
A Novel Framework on Security and Energy Enhancement Based on Internet of Medical Things for Healthcare 5.0


 ,
,  ,
,
Abstract
:1. Introduction
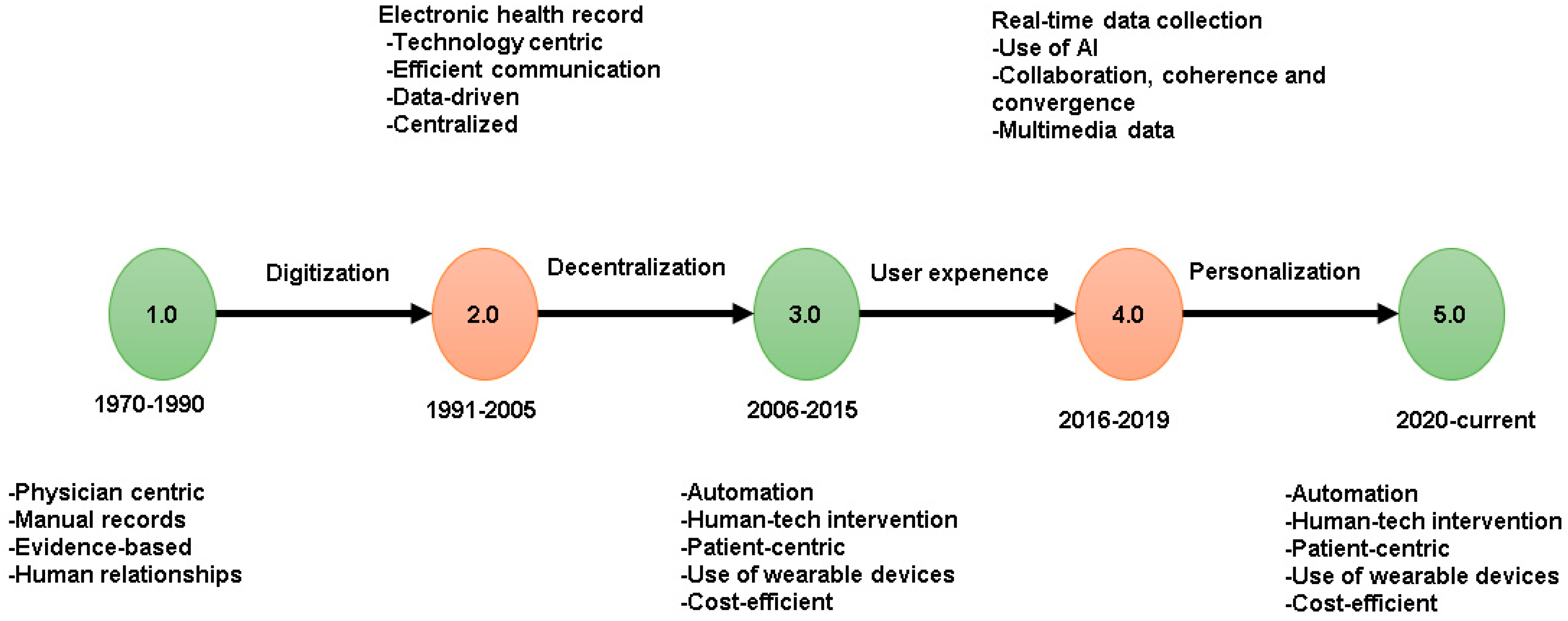
1.1. Historical Perspective on Healthcare’s Technological Development from Version 1.0 to 5.0
1.2. Contributions of the Study
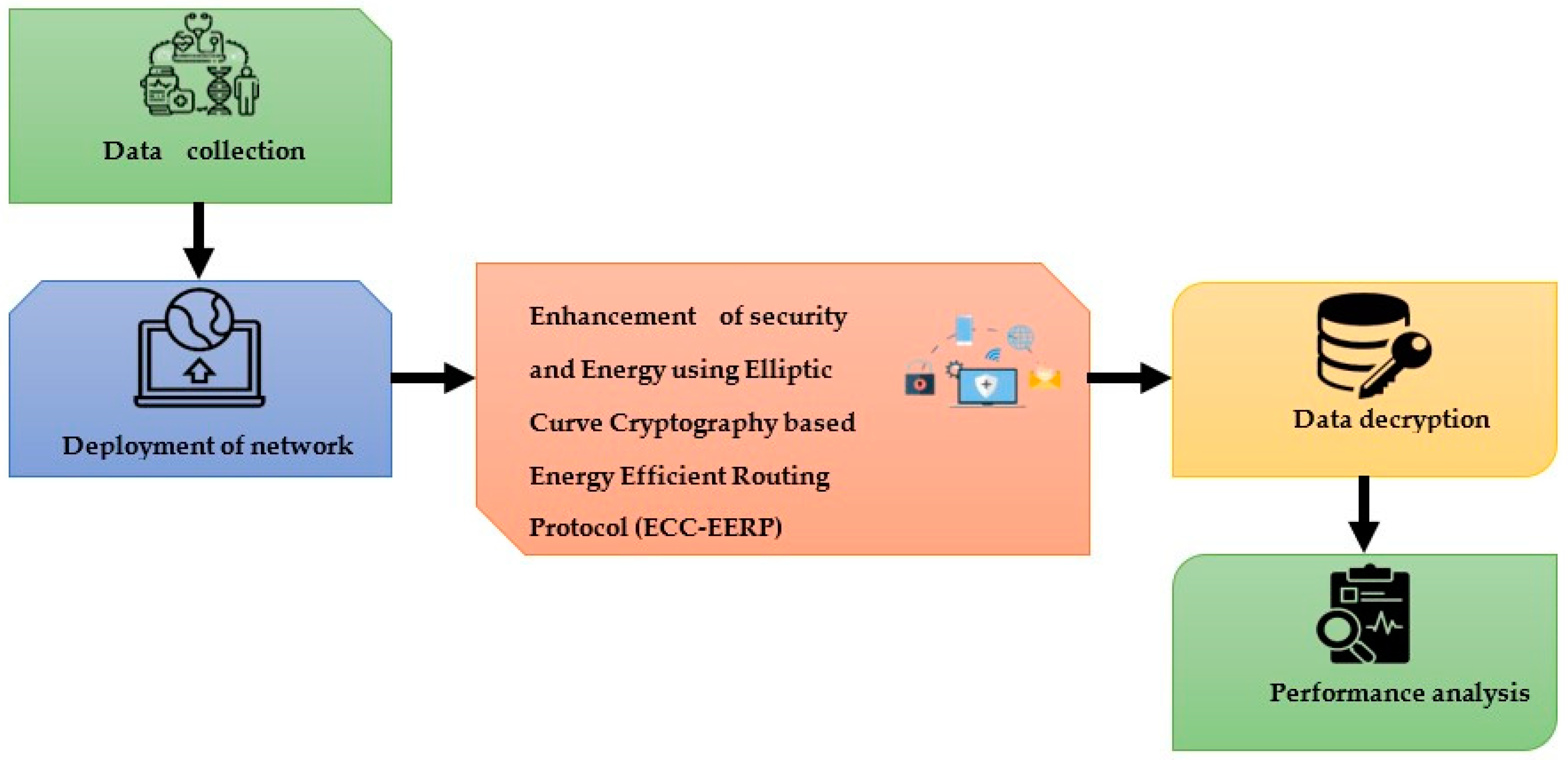
- Initially, the data were collected and stored in a network.
