
Prospective Visual Inspection of the Ventrum of Tongue (VIVOT) Vasculature Predicts the Presence of Esophageal Varices
Abstract
:1. Introduction
2. Results
3. Methods
3.1. Patient Recruitment
3.2. Grading
4. Statistical Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meseeha, M.; Attia, M. Esophageal Varices. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK448078/ (accessed on 7 August 2023).
- Ge, P.S.; Runyon, B.A. Treatment of patients with cirrhosis. N. Engl. J. Med. 2016, 375, 767–777. [Google Scholar] [CrossRef]
- Sporea, I.; Raţiu, I.; Sirli, R.; Popescu, A.; Bota, S. Value of transient elastography for the prediction of variceal bleeding. World J. Gastroenterol. 2011, 17, 2206–2210. [Google Scholar] [CrossRef]
- Morishita, N.; Hiramatsu, N.; Oze, T.; Harada, N.; Yamada, R.; Miyazaki, M.; Yakushiji, T.; Miyagi, T.; Yoshida, Y.; Tatsumi, T.; et al. Liver stiffness measurement by acoustic radiation force impulse is useful in predicting the presence of esophageal varices or high-risk esophageal varices among patients with HCV-related cirrhosis. J. Gastroenterol. 2014, 49, 1175–1182. [Google Scholar] [CrossRef]
- Hashemi, H.S.; Reza, R.Z.; Salcudeana, S.E.; Rohling, R.N. Ultrafast Ultrasound Imaging for 3D Shear Wave Absolute Vibro-Elastography. arXiv 2023, arXiv:2203.13949. [Google Scholar]
