
Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease

Department of Clinical and Health Psychology, University of Edinburgh, Edinburgh EH8 9YL, UK
*
Author to whom correspondence should be addressed.
†
Current address: NHS Grampian, Block A, Clerkseat Building, Royal Cornhill Hospital, Cornhill Road, Aberdeen AB25 2ZH, UK.
‡
Current address: Department of Social Sciences, University of Nicosia, Nicosia, 46 Makedonitissas Avenue, CY-2417, P.O. Box 24005, CY-1700 Nicosia, Cyprus.
Gastrointest. Disord. 2024, 6(1), 191-201; https://doi.org/10.3390/gidisord6010014
Submission received: 9 November 2023
/
Revised: 8 February 2024
/
Accepted: 9 February 2024
/
Published: 17 February 2024
Abstract
:In this study, an exploratory model was tested to investigate the mediating role of gastrointestinal-specific anxiety and perceived disability in the relation between disease activity and the outcomes of quality of life and depression in patients with inflammatory bowel disease (IBD). In a cross-sectional design, data from an online survey of patients with IBD (over the age of 16) recruited through a UK-based IBD charity were used to test a model of serial mediation. Measures targeted disease activity (self-reported), gastrointestinal-specific anxiety (Visceral Sensitivity Index), perceived disability (Perceived Disability Scale), IBD-specific quality of life (UK Inflammatory Bowel Disease Questionnaire), and depression (Depression subscale of the Depression, Anxiety, and Stress Scale). The theoretical model was investigated using model 6 of the PROCESS macro for SPSS. Bootstrapped 95% confidence intervals were constructed for each estimate A total of 320 participants provided valid responses to the survey. Gastrointestinal-specific anxiety and perceived disability were found to serially mediate the relationship between disease activity and quality of life (95%CI = −0.80 to −0.19) and disease activity and depression (95%CI = 0.13 to 0.59). Findings suggested that the effect of multiple psychosocial variables in the experience of people living with IBD and its respective outcomes should be taken into account when planning treatment. The theoretical and clinical implications of these findings are discussed.
1. Introduction
Inflammatory bowel disease (IBD) encompasses a variety of non-infectious diseases that cause chronic inflammation of the gastrointestinal (GI) tract [1]. The most common types are Crohn’s disease (CD, affecting any segment of the gastrointestinal tract) and ulcerative colitis (UC, affecting the colon only); however, rarer forms of microscopic colitis (collagenous colitis, lymphocytic colitis) are commonly included under the umbrella term of IBD [2]. Recently, a global disease burden study estimated that almost 5 million people in the world have an IBD diagnosis with prevalence rates estimated to be 59.25 per 100,000 people [1]. Diagnosis usually occurs between adolescence and early adulthood, with men and women equally affected [3]. This poses a great public health challenge as the early onset and chronic nature of the disease means that patients are likely to be affected by it throughout the remainder of their lives [3]. Further to this, recent epidemiological studies point to an increase in IBD prevalence in developing countries, further straining already challenged health resources [1]. Although IBD is thought to be the result of an uncontrolled immune response mediated by genetic and epigenetic factors or gut microbiota, the role of environmental factors as triggers or causes of this response continues to be a key topic of research [1].
IBD is chronic and unpredictable, with alternating periods of active illness and remission, and current treatment approaches are mainly aimed at managing the inflammatory response during flare episodes and maintaining remission in between episodes [3]. Most management includes adhering to a regular medication regimen (some with considerable side-effects and risks) and significant lifestyle changes (e.g., diet, smoking cessation) [4,5]. Adherence to these treatment regimens is usually a good predictor of remission and the maintenance of an episode-free life; however, several environmental and, in particular, psychological factors appear to affect the taking up of such measures [4,5].
Most individuals with chronic diseases are known to experience significant impairment in quality of life (QoL). Recent meta-analyses have shown that QoL in IBD tends to be lower (1) when compared to healthy controls or other chronic/life-long conditions (such as epilepsy, rheumatoid arthritis, renal disease, asthma, and multiple sclerosis); (2) when symptoms are active; and (3) in those presenting with CD; however, it does tend to improve with time [6,7]. This further illustrates the overall impact that IBD has on someone’s life, but also the importance of disease activity as a key factor in the management of IBD. In IBD, the chronic and unpredictable episodes of active illness and remission, as well as the significant burden from symptoms and treatment demands, are listed amongst the main causes of a lower QoL [8]. For example, in a study by Adler et al. [9], IBD was found to be intrusive and disruptive of education and socialization activities among college students, whilst Kemp et al. [10] report an impact on psychosocial functioning across a range of contexts, including employment, social life, engagement in leisure activities, and overall QoL. A recent study elucidates that patients with IBD tend to be primarily concerned about (1) stigma and how this affects their capacity to socialize; (2) how uncertainty about symptoms constrains patient’s lives as they never know when the next active phase is going to come; (3) how symptoms impact their body and mental wellbeing; (4) how symptoms lead to a sense of loss of body control (including sexuality); (5) whether they are likely to transmit the disease to their children; and (6) the long-term impact of the disease in terms of disability and risk of cancer [11].
