Activity Training on Predicted Vo2 max and Heart Rate Variability in Adolescents—A Randomized Control Trial. J. Basic Clin. Physiol. Pharmacol. 2017, 28, 225–238. [Google Scholar] [CrossRef] [PubMed]
- The International Physical Activity Questionnaire (IPAQ). Available online: https://sites.google.com/view/ipaq/score (accessed on 22 December 2023).
- Joseph, K.L.; Dagfinrud, H.; Christie, A.; Hagen, K.B.; Tveter, A.T. Criterion Validity of The International Physical Activity Questionnaire-Short Form (IPAQ-SF) for Use in Clinical Practice in Patients with Osteoarthritis. BMC Musculoskelet. Disord. 2021, 22, 232. [Google Scholar] [CrossRef] [PubMed]
- Tierney, M.; Fraser, A.; Kennedy, N. Criterion Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF) for Use in Patients with Rheumatoid Arthritis: Comparison with the SenseWear Armband. Physiotherapy 2015, 101, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Sjostrom, M.; Ainsworth, B.; Bauman, A.; Bull, F.; Hamilton-Craig, C.; Sallis, J. Guidelines for Data Processing Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. CiNii Articles 2005.
- Mackenzie, B. Harvard Step Test. Available online: https://www.brianmac.co.uk/havard.htm (accessed on 22 December 2023).
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Gibson, A.L.; Wagner, D.R.; Heyward, V.H. Advanced Fitness Assessment and Exercise Prescription, 8th ed.; Human Kinetics: Champaign, IL, USA, 2019; ISBN 978-1-4925-6134-7. [Google Scholar]
- Andersen, R.E.; Wadden, T.A. Validation of a Cycle Ergometry Equation for Predicting Steady-Rate Vo2 in Obese Women. Med. Sci. Sports Exerc. 1995, 27, 1457. [Google Scholar] [CrossRef] [PubMed]
- Jamnick, N.A.; By, S.; Pettitt, C.D.; Pettitt, R.W. Comparison of the YMCA and a Custom Submaximal Exercise Test for Determining Vo2 max. Med. Sci. Sports Exerc. 2016, 48, 254. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.J.L.; Ferrar, K.E.; Smith, A.E.; Parfitt, G.; Eston, R.G. A Systematic Review of Methods to Predict Maximal Oxygen Uptake from Submaximal, Open Circuit Spirometry in Healthy Adults. J. Sci. Med. Sport 2015, 18, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.; Davison, K.; Parfitt, G.; Eston, R. Validity of a Perceptually-Regulated Step Test Protocol for Assessing Cardiorespiratory Fitness in Healthy Adults. Eur. J. Appl. Physiol. 2016, 116, 2337–2344. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D. Statistical Methods for Assessing Agreement Between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2023; ISBN 978-1-975197-09-4. [Google Scholar]
- Arena, R.; Guazzi, M.; Myers, J.; Peberdy, M.A. Prognostic Value of Heart Rate Recovery in Patients with Heart Failure. Am. Heart J. 2006, 151, 851.e7–851.e13. [Google Scholar] [CrossRef]
- Vivekananthan, D.P.; Blackstone, E.H.; Pothier, C.E.; Lauer, M.S. Heart Rate Recovery after Exercise Is a Predictor of Mortality, Independent of the Angiographic Severity of Coronary Disease. J. Am. Coll. Cardiol. 2003, 42, 831–838. [Google Scholar] [CrossRef]
- Okutucu, S.; Karakulak, U.N.; Aytemir, K.; Oto, A. Heart Rate Recovery: A Practical Clinical Indicator of Abnormal Cardiac Autonomic Function. Expert Rev. Cardiovasc. Ther. 2011, 9, 1417–1430. [Google Scholar] [CrossRef] [PubMed]