- Next, an elliptic curve cryptography-based energy-efficient routing protocol (ECC-EERP) was developed for the enhancement of security and energy in IoT healthcare 5.0.
- Finally, the performance of the system was analyzed.
2. Literature
Problem Statement
3. Proposed Method
3.1. Data Collection
3.2. Elliptic Curve Cryptography (ECC)-Based Energy-Efficient Routing Protocol (EERP)
| Algorithm 1: Encryption procedure |
| Divide the text into 93-bit units Generate the 186-bit sequence Split into two equal parts, and , 88 bits each Determine the number of 1s in every byte of , …, ] as well as the number of 1s in every one of the 11 bits of in for do , where Perm is the permutation function , where Con is the concatenation function end for Return the ciphertext , where is the ciphertext of |
4. Performance Analysis
- Simulation Details
4.1. Security
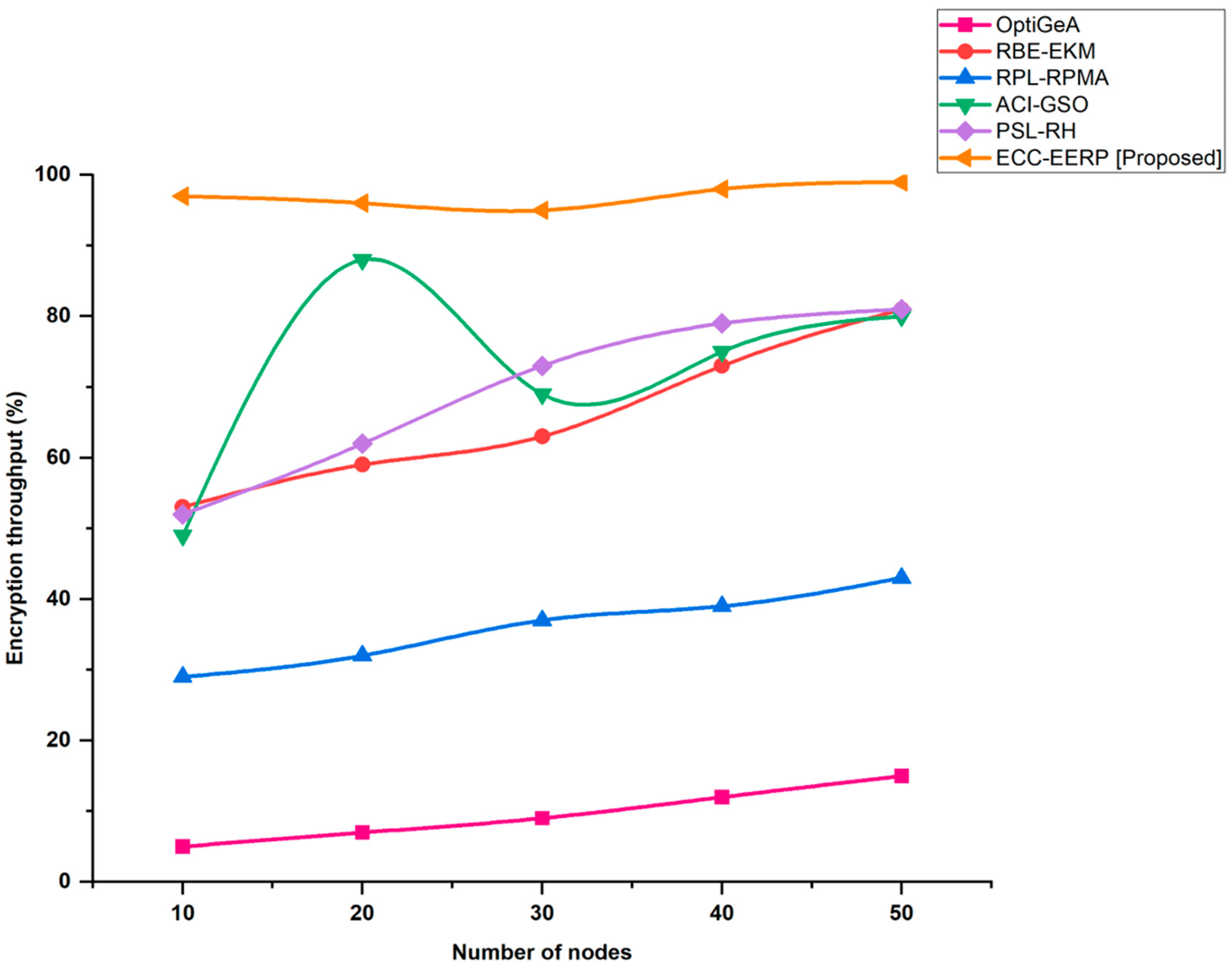
4.2. Encryption Throughput
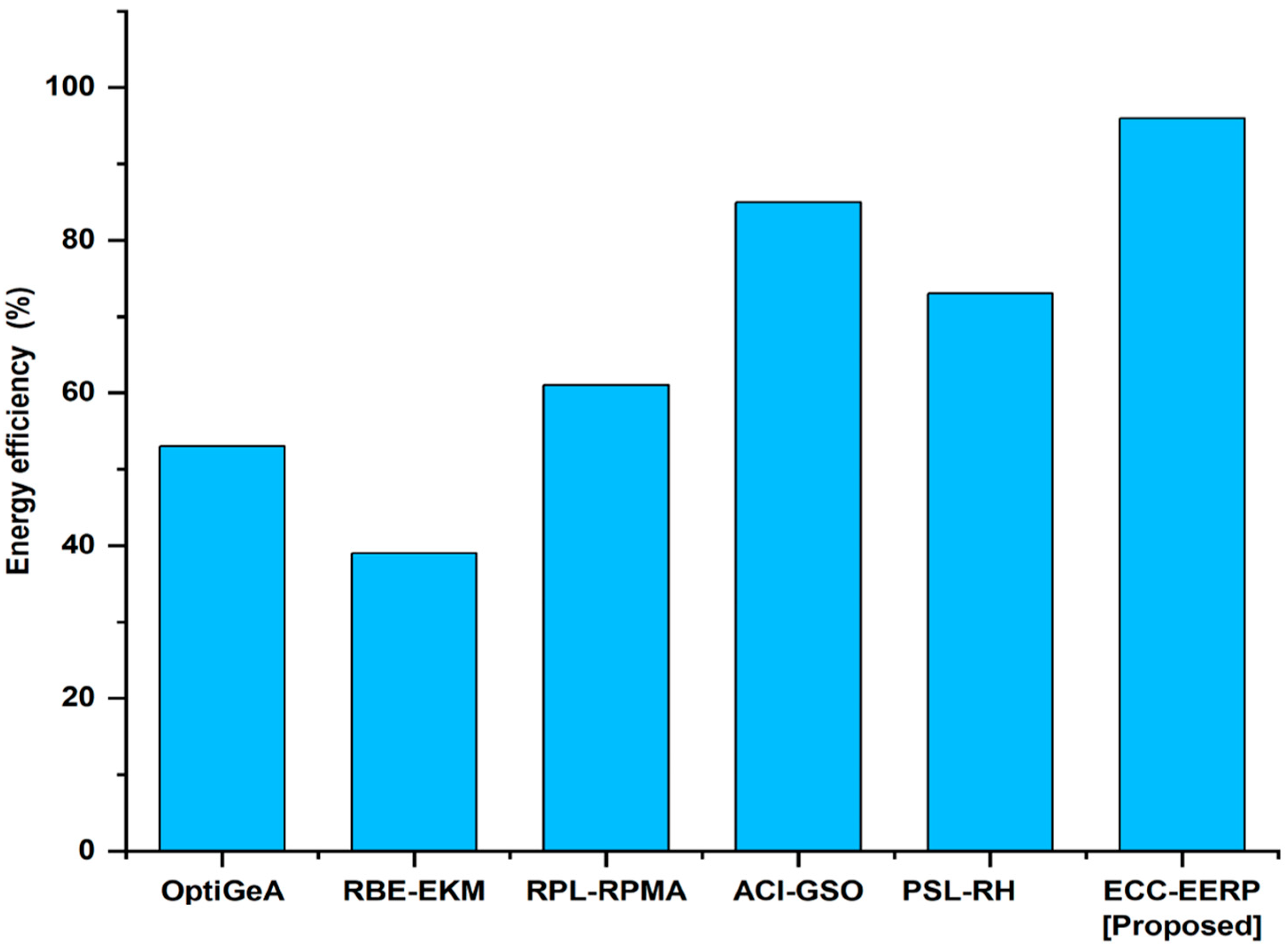
4.3. Energy Efficiency
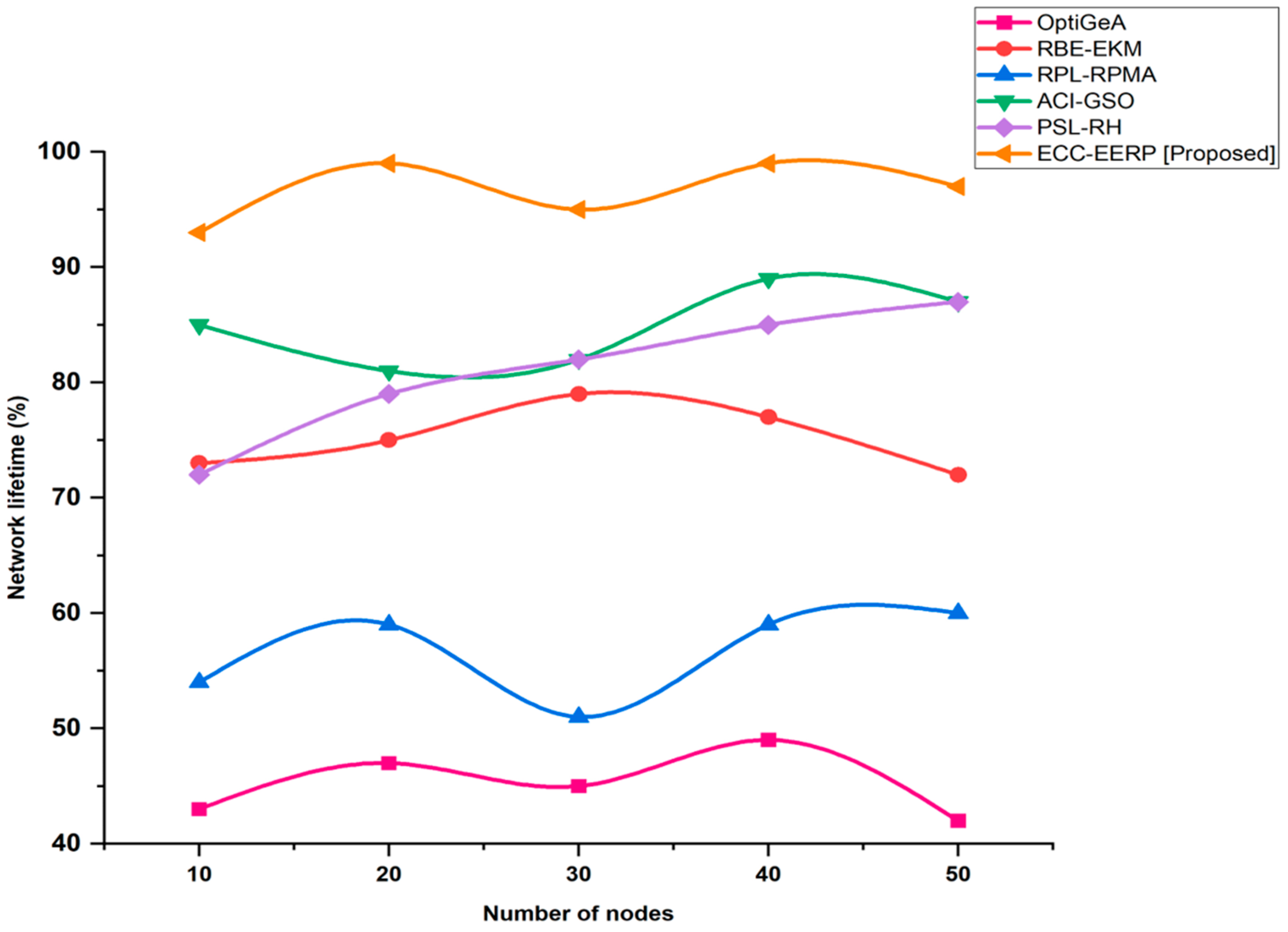
4.4. Network Lifetime
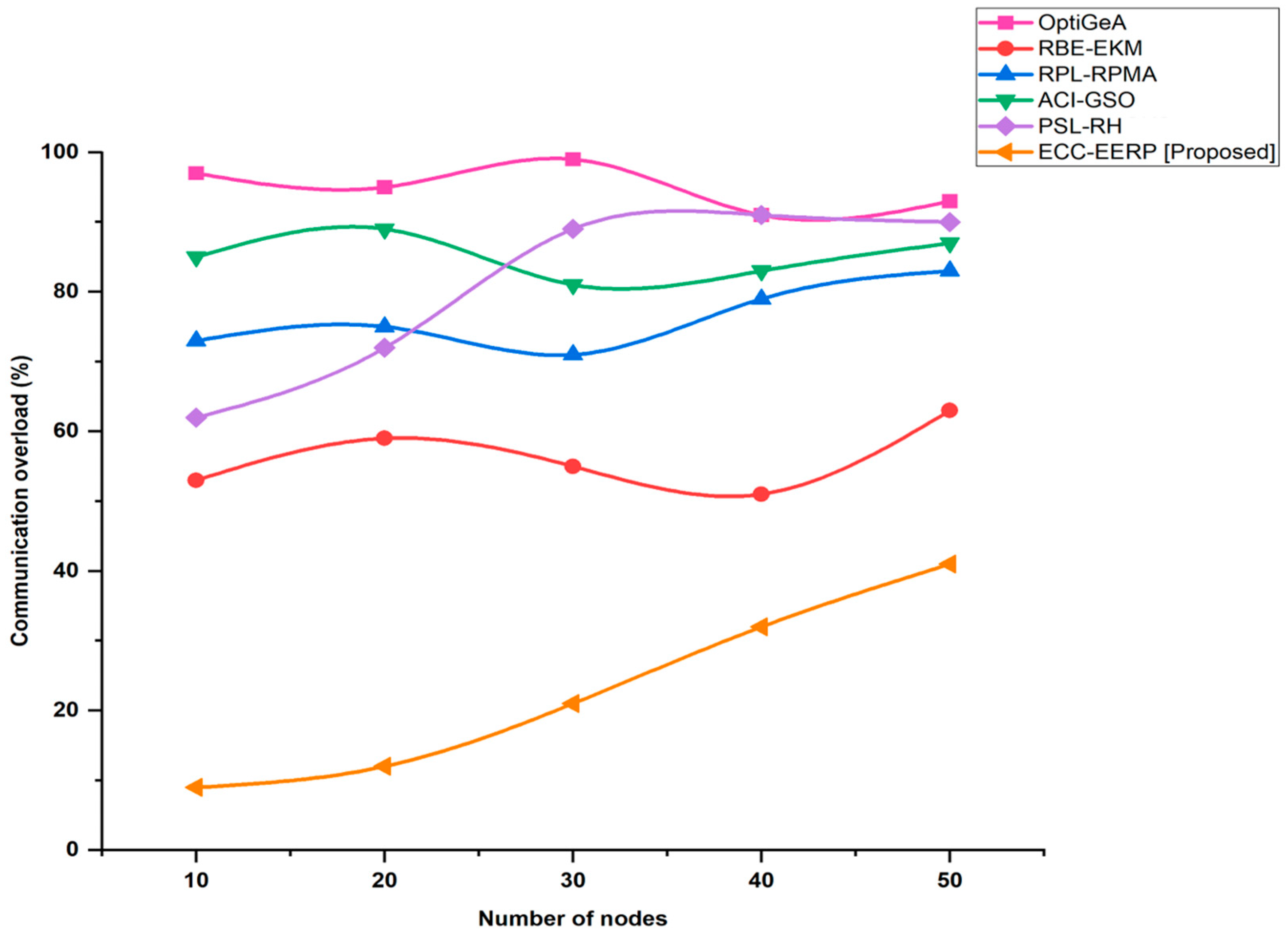
4.5. Communication Overload
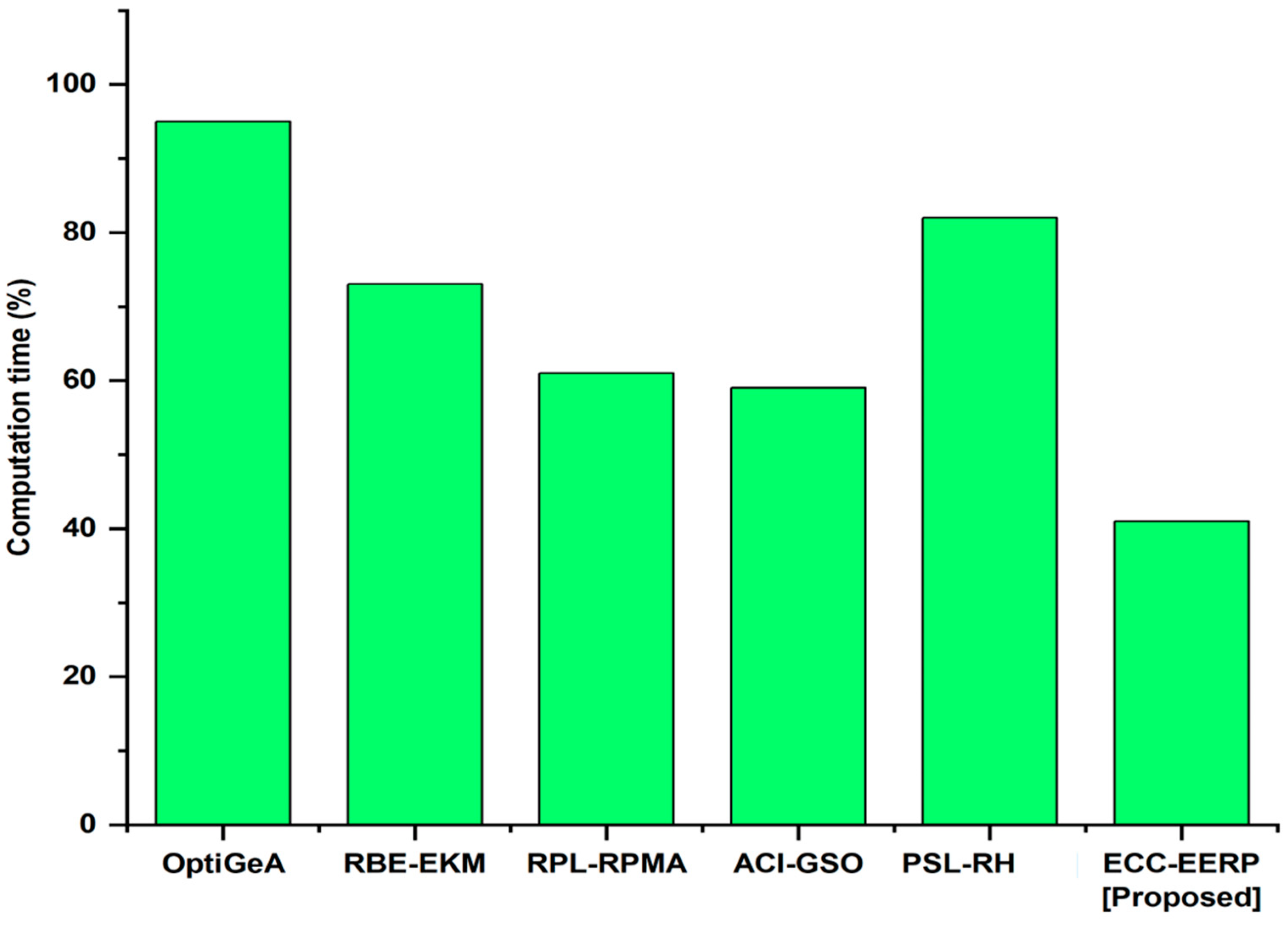
4.6. Computation Time
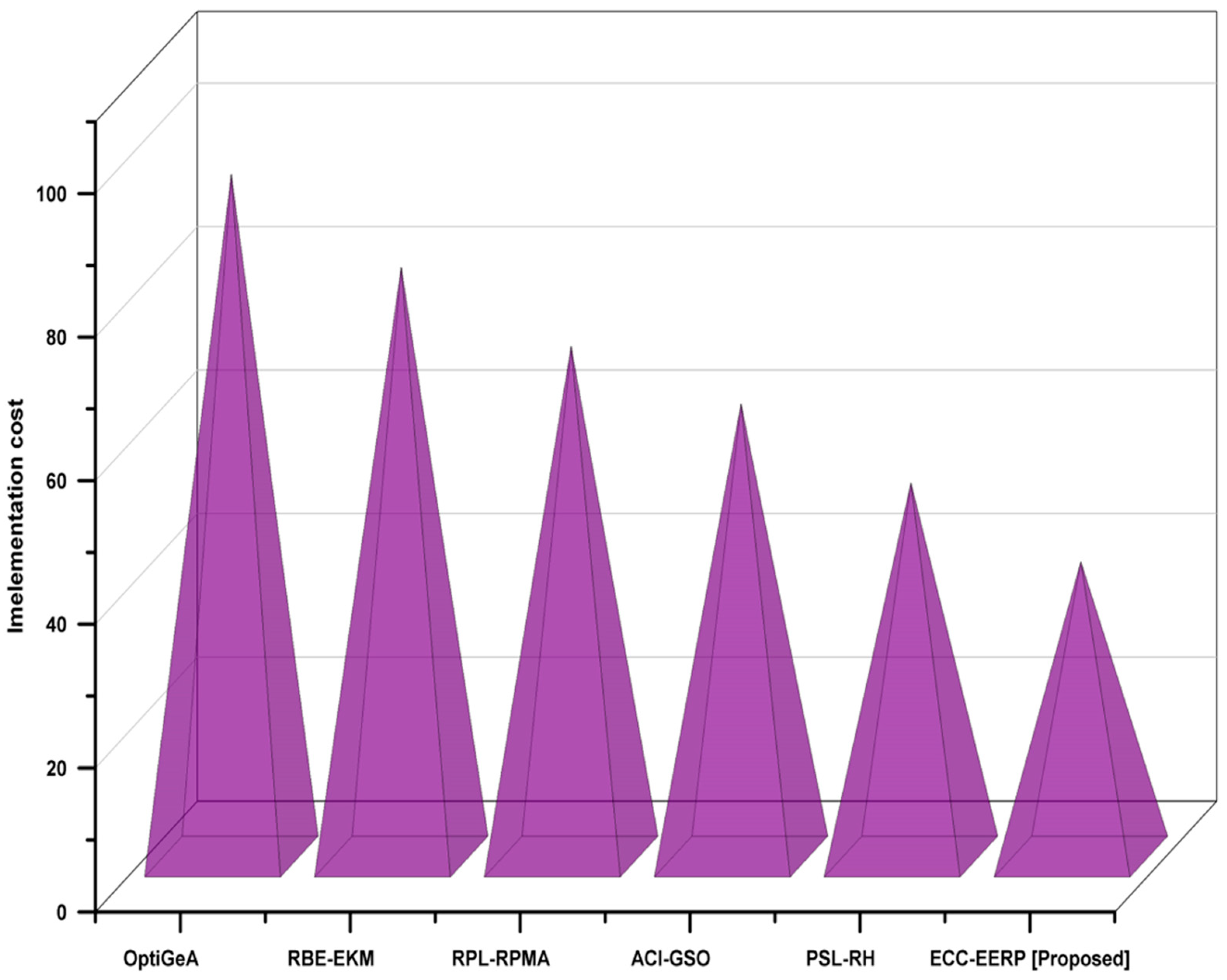
4.7. Implementation Cost
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Reegu, F.A.; Abas, H.; Jabbari, A.; Akmam, R.; Uddin, M.; Wu, C.M.; Chen, C.L.; Khalaf, O.I. Interoperability Requirements for Blockchain-Enabled Electronic Health Records in Healthcare: A Systematic Review and Open Research Challenges. Secur. Commun. Netw. 2022, 2022, 9227343. [Google Scholar] [CrossRef]
- Banumathy, D.; Khalaf, O.I.; Tavera Romero, C.A.; Raja, P.V.; Sharma, D.K. Breast calcifications and histopathological analysis on tumor detection by CNN. Comput. Syst. Sci. Eng. 2023, 44, 595–612. [Google Scholar] [CrossRef]
- Khalaf, O.I.; Natarajan, R.; Mahadev, N.; Christodoss, P.R.; Nainan, T.; Romero, C.A.T.; Abdulsahib, G.M. Blinder Oaxaca and Wilk Neutrosophic Fuzzy Set-based IoT Sensor Communication for Remote Healthcare Analysis. IEEE Access 2022, 21, 1–13. [Google Scholar] [CrossRef]
- Jabbar, M.A.; Shandilya, S.K.; Kumar, A.; Shandilya, S. Applications of cognitive internet of medical things in Modern Healthcare. Comput. Electr. Eng. 2022, 102, 108276. [Google Scholar] [CrossRef]
