
Diabetic Gastroparesis: Navigating Pathophysiology and Nutritional Interventions

 , , , , , , , ,
, , , , , , , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Epidemiology
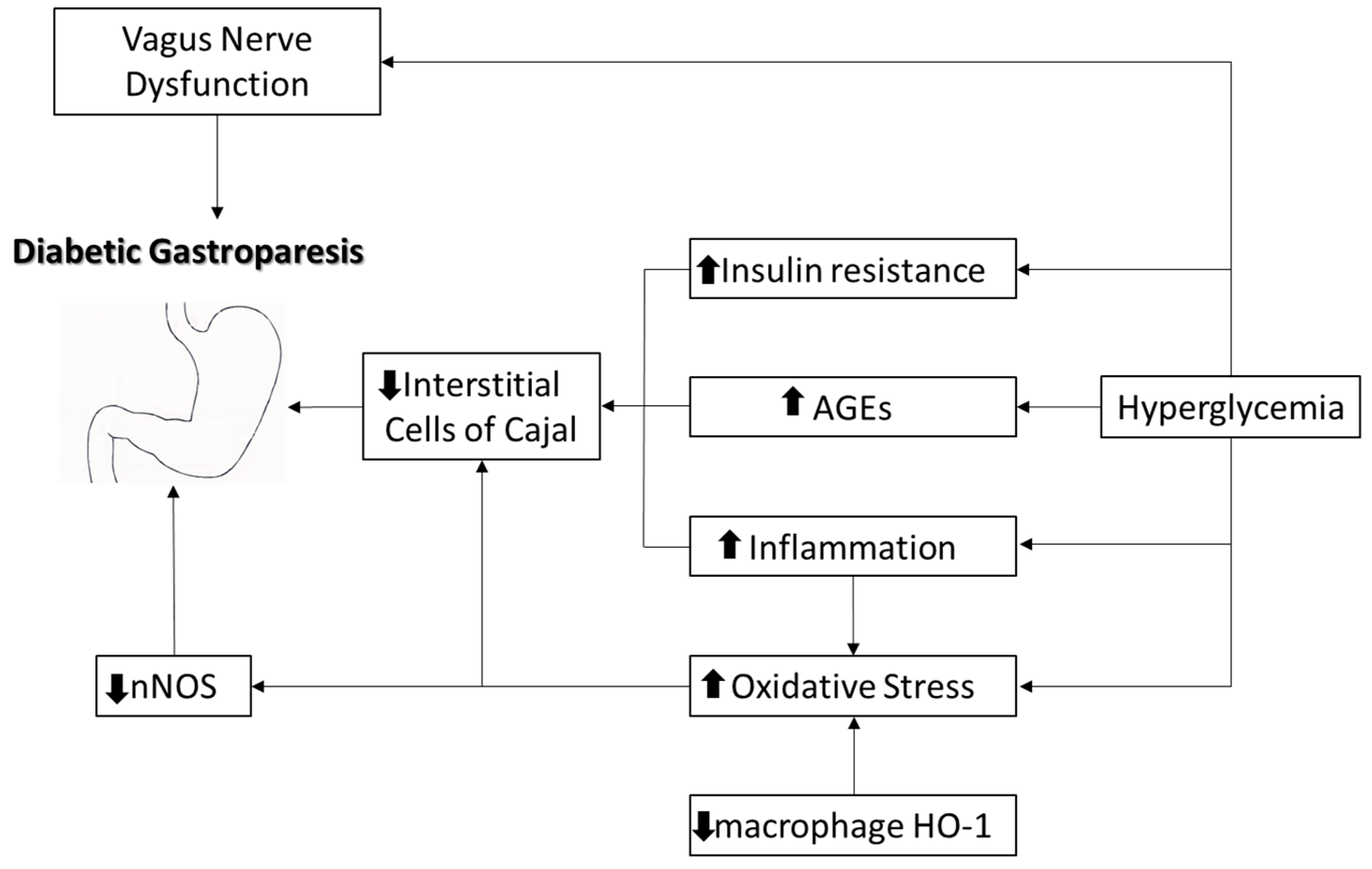
3. Pathophysiology
3.1. Gastric Motility Physiology
3.2. Diabetic Gastroparesis
3.3. Gender Difference
3.3.1. Sex Hormones
3.3.2. Nitric Oxide Signaling
3.3.3. Serotoninergic Signaling
3.3.4. Interstitial Cells of Cajal
4. Diagnosis
5. Differential Diagnosis
6. Effects of Diabetic Gastroparesis on Glycemia
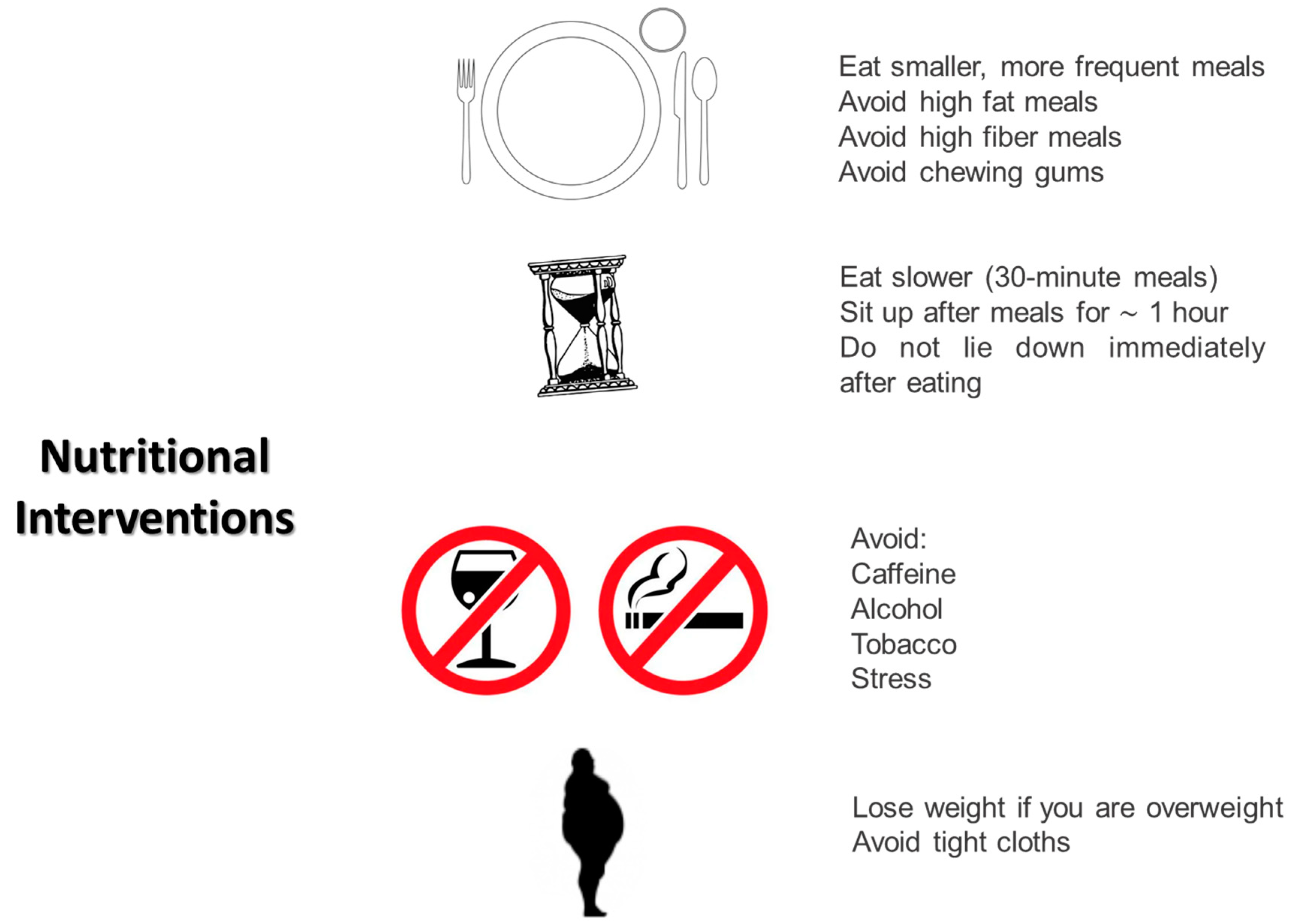
7. Nutritional Management of Diabetic Gastroparesis
- Eating smaller and more frequent meals;
- Eating slowly (30 min meals);
- Avoiding the supine position for at least the first hour after a meal;
- Sleeping with the head elevated 6–8 inches from the bed to minimize reflux;
- Avoiding tight clothes that could compress the abdomen;
- Avoiding meals in the later part of the day;
- Avoiding fats and fibers;
- Avoiding chewing gums that increase air swallowing;
- Avoiding CATS: caffeine, alcohol, tobacco, and stress;
- Avoiding all foods that can reduce lower esophageal sphincter pressure: peppermint, chocolate, fat, and caffeine.
