
Mesenchymal Tumors of the Gastrointestinal Tract—Beyond GIST—A Review

1
Serviço de Anatomia Patológica, Centro Hospitalar e Universitário de Coimbra, 3004-561 Coimbra, Portugal
2
Institute of Biomedical Sciences Abel Salazar, University of Porto (ICBAS-UP), 4050-313 Porto, Portugal
3
Centro de Investigação em Meio Ambiente, Genética e Oncobiologia—CIMAGO, Faculdade de Medicina, Universidade de Coimbra, 3004-535 Coimbra, Portugal
4
Coimbra Institute for Clinical and Biomedical Research—iCBR, Universidade de Coimbra, 3004-535 Coimbra, Portugal
5
Centro de Anatomia Patológica Germano de Sousa, 3000-377 Coimbra, Portugal
*
Author to whom correspondence should be addressed.
Gastrointest. Disord. 2024, 6(1), 257-291; https://doi.org/10.3390/gidisord6010019
Submission received: 16 December 2023
/
Revised: 22 February 2024
/
Accepted: 27 February 2024
/
Published: 4 March 2024
Abstract
:Sarcomas are rare lesions and encompass a wide variety of entities, depending on their nature. In recent years new entities have been described and new knowledge, especially that provided by molecular studies, has been increasing. This makes it very difficult to be updated with all the described entities, since only some of the centers have the desired ancillary studies for the correct diagnosis. Some lesions are extremely rare and may appear once or twice during the lifetime of a general pathologist. When we refer to sarcomas of the gastrointestinal tract, the gastrointestinal stromal tumor (GIST) is the most well-known lesion that the pathologist will most frequently find in daily practice. This paper aims to comprehensively review the sarcomas associated with the gastrointestinal tract, emphasizing histopathology and going beyond GIST. This review highlights the histopathology of rare types of sarcomas so it may increase awareness of common and rare lesions, prompting an easy and effective diagnosis.
1. Introduction
The gastrointestinal tract (GI) exhibits benign and malignant lesions with variable degrees of frequency. Lesions of an epithelial nature, such as polyps and carcinomas, are the most common, especially in the large bowel [1]. Mesenchymal lesions are rarer and encompass a wide variety since they can originate from muscle, neural, vascular, or fibroblastic tissue [2]. Of all the mesenchymal lesions, the most frequent and best known is the gastrointestinal stromal tumor (GIST) [3].
However, the GI tract houses a wide diversity of mesenchymal lesions, some of which are very rare and will probably never be seen by most pathologists. The increase in knowledge generated by next-generation immunohistochemistry and sequencing has provided us with new and fascinating entities [4].
This paper aims to perform a comprehensive review of the mesenchymal lesions of the GI tract, excluding GIST, focusing on pathological evaluation and genetics, with some relevant clinical background. The paper also excluded mesenchymal lesions originating in the liver and pancreas, focusing only on the “GI tract”.
2. Inflammatory Myofibroblastic Tumor
The inflammatory myofibroblastic tumor (IMT) is a rare mesenchymal tumor commonly found in children and young adults, usually in the lungs. Still, in some rare cases, it may be present in the GI tract. The colon and small intestine are the most frequent locations, followed by the stomach [5]. Its etiology is unknown, despite some case reports stating there is an association with infection by the Epstein–Barr virus and immune dysregulation [6]. Regarding its pathogenesis, up to two-thirds of cases have rearrangements of the ALK gene at the 2p23 position with several partners. The RANBP2::ALK fusion is the most common, with rare cases with RRBP1::ALK; in about 5% of cases ROS1, NTRK3, PDGFRB, and RET fusions are identified [7]. In most cases, ALK fusions were assessed by Fluorescence In Situ Hybridization (FISH), so the fusion partner was not known. However, in recent years several comprehensive genetic sequencings have been performed; these have discovered new fusion partners and added new data and possible therapeutic targets [8].
As stated before, most cases occur in the small bowel [9] and stomach [10], but any part of the GI tract may be affected; even in the gallbladder, according to case reports [11]. Clinical features are variable, from abdominal pain to obstruction. In circa 50% of patients, there is leukocytosis anemia and hypergammaglobulinemia [12].
On gross examination, the tumor size is usually variable, and an IMT may be up to 12 cm in length [13]. Histological examination shows uniform, plump spindle cells with pale cytoplasm organized into loose fascicles. The supporting stroma may be collagenous or myxoid and is usually associated with plasma cells and lymphocytes, with fewer eosinophils and neutrophils. The amount of stroma is variable, with some tumors not having much stroma. Mitotic activity is scarce and usually there is no necrosis [13,14]. An epithelioid variant is described, with round cells and large eosinophilic cytoplasm, supported by an abundant myxoid stroma with many neutrophils. Interestingly, this epithelioid variant usually has a RANBP2::ALK fusion and, less commonly, a RRBP1::ALK fusion [15].
The differential diagnosis may be wide since it encompasses almost every spindle cell lesion of the GI tract; however, the combination of morphology (especially inflammation) with ALK staining/fusion, provides the diagnosis.
A morphological example of an IMT can be seen in Figure 1.