Moreover, IBD has also been found to be associated with an increased incidence of mental health problems (e.g., anxiety and depression) when compared to the general population [12,13]. Depression, in particular, is thought to be an inflammatory trigger and to influence the clinical expression of IBD; while, in turn, inflammatory processes and related symptomatology seem to lead to increased levels of depression, therefore establishing a self-perpetuating loop [14,15].
There is a growing body of evidence suggesting that several psychological variables, which are potentially modifiable, contribute to IBD outcomes such as QoL or depression [16,17,18]. One such variable is gastrointestinal-specific anxiety (GSA), which could be defined as “the cognitive, affective and behavioural response stemming from fear of gastrointestinal sensations and symptoms and the context in which [they] occur” [19]. GSA is commonly associated with experiences of hypervigilance, fear, worry, or somatic hypersensitivity, along with the use of avoidance behaviors regarding situations associated with gastrointestinal functioning (e.g., meals outside the house, places with limited access to toilets) [19]. GSA has mainly been studied in the context of irritable bowel syndrome (IBS) and has shown to be related to both depression and quality of life [20]. However, recently, GSA has also been applied in the context of IBD. For example, higher levels of GSA have been shown to be associated with higher levels of pain and nausea in patients with IBD preparing for a colonoscopy [21]. GSA has also been shown to be higher in patients with IBD when compared to healthy controls (but not higher than IBS controls) and to be associated with higher levels of general anxiety and lower QoL [22]. Finally, GSA has also been shown to reduce when patients with IBD undergo psychological interventions, which indicates that it can be a changeable target in the management of IBD [23].
Perceived disability (PD), defined as the sense of limitation and disability an individual senses in multiple domains of daily functioning (e.g., social, occupational, recreation, self-care, physical, and sexual), has also been proposed as an important factor contributing to better adjustment in IBD [24]. Higher levels of PD have been shown to be related to lower levels of QoL, higher levels of depression, and higher associated health care costs [24,25]. Although PD tends to reduce across the life-span as patients adjust to the management of their IBD, it is still significantly higher than healthy controls and a major therapeutic target in the management of IBD [26,27]. The major predictors of PD levels seem to be both psychological factors and the length of the active disease [27,28].
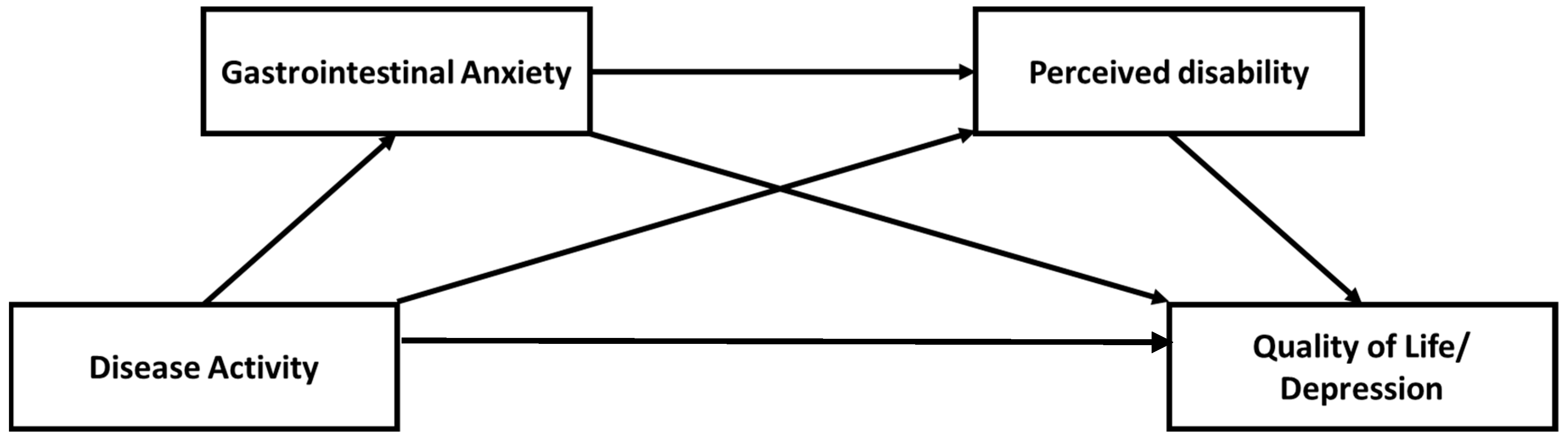
In this study, a theoretically driven model was hypothesized to explain the role that both GSA and PD might play in how IBD disease activity relates to the outcomes of QoL or depression. More specifically, it was hypothesized that the experiences of disease activity are likely to activate a gastrointestinal-specific anxiety response due to the nature of the symptoms, which is likely to lead to engagement with an avoidant type of behavior. This avoidant behavior is likely to be perceived as a form of disability provoked by the disease, which is then likely to affect QoL or experiences of depression (see Figure 1 for a depiction of the model). Therefore, this study hypothesized that GSA and PD would serially mediate the relationship between disease activity and the outcomes of Qol or depression.