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bharucha, A.E.; Kudva, Y.C.; Prichard, D.O. Diabetic Gastroparesis. Endocr. Rev. 2019, 40, 1318–1352. [Google Scholar] [CrossRef]
- Ahmed, M.S.O.; Forde, H.; Smith, D. Diabetic gastroparesis: Clinical features, diagnosis and management. Ir. J. Med. Sci. 2023, 192, 1687–1694. [Google Scholar] [CrossRef]
- Zahid, S.A.; Tated, R.; Mathew, M.; Rajkumar, D.; Karnik, S.B.; Pramod Roy, A.; Jacob, F.P.; Baskara Salian, R.; Razzaq, W.; Shivakumar, D.; et al. Diabetic Gastroparesis and its Emerging Therapeutic Options: A Narrative Review of the Literature. Cureus 2023, 15, e44870. [Google Scholar] [CrossRef]
- Li, L.; Wang, L.; Long, R.; Song, L.; Yue, R. Prevalence of gastroparesis in diabetic patients: A systematic review and meta-analysis. Sci. Rep. 2023, 13, 14015. [Google Scholar] [CrossRef]
- Jung, H.K.; Choung, R.S.; Locke, G.R., 3rd; Schleck, C.D.; Zinsmeister, A.R.; Szarka, L.A.; Mullan, B.; Talley, N.J. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology 2009, 136, 1225–1233. [Google Scholar] [CrossRef]
- Pafundi, P.C.; Garofalo, C.; Galiero, R.; Borrelli, S.; Caturano, A.; Rinaldi, L.; Provenzano, M.; Salvatore, T.; De Nicola, L.; Minutolo, R.; et al. Role of Albuminuria in Detecting Cardio-Renal Risk and Outcome in Diabetic Subjects. Diagnostics 2021, 11, 290. [Google Scholar] [CrossRef]
- Petri, M.; Singh, I.; Baker, C.; Underkofler, C.; Rasouli, N. Diabetic gastroparesis: An overview of pathogenesis, clinical presentation and novel therapies, with a focus on ghrelin receptor agonists. J. Diabetes Complicat. 2021, 35, 107733. [Google Scholar] [CrossRef]
- Goyal, R.K.; Guo, Y.; Mashimo, H. Advances in the physiology of gastric emptying. Neurogastroenterol. Motil. 2019, 31, e13546. [Google Scholar] [CrossRef] [PubMed]
- Ibba Manneschi, L.; Pacini, S.; Corsani, L.; Bechi, P.; Faussone-Pellegrini, M.S. Interstitital cells of Cajal in the human stomach: Distribution and relationship with enteric innervation. Histol. Histopathol. 2004, 19, 1153–1164. [Google Scholar] [PubMed]
- Harvey, R.F. Hormonal control of gastrointestinal motility. Am. J. Dig. Dis. 1975, 20, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Bharucha, A.E.; Farrugia, G. Epidemiology, mechanisms, and management of diabetic gastroparesis. Clin. Gastroenterol. Hepatol. 2011, 9, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Dockray, G.J. Gastrointestinal hormones and the dialogue between gut and brain. J. Physiol. 2014, 592, 2927–2941. [Google Scholar] [CrossRef] [PubMed]
- Samsom, M.; Roelofs, J.M.; Akkermans, L.M.; van Berge Henegouwen, G.P.; Smout, A.J. Proximal gastric motor activity in response to a liquid meal in type I diabetes mellitus with autonomic neuropathy. Dig. Dis. Sci. 1998, 43, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Gaddipati, K.V.; Simonian, H.P.; Kresge, K.M.; Boden, G.H.; Parkman, H.P. Abnormal ghrelin and pancreatic polypeptide responses in gastroparesis. Dig. Dis. Sci. 2006, 51, 1339–1346. [Google Scholar] [CrossRef]
- Buysschaert, M.; Donckier, J.; Dive, A.; Ketelslegers, J.M.; Lambert, A.E. Gastric acid and pancreatic polypeptide responses to sham feeding are impaired in diabetic subjects with autonomic neuropathy. Diabetes 1985, 34, 1181–1185. [Google Scholar] [CrossRef]
- Guy, R.J.; Dawson, J.L.; Garrett, J.R.; Laws, J.W.; Thomas, P.K.; Sharma, A.K.; Watkins, P.J. Diabetic gastroparesis from autonomic neuropathy: Surgical considerations and changes in vagus nerve morphology. J. Neurol. Neurosurg. Psychiatry 1984, 47, 686–691. [Google Scholar] [CrossRef]
- Schmidt, R.E.; Green, K.G.; Snipes, L.L.; Feng, D. Neuritic dystrophy and neuronopathy in Akita (Ins2(Akita)) diabetic mouse sympathetic ganglia. Exp. Neurol. 2009, 216, 207–218. [Google Scholar] [CrossRef]
- Carroll, S.L.; Byer, S.J.; Dorsey, D.A.; Watson, M.A.; Schmidt, R.E. Ganglion-specific patterns of diabetes-modulated gene expression are established in prevertebral and paravertebral sympathetic ganglia prior to the development of neuroaxonal dystrophy. J. Neuropathol. Exp. Neurol. 2004, 63, 1144–1154. [Google Scholar] [CrossRef]