- Mahesh, T.R.; Kumar, D.; Kumar, V.V.; Asghar, J.; Bazezew, B.M.; Natarajan, R.; Vivek, V. Blended Ensemble Learning Prediction Model for Strengthening Diagnosis and Treatment of Chronic Diabetes Disease. Comput. Intell. Neurosci. 2022, 2022, 4451792. [Google Scholar] [CrossRef]
- Islam, M.M.; Rahaman, A.; Islam, M.R. Development of Smart Healthcare Monitoring System in IOT environment. SN Comput. Sci. 2020, 1, 185. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Einav, S.; Pearse, R.; Jaber, S.; Kranke, P.; Overdyk, F.J.; Whitaker, D.K.; Gordo, F.; Dahan, A.; Hoeft, A. Improving detection of patient deterioration in the General Hospital Ward Environment. Eur. J. Anaesthesiol. 2018, 35, 325–333. [Google Scholar] [CrossRef]
- Wibrandt, I.; Lippert, A. Improving patient safety in handover from Intensive Care Unit to general Ward: A systematic review. J. Patient Saf. 2017, 16, 199–210. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R.; Rab, S. Biosensors applications in medical field: A brief review. Sens. Int. 2021, 2, 100100. [Google Scholar] [CrossRef]
- Mahari, S.; Gandhi, S. Recent advances in electrochemical biosensors for the detection of salmonellosis: Current prospective and challenges. Biosensors 2022, 12, 365. [Google Scholar] [CrossRef]
- Gaba, G.S.; Hedabou, M.; Kumar, P.; Braeken, A.; Liyanage, M.; Alazab, M. Zero knowledge proofs based authenticated key agreement protocol for sustainable healthcare. Sustain. Cities Soc. 2022, 80, 103766. [Google Scholar] [CrossRef]
- Rajesh, N.; Christodoss, P.R. Analysis of origin, risk factors influencing COVID-19 cases in India and its prediction using ensemble learning. Int. J. Syst. Assur. Eng. Manag. 2021, 75, 1–8. [Google Scholar] [CrossRef]
- Arvisais-Anhalt, S.; Lau, M.; Lehmann, C.U.; Holmgren, A.J.; Medford, R.J.; Ramirez, C.M.; Chen, C.N. The 21st Century Cures Act and Multiuser Electronic Health Record Access: Potential Pitfalls of Information Release. J. Med. Internet Res. 2022, 24, e34085. [Google Scholar] [CrossRef] [PubMed]
- Steinkamp, J.; Kantrowitz, J.J.; Airan-Javia, S. Prevalence and sources of duplicate information in the Electronic Medical Record. JAMA Netw. Open 2022, 5, e2233348. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Medical 4.0 technologies for healthcare: Features, capabilities, and applications. Internet Things Cyber-Phys. Syst. 2022, 2, 12–30. [Google Scholar] [CrossRef]