- Pang, J.X.; Zimmer, S.; Niu, S.; Crotty, P.; Tracey, J.; Pradhan, F.; Shaheen, A.A.; Coffin, C.S.; Heitman, S.J.; Kaplan, G.G.; et al. Liver stiffness by transient elastography predicts liver-related complications and mortality in patients with chronic liver disease. PLoS ONE 2014, 9, e95776. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Baumgartner, K.; Bositis, C. Cirrhosis: Diagnosis and Management. Am. Fam. Physician 2019, 100, 759–770. [Google Scholar] [PubMed]
- Crossan, C.; Tsochatzis, E.A.; Longworth, L.; Gurusamy, K.; Davidson, B.; Rodríguez-Perálvarez, M.; Mantzoukis, K.; O’Brien, J.; Thalassinos, E.; Papastergiou, V.; et al. Cost-effectiveness of non-invasive methods for assessment and monitoring of liver fibrosis and cirrhosis in patients with chronic liver disease: Systematic review and economic evaluation. Health Technol. Assess. 2015, 19, 1–409, v–vi. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Ryou, M. Gastric varices. Curr. Opin. Gastroenterol. 2023, 39, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Beste, L.A.; Leipertz, S.L.; Green, P.K.; Dominitz, J.A.; Ross, D.; Ioannou, G.N. Trends in burden of cirrhosis and hepatocellular carcinoma by underlying liver disease in US veterans, 2001–2013. Gastroenterology 2015, 149, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for Liver Cirrhosis 2020. J. Gastroenterol. 