
Clinico-Morphological Features and Immunohistochemical Profile of a Rare Case of Three Synchronous Primary Malignancies in the Female Genital Tract
 , ,
, ,
Abstract
:1. Introduction
2. Detailed Case Description
2.1. Clinical Presentation
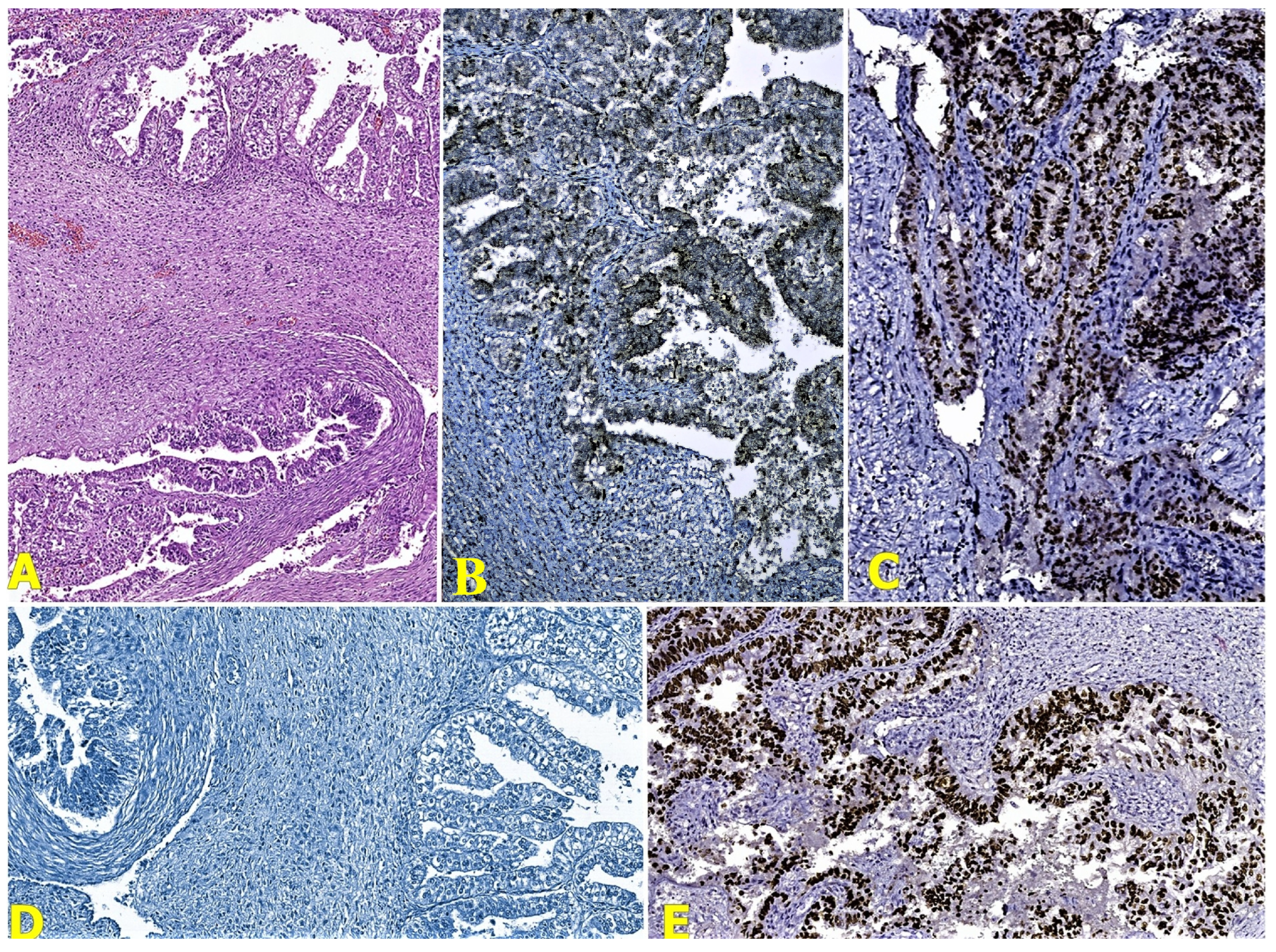
2.2. Pathological Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Das, S. Synchronous and Metachronous Cancers: An Update. Ann. Clin. Case Rep. 2017, 2, 1388. [Google Scholar]
- Gutierrez-Palomino, L.; Romo-de Los Reyes, J.M.; Pareja-Megia, M.J.; Garcia-Mejido, J.A. Triple synchronous primary gynaecological tumours. A case report. Cir. Cir. 2016, 84, 69–72. [Google Scholar] [CrossRef]
- Shah, M.; Aman, A.; Vaswani, B.; Rajesh, B.J.; Sreekanth, C.N. Triple Synchronous Primary Malignancies of Ovary, Endometrium and Cervix—A Rare Case Report. JMSCR 2018, 06, 16–22. [Google Scholar] [CrossRef]
- Kan, O.; Alkilic, A.; Turgay, B.; Gemici, A.; Atabekoglu, C.S. Triple Synchronous Malignancies in Genital Tract; Primary Endometrial, Ovarian and Fallopian Tube Carcinoma: A Case Report. J. Clin. Diagn. Res. 2017, 11, QD01–QD02. [Google Scholar] [CrossRef]
- Song, L.; Li, Q.; Yang, K.; Yin, R.; Wang, D. Three primary synchronous malignancies of the uterus, cervix, and fallopian tube: A case report. Medicine 2018, 97, e11107. [Google Scholar] [CrossRef]
- Karki, S.; Chapagain, U. Synchronous primary tumors of the endometrium and ovary. J. Pathol. Nepal 2012, 2, 189–192. [Google Scholar] [CrossRef]
- Zhang, Y.; Cao, L.; Nguyen, D.; Lu, H. TP53 mutations in epithelial ovarian cancer. Transl. Cancer Res. 2016, 5, 650–663. [Google Scholar] [CrossRef]
- Nakamura, M.; Obata, T.; Daikoku, T.; Fujiwara, H. The Association and Significance of p53 in Gynecologic Cancers: The Potential of Targeted Therapy. Int. J. Mol. Sci. 2019, 20, 5482. [Google Scholar] [CrossRef]
- Terada, K.Y.; Ahn, H.J.; Kessel, B. Differences in risk for type 1 and type 2 ovarian cancer in a large cancer screening trial. J. Gynecol. Oncol. 2016, 27, e25. [Google Scholar] [CrossRef]
- Skirnisdottir, I.; Bjersand, K.; Akerud, H.; Seidal, T. Napsin A as a marker of clear cell ovarian carcinoma. BMC Cancer 2013, 13, 524. [Google Scholar] [CrossRef]
- Liu, J.; Wang, H.; Zheng, M.; Deng, L.; Zhang, X.; Lin, B. p53 and ANXA4/NF κB p50 complexes regulate cell proliferation, apoptosis and tumor progression in ovarian clear cell carcinoma. Int. J. Mol. Med. 2020, 46, 2102–2114. [Google Scholar] [CrossRef]
