
Does Radial Extracorporeal Shockwave Therapy Applied to the Achilles Tendon Influence Ankle Functionality?
 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
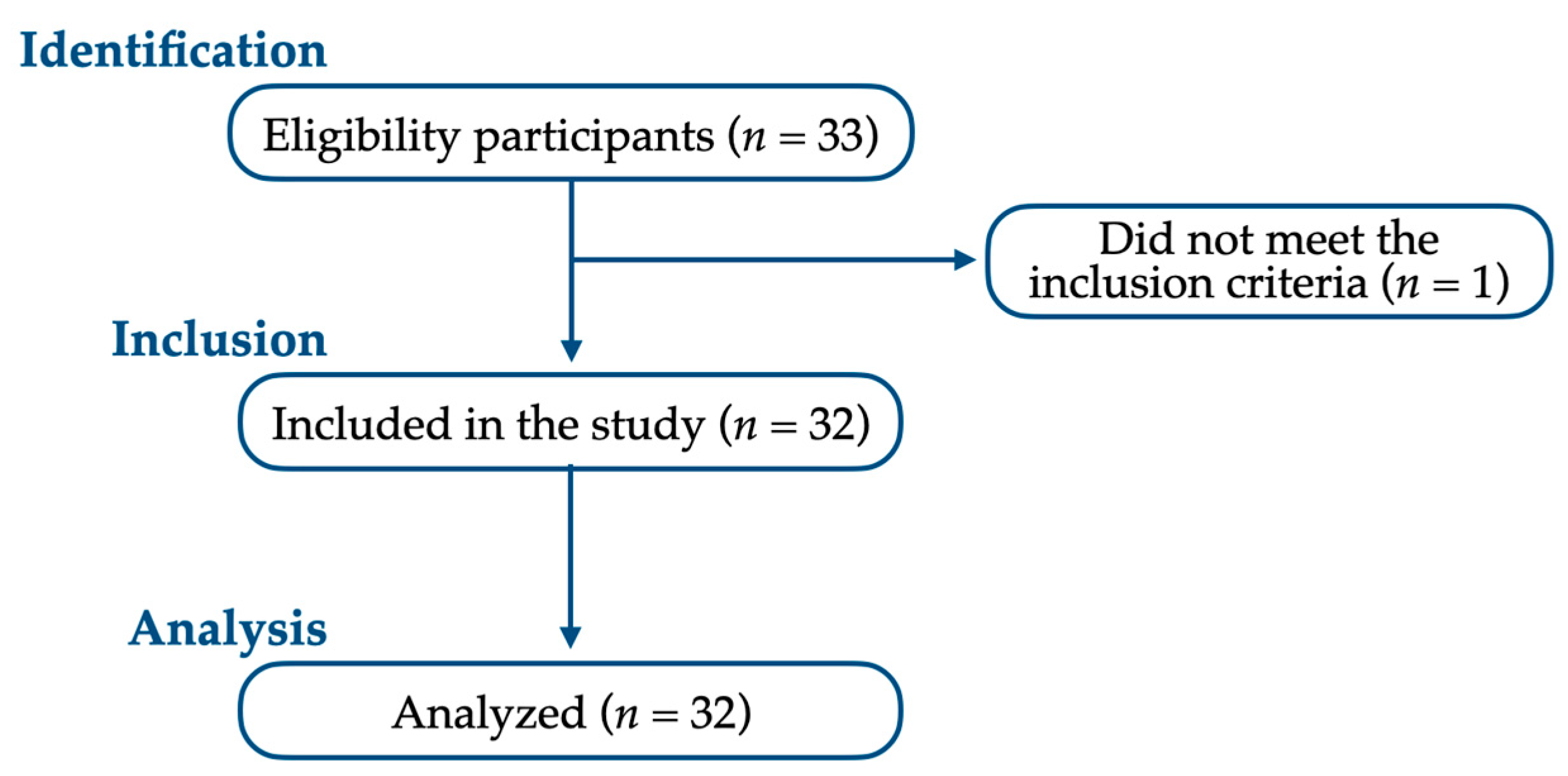
2.2. Participants
2.2.1. Inclusion Criteria
- Individuals with ankle-related pain scores of 0–2 on the Numeric Pain Rating Scale (NPRS).