- Iyamu, T. The interpretivist and analytics approaches for Healthcare Big Data Analytics. Adv. Big Data Anal. Healthc. Serv. Deliv. 2022, 76, 74–88. [Google Scholar] [CrossRef]
- Mbunge, E.; Muchemwa, B.; Jiyane, S.; Batani, J. Sensors and healthcare 5.0: Transformative SHIFT IN virtual care through Emerging Digital Health Technologies. Glob. Health J. 2021, 5, 169–177. [Google Scholar] [CrossRef]
- Subahi, A.F.; Khalaf, O.I.; Alotaibi, Y.; Natarajan, R.; Mahadev NRamesh, T. Modified Self-Adaptive Bayesian Algorithm for Smart Heart Disease Prediction in IoT System. Sustainability 2022, 14, 14208. [Google Scholar] [CrossRef]
- Hussein, A.; Mohammed, W.R.; Musa Jaber, M.; Ibrahim Khalaf, O. An Adaptive ECG Noise Removal Process Based on Empirical Mode Decomposition (EMD). Contrast Media Mol. Imaging 2022, 2022, 3346055. [Google Scholar] [CrossRef]
- Kandhro, I.A.; Uddin, M.; Hussain, S.; Chaudhery, T.J.; Shorfuzzaman, M.; Meshref, H.; Albalhaq, M.; Alsaqour, R.; Khalaf, O.I. Impact of Activation, Optimization, and Regularization Methods on the Facial Expression Model Using CNN. Comput. Intell. Neurosci. 2022, 2022, 3098604. [Google Scholar] [CrossRef]
- Meenakshi, R.; Ponnusamy, R.; Alghamdi, S.; Khalaf, O.I.; Alotaibi, Y. Development of a Mobile App to Support the Mobility of Visually Impaired People. CMC-Comput. Mater. Contin. 2022, 73, 3473–3495. [Google Scholar] [CrossRef]
- Radhakrishnan, K.; Ramakrishnan, D.; Khalaf, O.I.; Uddin, M.; Chen, C.L.; Wu, C.M. A Novel Deep Learning-Based Cooperative Communication Channel Model for Wireless Underground Sensor Networks. Sensors 2022, 22, 4475. [Google Scholar] [CrossRef]
- Asghar, J.; Tabasam, M.; Althobaiti, M.M.; Adnan Ashour, A.; Aleid, M.A.; Ibrahim Khalaf, O.; Aldhyani, T.H.H. A Randomized Clinical Trial Comparing Two Treatment Strategies, Evaluating the Meaningfulness of HAM-D Rating Scale in Patients with Major Depressive Disorder. Front. Psychiatry 2022, 13, 873693. [Google Scholar] [CrossRef]
- Ogudo, K.A.; Surendran, R.; Khalaf, O.I. Optimal artificial intelligence-based automated skin lesion detection and classification model. Comput. Syst. Sci. Eng. 2023, 44, 693–707. [Google Scholar] [CrossRef]