- Ho ES, C.; Lai, C.R.; Hsieh, Y.T.; Chen, J.T.; Lin, A.J.; Hung, M.J.; Liu, F.S. p53 Mutation Is Infrequent in Clear Cell Carcinoma of the Ovary. Gynecol. Oncol. 2001, 80, 189–193. [Google Scholar]
- Xiao, W.; Awadallah, A.; Xin, W. Loss of ARID1A/BAF250a expression in ovarian endometriosis and clear cell carcinoma. Int. J. Clin. Exp. Pathol. 2012, 5, 642–650. [Google Scholar]
- DeLair, D.; Oliva, E.; Kobel, M.; Macias, A.; Gilks, C.B.; Soslow, R.A. Morphologic spectrum of immunohistochemically characterized clear cell carcinoma of the ovary: A study of 155 cases. Am. J. Surg. Pathol. 2011, 35, 36–44. [Google Scholar] [CrossRef]
- Nakano, T.; Enoki, K.; Nakashima, M.; Ishikawa, H.; Ametani, Y.; Ohta, S.; Ohkuchi, A.; Satake, S.; Kojima, Y.; Funamoto, H.; et al. Survival in patients with clear cell carcinoma of the ovary. Gan Kagaku Ryoho 1998, 25, 67–73. [Google Scholar]
- Langland, G.T.; Yannone, S.M.; Langland, R.A.; Nakao, A.; Guan, Y.; Long, S.B.T.; Vonguyen, L.; Chen, D.J.; Gray, J.W.; Chen, F. Radiosensitivity profiles from a panel of ovarian cancer cell lines exhibiting genetic alterations in p53 and disparate DNA-dependent protein kinase activities. Oncol. Rep. 2010, 23, 1021–1026. [Google Scholar] [CrossRef]
- Angelico, G.; Santoro, A.; Straccia, P.; Inzani, F.; Cianfrini, F.; Spadola, S.; Arciuolo, D.; Valente, M.; D’Alessandris, N.; Mulè, A.; et al. Diagnostic and Prognostic Role of WT1 Immunohistochemical Expression in Uterine Carcinoma: A Systematic Review and Meta-Analysis across All Endometrial Carcinoma Histotypes. Diagnostics 2020, 10, 637. [Google Scholar] [CrossRef]
- Shen, Z.; Luo, H.; Li, S.; Sheng, B.; Zhao, M.; Zhu, H.; Zhu, X. Correlation between estrogen receptor expression and prognosis in epithelial ovarian cancer: A meta-analysis. Oncotarget 2017, 8, 62400–62413. [Google Scholar] [CrossRef]
- Iida, Y.; Okamoto, A.; Hollis, R.L.; Gourley, C.; Herrington, C.S. Clear cell carcinoma of the ovary: A clinical and molecular perspective. Int. J. Gynecol. Cancer 2021, 31, 605–616. [Google Scholar] [CrossRef]
- Zhu, C.; Zhu, J.; Qian, L.; Liu, H.; Shen, Z.; Wu, D.; Zhao, W.; Xiao, W.; Zhou, Y. Clinical characteristics and prognosis of ovarian clear cell carcinoma: A 10-year retrospective study. BMC Cancer 2021, 21, 322. [Google Scholar] [CrossRef]
