
Life-Threatening Obstetrical Emergency: Spontaneous Uterine Rupture Associated with Placenta Percreta in the First Trimester of Pregnancy—Case Report and Literature Review
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
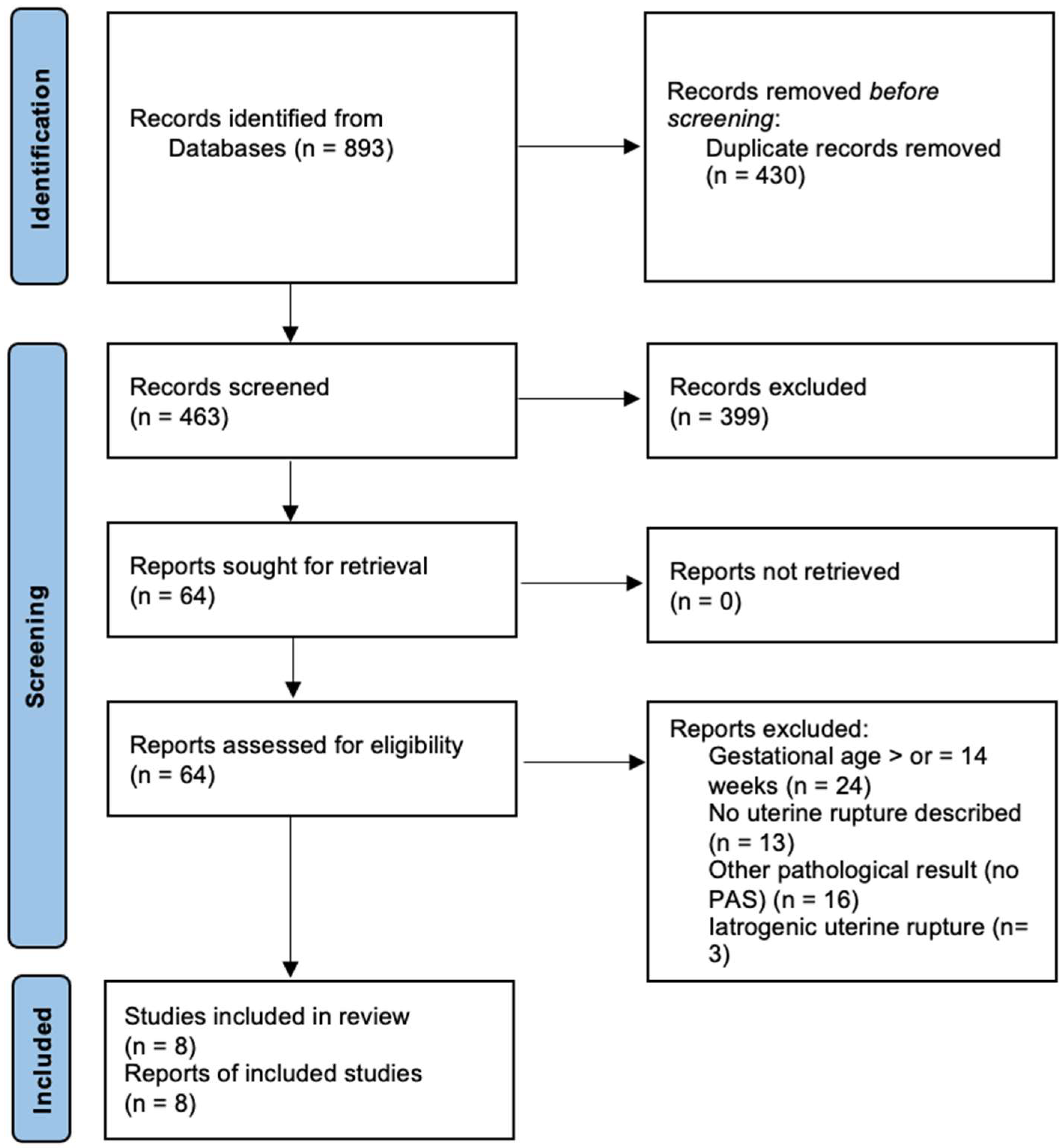
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Selection of Studies and Data Collection
2.4. Statistical Analysis
3. Results
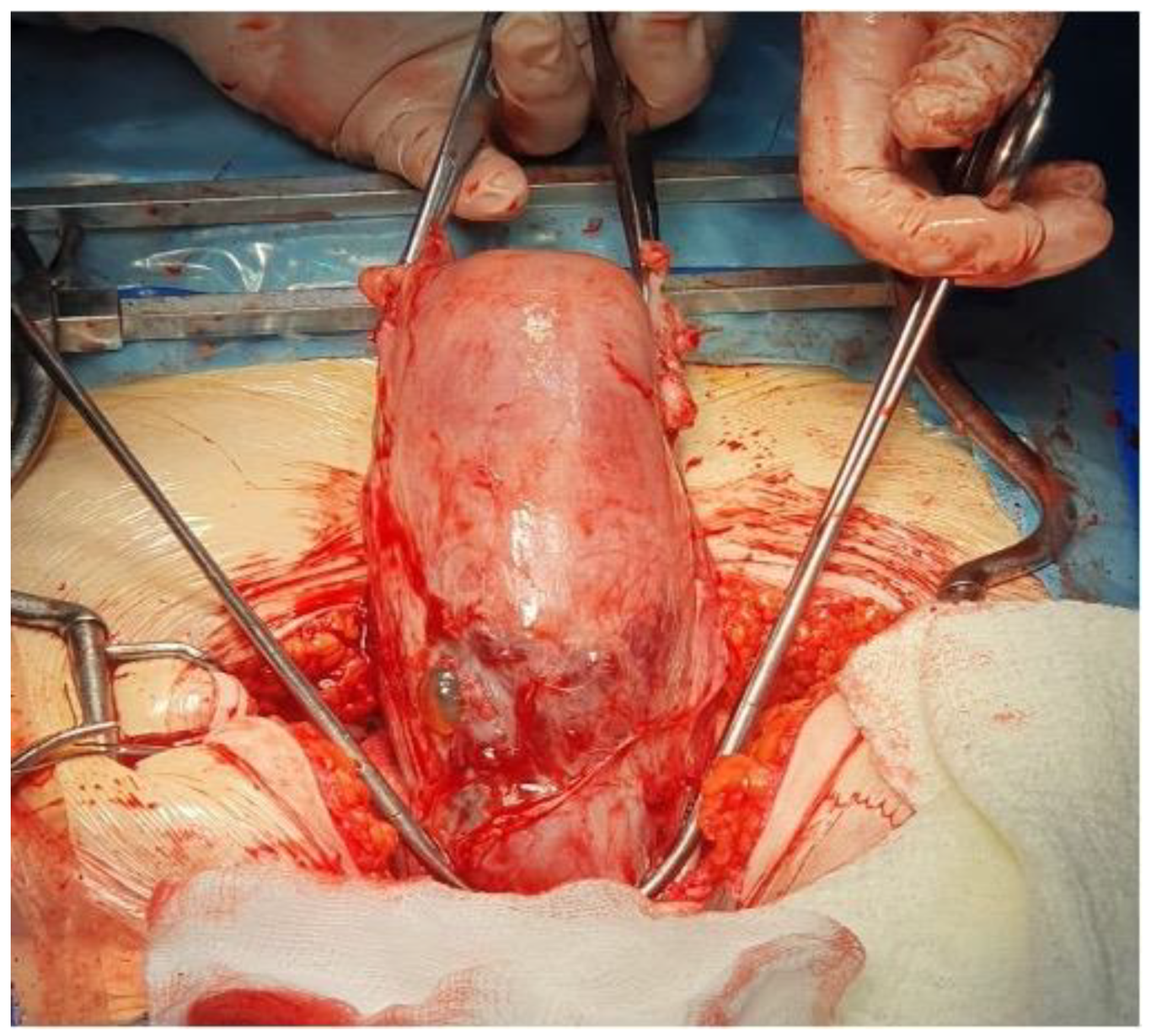
3.1. Case Report
3.2. Results of Systematic Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jauniaux, E.; Ayres-De-Campos, D.; Langhoff-Roos, J.; Fox, K.A.; Collins, S. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel. FIGO classification for the clinical diagnosis of placenta accreta spectrum disorders. Int. J. Gynaecol. Obstet. 2019, 146, 20–24. [Google Scholar] [CrossRef]
- Jauniaux, E.; Collins, S.; Burton, G.J. Placenta accreta spectrum: Pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am. J. Obstet. Gynecol. 2018, 218, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Rekowska, A.K.; Obuchowska, K.; Bartosik, M.; Kimber-Trojnar, Ż.; Słodzińska, M.; Wierzchowska-Opoka, M.; Leszczyńska-Gorzelak, B. Biomolecules Involved in Both Metastasis and Placenta Accreta Spectrum-Does the Common Pathophysiological Pathway Exist? Cancers 2023, 15, 2618. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Bunce, C.; Grønbeck, L.; Langhoff-Roos, J. Prevalence and main outcomes of placenta accreta spectrum: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 221, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, K.E.; Sellers, S.; Spark, P.; Kurinczuk, J.J.; Brocklehurst, P.; Knight, M. Incidence and risk factors for placenta accreta/increta/percreta in the UK: A national case-control study. PLoS ONE 2012, 7, e52893. [Google Scholar] [CrossRef] [PubMed]
- Timor-Tritsch, I.E.; Monteagudo, A.; Cali, G.; Vintzileos, A.; Viscarello, R.; Al-Khan, A.; Zamudio, S.; Mayberry, P.; Cordoba, M.M.; Dar, P. Cesarean scar pregnancy is a precursor of morbidly adherent placenta. Ultrasound Obstet. Gynecol. 2014, 44, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Kaser, D.J.; Melamed, A.; Bormann, C.L.; Myers, D.E.; Missmer, S.A.; Walsh, B.W.; Racowsky, C.; Carusi, D.A. Cryopreserved embryo transfer is an independent risk factor for placenta accreta. Fertil. Steril. 2015, 103, 1176–1184.e2. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.E.; Leonard, S.A.; Fox, K.A.; Carusi, D.A.; Lyell, D.J. Placenta Accreta Spectrum among Women with Twin Gestations. Obstet. Gynecol. 2021, 137, 132–138. [Google Scholar] [CrossRef]