2021, 56, 593–619. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Baveno VII Faculty. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Kochanek, K.D.; Murphy, S.L.; Xu, J.; Arias, E. Deaths: Final Data for 2017. Natl. Vital Stat. Rep. 2019, 68, 1–77. [Google Scholar] [PubMed]
- Li, L.; Yu, C.; Li, Y. Endoscopic band ligation versus pharmacological therapy for variceal bleeding in cirrhosis: A meta-analysis. Can. J. Gastroenterol. 2011, 25, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Tapper, E.B.; Ho, C.; Asrani, S.K.; Ovchinsky, N.; Poterucha, J.; Flores, A.; Ankoma-Sey, V.; Luxon, B.; Volk, M. Development of Quality Measures in Cirrhosis by the Practice Metrics Committee of the American Association for the Study of Liver Diseases. Hepatology 2019, 69, 1787–1797. [Google Scholar] [CrossRef]
- Meng, Y.; Liu, L.; Zheng, Y.; Li, L.; Liu, X.; Qin, J.; Xia, J.; Cui, D.; Liang, J.; Li, Z.; et al. Traditional Chinese Medicine Constitution Identification Based on Objective Facial and Tongue Features: A Delphi Study and a Diagnostic Nomogram for Blood Stasis Constitution. Evid. Based Complement. Alternat. Med. 2022, 2022, 6950529. [Google Scholar] [CrossRef]