- Grover, M.; Farrugia, G.; Stanghellini, V. Gastroparesis: A turning point in understanding and treatment. Gut 2019, 68, 2238–2250. [Google Scholar] [CrossRef]
- Tashima, K.; Nishijima, M.; Fujita, A.; Kubomi, M.; Takeuchi, K. Acid secretory changes in streptozotocin-diabetic rats: Different responses to various secretagogues. Dig. Dis. Sci. 2000, 45, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Malagelada, J.R. Abnormal intestinal motility in diabetics with the gastroparesis syndrome. Eur. J. Clin. Investig. 1984, 14, 420–427. [Google Scholar] [CrossRef]
- Yang, S.; Wu, B.; Sun, H.; Sun, T.; Han, K.; Li, D.; Ji, F.; Zhang, G.; Zhou, D. Impaired insulin/IGF-1 is responsible for diabetic gastroparesis by damaging myenteric cholinergic neurones and interstitial cells of Cajal. Biosci. Rep. 2017, 37, BSR20170776. [Google Scholar] [CrossRef] [PubMed]
- Forster, J.; Damjanov, I.; Lin, Z.; Sarosiek, I.; Wetzel, P.; McCallum, R.W. Absence of the interstitial cells of Cajal in patients with gastroparesis and correlation with clinical findings. J. Gastrointestig. Surg. 2005, 9, 102–108. [Google Scholar] [CrossRef]
- Grover, M.; Bernard, C.E.; Pasricha, P.J.; Lurken, M.S.; Faussone-Pellegrini, M.S.; Smyrk, T.C.; Parkman, H.P.; Abell, T.L.; Snape, W.J.; Hasler, W.L.; et al. Clinical-histological associations in gastroparesis: Results from the Gastroparesis Clinical Research Consortium. Neurogastroenterol. Motil. 2012, 24, 531–539. [Google Scholar] [CrossRef]
- Grover, M.; Farrugia, G.; Lurken, M.S.; Bernard, C.E.; Faussone-Pellegrini, M.S.; Smyrk, T.C.; Parkman, H.P.; Abell, T.L.; Snape, W.J.; Hasler, W.L.; et al. Cellular changes in diabetic and idiopathic gastroparesis. Gastroenterology 2011, 140, 1575–1585. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, H.; Kajimura, M.; Osawa, S.; Kanaoka, S.; Furuta, T.; Ikuma, M.; Hishida, A. A deficiency of gastric interstitial cells of Cajal accompanied by decreased expression of neuronal nitric oxide synthase and substance P in patients with type 2 diabetes mellitus. J. Gastroenterol. 2006, 41, 1076–1087. [Google Scholar] [CrossRef]
- He, C.L.; Soffer, E.E.; Ferris, C.D.; Walsh, R.M.; Szurszewski, J.H.; Farrugia, G. Loss of interstitial cells of Cajal and inhibitory innervation in insulin-dependent diabetes. Gastroenterology 2001, 121, 427–434. [Google Scholar] [CrossRef]
- Young, R.L.; Chia, B.; Isaacs, N.J.; Ma, J.; Khoo, J.; Wu, T.; Horowitz, M.; Rayner, C.K. Disordered control of intestinal sweet taste receptor expression and glucose absorption in type 2 diabetes. Diabetes 2013, 62, 3532–3541. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M. Gastrointestinal hormones and regulation of gastric emptying. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 3–10. [Google Scholar] [CrossRef]
- Meldgaard, T.; Olesen, S.S.; Farmer, A.D.; Krogh, K.; Wendel, A.A.; Brock, B.; Drewes, A.M.; Brock, C. Diabetic enteropathy: From molecule to mechanism-based treatment. J. Diabetes Res. 2018, 2018, 3827301. [Google Scholar] [CrossRef]
- Gangula, P.R.; Maner, W.L.; Micci, M.A.; Garfield, R.E.; Pasricha, P.J. Diabetes induces sex-dependent changes in neuronal nitric oxide synthase dimerization and function in the rat gastric antrum. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 292, G725–G733. [Google Scholar] [CrossRef]
- Gangula, P.R.; Sekhar, K.R.; Mukhopadhyay, S. Gender bias in gastroparesis: Is nitric oxide the answer? Dig. Dis. Sci. 2011, 56, 2520–2527. [Google Scholar] [CrossRef]
- Daff, S. NO synthase: Structures and mechanisms. Nitric Oxide 2010, 23, 1–11. [Google Scholar] [CrossRef]
- Yamamoto, I.; Fujimura, M.; Kihara, N.; Kumano, K.; Yamada, T.; Yamamoto, H.; Fujimiya, M. Nitric oxide formation in the dog sphincter of Oddi from nitric oxide donors as measured with in vivo micro-dialysis. Aliment. Pharmacol. Ther. 2000, 14, 1095–1101. [Google Scholar] [CrossRef]
- Takahashi, T. Pathophysiological significance of neuronal nitric oxide synthase in the gastrointestinal tract. J. Gastroenterol. 2003, 38, 421–430. [Google Scholar] [CrossRef]