- Individuals with no functional impairment in the ankle.
2.2.2. Exclusion Criteria
- Individuals who underwent surgical procedures, such as ankle joint arthrodesis.
- Individuals showing signs of functional impairment in ankle functionality.
- Individuals with ankle-related pain rated >3 on the NPRS.
- Individuals with acute ankle fractures.
2.3. Interventions
2.3.1. Radial Extracorporeal Shockwave Therapy
2.3.2. Sham Extracorporeal Shockwave Therapy
2.4. Outcome Measures
2.4.1. Primary Outcome Measure
2.4.2. Secondary Outcome Measures
- Achilles tendon stiffness
- 2.
- Ankle joint range of motion
- 3.
- Heel-rise
2.5. Ethics and Dissemination
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Enrolled Participants
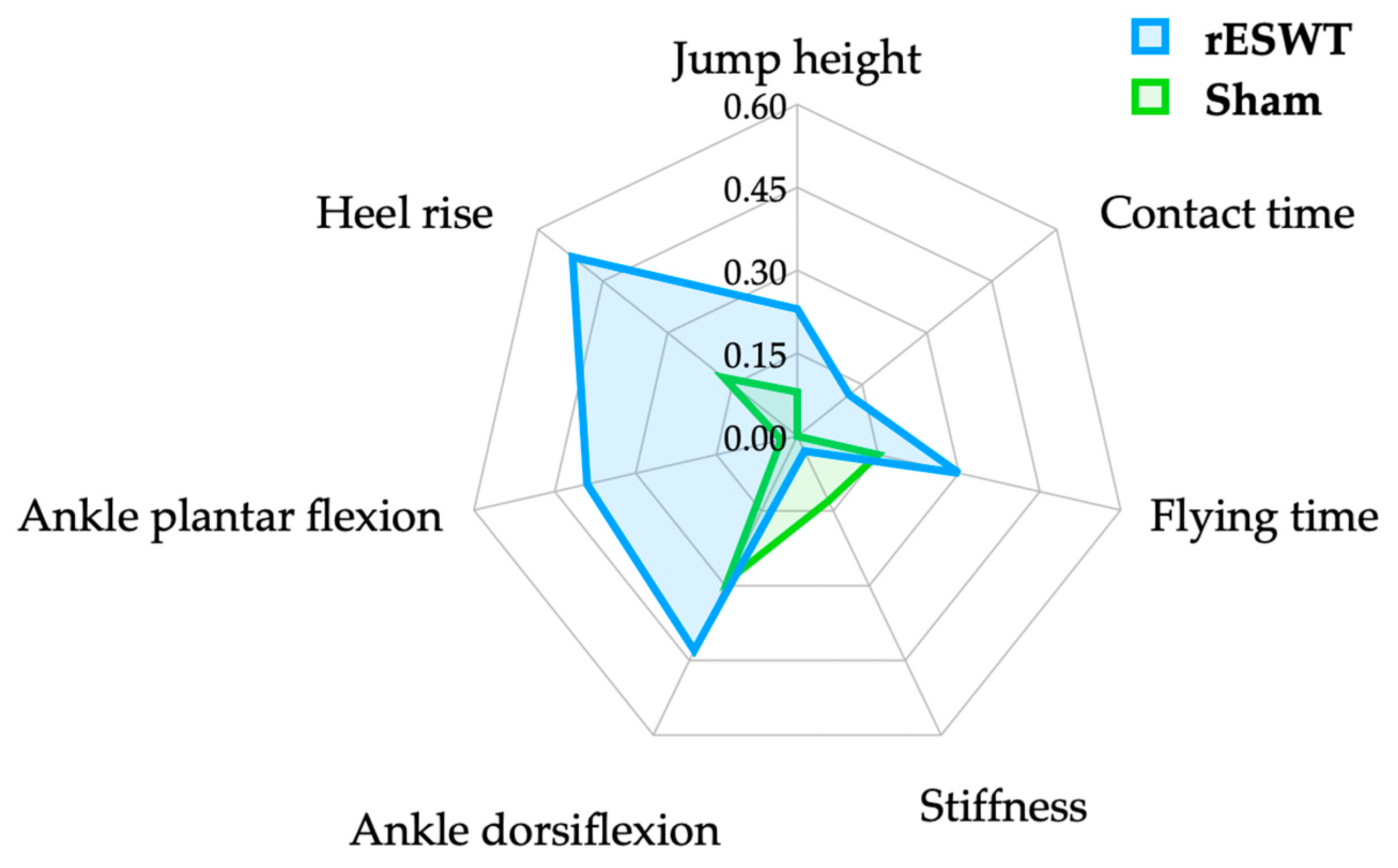
3.2. Jump Height Comparison
3.3. Comparison of Achilles Tendon Stiffness
3.4. Comparison of Ankle Joint Range of Motion
3.5. Heel-Rise Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Von Rickenbach, K.J.; Borgstrom, H.; Tenforde, A.; Borg-Stein, J.; McInnis, K.C. Achilles Tendinopathy: Evaluation, Rehabilitation, and Prevention. Curr. Sports Med. Rep. 2021, 20, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Aicale, R.; Oliviero, A.; Maffulli, N. Management of Achilles and patellar tendinopathy: What we know, what we can do. J. Foot Ankle Res. 2020, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br. J. Sports Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Elias, D.A.; Carne, A.; Bethapudi, S.; Engebretsen, L.; Budgett, R.; O’Connor, P. Imaging of plantar fascia and Achilles injuries undertaken at the London 2012 Olympics. Skelet. Radiol. 2013, 42, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Heiss, R.; Guermazi, A.; Jarraya, M.; Engebretsen, L.; Hotfiel, T.; Parva, P.; Roemer, F.W. Prevalence of MRI-detected ankle injuries in athletes in the Rio de Janeiro 2016 Summer Olympics. Acad. Radiol. 2019, 26, 1605–1617. [Google Scholar] [CrossRef] [PubMed]
- Alfredson, H.; Lorentzon, R. Chronic Achilles tendinosis: Recommendations for treatment and prevention. Sports Med. 2000, 29, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Paavola, M.; Kannus, P.; Järvinen, T.A.; Khan, K.; Józsa, L.; Järvinen, M. Achilles tendinopathy. J. Bone Jt. Surg. Am. 2002, 84, 2062–2076. [Google Scholar] [CrossRef] [PubMed]
- Kader, D.; Saxena, A.; Movin, T.; Maffulli, N. Achilles tendinopathy: Some aspects of basic science and clinical management. Br J. Sports Med. 2002, 36, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Alfredson, H. The chronic painful Achilles and patellar tendon: Research on basic biology and treatment. Scand. J. Med. Sci. Sports 2005, 15, 252–259. [Google Scholar] [CrossRef]