- Sami, S.S.; Harman, D.; Ragunath, K.; Böhning, D.; Parkes, J.; Guha, I.N. Non-invasive tests for the detection of oesophageal varices in compensated cirrhosis: Systematic review and meta-analysis. United Eur. Gastroenterol. J. 2018, 6, 806–818. [Google Scholar] [CrossRef]
- Madhira, M.; Tobi, M. Isolated Gastrointestinal spider nevi: Potential clinical significance. Am. J. Gastroenterol. 2000, 95, 26–27. [Google Scholar] [CrossRef]
- Akhras, J.; Patel, P.; Tobi, M. Dieulafoy’s lesion-like bleeding: An under-recognized cause of upper gastrointestinal cause of upper gastrointestinal bleeding in patients with advanced liver disease. Dig. Dis. Sci. 2007, 52, 722–726. [Google Scholar] [CrossRef]
- Patel, P.; Tobi, M. Dieulafoy Lesion-like Bleeding: In the loop. Gastroenterol. Hepatol. 2011, 7, 271–274. [Google Scholar]
- Castiglione, U.; Curcio, M.; Salvaggio, S.; Vancheri, F. Presentazione atipica di ipertensione portale: Sanguinamento da varici della base della lingua [Hemoptysis from dorsal tongue base varices secondary to portal hypertension]. Recent. Prog. Med. 2001, 92, 756. [Google Scholar]
- Liu, Q.; Yue, X.Q.; Deng, W.Z.; Ren, R.Z. Quantitative study on tongue color in primary liver cancer patients by analysis system for comprehensive information of tongue diagnosis. Zhong Xi Yi Jie He Xue Bao 2003, 1, 180–183. [Google Scholar] [CrossRef]