- Pors, J.; Segura, S.; Cheng, A.; Ji, J.X.; Tessier-Cloutier, B.; Cochrane, D.; Fix, D.J.; Park, K.; Gilks, B.; Hoang, L. Napsin-A and AMACR are Superior to HNF-1β in Distinguishing Between Mesonephric Carcinomas and Clear Cell Carcinomas of the Gynecologic Tract. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 593–601. [Google Scholar] [CrossRef]
- Nili, F.; Fathi, S.; Tavakoli, M.; Mirzaian, E.; Lotfi, M. Diagnostic Accuracy of Alpha-Methylacyl-CoA Racemase Immunohistochemical Expression for the Diagnosis of Ovarian and Endometrial Clear Cell Carcinomas. Iran J. Pathol. 2023, 18, 57–63. [Google Scholar] [CrossRef]
- Nili, F.; Sadri, M.; Ameli, F. Utility of AMACR immunohistochemical staining in differentiating Arias-Stella reaction from clear cell carcinoma of ovary and endometrium. BMC Cancer 2023, 23, 332. [Google Scholar] [CrossRef]
- Kim, K.R.; Lax, S.F.; Lazar, A.J.; Longacre, T.A.; Malpica, A.; Matias-Guiu, X. (Eds.) Chapter 6: Tumours of the uterine corpus. In Female Genital Tumours, 5th ed.; WHO Classification of Tumours Editorial Board; IARC: Lyon, France, 2020; Volume 4, p. 246. [Google Scholar]
- Kim, M.J.; Kim, D.S. Expression of p53 Protein in Endometrial Carcinoma. Korean J. Pathol. 1999, 33, 347–352. [Google Scholar]
- Opric, D.; Suskic, A.; Suskic, S.H.; Nikolic, G.; Filipovic, I. Value of p53 and estrogen receptors immunohistochemical staining in endometrial carcinoma. Int. J. Reprod Contracept. Obstet. Gynecol. 2019, 8, 4885–4890. [Google Scholar] [CrossRef]
- Hussein, Y.R.; Soslow, R.A. Molecular insights into the classification of high-grade endometrial carcinoma. Pathology 2018, 50, 151–161. [Google Scholar] [CrossRef]
- Visser, N.C.M.; van der Wurff, A.A.M.; Pijnenborg, J.M.A.; Massuger, L.F.A.G.; Bulten, J.; Nagtegaal, I.D. Tissue microarray is suitable for scientific biomarkers studies in endometrial cancer. Virchows Arch. 2018, 472, 407–413. [Google Scholar] [CrossRef]
- Kong, C.S.; Beck, A.H.; Longacre, T.A. A panel of 3 markers including p16, ProExC, or HPV ISH is optimal for distinguishing between primary endometrial and endocervical adenocarcinomas. Am. J. Surg. Pathol. 2010, 34, 915–926. [Google Scholar] [CrossRef]
- Porzio, R.; Cordini, C.; Rodolfi, A.M.; Brigati, F.; Ubiali, A.; Proietto, M.; Di Nunzio, C.; Cavanna, L. Triple negative endometrial cancer: Incidence and prognosis in a monoinstitutional series of 220 patients. Oncol. Lett. 2020, 19, 2522–2526. [Google Scholar] [CrossRef]