- Huang, P.L.; Dawson, T.M.; Bredt, D.S.; Snyder, S.H.; Fishman, M.C. Targeted disruption of the neuronal nitric oxide synthase gene. Cell 1993, 75, 1273. [Google Scholar] [CrossRef]
- Plourde, V.; Quintero, E.; Suto, G.; Coimbra, C.; Taché, Y. Delayed gastric emptying induced by inhibitors of nitric oxide synthase in rats. Eur. J. Pharmacol. 1994, 256, 125–129. [Google Scholar] [CrossRef]
- Takahashi, T.; Nakamura, K.; Itoh, H.; Sima, A.A.; Owyang, C. Impaired expression of nitric oxide synthase in the gastric myenteric plexus of spontaneously diabetic rats. Gastroenterology 1997, 113, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Watkins, C.C.; Sawa, A.; Jaffrey, S.; Blackshaw, S.; Barrow, R.K.; Snyder, S.H.; Ferris, C.D. Insulin restores neuronal nitric oxide synthase expression and function that is lost in diabetic gastropathy. J. Clin. Investig. 2000, 106, 803. [Google Scholar] [CrossRef] [PubMed]
- Cellek, S. Point of NO return for nitrergic nerves in diabetes: A new insight into diabetic complications. Curr. Pharm. Des. 2004, 10, 3683–3695. [Google Scholar] [CrossRef] [PubMed]
- Caturano, A.; D’Angelo, M.; Mormone, A.; Russo, V.; Mollica, M.P.; Salvatore, T.; Galiero, R.; Rinaldi, L.; Vetrano, E.; Marfella, R.; et al. Oxidative Stress in Type 2 Diabetes: Impacts from Pathogenesis to Lifestyle Modifications. Curr. Issues Mol. Biol. 2023, 45, 6651–6666. [Google Scholar] [CrossRef] [PubMed]
- Galiero, R.; Caturano, A.; Vetrano, E.; Beccia, D.; Brin, C.; Alfano, M.; Di Salvo, J.; Epifani, R.; Piacevole, A.; Tagliaferri, G.; et al. Peripheral Neuropathy in Diabetes Mellitus: Pathogenetic Mechanisms and Diagnostic Options. Int. J. Mol. Sci. 2023, 24, 3554. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.M.; Gibbons, S.J.; Nguyen, T.V.; Stoltz, G.J.; Lurken, M.S.; Ordog, T.; Szurszewski, J.H.; Farrugia, G. Heme oxygenase-1 protects interstitial cells of Cajal from oxidative stress and reverses diabetic gastroparesis. Gastroenterology 2008, 135, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.M.; Kashyap, P.C.; Dutta, N.; Stoltz, G.J.; Ordog, T.; Shea Donohue, T.; Bauer, A.J.; Linden, D.R.; Szurszewski, J.H.; Gibbons, S.J.; et al. CD206-positive M2 macrophages that express heme oxygenase-1 protect against diabetic gastroparesis in mice. Gastroenterology 2010, 138, 2399–2409. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, Z.; Loganathan, P.; Sarosiek, I.; McCallum, R.W. Gender-Related Differences in Gastroparesis. Am. J. Med. Sci. 2020, 360, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Guo, Y.; He, J.; Zhang, F.; Sun, X.; Yang, S.; Dong, H. Estrogen and estrogen receptors in the modulation of gastrointestinal epithelial secretion. Oncotarget 2017, 8, 97683–97692. [Google Scholar] [CrossRef] [PubMed]
- Zia, J.K.; Heitkemper, M.M. Upper gastrointestinal tract motility disorders in women, gastroparesis, and gastroesophageal reflux disease. Gastroenterol. Clin. N. Am. 2016, 45, 239–251. [Google Scholar] [CrossRef]
- Degen, L.P.; Phillips, S.F. Variability of gastrointestinal transit in healthy women and men. Gut 1996, 39, 299–305. [Google Scholar] [CrossRef]
- Jiang, Y.; Greenwood-Van Meerveld, B.; Johnson, A.C.; Travagli, R.A. Role of estrogen and stress on the brain-gut axis. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 317, G203–G209. [Google Scholar] [CrossRef]
- Petring, O.U.; Flachs, H. Inter- and intrasubject variability of gastric emptying in healthy volunteers measured by scintigraphy and paracetamol absorption. Br. J. Clin. Pharmacol. 1990, 29, 703–708. [Google Scholar] [CrossRef]
- Gill, R.C.; Murphy, P.D.; Hooper, H.R.; Bowes, K.L.; Kingma, Y.J. Effect of the menstrual cycle on gastric emptying. Digestion 1987, 36, 168–174. [Google Scholar] [CrossRef]
- Crimmins, S.; Smiley, R.; Preston, K.; Yau, A.; Mccallum, R.; Ali, M.S. Increased Expression of Pyloric ERβ Is Associated with Diabetic Gastroparesis in Streptozotocin-Induced Male Diabetic Rats. Gastroenterol. Res. 2016, 9, 39–46. [Google Scholar] [CrossRef]
- Bruce, L.A.; Behsudi, F.M. Differential inhibition of regional gastrointestinal tissue to progesterone in the rat. Life Sci. 1980, 27, 427–434. [Google Scholar] [CrossRef]