- Silver, R.M.; Barbour, K.D. Placenta accreta spectrum: Accreta, increta, and percreta. Obstet. Gynecol. Clin. North Am. 2015, 42, 381–402. [Google Scholar] [CrossRef]
- Arakaza, A.; Zou, L.; Zhu, J. Placenta Accreta Spectrum Diagnosis Challenges and Controversies in Current Obstetrics: A Review. Int. J. Women’s Health 2023, 15, 635–654. [Google Scholar] [CrossRef]
- Carusi, D.A. The Placenta Accreta Spectrum: Epidemiology and Risk Factors. Clin. Obstet. Gynecol. 2018, 61, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Turgut, A.; Ozler, A.; Evsen, M.S.; Soydinc, H.E.; Goruk, N.Y.; Karacor, T.; Gul, T. Uterine rupture revisited: Predisposing factors, clinical features, management and outcomes from a tertiary care center in Turkey. Pak. J. Med. Sci. 2013, 29, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Fox, K.A.; Barton, J.R.; Abuhamad, A.Z.; Simhan, H.; Huls, C.K.; Belfort, M.A.; Wright, J.D. Center of excellence for placenta accreta. Am. J. Obstet. Gynecol. 2014, 212, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Abinader, R.R.; Macdisi, N.; El Moudden, I.; Abuhamad, A. First-trimester ultrasound diagnostic features of placenta accreta spectrum in low-implantation pregnancy. Ultrasound Obstet. Gynecol. 2021, 59, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Boujida, S.; M’Hamdi, O.; Flissate, F.; Baidada, A.; Kharbach, A. Placenta percreta as a cause of uterine rupture in the second trimester: Case report. Int. J. Surg. Case Rep. 2022, 94, 107069. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Takiuchi, T.; Kanagawa, T.; Matsuzaki, S.; Lee, M.; Maeda, M.; Endo, M.; Kimura, T. Maternal and Fetal Outcomes after Prior Mid-Trimester Uterine Rupture: A Systematic Review with Our Experience. Medicina 2021, 57, 1294. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Marcus, S.; Cheng, E.; Goff, B. Extrauterine pregnancy resulting from early uterine rupture. Obstet. Gynecol. 1999, 94, 804–805. [Google Scholar] [CrossRef]
- Esmans, A.; Gerris, J.; Corthout, E.; Verdonk, P.; Declercq, S. Placenta percreta causing rupture of an unscarred uterus at the end of the first trimester of pregnancy: Case report. Hum. Reprod. 2004, 19, 2401–2403. [Google Scholar] [CrossRef]
- Deroux, S.J.; Prendergast, N.C.; Adsay, N.V. Spontaneous uterine rupture with fatal hemoperitoneum due to placenta accreta percreta: A case report and review of the literature. Int. J. Gynecol. Pathol. 1999, 18, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Dabulis, S.A.; McGuirk, T.D. An unusual case of hemoperitoneum: Uterine rupture at 9 weeks gestational age. J. Emerg. Med. 2007, 33, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Hanif, S.; Hanif, H.; Sharif, S. Acute abdomen at 12 weeks secondary to placenta percreta. J. Coll. Physicians Surg. Pak. 2011, 21, 572–573. [Google Scholar] [PubMed]