- Jassar, P.; Jaramillo, M.; Nunez, D.A. Base of tongue varices associated with portal hypertension. Postgrad. Med. J. 2000, 76, 576–577. [Google Scholar] [CrossRef]
- Philips, A.C.; Sahney, A. Oesophageal and gastric varices: Historical aspects, classification and grading: Everything in one place. Gastroenterol. Rep. 2016, 4, 186–195. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Sanyal, A.J.; Grace, N.D.; Carey, W. Practice Guidelines Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology 2007, 46, 922–938. [Google Scholar] [CrossRef]
- Kanwal, F.; Khaderi, S.; Singal, A.G.; Marrero, J.A.; Loo, N.; Asrani, S.K.; Amos, C.I.; Thrift, A.P.; Gu, X.; Luster, M.; et al. Risk factors for HCC in contemporary cohorts of patients with cirrhosis. Hepatology 2023, 77, 997–1005. [Google Scholar] [CrossRef]
- Di Martino, V.; Simone, F.; Grasso, M.; Abdel-Hadi, Y.; Peralta, M.; Veneziano, M.; Lombardo, A.; Peralta, S.; Calvaruso, V. Child-Pugh class and not thrombocytopenia impacts the risk of complications of endoscopic band ligation in patients with cirrhosis and high risk varices. J. Pers. Med. 2023, 13, 764. [Google Scholar] [CrossRef]
- Ridola, L.; Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O. Hepatic Encephalopathy: Diagnosis and Management. J. Transl. Int. Med. 2020, 8, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Tobi, M.; Antaki, F.; Rambus, M.A.; Yang, Y.X.; Kaplan, D.; Rodriguez, R.; Maliakkal, B.; Majumdar, A.; Demian, E.; Tobi, Y.Y.; et