2. Methods
2.1. Participants
Data were obtained from a convenience sample of participants with self-reported diagnosis of IBD. Participants had to be 16 years of age or older (age of consent in Scotland at the time of data collection) to have received their diagnosis from a medical practitioner and not to have any self-reported comorbidities such as dyspepsia or IBS.
2.2. Measures
Disease activity: Disease activity was measured with a self-assessment question developed specifically for this study. The question asked participants if they considered, in the last year, their disease to have been rarely active/in remission (1); sometimes/occasionally active (2); constantly or often active (3). The higher the score, the more the participant experiences their disease to be active.
Gastrointestinal-specific anxiety: Visceral Sensitivity Index (VSI) [19]. The Visceral Sensitivity Index is a 15-item instrument designed to measure gastrointestinal symptom-specific anxiety on a 6-item Likert scale ranging from 1 (strongly agree) to 6 (strongly disagree). The scale assesses fear-related psychological and behavioral responses to visceral symptoms and the context in which they arise. Higher scores convey greater GI-related anxiety. The scale has good internal consistency (α = 0.92), content, and predictive validity [19,22].
Perceived disability: Perceived Disability Scale (PDS) [29]. The PDS is a 10-item questionnaire that assesses perceived limitations and disability associated with tasks of daily living. Patients report their current level of disability on a 10-item Likert scale ranging from 0 (no disability) to 10 (total disability). Scores range from 0 to 100, with higher scores indicating greater perceived disability. It has been found to have good psychometric properties [24] for use with individuals with IBD (α = 0.92).
Psychological functioning: Depression Scale of the short-form Depression Anxiety and Stress Scales (DASS 21) [30]. The Depression Scale of the DASS 21 is a 7-item questionnaire designed to measure the negative emotional and physical states of depression on a 4-item Likert scale ranging from 0 (never) to 3 (almost always). It has been found to have good psychometric properties [30] (α = 0.93).
Quality of Life: UK Inflammatory Bowel Disease Questionnaire (IBDQ) [31]. The UK IBDQ is a 32-item measure that assesses health-related QoL specifically in patients with IBD. Patients are asked to respond to questions indicating the extent to which they experience a particular bowel problem and how it has affected their life. Scores reflect symptom severity and QoL on four domains: gastrointestinal and systemic symptoms, and emotional and social functioning. It has been found to be a reliable and valid measure of IBD [31] (α = 0.94).
2.3. Procedures
An exploratory cross-sectional design was used. Participants were recruited through the IBD charity “Crohn’s and Colitis UK”. This was accomplished by advertising on their website and using their research social media pages (and through their respective regional groups). The research was also advertised on other social media forums used by those with an IBD diagnosis, including “IBD Sucks” and “Crohn’s Zone”. A Web-based questionnaire was designed using the secure third-party survey provider “Bristol Online Survey” and was embedded in a custom HTML website introducing the study to participants. This data collection methodology was deemed appropriate as Internet use among those with IBD has been found to be high (81%) and individuals with IBD are likely to use the Internet to find out information about their diagnosis [32].
2.4. Statistical Analyses
All analyses were completed using SPSS, version 25. Preliminary analyses included a one-way ANOVA to compare different types of IBD across all variables of interest and an exploratory correlation analysis to investigate the association between the variables of interest. For the serial mediation model, the PROCESS v3 macro for SPSS, model 6 was used [33]. This model estimates (i) the direct (disease activity quality of life/depression) and ii) indirect (disease activity → gastrointestinal-specific anxiety → perceived disability → quality of life/depression) pathways. Ordinary least squared (OLS) regression-based path analysis was employed to test this hypothesis. Unstandardized regression coefficients were estimated as recommended in Hayes [33], quantifying each step of the hypothesised model. For statistical inference, bootstrapped 95% confidence intervals were constructed for each estimate [33]. Bootstrapping samples were set to 5000, and those which straddled zero were considered insignificant.
3. Results
3.1. Descriptive Statistics
The final sample included 320 individuals with IBD (N = 265, 82.8% females; N = 55 males, 17.2%). The majority were between 25 and 34 years old (N = 198, 30.6%) and were married or in a domestic partnership (N = 161, 50.3%). Most had a self-reported diagnosis of CD (N = 195, 60.9%) or UC (N = 125, 39.1%). Of the participants, 283 (88.5%) were diagnosed one or more years ago and 141 (44.1%) experienced constantly or often-active disease (see Table 1 for sample characteristics). The percentage of missing data in the demographic variables was minimal even though this part of the online questionnaire had no forced entry requirement.