- Alfredson, H. Chronic midportion Achilles tendinopathy: An update on research and treatment. Clin. Sports Med. 2003, 22, 727–741. [Google Scholar] [CrossRef]
- Alfredson, H.; Ohberg, L. Sclerosing injections to areas of neo-vascularisation reduce pain in chronic Achilles tendinopathy: A double-blind randomised controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Dunn, W.R.; Thomson, A.B. Nonoperative treatment of midportion Achilles tendinopathy: A systematic review. Clin. J. Sport Med. 2009, 19, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Lichtwark, G.; Bougoulias, K.; Wilson, A. Muscle fascicle and series elastic element length changes along the length of the human gastrocnemius during walking and running. J. Biomech. 2007, 40, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Doral, M.N.; Alam, M.; Bozkurt, M.; Turhan, E.; Atay, O.A.; Dönmez, G.; Maffulli, N. Functional anatomy of the Achilles tendon. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Punnoose, A.; Norrish, A.; Pak, K. Extracorporeal shock wave therapy for achilles and patellar tendinopathy: Meta-analysis and a systematic review of the literature. J. Physiother. Phys. Rehabil. 2017, 2, 1000124. [Google Scholar] [CrossRef]
- Xu, D.; Zhou, H.; Quan, W.; Gusztav, F.; Wang, M.; Baker, J.S.; Gu, Y. Accurately and effectively predict the ACL force: Utilizing biomechanical landing pattern before and after-fatigue. Comput. Methods Programs Biomed. 2023, 241, 107761. [Google Scholar] [CrossRef] [PubMed]
- Stania, M.; Juras, G.; Chmielewska, D.; Polak, A.; Kucio, C.; Król, P. Extracorporeal Shock Wave Therapy for Achilles Tendinopathy. BioMed Res. Int. 2019, 2019, 3086910. [Google Scholar] [CrossRef] [PubMed]
- Walewicz, K.; Taradaj, J.; Rajfur, K.; Ptaszkowski, K.; Kuszewski, M.T.; Sopel, M.; Dymarek, R. The effectiveness of radial extracorporeal shock wave therapy in patients with chronic low back pain: A prospective, randomized, single-blinded pilot study. Clin. Interv. Aging 2019, 14, 1859. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Choi, W.; Jung, J.; Park, S.; Joo, Y.; Lee, S.; Lee, S. Efficacy of radial extracorporeal shockwave therapy in rehabilitation following arthroscopic rotator cuff repair: A STROBE compliant study. Medicine 2022, 101, e30053. [Google Scholar] [CrossRef]
- Prudêncio, D.A.; Serafim, T.T.; Marinho Mateus Lopes, A.P.S.R.; Maffulli, N.; Okubo, R. Questionnaires and scales for assessment of ankle function: A systematic review of instruments translated and validated for Brazilian Portuguese. Disabil. Rehabil. 2019, 43, 309–316. [Google Scholar] [CrossRef]
- In, T.-S.; Jung, J.-H.; Kim, K.; Jung, K.-S.; Cho, H.-Y. The reliability and validity of the Korean version of the foot function index for patients with foot complaints. J. Phys. Ther. Sci. 2017, 29, 53–56. [Google Scholar] [CrossRef]