- Davis, M.; Ryan, J.P. Influence of progesterone on guinea pig gallbladder motility in vitro. Dig. Dis. Sci. 1986, 31, 513–518. [Google Scholar] [CrossRef]
- O’Sullivan, G.M.; Sutton, A.J.; Thompson, S.A.; Carrie, L.E.; Bullingham, R.E. Noninvasive measurement of gastric emptying in obstetric patients. Anesth. Analg. 1987, 66, 505–511. [Google Scholar] [CrossRef]
- Davison, J.S.; Davison, M.C.; Hay, D.M. Gastric emptying time in late pregnancy and labour. J. Obstet. Gynaecol. Br. Commonw. 1970, 77, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Davison, J.S. Letter: Gastric emptying in labour. Lancet 1975, 2, 227–228. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.H.; Stakes, A.F.; Miller, M. Pregnancy delays paracetamol absorption and gastric emptying in patients undergoing surgery. Br. J. Anaesth. 1988, 60, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.P.; Bhojwani, A.; Wang, M.B. Effect of pregnancy on gastric motility in vivo and in vitro in the guinea pig. Gastroenterology 1987, 93, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Chiloiro, M.; Darconza, G.; Piccioli, E.; De Carne, M.; Clemente, C.; Riezzo, G. Gastric emptying and orocecal transit time in pregnancy. J. Gastroenterol. 2001, 36, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Datz, F.; Christian, P.; Moore, J. Differences in gastric emptying rates between menstruating and postmenopausal women. J. Nucl. Med. 1987, 28, 604–605. [Google Scholar]
- Hutson, W.R.; Roehrkasse, R.L.; Wald, A. Influence of gender and menopause on gastric emptying and motility. Gastroenterology 1989, 96, 11–17. [Google Scholar] [CrossRef]
- Al-Shboul, O.A.; Nazzal, M.S.; Mustafa, A.G.; Al-Dwairi, A.N.; Alqudah, M.A.; Abu Omar, A.; Alfaqih, M.A.; Alsalem, M.I. Estrogen relaxes gastric muscle cells via a nitric oxide- and cyclic guanosine monophosphate-dependent mechanism: A sex-associated differential effect. Exp. Ther. Med. 2018, 16, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Showkat Ali, M.; Tiscareno-Grejada, I.; Locovei, S.; Smiley, R.; Collins, T.; Sarosiek, J.; McCallum, R. Gender and estradiol as major factors in the expression and dimerization of nNOSα in rats with experimental diabetic gastroparesis. Dig. Dis. Sci. 2012, 57, 2814–2825. [Google Scholar] [CrossRef] [PubMed]
- Krishnasamy, S.; Abell, T.L. Diabetic Gastroparesis: Principles and Current Trends in Management. Diabetes Ther. 2018, 9 (Suppl. S1), 1–42. [Google Scholar] [CrossRef]
- Gangula, P.R.; Mukhopadhyay, S.; Ravella, K.; Cai, S.; Channon, K.M.; Garfield, R.E.; Pasricha, P.J. Tetrahydrobiopterin (BH4), a cofactor for nNOS, restores gastric emptying and nNOS expression in female diabetic rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G692–G699. [Google Scholar] [CrossRef] [PubMed]
- van Lelyveld, N.; Ter Linde, J.; Schipper, M.; Samsom, M. Serotonergic signalling in the stomach and duodenum of patients with gastroparesis. Neurogastroenterol. Motil. 2008, 20, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Spohn, S.N.; Mawe, G.M. Non-conventional features of peripheral serotonin signalling—The gut and beyond. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Neal, K.B.; Parry, L.J.; Bornstein, J.C. Strain-specific genetics, anatomy and function of enteric neural serotonergic pathways in inbred mice. J. Physiol. 2009, 587, 567–586. [Google Scholar] [CrossRef] [PubMed]
- Gershon, M.D. 5-HT4-mediated neuroprotection: A new therapeutic modality on the way? Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 310, G766–G767. [Google Scholar] [CrossRef]