3.2. Preliminary Analyses
There were no missing data regarding the variables of interest for the study as the online questionnaire had a forced completion option. Boxplots were plotted for all outcome variables, and screening the data did not reveal any outliers. Normality was checked and all assumptions were met. An independent samples t-test was conducted comparing the main variables of interest across the different IBD diagnoses. No significant statistical differences were found for any of the variables of interest across CD and UC. Zero order correlations show all variables of interest to be related to each other in a theoretically consistent manner (Table 2).
3.3. Serial Mediation
A model of serial mediation (Table 3) confirmed the significance of the direct effect of disease activity on QoL but not depression. The indirect regression paths via GSA or PD find each step in the hypothesized mediation to be significant for both outcomes of QoL and depression; that is, the relation between perceived disease activity and each of the outcomes is mediated by their gastrointestinal-specific anxiety or perceived disability. Finally, the serially mediated path through GSA and PD was found to be significant in mediating both the relationship between disease activity and QoL and disease activity and depression. Practically, this means that as disease activity increases, so does GSA, which leads to a perception of higher disability which then leads to an experience of either lower quality of life or higher depressive symptoms. These results are particularly relevant regarding the outcome of depression as they highlight that the relation between disease activity and depression is fully mediated by either GSA or PD individually or in a serial manner. Therefore, this might indicate that depression in IBD is less dependent on the actual experience of symptoms but on how these are interpreted in light of the anxiety and disability they provoke.
4. Discussion
The present study aimed to investigate the serial mediational path composed of GSA and PD in the relationship between disease activity and the outcomes of QoL or depression. Our findings suggest that we can retain our hypothesized model and propose that the experiences of disease activity are likely to activate a GSA response due to the nature of the symptoms and/or the treatment regimen, which is likely to lead to an increased sense of disability which ultimately impacts QoL or heightens the experience of depressive symptoms.
The literature on the role of GSA and PD in IBD is still in its infancy; therefore, there is a dearth of studies incorporating these variables, and to the author’s knowledge, no study has so far tried to investigate this type of more complex theoretically derived model. However, the findings presented in this study do agree with what we know so far about GSA and PD in IBD and add significantly to the literature on the field of psychogastroenterology as a whole.
Regarding PD, only one study [24] has looked into this construct as presented in this paper. Similarly, the findings of the present study also show medium-to-large correlations between the experience of PD and QoL. Further to this, the study by Kiebles and colleagues [24] has also identified associations between PD and a global measure of psychological distress that taps into depression; therefore, the correlation shown in our study between PD and depression further extends the previous findings. More recent studies [27,28] have also tapped into this construct using slightly different methods of assessing it; however, the key role that disease activity and psychological factors (in this case GSA) play in PD were reproduced. Although PD was formulated in this study as being part of a causal path of events leading to QoL or depression, the results from our study confirm the importance of PD as an outcome on its own right, as highlighted in the recent update for Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE-II) [34].
Regarding GSA, it has been associated with lower QoL [22] and higher depression and disease activity [18]. Again, the findings from this study mirror those of previous studies, with similar medium-to-large correlations being found. It is, however, important to note that in the study by Trieschman and colleagues [22], the main focus of the study was to validate the use of the Visceral Sensitivity Index [19] in an IBD population, and that the reported finding regarding the influence of GSA on QoL was not the main aim of the study, so no confounding variables were checked or taken into account. Regarding the study by Bessissow and colleagues [21], the findings were related to the very-specific situation of a sample of patients with IBD undergoing full bowel cleansing in preparation for a colonoscopy. Therefore, the results from this study might not reflect the day-to-day experience of the patients, only their reaction to a specific context. In light of these notes, it is possible to say that the current study might be more representative of the experience of patients with IBD and more robust in its findings given that it accounts for more related variables. It is, however, encouraging that as a process variable, GSA seems to have a similar role in the development of problems with QoL as observed in IBS populations [35]; it can be specifically targeted through several types of psychological interventions (e.g., [36]).
A further interesting finding of this study relates to the relationship between disease activity and depressive symptoms. Although studies suggest increased disease activity to be connected to increased levels of depression [37,38], this direct effect disappeared in the presence of the proposed mediators of GSA and PD. This suggests that the path between disease activity and depressive symptomatology is likely more complex than a simple direct relationship. In fact, several other studies have observed a similar pattern of this relationship being better explained through the introduction of psychologically relevant mediators such as illness-related shame [39] or emotion regulation [40]. Therefore, one can posit that the context in which the activity of the disease is experienced in the light of a complex psychological system is more relevant in predicting depressive symptomatology than just the level of activity on its own.