- Gnanavel, S.; Sreekrishna, M.; Mani, V.; Kumaran, G.; Amshavalli, R.S.; Alharbi, S.; Maashi, M.; Khalaf, O.I.; Abdulsahib, G.M.; Alghamdi, A.D.; et al. Analysis of Fault Classifiers to Detect the Faults and Node Failures in a Wireless Sensor Network. Electronics 2022, 11, 1609. [Google Scholar] [CrossRef]
- Ortiz, J.H.; Romero, C.A.T.; Ahmed, B.T.; Khalaf, O.I. Qos in fanet business and swarm data. Comput. Mater. Contin. 2022, 72, 1877–1899. [Google Scholar]
- Banumathy, D.; Khalaf, O.I.; Romero, C.A.T.; Indra, J.; Sharma, D.K. Cad of BCD from thermal mammogram images using machine learning. Intell. Autom. Soft Comput. 2022, 34, 667–685. [Google Scholar] [CrossRef]
- Sengan, S.; Khalaf, O.I.; Ettiyagounder, P.; Sharma, D.K.; Karrupusamy, R. Novel Approximation Booths Multipliers for Error Recovery of Data-Driven Using Machine Learning. In Emerging Technology Trends in Internet of Things and Computing, Proceedings of the TIOTC 2021, Erbil, Iraq, 6–8 June 2021; Communications in Computer and Information Science; Liatsis, P., Hussain, A., Mostafa, S.A., Al-Jumeily, D., Eds.; Springer: Cham, Switzerland, 2022; Volume 1548. [Google Scholar] [CrossRef]
- Malik, P.K.; Naim, A.; Singh, R. Printed Antennas: Design and Challenges; CRC Press: Boca Raton, FL, USA, 2022. [Google Scholar]
- Rajagopal, N.K.; Saini, M.; Huerta-Soto, R.; Vílchez-Vásquez, R.; Kumar, J.N.V.R.; Gupta, S.K.; Perumal, S. Human resource demand prediction and configuration model based on grey wolf optimization and recurrent neural network. Comput. Intell. Neurosci. 2022, 2022, 5613407. [Google Scholar] [CrossRef]
- Refaee, E.; Parveen, S.; Begum, K.M.J.; Parveen, F.; Raja, M.C.; Gupta, S.K.; Krishnan, S. Secure and Scalable Healthcare Data Transmission in IoT Based on Optimized Routing Protocols for Mobile Computing Applications. Wirel. Commun. Mob. Comput. 2022, 2022, 5665408. [Google Scholar] [CrossRef]
- Kaushal, R.K.; Bhardwaj, R.; Kumar, N.; Aljohani, A.A.; Gupta, S.K.; Singh, P.; Purohit, N. Using Mobile Computing to Provide a Smart and Secure Internet of Things (IoT) Framework for Medical Applications. Wirel. Commun. Mob. Comput. 2022, 2022, 8741357. [Google Scholar] [CrossRef]
- Hazela, B.; Gupta, S.K.; Soni, N.; Saranya, C.N. Securing the Confidentiality and Integrity of Cloud Computing Data. ECS Trans. 2022, 107, 2651. [Google Scholar] [CrossRef]