- Tack, J.; Broekaert, D.; Coulie, B.; Fischler, B.; Janssens, J. Influence of the selective serotonin re-uptake inhibitor, paroxetine, on gastric sensorimotor function in humans. Aliment. Pharmacol. Ther. 2003, 17, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Coleman, N.S.; Marciani, L.; Blackshaw, E.; Wright, J.; Parker, M.; Yano, T.; Yamazaki, S.; Chan, P.Q.; Wilde, K.; Gowland, P.A.; et al. Effect of a novel 5-HT3 receptor agonist MKC-733 on upper gastrointestinal motility in humans. Aliment. Pharmacol. Ther. 2003, 18, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Waseem, S.; Moshiree, B.; Draganov, P.V. Gastroparesis: Current diagnostic challenges and management considerations. World J. Gastroenterol. 2009, 15, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, S.; Benkelfat, C.; Young, S.N.; Leyton, M.; Mzengeza, S.; de Montigny, C.; Blier, P.; Diksic, M. Differences between males and females in rates of serotonin synthesis in human brain. Proc. Natl. Acad. Sci. USA 1997, 94, 5308–5313. [Google Scholar] [CrossRef] [PubMed]
- Bashashati, M.; McCallum, R.W. Is Interstitial Cells of Cajal−opathy Present in Gastroparesis? J. Neurogastroenterol. Motil. 2015, 21, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Farmer, A.D.; Kadirkamanathan, S.S.; Aziz, Q. Diabetic gastroparesis: Pathophysiology, evaluation and management. Br. J. Hosp. Med. 2012, 73, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Iturrino, J.; Bharucha, A.E.; Burton, D.; Shin, A.; Jeong, I.D.; Zinsmeister, A.R. Performance characteristics of scintigraphic measurement of gastric emptying of solids in healthy participants. Neurogastroenterol. Motil. 2012, 24, 1076-e562. [Google Scholar] [CrossRef]
- Parkman, H.P.; Hasler, W.L.; Fisher, R.S.; American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004, 127, 1592–1622. [Google Scholar] [CrossRef]
- Young, C.F.; Moussa, M.; Shubrook, J.H. Diabetic Gastroparesis: A Review. Diabetes Spectr. 2020, 33, 290–297. [Google Scholar] [CrossRef]
- Meldgaard, T.; Keller, J.; Olesen, A.E.; Olesen, S.S.; Krogh, K.; Borre, M.; Farmer, A.; Brock, B.; Brock, C.; Drewes, A.M. Pathophysiology and management of diabetic gastroenteropathy. Therap. Adv. Gastroenterol. 2019, 12, 1–17. [Google Scholar] [CrossRef]
- Vijayvargiya, P.; Jameie-Oskooei, S.; Camilleri, M.; Chedid, V.; Erwin, P.J.; Murad, M.H. Association between delayed gastric emptying and upper gastrointestinal symptoms: A systematic review and meta-analysis. Gut 2019, 68, 804–813. [Google Scholar] [CrossRef]
- Teigland, T.; Iversen, M.M.; Sangnes, D.A.; Dimcevski, G.; Søfteland, E. A longitudinal study on patients with diabetes and symptoms of gastroparesis—Associations with impaired quality of life and increased depressive and anxiety symptoms. J Diabetes Complicat. 2018, 32, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R. Diabetic autonomic neuropathy. Handb. Clin. Neurol. 2014, 126, 63–79. [Google Scholar]
- Khayyam, U.; Sachdeva, P.; Gomez, J.; Ramzan, Z.; Smith, M.S.; Maurer, A.H.; Fisher, R.S.; Parkman, H.P. Assessment of symptoms during gastric emptying scintigraphy to correlate symptoms to delayed gastric emptying. Neurogastroenterol. Motil. 2010, 22, 539–545. [Google Scholar] [CrossRef]
- Janssen, P.; Harris, M.S.; Jones, M.; Masaoka, T.; Farré, R.; Törnblom, H.; Van Oudenhove, L.; Simrén, M.; Tack, J. The relation between symptom improvement and gastric emptying in the treatment of diabetic and idiopathic gastroparesis. Am. J. Gastroenterol. 2013, 108, 1382–1391. [Google Scholar] [CrossRef]
- Caturano, A.; Galiero, R.; Pafundi, P.C. Metformin for Type 2 Diabetes. JAMA 2019, 322, 1312. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, T.; Galiero, R.; Caturano, A.; Vetrano, E.; Loffredo, G.; Rinaldi, L.; Catalini, C.; Gjeloshi, K.; Albanese, G.; Di Martino, A.; et al. Coronary Microvascular Dysfunction in Diabetes Mellitus: Pathogenetic Mechanisms and Potential Therapeutic Options. Biomedicines 2022, 10, 2274. [Google Scholar] [CrossRef]
- Salvatore, T.; Galiero, R.; Caturano, A.; Vetrano, E.; Rinaldi, L.; Coviello, F.; Di Martino, A.; Albanese, G.; Colantuoni, S.; Medicamento, G.; et al. Dysregulated Epicardial Adipose Tissue as a Risk Factor and Potential Therapeutic Target of Heart Failure with Preserved Ejection Fraction in Diabetes. Biomolecules 2022, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.S.; Camilleri, M. Diagnostic assessment of diabetic gastroparesis. Diabetes 2013, 62, 2667–2673. [Google Scholar] [CrossRef]