Finally, it is important to note the utility of this study in the development of future treatment interventions. The findings provide a potential pathway for topics to be addressed in psychological interventions for IBD. Psychotherapeutic interventions already address aspects related to anxiety, depression, and quality of life in IBD; however, the efficacy of these interventions is still debatable [41]. A recent meta-analysis [42] highlights the usefulness of psychological interventions with regard to the short-term relief of depression, anxiety, stress, and improvement in QoL; however, the quality of the evidence is still marred by high degrees of bias. Some psychotherapy models, however, seem to hold more promise in the light of the current study’s findings. For example, cognitive behavioral therapy has already been shown to be able to reduce GSA in an IBD sample [23] and to improve depression and QoL [42]. In fact, more recent advancements in behaviorally informed interventions such as acceptance and commitment therapy (ACT), which places a great focus on behavioral activation, might be decisive in addressing the issues regarding perceived disability. In a series of recent studies [43,44,45], ACT was found to improve stress, depression, and general wellbeing through an increase in psychological flexibility defined as the degree to which patients were able to adjust their behavior to engage in more highly valued activities in the presence of difficult experiences (physiological, cognitive, and emotional). Therefore, the current model tested in this study could provide a blueprint for a targeted combination of CBT and ACT that would be more suited to patients with IBD.
5. Strengths and Limitations
As a strength, this study recruited a healthy sized sample (when compared to previous studies on the role of psychosocial variables in IBD) and used robust analyses to test a theoretically driven model. Further to this, the sample seems to mirror the demographic characteristics usually seen in clinical practice, lending, therefore, to a greater applicability of the findings in applied settings. There are, however, some limitations worth noting. The conclusions drawn from the present study should be seen as tentative and as a useful model for further exploration. This is mainly due to the single time-point, cross-sectional nature of the data, which curtails any causal inferences. Future studies should investigate models incorporating longitudinal data operationalizing the hypothesized mediators in order to increase the explanatory power of the serial mediation model. Also, given a lack of a comparator group (e.g., healthy controls), it is still difficult to provide a strong case for causal inference. Due to data collection being made exclusively online and through a specific charitable organization, a significant part of the population with IBD who do not have access to either the Internet or to Crohn’s and Colitis UK’s newsletter would have been excluded. Further to this, the online data collection method also precluded checks for language understanding and potential comorbidities that might affect cognitive functioning. Also, disease activity measurement was based only on purely self-reported data, with no clinical confirmation. Therefore, the authors recognize that this is a self-selected sample. However, as mentioned above, the sample seems to broadly mirror most patients seen in clinical practice. Finally, there are a number of variables (e.g., resilience, medication adherence) that were not accounted for and which could be responsible for epiphenomenal association, determining the observed relationships in our results, or which could alternatively mediate/moderate the relationship between disease activity and QoL or depression.
6. Conclusions
The present study presents a more advantageous theoretically driven model for understanding the role of some key psychosocial variables in the experience of patients with IBD. The findings give a more comprehensive picture of the interaction between GSA and PD in the relationship between disease activity and the outcomes of QoL and depression. This could pave the way for more effective models in predicting the outcome of IBD and for individually tailored treatments. The present study takes tentative steps toward reframing how we conceptualize psychological variables in IBD and adds weight to the rationale behind the assessment and interventional targeting of these constructs in clinical contexts.
Author Contributions
A.S.—Data collection, initial analyses, manuscript draft feedback; N.F.—Conceptualization, Supervision, Manuscript draft, Statistical analyses. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the Department of Clinical and Health Psychology of the University of Edinburgh (16 June 2015).