- Huh, J.-W.; Eun, I.-S.; Ko, Y.-C.; Park, M.-J.; Hwang, K.-M.; Park, S.-H.; Park, T.-h.; Park, J.-h. Reliability and validity of the Korean version of the Foot Function Index. J. Foot Ankle Surg. 2016, 55, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Dreisilker, U. Enthesiopathies II: Radial Shock Wave Treatment of Tendinopathies, 1st ed.; Level10 Buchverlag: Heilbronn, Germany, 2015. [Google Scholar]
- Walewicz, K.; Taradaj, J.; Dobrzyński, M.; Sopel, M.; Kowal, M.; Ptaszkowski, K.; Dymarek, R. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. J. Clin. Med. 2020, 9, 568. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, L.; Yang, J. Instant analgesic effect of radial extracorporeal shock wave therapy on primary dysmenorrhoea according to functional magnetic resonance imaging: Study protocol for a randomised placebo-controlled trial. Trials 2020, 21, 164. [Google Scholar] [CrossRef] [PubMed]
- Jidovtseff, B.; Apolloni, J.; Harris, N.; Cronin, J. Modeling relationships between jump height, ground contact time, reactivity and stiffness. In Proceedings of the Abstract Book of 8th International Conference on Strength Training, Oslo, Norway, 24–28 October 2012. [Google Scholar]
- Attia, A.; Dhahbi, W.; Chaouachi, A.; Padulo, J.; Wong, D.; Chamari, K. Measurement errors when estimating the vertical jump height with flight time using photocell devices: The example of Optojump. Biol. Sport 2017, 34, 63. [Google Scholar] [CrossRef] [PubMed]
- Glatthorn, J.F.; Gouge, S.; Nussbaumer, S.; Stauffacher, S.; Impellizzeri, F.M.; Maffiuletti, N.A. Validity and reliability of Optojump photoelectric cells for estimating vertical jump height. J. Strength Cond. Res. 2011, 25, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Sánchez, A.; Abián, P.; Sánchez-Infante, J.; Esteban-Gacía, P.; Jiménez, F.; Abián-Vicén, J. Objective Assessment of Regional Stiffness in Vastus Lateralis with Different Measurement Methods: A Reliability Study. Sensors 2021, 21, 3213. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-w. Effects of McKenzie exercise on the functional recovery and forward head posture of choronic neck pain patients. J. Korean Soc. Phys. Med. 2006, 1, 93–108. [Google Scholar]
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry; FA Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Mullaney, M.J.; McHugh, M.P.; Johnson, C.P.; Tyler, T.F. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother Theory Pr. 2010, 26, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Carmont, M.R.; Zellers, J.A.; Brorsson, A.; Nilsson-Helander, K.; Karlsson, J.; Grävare Silbernagel, K. Age and Tightness of Repair Are Predictors of Heel-Rise Height After Achilles Tendon Rupture. Orthop. J. Sports Med. 2020, 8, 2325967120909556. [Google Scholar] [CrossRef]