- Gupta, S.K.; Tiwari, S.; Abd Jamil, A.; Singh, P. Faster as well as Early Measurements from Big Data Predictive Analytics Model. ECS Trans. 2022, 107, 2927. [Google Scholar] [CrossRef]
- Rehman, A.; Abbas, S.; Khan, M.A.; Ghazal, T.M.; Adnan, K.M.; Mosavi, A. A Secure Healthcare 5.0 System Based on Blockchain Technology Entangled with Federated Learning Technique. Comput. Biol. Med. 2022, 150, 106019. [Google Scholar] [CrossRef]
- Shadab, A.; Shuaib, M.; Ahmad, S.; Jayakody, D.N.; Muthanna, A.; Bharany, S.; Elgendy, I.A. Blockchain-Based Solutions Supporting Reliable Healthcare for Fog Computing and Internet of Medical Things (IOMT) Integration. Sustainability 2022, 14, 15312. [Google Scholar] [CrossRef]
- Wazid, M.; Ashok, K.D.; Park, Y. Blockchain-Enabled Secure Communication Mechanism for IOT-Driven Personal Health Records. Trans. Emerg. Telecommun. Technol. 2021, 33, e4421. [Google Scholar] [CrossRef]
- Zaidi, S.Y.; Munam, A.S.; Khattak, H.A.; Maple, C.; Rauf, H.T.; El-Sherbeeny, A.M.; El-Meligy, M.A. An Attribute-Based Access Control for IOT Using Blockchain and Smart Contracts. Sustainability 2021, 13, 10556. [Google Scholar] [CrossRef]
- Liang, X.; Tang, B.; Cai, Z.; Huang, Z.; Luo, B.; Lin, B.; Yang, Y.; Liu, Q.; Zhou, H. Metabolic Feature Profiling and Metabolic Vulnerability Targeting in B-Cell Lymphoblastic Leukemia. Blood 2022, 140 (Suppl. 1), 6361–6362. [Google Scholar] [CrossRef]
- Thirukrishna, J.T.; Aishwarya, M.V.; Mansi, S.; Mounisha, B.; Naksha, K. Efficient data Transmission in WSN using wearable sensors for Healthcare Monitoring. Int. J. Adv. Res. Innov. Ideas Educ. 2021, 7, 446–457. [Google Scholar]
- Singh, S.; Nandan, A.S.; Sikka, G.; Malik, A.; Vidyarthi, A. A secure energy-efficient routing protocol for disease data transmission using IoMT. Comput. Electr. Eng. 2022, 101, 108113. [Google Scholar] [CrossRef]
- Anbarasu, S. Rank-Based Energy Efficient Key Management (RBE-EKM) Scheme Based Routing for Internet of Medical Things (IOMT); Bharathiar University: Tamil Nadu, India, 2022. [Google Scholar]
- Ambika, K.; Malliga, S. Secure hyper intelligence in routing protocol with low-power (RPL) Networks in IoT. Adv. Eng. Softw. 2022, 173, 103247. [Google Scholar] [CrossRef]