- Brown, J.V.; Epstein, H.D.; Laflamme, L.A.; Goldstein, B.H.; Iii, J.V.B. First-trimester placenta percreta with urinary bladder invasion. Int. J. Gynecol. Obstet. 2015, 132, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.K.; Ryu, H.K.; Kim, C.H. Placenta Percreta-Induced Uterine Rupture at 7th Week of Pregnancy after In Vitro Fertilization in a Primigravida Woman: Case Report. J. Emerg. Med. 2017, 53, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Ambrogi, G.; Ambrogi, G.; Marchi, A.A. Placenta Percreta and Uterine Rupture in the First Trimester of Pregnancy. Case Rep. Obstet. Gynecol. 2018, 2018, 6842892. [Google Scholar] [CrossRef]
- Roeters, A.E.; Oudijk, M.A.; Heydanus, R.; Bruinse, H.W. Pregnancy outcome after intra-abdominal bleeding due to placenta percreta at 14 weeks of gestation. Obstet. Gynecol. 2007, 109, 574–576. [Google Scholar] [CrossRef]
- Smith, L.; Mueller, P. Abdominal pain and hemoperitoneum in the gravid patient: A case report of placenta percreta. Am. J. Emerg. Med. 1996, 14, 45–47. [Google Scholar] [CrossRef]
- Oral, B.; Güney, M.; Özsoy, M.; Sönal, S. Placenta accreta associated with a ruptured pregnant rudimentary uterine horn. Case report and review of the literature. Arch. Gynecol. Obstet. 2001, 265, 100–102. [Google Scholar] [CrossRef]
- Masia, F.; Zoric, L.; Ripart-Neveu, S.; Marès, P.; Ripart, J. Spontaneous uterine rupture at 14 weeks gestation during a pregnancy consecutive to an oocyte donation in a woman with Turner’s syndrome. Anaesth. Crit. Care Pain Med. 2015, 34, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, R.J.; Nicholl, M.; Gibson, J.S. A case of placenta percreta presenting in the first trimester of pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 1987, 27, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Tanyi, J.L.; Coleman, N.M.; Johnston, N.D.; Ayensu-Coker, L.; Rajkovic, A. Placenta percreta at 7th week of pregnancy in a woman with previous caesarean section. J. Obstet. Gynaecol. 2008, 28, 338–340. [Google Scholar] [CrossRef]
- López, J.A.G.; Sánchez, L.G.; Pinilla-Monsalve, G.D.; Timor-Tritsch, I.E. Placenta accreta spectrum disorders in the first trimester: A systematic review. J. Obstet. Gynaecol. 2022, 42, 1703–1710. [Google Scholar] [CrossRef]
- Rahimi-Sharbaf, F.; Jamal, A.; Mesdaghinia, E.; Kalahroudi, M.A.; Niroomanesh, S.; Atoof, F. Ultrasound detection of placenta accreta in the first trimester of pregnancy. Iran. J. Reprod. Med. 2014, 12, 421–426. [Google Scholar]