- Van Ravenswaaij-Arts, C.M.A.; Kollee, L.A.A.; Hopman, J.C.W.; Stoelinga, G.B.A.; van Geijn, H.P. Heart Rate Variability. Ann. Intern. Med. 1993, 118, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Latchman, P.L.; Yang, Q.; Kong, L.; Zhang, H.; Sebagisha, J.; Meersman, R.E.D. Heart Rate Recovery, Central Systolic Pressure, and Augmentation Index in Young Healthy Individuals. Vasc. Health Risk Manag. 2022, 18, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, Z.; Lim, Y.Z. A Comparison of Low and High Dose of Moderate Intensity Aerobic Exercise on Heart Rate Recovery of the Sedentary Adults: A Pragmatic Randomized Controlled Trial. J. Sports Med. Phys. Fit. 2023, 63, 310–318. [Google Scholar] [CrossRef]
- Adabag, S.; Pierpont, G.L. Exercise Heart Rate Recovery: Analysis of Methods and Call for Standards. Heart 2013, 99, 1711–1712. [Google Scholar] [CrossRef]
- Gupta, M.; Bansal, V.; Chhabra, S.K. Abnormal Heart Rate Recovery and Chronotropic Incompetence on Exercise in Chronic Obstructive Pulmonary Disease. Chronic Respir. Dis. 2013, 10, 117–126. [Google Scholar] [CrossRef]
- Carnethon, M.R.; Jacobs, D.R.; Sidney, S.; Sternfeld, B.; Gidding, S.S.; Shoushtari, C.; Liu, K. A Longitudinal Study of Physical Activity and Heart Rate Recovery: CARDIA, 1987–1993. Med. Sci. Sports Exerc. 2005, 37, 606–612. [Google Scholar] [CrossRef]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Fisiologia do Exercício: Energia, Nutrição e Desempenho Humano, 6th ed.; Guanabara-Koogan: Rio de Janeiro, Brazil, 2008. [Google Scholar]
- TANITA. Improving Your Vo2 Max: Definition, Tables & Norms|Tanita.Eu. Available online: https://tanita.eu/blog/could-improving-your-vo2-max-be-the-secret-of-success (accessed on 22 December 2023).
- StepTest4all. Available online: https://www.facebook.com/StepTest4all (accessed on 22 December 2023).
Figure 1.
StepTest4all infogram.

Figure 2.
Visual representation of StepTest4all.

Figure 3.
Bland–Altman plots of the measured and predicted VO2max. The y-axes refer to the difference between the measured and predicted VO2max [mL·kg−1·min−1]. The x-axes refer to the average between the measured and predicted VO2max [mL·kg−1·min−1].
Figure 3.
Bland–Altman plots of the measured and predicted VO2max. The y-axes refer to the difference between the measured and predicted VO2max [mL·kg−1·min−1]. The x-axes refer to the average between the measured and predicted VO2max [mL·kg−1·min−1].


{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of the participants.
| Equation Group | Validation Group | |||||
|---|---|---|---|---|---|---|
| Mean ± 1 SD | Mean ± 1 SD | |||||
| Women (n = 17) | Men (n = 13) | Total | Women (n = 10) | Men (n = 29) | Total | |
| Age [years] | 20.8 ± 2.3 | 21.6 ± 2.8 | 21.7 ± 2.4 | 23.1 ± 4.8 | 21.7 ± 3.6 | 22.1 ± 3.9 |
| Body mass [kg] | 57.0 ± 6.8 | 71.6 ± 7.0 | 68.7 ± 11.5 | 74.6 ± 18.2 | 72.2 ± 7.6 | 71.8 ± 11.0 |
| Height [m] | 1.61 ± 0.04 | 1.77 ± 0.07 | 1.72 ± 0.09 | 1.68 ± 0.07 | 1.77 ± 0.07 | 1.74 ± 0.08 |
| BMI [kg/m2] | 22.0 ± 3.1 | 22.8 ± 1.6 | 23.3 ± 3.7 | 26.7 ± 6.9 | 23.2 ± 2.3 | 24.1 ± 4.2 |
| HRR60 [bpm] | 36 ± 9 | 36 ± 11 | 36 ± 10 | 37 ± 10 | 38 ± 11 | 38 ± 11 |
| VO2max [mL·kg−1·min−1] | 32.86 ± 4.95 | 45.03 ± 8.19 | 39.83 ± 9.38 | 32.95 ± 9.20 | 43.97 ± 8.19 | 41.14 ± 9.65 |
| HRRrest [bpm] | 83 ± 11 | 67 ± 11 | 76 ± 13 | 78 ± 12 | 69 ± 11 | 71 ± 12 |
| VO2rest [mL·kg−1·min−1] | 3.53 ± 0.56 | 3.97 ± 0.67 | 3.73 ± 0.64 | 3.17 ± 0.92 | 3.44 ± 0.61 | 3.37 ± 0.70 |
Note: Total—both sexes summed together.