- Zellers, J.A.; Marmon, A.R.; Ebrahimi, A.; Silbernagel, K.G. Lower Extremity Work Along with Triceps Surae Structure and Activation Is Altered with Jumping after Achilles Tendon Repair. J. Orthop. Res. 2019, 37, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Shih, K.-S.; Chen, P.-Y.; Yeh, W.-L.; Ma, H.-L.; Farn, C.-J.; Hou, C.-H.; Peng, W.-C.; Wang, H.-K. Modified Ankle Joint Neuromechanics during One-Legged Heel Raise Test after an Achilles Rupture and Its Associations with Jumping. Appl. Sci. 2021, 11, 2227. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol Bull 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Akınoğlu, B.; Köse, N. A comparison of the acute effects of radial extracorporeal shockwave therapy, ultrasound therapy, and exercise therapy in plantar fasciitis. J. Exerc.Rehabil. 2018, 14, 306–312. [Google Scholar] [CrossRef]
- Marusiak, J.; Kisiel-Sajewicz, K.; Jaskólska, A.; Jaskólski, A. Higher muscle passive stiffness in Parkinson’s disease patients than in controls measured by myotonometry. Arch. Phys. Med. Rehabil. 2010, 91, 800–802. [Google Scholar] [CrossRef] [PubMed]
- Zellers, J.A.; van Ostrand, K.; Silbernagel, K.G. Calf endurance and Achilles tendon structure in classical ballet dancers. J. Danc. Med. Sci. 2017, 21, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, A.; Nakhostin Roohi, B. Effect of extracorporeal shockwave therapy versus stretching in the treatment of athletes with chronic plantar fasciitis. Phys. Treat. 2019, 9, 117–124. [Google Scholar] [CrossRef]
- Oleksy, Ł.; Mika, A.; Kuchciak, M.; Bril, G.; Kielnar, R.; Adamska, O.; Wolański, P.; Deszczyński, M. Does Restricted Ankle Joint Mobility Influence Hamstring Muscle Strength, Work and Power in Football Players after ACL Reconstruction and Non-Injured Players? J. Clin. Med. 2023, 12, 6330. [Google Scholar] [CrossRef]
- Radinmehr, H.; Nakhostin Ansari, N.; Naghdi, S.; Olyaei, G.; Tabatabaei, A. Effects of one session radial extracorporeal shockwave therapy on post-stroke plantarflexor spasticity: A single-blind clinical trial. Disabil. Rehabil. 2017, 39, 483–490. [Google Scholar] [CrossRef]
- Fan, T.; Zhou, X.; He, P.; Zhan, X.; Zheng, P.; Chen, R.; Li, R.; Li, R.; Wei, M.; Zhang, X.; et al. Effects of Radial Extracorporeal Shock Wave Therapy on Flexor Spasticity of the Upper Limb in Post-stroke Patients: Study Protocol for a Randomized Controlled Trial. Front. Neurol. 2021, 12, 712512. [Google Scholar] [CrossRef]
- Lee, K.W.; Bae, J.-Y.; Ho, B.C.; Kim, J.H.; Seo, D.-K. Immediate weightbearing and ankle motion exercise after acute Achilles tendon rupture repair. J. Foot Ankle Surg. 2022, 61, 604–608. [Google Scholar]