al. The Non-Invasive Prediction of Colorectal Neoplasia (NIPCON) Study 1995–2022: A Comparison of Guaiac-Based Fecal Occult Blood Test (FOBT) and an Anti-Adenoma Antibody, Adnab-9. Int. J. Mol. Sci. 2023, 24, 17257. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.; Park, A.; Yakovchenko, V.; Rogal, S.; Chartier, M.; Morgan, T.R.; Ross, D. HCV Elimination in the US Department of Veterans Affairs. Clin. Liver Dis. 2021, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
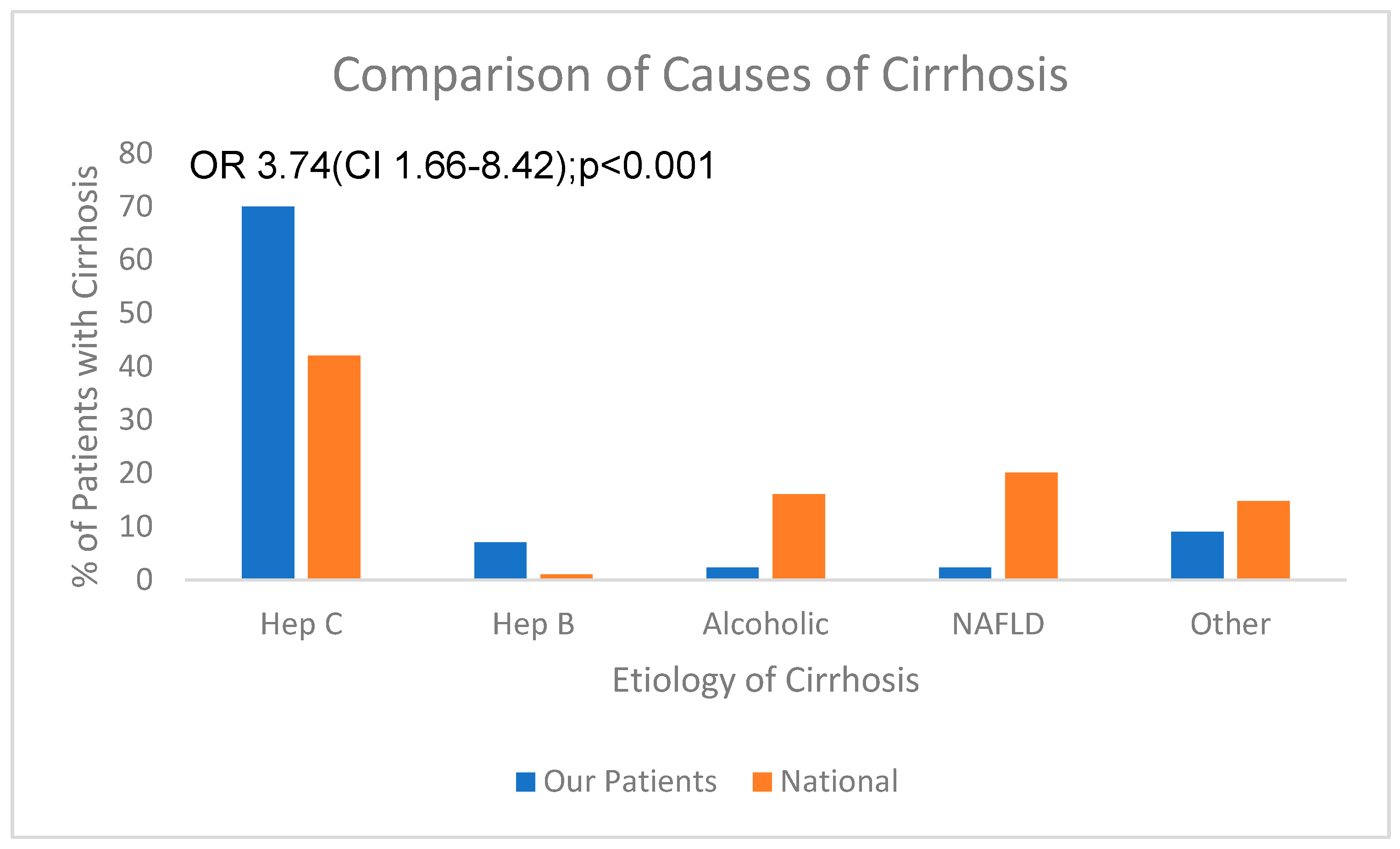
| Parameter | Total | % Male | % Ethnicity AA | % Varices+ | Mean Age * (yrs ± sd) |
|---|---|---|---|---|---|
| All Patients | 131 | 93 | 59 | 56 | 59.5 ± 5.4 |
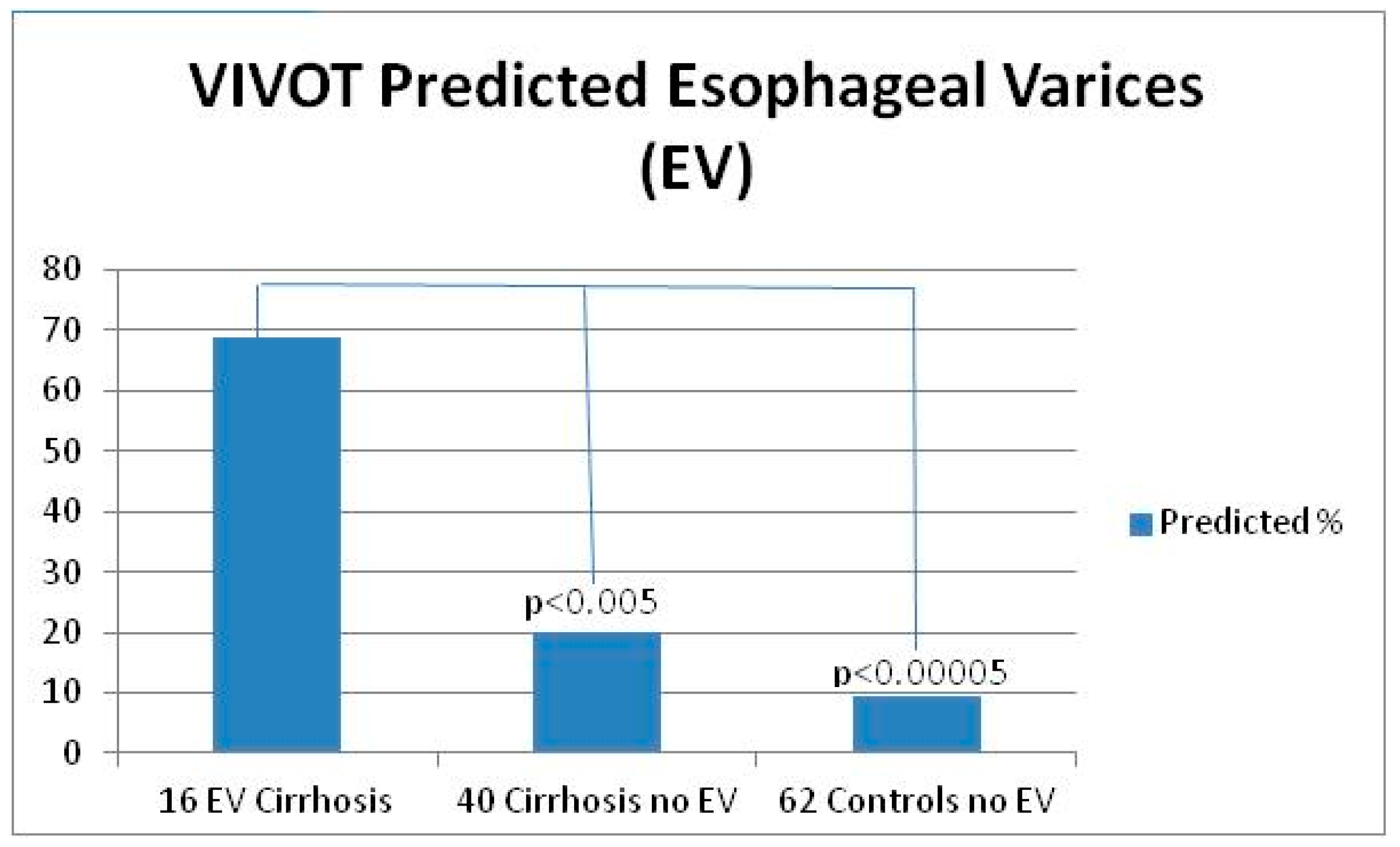
| Cirrhosis Group 1 | 59 | 100 | 39 | 32 (16 EV:3 GV) | 59.5 ± 5.4 |
| Control Group 2 | 62 | 86 | 53 | 0 | 59.0 ± 13 |
| Parameter | % Sensitivity | % Specificity | % Positive Predictive Value | % Negative Predictive Value |
|---|---|---|---|---|
| Group 1 | 69 | 80 | 59 | 84 |
| All Groups | 69 | 86.3 | 42 | 95 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
All patients undergoing any of the following:
|
|
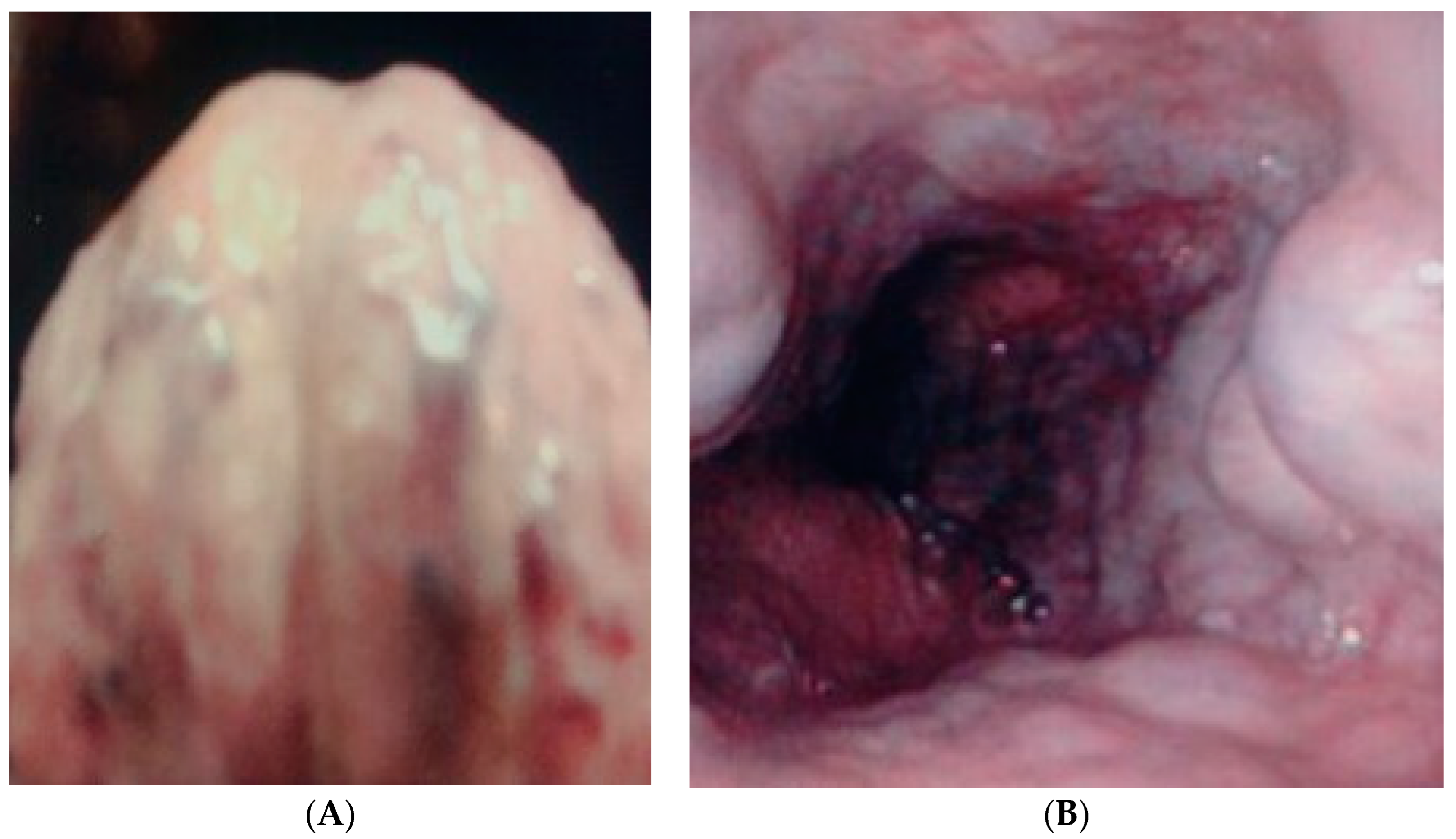
| Grading (Photograph by Ruler) | Varices (Continuous) |