- Kilcoyne, A.; Shenoy-Bhangle, A.S.; Roberts, D.J.; Sisodia, R.C.; Gervais, D.A.; Lee, S.I. MRI of Placenta Accreta, Placenta Increta, and Placenta Percreta: Pearls and Pitfalls. Am. J. Roentgenol. 2017, 208, 214–221. [Google Scholar] [CrossRef]
- Perdue, M.; Felder, L.; Berghella, V. First-trimester uterine rupture: A case report and systematic review of the literature. Am. J. Obstet. Gynecol. 2022, 227, 209–217. [Google Scholar] [CrossRef]
- Cecchini, F.; Tassi, A.; Londero, A.P.; Baccarini, G.; Driul, L.; Xodo, S. First Trimester Uterine Rupture: A Case Report and Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 2976. [Google Scholar] [CrossRef] [PubMed]
- Vaezi, M. Unexpected Rupture of Unscarred Uterus at 12 Weeks of Pregnancy: A Case Report and Literature Review. Int. J. Women’s Health Reprod. Sci. 2017, 5, 339–341. [Google Scholar] [CrossRef]
- Park, Y.-J.; Ryu, K.-Y.; Lee, J.-I.; Park, M.-I. Spontaneous uterine rupture in the first trimester: A case report. J. Korean Med. Sci. 2005, 20, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Bandarian, M.; Bandarian, F. Spontaneous rupture of the uterus during the 1st trimester of pregnancy. J. Obstet. Gynaecol. 2014, 35, 199–200. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Gestational Age (Weeks) | Maternal Age (Years) | Gesta Para | Risk Factors | Management | Type of PAS |
|---|---|---|---|---|---|---|
| Marcus et al. (1999) [18] | 13 | 38 | G4 P2 | 2 C-sections | Uterine arteries’ embolization and MTX before hysterectomy | percreta |
| deRoux et al. (1999) [20] | 12 | 22 | G9 P2 | no risk factors | No surgery; maternal death | percreta |
| Esmas et al. (2004) [19] | 13 | 40 | G2 P1 | history of placenta accreta | Hysterectomy | percreta |
| Dabulis et al. (2007) [21] | 9 | * | G5 P3 | 3 C-sections | Hysterectomy | percreta |
| Hanif et al. (2011) [22] | 12 | 24 | G5 P2 | 2 C-sections | Hysterectomy | percreta |
| Brown et al. (2015) [23] | 12 | 28 | G2 P1 | 1 C-section | Hysterectomy | percreta |
| Cho et al. (2017) [24] | 7 | 34 | G1 P0 | frozen embryo transfer | Hysterectomy | percreta |
| Ambrogi et al. (2018) [25] | 13 | 36 | G2 P1 | 1 C-section | Excision of the edges of the uterine rupture and uterine reconstruction | Accreta |
| Our case | 12 | 33 | G3 P2 | 2 C-sections | Hysterectomy | Percreta |
| Author | Clinical Presentation | Ultrasound Scan | Intraoperative Findings | Blood Transfusion |
|---|---|---|---|---|
| Marcus et al. (1999) [18] | cramping and spotting | Pregnancy with cardiac activity abnormally located (a saccular structure anterior but contiguous with the uterus); the endometrium was seen superior to but not surrounding the saccular structure | lower segment UR | * |