Informed Consent Statement
All participants were informed of the nature of the study and the voluntarily nature of their participation. All participants signed a consent form indicating the above-stated.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
The authors would like to acknowledge the help of Crohn’s and Colitis UK in the dissemination of invitations to participate in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, R.; Li, Z.; Liu, S.; Zhang, D. Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: A systematic analysis based on the Global Burden of Disease Study 2019. BMJ Open 2023, 13, e065186. [Google Scholar] [CrossRef]
- Sairenji, T.; Collins, K.L.; Evans, D.V. An Update on Inflammatory Bowel Disease. Prim. Care 2017, 44, 673–692. [Google Scholar] [CrossRef]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef]
- Knowles, S.R.; Graff, L.A.; Wilding, H.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part I. Inflamm. Bowel Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef]
- Knowles, S.R.; Keefer, L.; Wilding, H.; Hewitt, C.; Graff, L.A.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part II. Inflamm. Bowel Dis. 2018, 24, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Larsson, K.; Lööf, L.; Rönnblom, A.; Nordin, K. Quality of life for patients with exacerbation in inflammatory bowel disease and how they cope with disease activity. J. Psychosom. Res. 2008, 64, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Adler, J.; Raju, S.; Beveridge, A.S.; Wang, S.; Zhu, J.; Zimmermann, E.M. College adjustment in University of Michigan students with Crohn’s and colitis. Inflamm. Bowel Dis. 2008, 14, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Kemp, K.; Griffiths, J.; Lovell, K. Understanding the health and social care needs of people living with IBD: A meta-synthesis of the evidence. World J. Gastroenterol. 2012, 18, 6240–6249. [Google Scholar] [CrossRef] [PubMed]
- Pittet, V.; Vaucher, C.; Froehlich, F.; Burnand, B.; Michetti, P.; Maillard, M.H.; Swiss IBD Cohort Study Group. Patient self-reported concerns in inflammatory bowel diseases: A gender-specific subjective quality-of-life indicator. PLoS ONE 2017, 12, e0171864. [Google Scholar] [CrossRef] [PubMed]
- Eugenicos, M.P.; Ferreira, N.B. Psychological factors associated with inflammatory bowel disease. Br. Med. Bull. 2021, 138, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Mikocka-Walus, A.; Knowles, S.R.; Keefer, L.; Graff, L. Controversies Revisited: A Systematic Review of the Comorbidity of Depression and Anxiety with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2016, 22, 752–762. [Google Scholar] [CrossRef]
- Martin-Subero, M.; Anderson, G.; Kanchanatawan, B.; Berk, M.; Maes, M. Comorbidity between depression and inflammatory bowel disease explained by immune-inflammatory, oxidative, and nitrosative stress; tryptophan catabolite; and gut-brain pathways. CNS Spectr. 2016, 21, 184–198. [Google Scholar] [CrossRef]
- Kredentser, M.S.; Graff, L.A.; Bernstein, C.N. Psychological Comorbidity and Intervention in Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2021, 55, 30–35. [Google Scholar] [CrossRef]
- Szigethy, E.M.; Allen, J.I.; Reiss, M.; Cohen, W.; Perera, L.P.; Brillstein, L.; Cross, R.K.; Schwartz, D.A.; Kosinski, L.R.; Colton, J.B.; et al. White Paper AGA: The Impact of Mental and Psychosocial Factors on the Care of Patients with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 986–997. [Google Scholar] [CrossRef]
- Moradkhani, A.; Beckman, L.J.; Tabibian, J.H. Health-related quality of life in inflammatory bowel disease: Psychosocial, clinical, socioeconomic, and demographic predictors. J. Crohns Colitis 2013, 7, 467–473. [Google Scholar] [CrossRef]
- Labus, J.S.; Bolus, R.; Chang, L.; Wiklund, I.; Naesdal, J.; Mayer, E.A.; Naliboff, B.D. The Visceral Sensitivity Index: Development and validation of a gastrointestinal symptom-specific anxiety scale. Aliment. Pharmacol. Ther. 2004, 20, 89–97. [Google Scholar] [CrossRef]
- Jerndal, P.; Ringström, G.; Agerforz, P.; Karpefors, M.; Akkermans, L.M.; Bayati, A.; Simrén, M. Gastrointestinal-specific anxiety: An important factor for severity of GI symptoms and quality of life in IBS. J. Neurogastroenterol. Motil. 2010, 22, 646-e179. [Google Scholar] [CrossRef] [PubMed]
- Bessissow, T.; Van Keerberghen, C.A.; Van Oudenhove, L.; Ferrante, M.; Vermeire, S.; Rutgeerts, P.; Van Assche, G. Anxiety is associated with impaired tolerance of colonoscopy preparation in inflammatory bowel disease and controls. J. Crohns Colitis 2013, 7, e580–e587. [Google Scholar] [CrossRef]
- Trieschmann, K.; Chang, L.; Park, S.; Naliboff, B.; Joshi, S.; Labus, J.S.; Sauk, J.S.; Limketkai, B.N.; Mayer, E.A. The visceral sensitivity index: A novel tool for measuring GI-symptom-specific anxiety in inflammatory bowel disease. J. Neurogastroenterol. Motil. 2022, 34, e14384. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.G.; Loftus, P.; Accardo, M.; Keenan, M.; Chen, L.; Osterman, M.T. Self-help Cognitive Behavioral Therapy Improves Health-Related Quality of Life for Inflammatory Bowel Disease Patients: A Randomized Controlled Effectiveness Trial. J. Clin. Psychol. Med. Settings 2020, 27, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Kiebles, J.L.; Doerfler, B.; Keefer, L. Preliminary evidence supporting a framework of psychological adjustment to inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, K.; Kapsoritakis, A.; Oikonomou, K.; Manolakis, A.; Tsakiridou, E.; Potamianos, S. Disability in Patients with Inflammatory Bowel Disease: Correlations with Quality of Life and Patient’s Characteristics. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6138105. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.S.; Hunt, M.G.; Brown, L.A.; Lewis, J.D. Inflammatory Bowel Diseases-related Disability: Risk Factors, Outcomes, and Interventions. Inflamm. Bowel Dis. 2023, izad182. [Google Scholar] [CrossRef] [PubMed]