|---|---|
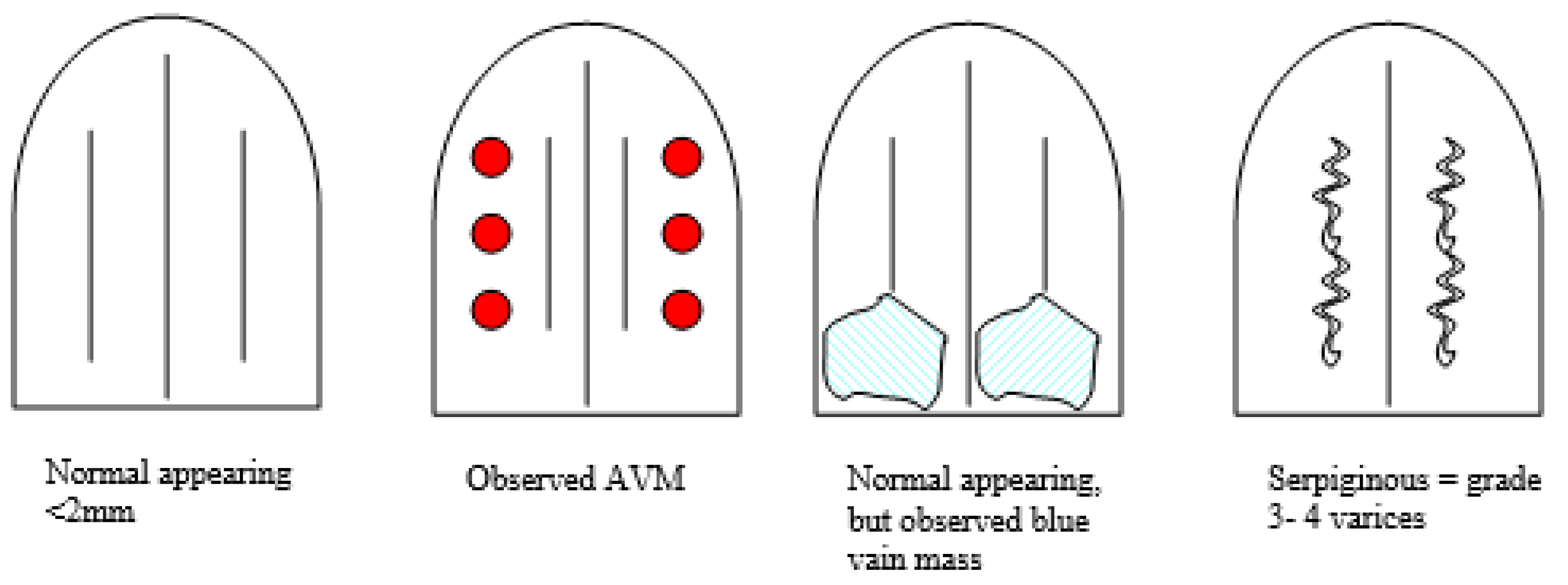
| Sublingual varices | 0—normal-appearing veins < 2 mm |
| (also see figures) | 1—normal but serpiginous |
| 2—veins > 2 mm | |
| 3—veins > 2 mm and serpiginous | |
| 4—dilated, serpiginous veins extending beyond borders of the frenulum continuous with varices | |
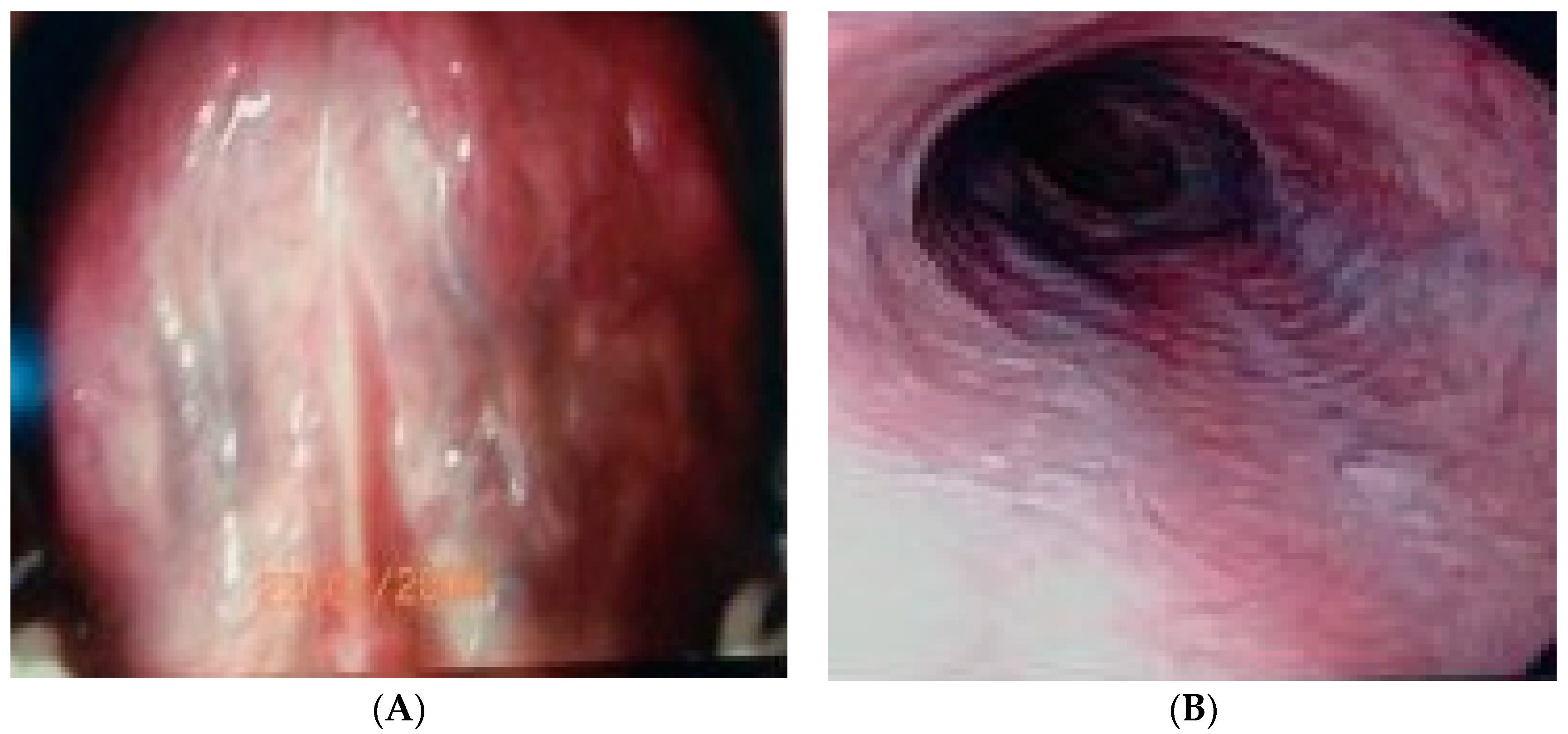
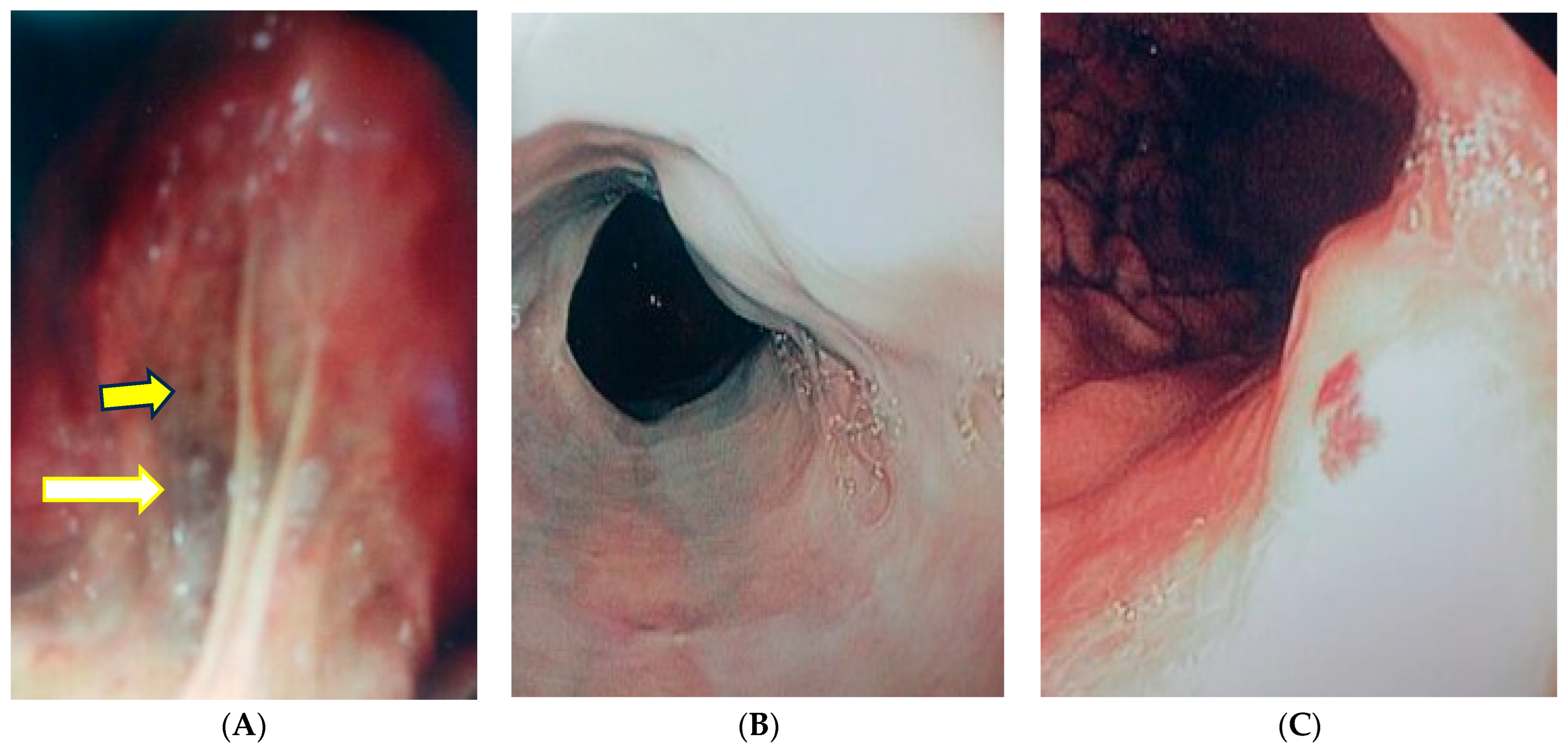
| Esophageal varices | 0—normal-appearing veins |
| (esophagus, stomach, | 1—normal ≥1 mm but <1 cm |
| duodenum, jejunum, and | 2—thin-walled, distended veins |
| ileum) | 3—varicosities, distended >1 cm |
| 4—distended approximately 2 cm | |
| Gastric varices GOV1 and GOV2, IGV1 and IGV2 by Sarin’s Method | 1—esophageal and gastric varices that extend to the lesser curvature 2—esophageal and gastric varices that extend to the greater curvature 1—isolated gastric (IGV1) alone, confined to the fundus 2—isolated gastric or duodenal varices (IGV2) |
| (by location) | |
| Duodenum | 0—none |
| 1—present regardless of size |
| Patients Use of NSBB | Elastography Criteria/Ascites | Platelet Criteria | Endoscopy (E) Indicated |
|---|---|---|---|
| Unable | Greater than 20 kPa/None | ≤150 × 109/L | Yes (C1, Section 2.19) |
| Unable but avoiding | Greater than 20 kPa/None | ≤150 × 109/L | Unchanged (D1, Section E 2.2) |