| deRoux et al. (1999) [20] | abdominal pain and unresponsive patient | Fetal death; no free fluid intraabdominally | fundal UR | * |
| Esmas et al. (2004) [19] | abdominal pain | Intrauterine pregnancy with cardiac activity; free fluid in the abdomen | fundal UR | yes |
| Dabulis et al. (2007) [21] | abdominal pain, bloating, vomiting, and diarrhea | Intrauterine pregnancy with cardiac activity; free fluid in the cul-de-sac | C-section scar UR | * |
| Hanif et al. (2011) [22] | vomiting, syncope, sharp lower abdominal pain, and abdominal distension | Extrauterine pregnancy; moderate free fluid in the peritoneal cavity | C-section scar UR; bladder invasion | * |
| Brown et al. (2015) [23] | syncopal episode and vaginal bleeding | * | lower segment UR; bladder invasion | yes |
| Cho et al. (2017) [24] | sudden severe abdominal pain | Intrauterine pregnancy with cardiac activity; free fluid in the abdominal cavity | fundal UR | * |
| Ambrogi et al. (2018) [25] | moderate abdominal pain | Intrauterine pregnancy with cardiac activity; free fluid next to the liver and the spleen and in the pelvis | right uterine horn rupture | * |
| Our case | lower diffuse abdominal pain and syncope | Intrauterine pregnancy with cardiac activity; free fluid next to the liver and in the pelvis; placental tissue on the anterior uterine wall; no myometrium or serosa at the level of the C-section scar | C-section scar UR | yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amza, M.; Loghin, M.-G.; Vâlcea, D.-I.; Gică, N.; Conea, I.-M.; Gorecki, G.-P.; Mirică, A.; Sima, R.-M.; Pleș, L. Life-Threatening Obstetrical Emergency: Spontaneous Uterine Rupture Associated with Placenta Percreta in the First Trimester of Pregnancy—Case Report and Literature Review. Reports 2024, 7, 21. https://doi.org/10.3390/reports7010021
Amza M, Loghin M-G, Vâlcea D-I, Gică N, Conea I-M, Gorecki G-P, Mirică A, Sima R-M, Pleș L. Life-Threatening Obstetrical Emergency: Spontaneous Uterine Rupture Associated with Placenta Percreta in the First Trimester of Pregnancy—Case Report and Literature Review. Reports. 2024; 7(1):21. https://doi.org/10.3390/reports7010021
Chicago/Turabian StyleAmza, Mihaela, Mihai-George Loghin, Didel-Ionuț Vâlcea, Nicolae Gică, Ileana-Maria Conea, Gabriel-Petre Gorecki, Alexandra Mirică, Romina-Marina Sima, and Liana Pleș. 2024. "Life-Threatening Obstetrical Emergency: Spontaneous Uterine Rupture Associated with Placenta Percreta in the First Trimester of Pregnancy—Case Report and Literature Review" Reports 7, no. 1: 21. https://doi.org/10.3390/reports7010021