
Comparison between SARS-CoV-2-Associated Acute Disseminated Encephalomyelitis and Acute Stroke: A Case Report

 ,
, 

Abstract
:1. Introduction
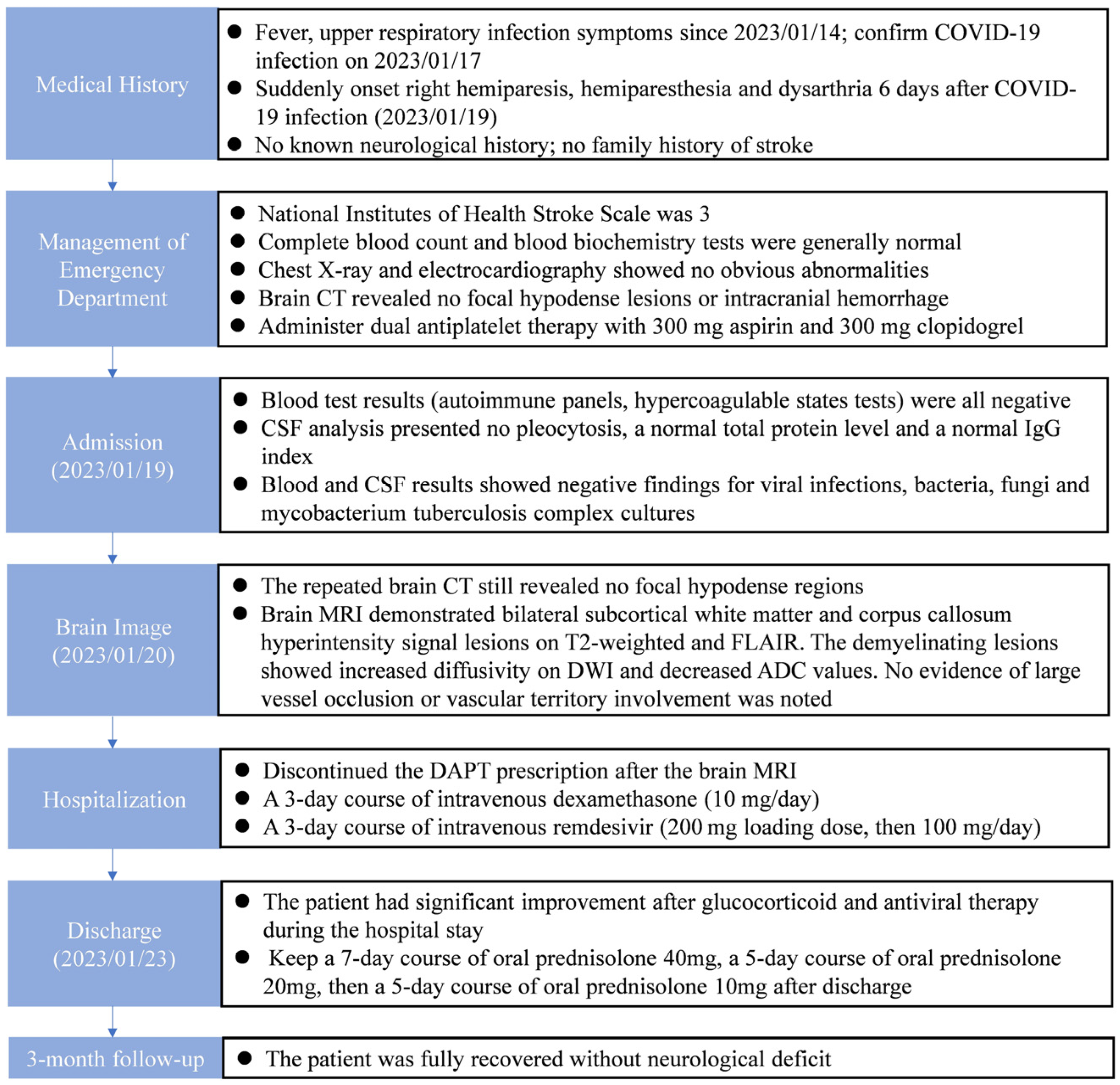
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Misra, S.; Misra, S.; Kolappa, K.; Kolappa, K.; Prasad, M.; Prasad, M.; Radhakrishnan, D.; Radhakrishnan, D.; Thakur, K.T.; Thakur, K.T.; et al. Frequency of Neurologic Manifestations in COVID-19: A Systematic Review and Meta-analysis. Neurology 2021, 97, e2269–e2281. [Google Scholar] [CrossRef] [PubMed]
- Gavriilaki, E.; Anyfanti, P.; Gavriilaki, M.; Lazaridis, A.; Douma, S.; Gkaliagkousi, E. Endothelial Dysfunction in COVID-19: Lessons Learned from Coronaviruses. Curr. Hypertens. Rep. 2020, 22, 63. [Google Scholar] [CrossRef]
- Dai, X.; Cao, X.; Jiang, Q.; Wu, B.; Lou, T.; Shao, Y.; Hu, Y.; Lan, Q. Neurological complications of COVID-19. Qjm Int. J. Med. 2023, 116, 161–180. [Google Scholar] [CrossRef] [PubMed]
- Stoian, A.; Bajko, Z.; Stoian, M.; Cioflinc, R.A.; Niculescu, R.; Arbănași, E.M.; Russu, E.; Botoncea, M.; Bălașa, R. The Occurrence of Acute Disseminated Encephalomyelitis in SARS-CoV-2 Infection/Vaccination: Our Experience and a Systematic Review of the Literature. Vaccines 2023, 11, 1225. [Google Scholar] [CrossRef] [PubMed]
- Feizi, P.; Sharma, K.; Pasham, S.R.; Nirwan, L.; Joseph, J.; Jaiswal, S.; Sriwastava, S. Central nervous system (CNS) inflammatory demyelinating diseases (IDDs) associated with COVID-19: A case series and review. J. Neuroimmunol. 2022, 371, 577939. [Google Scholar] [CrossRef]
- Zanin, L.; Saraceno, G.; Panciani, P.P.; Renisi, G.; Signorini, L.; Migliorati, K.; Fontanella, M.M. SARS-CoV-2 can induce brain and spine demyelinating lesions. Acta Neurochir. 2020, 162, 1491–1494. [Google Scholar] [CrossRef]
- Manzano, G.S.; McEntire, C.R.S.; Martinez-Lage, M.; Mateen, F.J.; Hutto, S.K. Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalitis Following COVID-19: Systematic Review and Meta-synthesis. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, 1080. [Google Scholar] [CrossRef]
- Parsons, T.; Banks, S.; Bae, C.; Gelber, J.; Alahmadi, H.; Tichauer, M. COVID-19-associated acute disseminated encephalomyelitis (ADEM). J. Neurol. 2020, 267, 2799–2802. [Google Scholar] [CrossRef]
- Nabizadeh, F.; Noori, M.; Rahmani, S.; Hosseini, H. Acute disseminated encephalomyelitis (ADEM) following COVID-19 vaccination: A systematic review. J. Clin. Neurosci. 2023, 111, 57–70. [Google Scholar] [CrossRef]
- Kakovan, M.; Shirkouhi, S.G.; Zarei, M.; Andalib, S. Stroke Associated with COVID-19 Vaccines. J. Stroke Cerebrovasc. Dis. 2022, 31, 106440. [Google Scholar] [CrossRef]
- Wang, R.L.; Chiang, W.F.; Shyu, H.Y.; Chen, M.H.; Lin, C.I.; Wu, K.A.; Yang, C.C.; Huang, L.Y.; Hsiao, P.J. COVID-19 vaccine-associated acute cerebral venous thrombosis and pulmonary artery embolism. Qjm Int. J. Med. 2021, 114, 506–507. [Google Scholar] [CrossRef]