| Unable but avoiding | Less than 40 kPa/None | ≤150 × 109/L | No E (C2, Section E 2.2) |
| Hepatitis comp | Less than 14 kPa | ≤150 × 109/L | No E (B1, Section 3.7) |
| Able, treated | Less than 25 kPa (E 1–2 years) | N/A | E-cACLD E-ve; dcNSBB (C2, Section 3.9) |
| Able, comp | N/A | N/A | No E (B2, Section 5.7) |
| No NSBB/ascites | N/A | N/A | E-yes (B2, Section 7.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tobi, M.; Pascua, M.; Rodriguez, R.; Yang, Y.-X.; Lieb, J.; Weinstein, D.; Kaplan, D.E. Prospective Visual Inspection of the Ventrum of Tongue (VIVOT) Vasculature Predicts the Presence of Esophageal Varices. Gastrointest. Disord. 2024, 6, 230-240. https://doi.org/10.3390/gidisord6010017
Tobi M, Pascua M, Rodriguez R, Yang Y-X, Lieb J, Weinstein D, Kaplan DE. Prospective Visual Inspection of the Ventrum of Tongue (VIVOT) Vasculature Predicts the Presence of Esophageal Varices. Gastrointestinal Disorders. 2024; 6(1):230-240. https://doi.org/10.3390/gidisord6010017
Chicago/Turabian StyleTobi, Martin, Monina Pascua, Rebecca Rodriguez, Yu-Xiao Yang, John Lieb, Douglas Weinstein, and David E. Kaplan. 2024. "Prospective Visual Inspection of the Ventrum of Tongue (VIVOT) Vasculature Predicts the Presence of Esophageal Varices" Gastrointestinal Disorders 6, no. 1: 230-240. https://doi.org/10.3390/gidisord6010017