- Smith, D.; Stewart, C.J.; Clarke, E.M.; Lose, F.; Davies, C.; Armes, J.; Obermair, A.; Brennan, D.; Webb, P.M.; Nagle, C.M.; et al. ER and PR expression and survival after endometrial cancer. Gynecol. Oncol. 2018, 148, 258–266. [Google Scholar] [CrossRef]
- Waqar, S.; Khan, S.A.; Sarfraz, T.; Waqar, S. Expression of Estrogen Receptors (ER), Progesterone Receptors (PR) and HER-2/neu receptors in Endometrial Carcinoma and their associations with histological types, grades and stages of the tumor. Pak. J. Med. Sci. 2018, 34, 266–271. [Google Scholar] [CrossRef]
- Stolnicu, S.; Hoang, L.; Hanko-Bauer, O.; Barsan, I.; Terinte, C.; Pesci, A.; Aviel-Ronen, S.; Kiyokawa, T.; Alvarado-Cabrero, I.; Oliva, E.; et al. Cervical adenosquamous carcinoma: Detailed analysis of morphology, immunohistochemical profile, and clinical outcomes in 59 cases. Mod. Pathol. 2019, 32, 269–279. [Google Scholar] [CrossRef]
- Freier, C.P.; Stiasny, A.; Kuhn, C.; Mayr, D.; Alexiou, C.; Janko, C.; Wiest, I.; Jeschke, U.; Kost, B. Immunohistochemical Evaluation of the Role of p53 Mutation in Cervical Cancer: Ser-20 p53-Mutant Correlates with Better Prognosis. Anticancer Res. 2016, 36, 3131–3137. [Google Scholar]
- Gbadegesin, M.A.; Omotoso, O.E.; Oluwasola, T.A.; Okolo, C.A.; Soremekun, O.; Ogun, G.O.; Oluwasola, A.O.; Odunola, O.A. Mutational analysis of p53 gene in cervical cancer and useful polymorphic variants in exons 3 and 4. Egypt J. Med. Hum. Genet. 2021, 22, 1–8. [Google Scholar] [CrossRef]
- Li, M.; Yang, J.; Liu, K.; Yang, J.; Zhan, X.; Wang, L.; Shen, X.; Chen, J.; Mao, Z. p16 promotes proliferation in cervical carcinoma cells through CDK6-HuR-IL1A axis. J. Cancer 2020, 11, 1457–1467. [Google Scholar] [CrossRef]
- Fisher, M.L.; Balinth, S.; Mills, A.A. p63-related signaling at a glance. J. Cell Sci. 2020, 133, jcs228015. [Google Scholar] [CrossRef]
- Steurer, S.; Riemann, C.; Büscheck, F.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Hoflmayer, D.; Weidemann, S.; Fraune, C.; et al. p63 expression in human tumors and normal tissues: A tissue microarray study on 10,200 tumors. Biomark Res. 2021, 9, 7. [Google Scholar] [CrossRef]