- Fan, H.T.; Lin, Y.Y.; Chiang, W.F.; Lin, C.Y.; Chen, M.H.; Wu, K.A.; Chan, J.S.; Kao, Y.H.; Shyu, H.Y.; Hsiao, P.J. COVID-19 vaccine-induced encephalitis and status epilepticus. Qjm Int. J. Med. 2022, 115, 91–93. [Google Scholar] [CrossRef]
- Chen, W.-P.; Chen, M.-H.; Shang, S.-T.; Kao, Y.-H.; Wu, K.-A.; Chiang, W.-F.; Chan, J.-S.; Shyu, H.-Y.; Hsiao, P.-J. Investigation of Neurological Complications after COVID-19 Vaccination: Report of the Clinical Scenarios and Review of the Literature. Vaccines 2023, 11, 425. [Google Scholar] [CrossRef] [PubMed]
- Pohl, D.; Alper, G.; Van Haren, K.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. Neurology 2016, 87 (Suppl. S2), S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Bhawna, S.; Rahul, H.; Kadam, N.; Swayam, P.; Gupta, P.K.; Agrawal, R.; Sisodiya, M.S. Transient splenial diffusion-weighted image restriction mimicking stroke. Am. J. Emerg. Med. 2014, 32, 1156.e1–1156.e2. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanya, K.S.; Kovoor, J.M.E.; Jayakumar, P.N.; Ravishankar, S.; Kamble, R.B.; Panicker, J.; Nagaraja, D. Diffusion-weighted imaging and proton MR spectroscopy in the characterization of acute disseminated encephalomyelitis. Neuroradiology 2007, 49, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Tardieu, M.; Amato, M.P.; Banwell, B.; Chitnis, T.; Dale, R.C.; Ghezzi, A.; Hintzen, R.; Kornberg, A.; Pohl, D.; et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: Revisions to the 2007 definitions. Mult. Scler. J. 2013, 19, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Koelman, D.L.; Chahin, S.; Mar, S.S.; Venkatesan, A.; Hoganson, G.M.; Yeshokumar, A.K.; Barreras, P.; Majmudar, B.; Klein, J.P.; Chitnis, T.; et al. Acute disseminated encephalomyelitis in 228 patients: A retrospective, multicenter US study. Neurology 2016, 86, 2085–2093. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Murthy, J.M.K. Acute disseminated encephalomyelitis: Treatment guidelines. Ann. Indian. Acad. Neurol. 2011, 14 (Suppl. S1), S60–S64. [Google Scholar] [CrossRef]
- Nannoni, S.; de Groot, R.; Bell, S.; Markus, H.S. Stroke in COVID-19: A systematic review and meta-analysis. Int. J. Stroke. 2021, 16, 137–149. [Google Scholar] [CrossRef]
- Kits, A.; Pantalone, M.R.; Illies, C.; Antovic, A.; Landtblom, A.-M.; Iacobaeus, E. Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report. Vaccines 2022, 10, 2046. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Item | Result | Unit | Normal Range |
|---|---|---|---|
| White blood cells | 5280 | /μL | 4800–10,800 |
| C-reactive protein | 0.57 | mg/dL | <0.5 |
| Procalcitonin | <0.05 | ng/mL | <0.07 |
| Triglyceride | 72.3 | mg/dL | 21–175 |
| Total cholesterol | 131.3 | mg/dL | 110–200 |
| LDL cholesterol | 84.9 | mg/dL | <100 |
| Prothrombin time | 11.4 | s | 9.4–12 |
| Activated partial thromboplastin time | 31.2 | s | 25.3–32.3 |
| ESR | 21 | mm/1 h | <29 |
| ANA | Negative | ||
| Anti-ds DNA | Negative | ||
| Rheumatoid factor | <10 | IU/mL | <14 |