- Israeli, E.; Graff, L.A.; Clara, I.; Walker, J.R.; Lix, L.M.; Targownik, L.E.; Bernstein, C.N. Low prevalence of disability among patients with inflammatory bowel diseases a decade after diagnosis. Clin. Gastroenterol. Hepatol. 2014, 12, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- van der Have, M.; Fidder, H.H.; Leenders, M.; Kaptein, A.A.; van der Valk, M.E.; van Bodegraven, A.A.; Dijkstra, G.; de Jong, D.J.; Pierik, M.; Ponsioen, C.Y.; et al. Self-reported disability in patients with inflammatory bowel disease largely determined by disease activity and illness perceptions. Inflamm. Bowel Dis. 2015, 21, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Beckman, N.; Turer, E.; Scherdell, T.; Dux, M.; Lofland, K. Long-term outcomes in chronic pain patients: The relationship between perceived disability, cognitive and affective factors, and adjustment. J. Pain 2008, 9 (Suppl. 2), 59. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef]
- Cheung, W.Y.; Garratt, A.M.; Russell, I.T.; Williams, J.G. The UK IBDQ-a British version of the inflammatory bowel disease questionnaire. development and validation. J. Clin. Epidemiol. 2000, 53, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.R.; Anderson, K.J.; Larson, D.W.; Dozois, E.J.; Hassan, I.; Sandborn, W.J.; Loftus, E.V.; Pemberton, J.H. Internet use by patients in an inflammatory bowel disease specialty clinic. Inflamm. Bowel Dis. 2007, 13, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; ISBN 9781462534654. [Google Scholar]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Bowers, H.; Gillanders, D.; Ferreira, N. Moderating effect of IBS acceptance on psychosocial mediators of Irritable Bowel Syndrome. J. Context. Behav. Sci. 2020, 16, 30–36. [Google Scholar] [CrossRef]
- Ferreira, N.B.; Gillanders, D.; Morris, P.G.; Eugenicos, M. Pilot study of acceptance and commitment therapy for irritable bowel syndrome: A preliminary analysis of treatment outcomes and processes of change. Clin. Psychol. (Aust. Psychol. Soc.) 2018, 22, 241–250. [Google Scholar] [CrossRef]
- Marrie, R.A.; Graff, L.A.; Fisk, J.D.; Patten, S.B.; Bernstein, C.N. The Relationship Between Symptoms of Depression and Anxiety and Disease Activity in IBD Over Time. Inflamm. Bowel Dis. 2021, 27, 1285–1293. [Google Scholar] [CrossRef]
- van den Brink, G.; Stapersma, L.; Vlug, L.E.; Rizopolous, D.; Bodelier, A.G.; van Wering, H.; Hurkmans, P.C.W.M.; Stuyt, R.J.L.; Hendriks, D.M.; van der Burg, J.A.T.; et al. Clinical disease activity is associated with anxiety and depressive symptoms in adolescents and young adults with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2018, 48, 358–369. [Google Scholar] [CrossRef]
- Trindade, I.A.; Ferreira, C.; Pinto-Gouveia, J. Chronic Illness-Related Shame: Development of a New Scale and Novel Approach for IBD Patients’ Depressive Symptomatology. Clin. Psyhcol. Psychot. 2017, 24, 255–263. [Google Scholar] [CrossRef]
- Trindade, I.A.; Ferreira, C.; Moura-Ramos, M.; Pinto-Gouveia, J. An 18-month study of the effects of IBD symptomatology and emotion regulation on depressed mood. Int. J. Colorectal Dis. 2017, 32, 651–660. [Google Scholar] [CrossRef]
- Timmer, A.; Preiss, J.C.; Motschall, E.; Rücker, G.; Jantschek, G.; Moser, G. Psychological interventions for treatment of inflammatory bowel disease. Cochrane Database Syst. Rev. 2011, CD006913. [Google Scholar] [CrossRef]
- Taft, T.H.; Ballou, S.; Bedell, A.; Lincenberg, D. Psychological Considerations and Interventions in Inflammatory Bowel Disease Patient Care. Gastroenterol. Clin. N. Am. 2017, 46, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Wynne, B.; McHugh, L.; Gao, W.; Keegan, D.; Byrne, K.; Rowan, C.; Hartery, K.; Kirschbaum, C.; Doherty, G.; Cullen, G.; et al. Acceptance and Commitment Therapy Reduces Psychological Stress in Patients with Inflammatory Bowel Diseases. Gastroenterology 2019, 156, 935–945.e1. [Google Scholar] [CrossRef] [PubMed]
- Lavelle, J.; Storan, D.; Eswara Murthy, V.; De Dominicis, N.; Mulcahy, H.E.; McHugh, L. Brief and Telehealth Acceptance and Commitment Therapy (ACT) Interventions for Stress in Inflammatory Bowel Disease (IBD): A Series of Single Case Experimental Design (SCED) Studies. J. Clin. Med. 2022, 11, 2757. [Google Scholar] [CrossRef] [PubMed]
- Romano, D.; Chesterman, S.; Fuller-Tyszkiewicz, M.; Evans, S.; Dober, M.; Gearry, R.; Gibson, P.R.; Knowles, S.; McCombie, A.; Eric, O.; et al. Feasibility, Acceptability, and Preliminary Efficacy of Acceptance Commitment Therapy for Adults Living with Inflammatory Bowel Disease and Distress. Inflamm. Bowel Dis. 2023, izad122. [Google Scholar] [CrossRef]
Figure 1.