{kind=link}
{kind=link}
| Mean ± Standard Deviation | |
|---|---|
| Sex (male/female) | 11/21 |
| Age (years) | 28.77 ± 5.45 |
| Height (cm) | 167.77 ± 7.35 |
| Weight (kg) | 61.89 ± 10.32 |
| rESWT | Sham | Change ‡ | ||
|---|---|---|---|---|
| Jump height a (cm) | Pre-test | 7.33 ± 4.09 | 8.13 ± 4.11 | |
| Post-test | 8.32 ± 4.40 | 8.46 ± 4.60 | −0.14 (−0.61, 0.32) † | |
| Change ‡ | 0.23 (0.61, 1.37) *** | 0.08 (−0.11, 1.28) | 0.55 (0.68, 1.32) * | |
| Contact time b (ms) | Pre-test | 0.47 ± 0.17 | 0.43 ± 0.14 | |
| Post-test | 0.45 ± 0.17 | 0.43 ± 0.14 | 0.01 (−0.01, 0.04) † | |
| Change ‡ | 0.12 (−0.05, 0.01) | 0.00 (−0.02, 0.02) | 0.26 (−0.02, 0.01) | |
| Flying time a (ms) | Pre-test | 0.21 ± 0.07 | 0.23 ± 0.06 | |
| Post-test | 0.23 ± 0.07 | 0.24 ± 0.07 | 0.00 (−0.01, 0.00) † | |
| Change ‡ | 0.30 (0.01, 0.03) *** | 0.15 (0.00, 0.02) | 0.48 (0.01, 0.02) * | |
| Stiffness a (N/m) | Pre-test | 974.72 ± 199.44 | 963.25 ± 188.40 | |
| Post-test | 981.94 ± 270.99 | 992.81 ± 268.34 | −10.88 (−81.35, 59.60) † | |
| Change ‡ | 0.03 (−52.48, 66.92) | 0.13 (−27.06, 86.18) | 0.13 (−25.06, 58.49) | |
| Ankle dorsiflexion b (°) | Pre-test | 12.78 ± 7.79 | 11.56 ± 6.81 | |
| Post-test | 16.03 ± 7.33 | 13.38 ± 5.79 | 2.66 (0.90, 4.41) † | |
| Change ‡ | 0.43 (1.84, 4.66) *** | 0.29 (0.30, 3.32) * | 0.34 (1.46, 3.66) | |
| Ankle plantar flexion b (°) | Pre-test | 59.59 ± 8.86 | 62.75 ± 10.59 | |
| Post-test | 63.78 ± 12.23 | 62.41 ± 10.24 | 1.38 (−1.23, 3.98) † | |
| Change ‡ | 0.39 (1.23, 7.15) * | 0.03 (−3.14, 2.46) | 0.54 (4.40, 8.53) * | |
| Heel-rise a (cm) | Pre-test | 12.01 ± 1.33 | 12.03 ± 1.52 | |
| Post-test | 12.72 ± 1.39 | 12.28 ± 1.36 | 0.44 (0.20, 0.69) † | |
| Change ‡ | 0.52 (0.50, 0.92) *** | 0.17 (0.02, 0.48) * | 0.73 (0.46, 0.79) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joo, Y.; Choi, W.; Jung, J.; Kim, H.; Park, S.; Lee, S.; Lee, S. Does Radial Extracorporeal Shockwave Therapy Applied to the Achilles Tendon Influence Ankle Functionality? J. Funct. Morphol. Kinesiol. 2024, 9, 67. https://doi.org/10.3390/jfmk9020067
Joo Y, Choi W, Jung J, Kim H, Park S, Lee S, Lee S. Does Radial Extracorporeal Shockwave Therapy Applied to the Achilles Tendon Influence Ankle Functionality? Journal of Functional Morphology and Kinesiology. 2024; 9(2):67. https://doi.org/10.3390/jfmk9020067
Chicago/Turabian StyleJoo, Younglan, Wonjae Choi, Jihye Jung, Hyunjoong Kim, Sungeon Park, Sangbong Lee, and Seungwon Lee. 2024. "Does Radial Extracorporeal Shockwave Therapy Applied to the Achilles Tendon Influence Ankle Functionality?" Journal of Functional Morphology and Kinesiology 9, no. 2: 67. https://doi.org/10.3390/jfmk9020067