| cANCA | Negative | ||
| pANCA | Negative | ||
| C3 | 82.9 | mg/dL | 87–200 |
| C4 | 36.5 | mg/dL | 19–52 |
| Anti-cardiolipin IgM | Negative | ||
| Anti-cardiolipin IgG | Negative | ||
| Anti-phospholipid antibody IgG | Negative | ||
| Anti-β2 glycoprotein IgG | Negative | ||
| Protein C | 75.5 | % | 70–140 |
| Protein S | 81.8 | % | 63.5–149 |
| Antithrombin III | 94.7 | % | 83–128 |
| SARS-CoV-2 PCR | Positive, cycle threshold value 14 | ||
| Anti-HIV test | Nonreactive | ||
| RPR | Nonreactive | ||
| TPPA/TPHA test | Negative | ||
| Anti-HCV | Nonreactive | ||
| HBsAg | Nonreactive | ||
| Herpes simplex virus 1 IgM | Negative | ||
| Herpes simplex virus 2 IgM | Negative | ||
| Cytomegalovirus IgM | Negative | ||
| Epstein-Barr virus IgM | Negative |
| Item | Result | Unit | Normal Range |
|---|---|---|---|
| pH | 7.103 | ||
| White blood cells | <5 | /μL | |
| Red blood cells | 25 | /μL | |
| Total protein | 30.5 | mg/dL | 15–45 |
| Glucose | 57.39 | mg/dL | 40–70 |
| LDH | 25.5 | U/L | |
| Chloride | 127.9 | mmol/L | |
| IgG index | 0.62 | 0–0.7 | |
| Gram stain | No bacteria | ||
| CSF culture | No bacteria | ||
| Indian ink | Not found | ||
| Acid-fast stain | Not found | ||
| TB PCR DNA | Negative | ||
| TB culture | Negative | ||
| VDRL | Non-Reactive | ||
| Cytomegalovirus PCR | Not detected | ||
| Herpes simplex virus 1 PCR | Not detected | ||
| Herpes simplex virus 2 PCR | Not detected | ||
| Human herpesvirus 6 PCR | Not detected | ||
| Human parechovirus PCR | Not detected | ||
| Enterovirus PCR | Not detected | ||
| Varicella zoster virus PCR | Not detected | ||
| Cryptococcus neoformans/gattii PCR | Not detected | ||
| Neisseria meningitidis | Not detected | ||
| Listeria monocytogenes | Not detected | ||
| Streptococcus agalactiae | Not detected | ||
| Streptococcus pneumoniae | Not detected | ||
| Escherichia coli K1 | Not detected | ||
| Haemophilus influenzae | Not detected |
| Clinical Characteristics | COVID-19-Associated ADEM [6] | COVID-19-Associated Stroke [20] |
|---|---|---|
| Incidence | The incidence of classic ADEM is approximately 2–5 per million per year in children. | Pooled incidence of 1.4% |
| However, the incidence of COVID-19-associated ADEM and ADEM in adults is not clear due to the lack of standardized reporting of cases. | ||
| Age | Advanced age (nearly half are >50 years old) | Median 65.3 years |
| In contrast to classic ADEM, COVID-19-associated ADEM occurs more in adults than children. | In comparison to stroke patients without COVID-19, people with COVID-19 and stroke were younger. | |
| Duration since COVID-19 symptom onset | Usually occurring within 15–30 days | Median 8.8 days |
| Neurologic signs | Encephalopathy Focal motor deficits (paraparesis, quadriparesis) Cranial nerve deficits (oculomotor deficits, dysarthria) Focal sensory deficits Seizure Aphasia | Unilateral numbness or weakness of the face, arm or leg Aphasia Dysarthria Disorientation Ataxia Median NIHSS † 15 |