- Reddy, D.L.; Puttamadappa, C.; Suresh, H.N. Merged glowworm swarm with ant colony optimization for energy efficient clustering and routing in the wireless sensor network. Pervasive Mob. Comput. 2021, 71, 101338. [Google Scholar] [CrossRef]
- Khadidos, A.O.; Shitharth, S.; Khadidos, A.O.; Sangeetha, K.; Alyoubi, K.H. Healthcare Data Security Using IoT Sensors Based on Random Hashing Mechanism. J. Sens. 2022, 2022, 8457116. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No | Reference | Method | Advantage | Disadvantage |
|---|---|---|---|---|
| 1 | [35] | Real-time deep extreme learning system (RTS-DELM) | Effectively evaluates federated learning-based healthcare 5.0 network’s dependability | Travel time, chance of patient catching an illness, and line-ups |
| 2 | [36] | Blockchain-based fog computing model (BFCM) | Interchange of information and data between medical institutions is facilitated by IoMT technology in healthcare industry | IoMT devices are susceptible to variety of attacked due to lack of hardware and software security features |
| 3 | [37] | Blockchain-enabled secure communication mechanism for IoT-driven personal health records (BIPHRS) | Dependable security system to protect transfer and storage of healthcare data | Data that have already been recorded cannot be easily changed, all of block codes must be rewritten |
| 4 | [38] | Cipher policy-attribute-based encryption (CP-ABE) | In an IoT-enabled world, healthcare 5.0 must protect client data security | Uses patient-centered digital well-being and strains capabilities of healthcare 4.0 |
| 5 | [39] | Mobile medical service system (MMSS) | Correlation of different medicinal goods is calculated using correlation functions, such as cosine correlation | Large-scale IoT medical systems are challenging to design or administer on single cloud platform |
| Kubernetes and Devices | Hardware Instruments |
|---|---|
| Master Node | Laptop dell E6520 |
| Intel core i7-CPU 2760QM @ 2.40 GHz | |
| 8 GB RAM DDR3 | |
| Work Node | Raspberry pi 4 |
| ARM Cortex-A72 | |
| IoT Device | Finger Pulse Oximeter Jumper JPD-450F |
| 1.6 V | |
| with Bluetooth v4.2 |
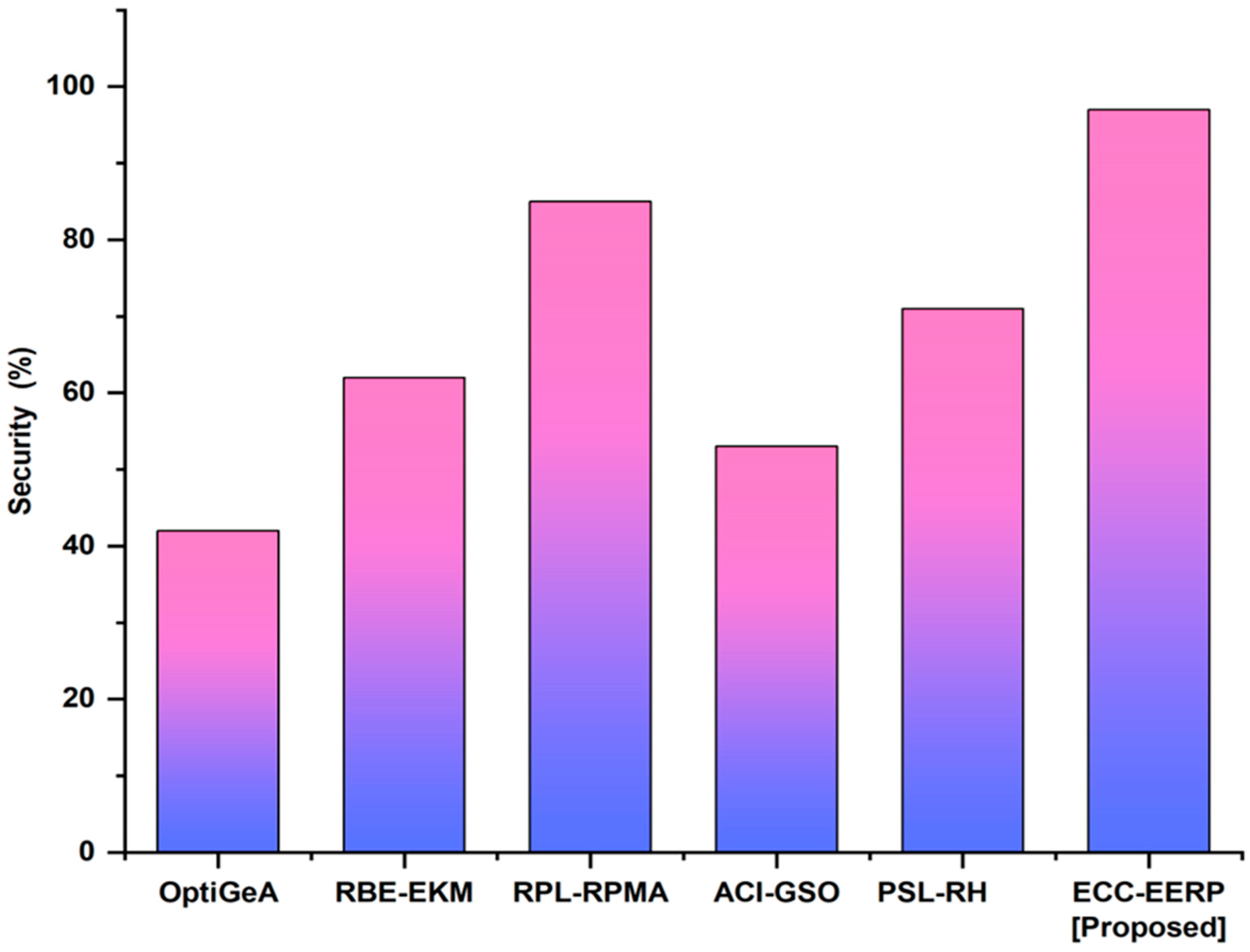
| Method | Security (%) |
|---|---|
| OptiGeA [41] | 42 |
| RBE-EKM [42] | 62 |
| RPL-RPMA [43] | 85 |