- Abu-Zaid, A.; Alsabban, M.; Abuzaid, M.; Alomar, O.; Salem, H.; Al-Badawi, I.A. Triple Synchronous Primary Neoplasms of the Cervix, Endometrium, and Ovary: A Rare Case Report and Summary of All the English PubMed-Indexed Literature. Case Rep. Obstet. Gynecol. 2017, 2017, 9705078. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Immunohistochemical Markers (Clone) | Results | ||
|---|---|---|---|
| Clear-Cell Ovarian Carcinoma | Uterine Endometrioid Adenocarcinoma | Cervical Adenosquamous Carcinoma | |
| P53 (EP9) | Over-expression pattern | Over-expression pattern | Wild-type pattern |
| P16 (BC42) | Negative reaction | Intense positive nuclear reaction with mosaic pattern | Intense diffuse positive nuclear reaction |
| P63 (4A4) | Negative reaction | Negative reaction | Diffuse positive nuclear reaction in the squamous component |
| WT1 (rWT1/857) | Negative reaction | Negative reaction | Negative reaction |
| ER (SP1) | Intense positive nuclear reaction in tumoral glands | Intense positive nuclear reaction in tumoral glands | Negative reaction |
| Napsin A (TMU-Ad 02) | Intense focal positive cytoplasmic reaction | Negative reaction | Negative reaction |
| Vimentin (SP20) | Negative reaction | Intense diffuse positive cytoplasmic reaction | Negative reaction |
| AMACR (13H4) | Intense diffuse positive cytoplasmic reaction | Negative reaction | Negative reaction |
| PR (16) | Negative reaction | Negative reaction | Negative reaction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boșoteanu, M.; Vodă, R.I.; Balţǎtescu, G.I.; Aşchie, M.; Nurla, L.-A.; Orǎşanu, C.I. Clinico-Morphological Features and Immunohistochemical Profile of a Rare Case of Three Synchronous Primary Malignancies in the Female Genital Tract. Reports 2024, 7, 14. https://doi.org/10.3390/reports7010014
Boșoteanu M, Vodă RI, Balţǎtescu GI, Aşchie M, Nurla L-A, Orǎşanu CI. Clinico-Morphological Features and Immunohistochemical Profile of a Rare Case of Three Synchronous Primary Malignancies in the Female Genital Tract. Reports. 2024; 7(1):14. https://doi.org/10.3390/reports7010014
Chicago/Turabian StyleBoșoteanu, Mădălina, Raluca Ioana Vodă, Gabriela Izabela Balţǎtescu, Mariana Aşchie, Luana-Andreea Nurla, and Cristian Ionuţ Orǎşanu. 2024. "Clinico-Morphological Features and Immunohistochemical Profile of a Rare Case of Three Synchronous Primary Malignancies in the Female Genital Tract" Reports 7, no. 1: 14. https://doi.org/10.3390/reports7010014