| Radiological features | T2 FLAIR: diffuse, multifocal hyperintensities in the supratentorial and infratentorial white matter, but may also involve gray matter and/or the spinal cord. DWI: increased diffusivity ADC: decreased values in the acute stage; increased values in the subacute stage [16]. Some patients (42%) had evidence for hemorrhage on brain MRI, significantly higher than classic ADEM (2% in prior studies) [6]. | Large vessel occlusion Multiple vascular territory infarction |
| Treatment | IV methylprednisolone IV immunoglobulin Plasmapheresis COVID-19-directed therapies | Antiplatelet therapy IV thrombolysis Endovascular thrombectomy |
| Prognosis | mRS ‡ score 6 (mortality): 20% mRS score 4–5 (severe disability): 20% mRS score 0–1 (no disability): 11% | In-hospital death: 31.5% Discharged to rehabilitation facilities: 25.7% Discharged home: 19.1% |
| Acute Disseminated Encephalomyelitis | Multiple Sclerosis | Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease | Neuromyelitis Optica Spectrum Disorder | |
|---|---|---|---|---|
| Clinical features | Acute and fulminant encephalopathy with multifocal neurologic findings; monophase; typically follows a prodromal viral illness | Chronic inflammation and demyelination; relapsing–remitting course; the multiphase; may not follow a prodromal viral illness | Central nervous system demyelination including ADEM, ON, TM; the most common is ON; monophasic or relapsing | ON, TM, area postrema syndrome; typically relapsing |
| Radiographic features | Poorly marginated lesions with larger bilateral but asymmetric white matter abnormalities in MRI | Ovoid plaques MRI lesions; hypointense T1-weighted lesions (black holes); Dawson fingers on sagittal views | ADEM-like MRI; enhancement of optic nerve MRI | Enhancement of optic nerve MRI |
| CSF analysis | Variable; nonspecific | Presence of oligoclonal bands; elevated proteins | Oligoclonal bands are typically absent; MOG-IgG autoantibody (+) in CSF | Variable; nonspecific |
| Serum autoantibodies | No specific biomarkers | No specific biomarkers | MOG-IgG autoantibody (+) | Anti-AQP4-IgG antibody (+) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, Y.-X.; Chen, M.-H.; Lin, Y.-Y.; Kao, Y.-H.; Liao, T.-W.; Chiu, C.-C.; Hsiao, P.-J. Comparison between SARS-CoV-2-Associated Acute Disseminated Encephalomyelitis and Acute Stroke: A Case Report. Reports 2024, 7, 18. https://doi.org/10.3390/reports7010018
Jiang Y-X, Chen M-H, Lin Y-Y, Kao Y-H, Liao T-W, Chiu C-C, Hsiao P-J. Comparison between SARS-CoV-2-Associated Acute Disseminated Encephalomyelitis and Acute Stroke: A Case Report. Reports. 2024; 7(1):18. https://doi.org/10.3390/reports7010018
Chicago/Turabian StyleJiang, Yu-Xuan, Ming-Hua Chen, Yen-Yue Lin, Yung-Hsi Kao, Ting-Wei Liao, Chih-Chien Chiu, and Po-Jen Hsiao. 2024. "Comparison between SARS-CoV-2-Associated Acute Disseminated Encephalomyelitis and Acute Stroke: A Case Report" Reports 7, no. 1: 18. https://doi.org/10.3390/reports7010018