| ACI-GSO [44] | 53 |
| PSL-RH [45] | 71 |
| ECC-EERP (Proposed) | 97 |
| Number of Nodes | Encryption Throughput (%) | |||||
|---|---|---|---|---|---|---|
| OptiGeA [41] | RBE-EKM [42] | RPL-RPMA [43] | ACI-GSO [44] | PSL-RH [45] | ECC-EERP (Proposed) | |
| 10 | 5 | 53 | 29 | 49 | 52 | 97 |
| 20 | 7 | 59 | 32 | 88 | 62 | 96 |
| 30 | 9 | 63 | 37 | 69 | 73 | 95 |
| 40 | 12 | 73 | 39 | 75 | 79 | 98 |
| 50 | 15 | 81 | 43 | 80 | 81 | 99 |
| Method | Energy Efficiency (%) |
|---|---|
| OptiGeA [41] | 53 |
| RBE-EKM [42] | 39 |
| RPL-RPMA [43] | 61 |
| ACI-GSO [44] | 85 |
| PSL-RH [45] | 73 |
| ECC-EERP (Proposed) | 96 |
| Number of Nodes | Network Lifetime (%) | |||||
|---|---|---|---|---|---|---|
| OptiGeA [41] | RBE-EKM [42] | RPL-RPMA [43] | ACI-GSO [44] | PSL-RH [45] | ECC-EERP (Proposed) | |
| 10 | 43 | 73 | 54 | 85 | 72 | 93 |
| 20 | 47 | 75 | 59 | 81 | 79 | 99 |
| 30 | 45 | 79 | 51 | 82 | 82 | 95 |
| 40 | 49 | 77 | 59 | 89 | 85 | 99 |
| 50 | 42 | 72 | 60 | 87 | 87 | 97 |
| Number of Nodes | Communication Overload (%) | |||||
|---|---|---|---|---|---|---|
| OptiGeA [41] | RBE-EKM [42] | RPL-RPMA [43] | ACI-GSO [44] | PSL-RH [45] | ECC-EERP (Proposed) | |
| 10 | 97 | 53 | 73 | 85 | 62 | 9 |
| 20 | 95 | 59 | 75 | 89 | 72 | 12 |
| 30 | 99 | 55 | 71 | 81 | 89 | 21 |
| 40 | 91 | 51 | 79 | 83 | 91 | 32 |
| 50 | 93 | 63 | 83 | 87 | 90 | 41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natarajan, R.; Lokesh, G.H.; Flammini, F.; Premkumar, A.; Venkatesan, V.K.; Gupta, S.K. A Novel Framework on Security and Energy Enhancement Based on Internet of Medical Things for Healthcare 5.0. Infrastructures 2023, 8, 22. https://doi.org/10.3390/infrastructures8020022
Natarajan R, Lokesh GH, Flammini F, Premkumar A, Venkatesan VK, Gupta SK. A Novel Framework on Security and Energy Enhancement Based on Internet of Medical Things for Healthcare 5.0. Infrastructures. 2023; 8(2):22. https://doi.org/10.3390/infrastructures8020022
Chicago/Turabian StyleNatarajan, Rajesh, Gururaj Harinahallo Lokesh, Francesco Flammini, Anitha Premkumar, Vinoth Kumar Venkatesan, and Shashi Kant Gupta. 2023. "A Novel Framework on Security and Energy Enhancement Based on Internet of Medical Things for Healthcare 5.0" Infrastructures 8, no. 2: 22. https://doi.org/10.3390/infrastructures8020022