- Woerle, H.J.; Albrecht, M.; Linke, R.; Zschau, S.; Neumann, C.; Nicolaus, M.; Gerich, J.; Göke, B.; Schirra, J. Importance of changes in gastric emptying for postprandial plasma glucose fluxes in healthy humans. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E103–E109. [Google Scholar] [CrossRef]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Woerle, H.J.; Meyer, C.; Dostou, J.M.; Gosmanov, N.R.; Islam, N.; Popa, E.; Wittlin, S.D.; Welle, S.L.; Gerich, J.E. Pathways for glucose disposal after meal ingestion in humans. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E716–E725. [Google Scholar] [CrossRef]
- Horowitz, M.; Edelbroek, M.A.; Wishart, J.M.; Straathof, J.W. Relationship between oral glucose tolerance and gastric emptying in normal healthy subjects. Diabetologia 1993, 36, 857–862. [Google Scholar] [CrossRef]
- Jones, K.L.; Horowitz, M.; Carney, B.I.; Wishart, J.M.; Guha, S.; Green, L. Gastric emptying in early noninsulin-dependent diabetes mellitus. J. Nucl. Med. 1996, 37, 1643–1648. [Google Scholar]
- Ishii, M.; Nakamura, T.; Kasai, F.; Onuma, T.; Baba, T.; Takebe, K. Altered postprandial insulin requirement in IDDM patients with gastroparesis. Diabetes Care 1994, 17, 901–903. [Google Scholar] [CrossRef] [PubMed]
- Gonlachanvit, S.; Hsu, C.W.; Boden, G.H.; Knight, L.C.; Maurer, A.H.; Fisher, R.S.; Parkman, H.P. Effect of altering gastric emptying on postprandial plasma glucose concentrations following a physiologic meal in type-II diabetic patients. Dig. Dis. Sci. 2003, 48, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Perano, S.J.; Rayner, C.K.; Kritas, S.; Horowitz, M.; Donaghue, K.; Mpundu-Kaambwa, C.; Giles, L.; Couper, J.J. Gastric emptying is more rapid in adolescents with type 1 diabetes and impacts on postprandial glycemia. J. Clin. Endocrinol. Metab. 2015, 100, 2248–2253. [Google Scholar] [CrossRef] [PubMed]
- Rayner, C.K.; Horowitz, M. New management approaches for gastroparesis. Nat. Clin. Pract. Gastroenterol. Hepatol. 2005, 2, 454–493. [Google Scholar] [CrossRef] [PubMed]
- Parkman, H.P.; Yates, K.P.; Hasler, W.L.; Nguyen, L.; Pasricha, P.J.; Snape, W.J.; Farrugia, G.; Calles, J.; Koch, K.L.; Abell, T.L.; et al. Dietary intake and nutritional deficiencies in patients with diabetic or idiopathic gastroparesis. Gastroenterology 2011, 141, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Sadiya, A. Nutritional therapy for the management of diabetic gastroparesis: Clinical review. Diabetes Metab. Syndr. Obes. 2012, 5, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Di Francia, R.; Rinaldi, L.; Cillo, M.; Varriale, E.; Facchini, G.; D’Aniello, C.; Marotta, G.; Berretta, M. Antioxidant diet and genotyping as tools for the prevention of liver disease. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 5155–5163. [Google Scholar] [PubMed]
- Parrish, C.S.; Pastors, J.G. Nutritional Management of Gastroparesis in People with Diabetes. Diabetes Spectr. 2007, 20, 231–234. [Google Scholar] [CrossRef]
- Suresh, H.; Zhou, J.; Ho, V. The Short-Term Effects and Tolerability of Low-Viscosity Soluble Fibre on Gastroparesis Patients: A Pilot Clinical Intervention Study. Nutrients 2021, 13, 4298. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caturano, A.; Cavallo, M.; Nilo, D.; Vaudo, G.; Russo, V.; Galiero, R.; Rinaldi, L.; Marfella, R.; Monda, M.; Luca, G.; et al. Diabetic Gastroparesis: Navigating Pathophysiology and Nutritional Interventions. Gastrointest. Disord. 2024, 6, 214-229. https://doi.org/10.3390/gidisord6010016
Caturano A, Cavallo M, Nilo D, Vaudo G, Russo V, Galiero R, Rinaldi L, Marfella R, Monda M, Luca G, et al. Diabetic Gastroparesis: Navigating Pathophysiology and Nutritional Interventions. Gastrointestinal Disorders. 2024; 6(1):214-229. https://doi.org/10.3390/gidisord6010016
Chicago/Turabian StyleCaturano, Alfredo, Massimiliano Cavallo, Davide Nilo, Gaetano Vaudo, Vincenzo Russo, Raffaele Galiero, Luca Rinaldi, Raffaele Marfella, Marcellino Monda, Giovanni Luca, and et al. 2024. "Diabetic Gastroparesis: Navigating Pathophysiology and Nutritional Interventions" Gastrointestinal Disorders 6, no. 1: 214-229. https://doi.org/10.3390/gidisord6010016