Serial mediation model.


{kind=link}
Table 1.
Demographic characteristics of the sample.
| Variable | Number (N) | Percentage (%) | |
|---|---|---|---|
| Age (years) | 16–17 | 2 | 0.6 |
| 18–24 | 53 | 16.6 | |
| 25–34 | 98 | 30.6 | |
| 35–44 | 74 | 23.1 | |
| 45–54 | 56 | 17.5 | |
| 55–64 | 30 | 9.4 | |
| 55–64 | 6 | 1.9 | |
| 65–older | 1 | 0.3 | |
| Marital status | Married/domestic partnership | 161 | 50.3 |
| Single | 129 | 40.3 | |
| Divorced | 20 | 6.3 | |
| Separated | 4 | 1.3 | |
| Missing | 6 | 1.9 | |
| Diagnosis | CD | 195 | 60.9 |
| UC | 125 | 39.1 | |
| Time since diagnosis | <6 months–1 year ago | 35 | 10.9 |
| >1 years ago | 283 | 88.5 | |
| Missing | 2 | 0.6 | |
| Disease activity | Constantly or often active disease | 141 | 44.1 |
| Sometimes or occasionally active disease | 122 | 38.1 | |
| Rarely/in remission/absence of IBD symptoms | 57 | 17.8 |
Table 2.
Correlations between the model variables.
| IBDQ | DASS Dep | Disease Activity | VSI | |
|---|---|---|---|---|
| DASS Dep | −0.56 | - | - | - |
| Disease Activity | −0.50 | 0.22 | - | - |
| VSI | −0.46 | 0.38 | 0.22 | - |
| PDS | −0.56 | 0.46 | 0.31 | 0.34 |
Note: IBDQ—Inflammatory Bowel Disease Questionnaire; DASS Dep—Depression scale of the Depression Anxiety and Stress Scales; Disease Activity—self-reported disease activity; VSI—Visceral Sensitivity Index; PDS—Perceived Disability Scale. All p < 0.001.
Table 3.
Unstandardized regression coefficients for full proposed models of serial mediation.
| Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|
| Quality of Life | Depression | |||||||
| Coeff. | SE | p | 95% CI | Coeff. | SE | p | 95% CI | |
| Direct Effect | ||||||||
| DA→Outcome | −6.65 | 0.86 | <0.001 | −8.34; −4.96 | 0.80 | 0.75 | 0.29 | −0.68; 2.28 |
| Indirect Effect | ||||||||
| DA→GSA→Outcome | −1.15 | 0.39 | - | −1.99; −0.50 | 0.77 | 0.29 | - | 0.28; 1.42 |
| DA→PDS→Outcome | −1.42 | 0.48 | - | −2.81; −0.94 | 1.34 | 0.38 | - | 0.68; 2.17 |
| DA→GSA→PDS→Outcome | −0.46 | 0.16 | - | −0.80; −0.19 | 0.36 | 0.12 | - | 0.13; 0.59 |
Note: Standard errors and significance levels constructed from 5000 bootstrapped samples. DA—disease activity; GSA—gastrointestinal-specific anxiety; PDS—perceived disability.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Seaman, A.; Ferreira, N. Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease. Gastrointest. Disord. 2024, 6, 191-201. https://doi.org/10.3390/gidisord6010014
AMA Style
Seaman A, Ferreira N. Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease. Gastrointestinal Disorders. 2024; 6(1):191-201. https://doi.org/10.3390/gidisord6010014
Chicago/Turabian StyleSeaman, Angela, and Nuno Ferreira. 2024. "Investigating the Role of Gastrointestinal-Specific Anxiety and Perceived Disability in the Adjustment to Inflammatory Bowel Disease" Gastrointestinal Disorders 6, no. 1: 191-201. https://doi.org/10.3390/gidisord6010014