Table 2.
Physical activity levels (PAlevels) of the participants.
| Equation Group | Validation Group | |||
|---|---|---|---|---|
| Women (n = 17) | Men (n = 13) | Women (n = 10) | Men (n = 29) | |
| PAlevel | ||||
| 1 | 8 | 0 | 7 | 3 |
| 2 | 6 | 7 | 2 | 17 |
| 3 | 3 | 6 | 1 | 9 |
Note: PAlevel—physical activity level.
Table 3.
Paired samples t-test comparison between measured and estimated VO2max in the validation group. The effect size index (Cohen’s d) is also shown.
Table 3.
Paired samples t-test comparison between measured and estimated VO2max in the validation group. The effect size index (Cohen’s d) is also shown.
| Measured VO2max [mL·kg−1·min−1] | Estimated VO2max [mL·kg−1·min−1] | |||
|---|---|---|---|---|
| Mean ± 1 SD | Mean ± 1 SD | Mean Difference (95% CI) | t-Test (p Value) | d [Descriptor] |
| 41.14 ± 9.65 | 41.48 ± 6.94 | −0.345 (−2.767 to 2.076) | −0.289 (0.774) | 0.04 [trivial] |
Note: VO2max: maximal oxygen uptake.
Table 4.
Cardiovascular capacity (CVC) classification based on HRR60 and corresponding HRR cut-off values.
Table 4.
Cardiovascular capacity (CVC) classification based on HRR60 and corresponding HRR cut-off values.
| CVC Classification | HRR60 | Men | Women | ||
|---|---|---|---|---|---|
| VO2max | McArdle et al., 2003 [52] | VO2max | McArdle et al., 2003 [52] | ||
| Poor | <25 | <40 | <36.5 | <28 | <29 |
| Moderate | 25–39 | 42–44.2 | 36.5–42.4 | 28–32.2 | 29–32 |
| Good | 40–54 | 44.3–49 | 42.5–46.4 | 32.3–36.9 | 33–36 |
| Excellent | ≥55 | ≥49 | ≥46.5 | ≥37 | ≥37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sampaio, T.; Morais, J.E.; Bragada, J.A. StepTest4all: Improving the Prediction of Cardiovascular Capacity Assessment in Young Adults. J. Funct. Morphol. Kinesiol. 2024, 9, 30. https://doi.org/10.3390/jfmk9010030
AMA Style
Sampaio T, Morais JE, Bragada JA. StepTest4all: Improving the Prediction of Cardiovascular Capacity Assessment in Young Adults. Journal of Functional Morphology and Kinesiology. 2024; 9(1):30. https://doi.org/10.3390/jfmk9010030
Chicago/Turabian StyleSampaio, Tatiana, Jorge E. Morais, and José A. Bragada. 2024. "StepTest4all: Improving the Prediction of Cardiovascular Capacity Assessment in Young Adults" Journal of Functional Morphology and Kinesiology 9, no. 1: 30. https://doi.org/10.3390/jfmk9010030