3. Desmoid Fibromatosis
Desmoid fibromatosis is a locally aggressive, non-metastasizing neoplasm [13]. It usually develops in the mesentery of the small bowel, and therefore it is considered a GI-associated lesion. It has an infiltrative growth pattern and on radiology evaluation in some cases it may be mistaken for a more aggressive tumor [16].
Symptoms are rather unspecific; most commonly, abdominal pain is present. Both sexes are equally affected, and there is a broad range of higher incidences between 30 and 40 years [17]. There are multiple causes, but circa 15% are associated with mutations in the adenomatous polyposis coli (APC) gene and in these patients it usually presents at a younger age [18]. Tumors can be large, up to 31 cm [19].
Almost all tumors have a dysregulated WNT/β-catenin pathway [20]. Patients with germline mutations usually have an APC or CTNBB1 mutation (mutually exclusive), which is the initiating event. In rare cases, with somatic changes, there is an accumulation of the β-catenin in the cytoplasm, which causes increased transcriptional effects [21].
Histologically, it is composed of long fascicles of spindle cells with ovoid nuclei without atypia or necrosis. The background is variable and can present with myxoid areas or keloidal fibers [22]. The hallmark for diagnosis is nuclear staining for β-catenin [23].
Molecular pathology may be necessary for the diagnosis, and in about 95% of cases a mutation in the exon 3 of β-catenin is found [24]. The APC mutations are usually located at codon 1444 [25]. Some authors advise that a colonoscopy should be performed even in the absence of a mutation in CTNBB1 in apparently sporadic tumors, as it may be associated with a non-recognized form of desmoid fibromatosis [26].
Treatment is surgical, comprising a complete excision. In cases of incomplete resection, there is a high rate of recurrence [27]. Chemotherapy with anthracycline and hormonal therapy may be performed before surgery for tumor shrinkage and to allow a more conservative surgery; or after surgery in cases of incomplete resection [28,29]. A genetic study has a role in prognosis since mutations of the CTNNB1 p.S45F have a worse recurrence-free survival [30]. Currently, some target therapies are under investigation in clinical trials [30] but these are not yet widely available in clinical practice.
Diagnosis is usually straightforward, but a differential diagnosis of GIST must be kept in mind. The correct immunohistochemistry provides the right diagnosis.
4. Solitary Fibrous Tumor
The solitary fibrous tumor is fibroblastic in nature, and is more common in pleural locations [31]. However, it has been described in various anatomical sites, including the GI tract [32].
Usually, it is seen in adults within a wide age range (20 to 70 years). Both sexes are equally affected; symptoms are unspecific, are usually associated with compression and sometimes hemorrhage [33].
Its pathogenesis is defined by a NAB2::STAT6 fusion, in which the repressor domain of NAB2 is replaced by an active domain of STAT6, resulting in constitutive activation of RGR-mediated transcription [34].
Recent studies in thoracic tumors have found three groups of fusions: a predominant NAB2ex4::STAT6ex2, the NAB2ex6::STAT6ex16, and the NAB2ex6::STAT6ex17 (n = 16), which were associated with different clinical features [35]. Recently, a variant called STAT6::TAD was associated with higher mitotic count and lower recurrence-free and overall survival due to increased expression of FGF2 [36].
Grossly, tumors are well circumscribed and can measure up to 25 cm. Morphologically, they are composed of ovoid/spindle cells arranged in poorly defined fascicles, supported by thin-walled vessels dilated in a staghorn pattern. Stromal hyalinization is also a characteristic feature and may be prominent. Myxoid changes, cystic dilation, and hemorrhage may be present [13]. A subset of solitary fibrous tumors exhibit a mature adipose tissue component—the so-called lipomatous solitary fibrous tumor [37]. Immunohistochemistry shows positivity for CD34 and STAT6; the latter considered with high specificity and sensibility [38] and allows the differential diagnosis with GIST.
Treatment is surgical, and the majority of tumors behave benignly. About 10% have an aggressive course. Features associated with worse outcomes are older age, larger size, high cellularity, necrosis, cytological atypia, and high mitotic activity [39].
A study by the French sarcoma group incorporates clinical data, pathological features, and history of radiotherapy to predict survival, recurrence, and distant metastasis [40]. Recently, some cases of dedifferentiated solitary fibrous tumors have been described, and in these cases, chemotherapy seems to be the best choice of treatment [41]. Malignant behavior in solitary fibrous tumors is hard to predict. While most have a benign clinical course, a significant group can recur or metastasize, sometimes after 10 years [42]. Images of SFT can be seen in Figure 6 and Figure 7.
5. Lipoma
Lipomas are benign lesions composed of mature adipose tissue. They are relatively common in soft tissues and may appear in any location in the GI tract [43].
Most lipomas appear in the submucosa and the caecum/ascending colon. Some rare cases can appear in the subserosa and mucosa. The latter is sometimes associated with Cowden syndrome [44].
Clinically, lipomas are commonly asymptomatic and represent incidental findings; however, in some cases—especially when the tumor is in the caecum or is large in size— they can cause obstruction [45]. Ulceration and hemorrhage may be referred by patients [46].
Morphologically, lipomas in the GI tract are identical to their soft tissue counterparts: mature adipocytes of uniform size without atypia. If they exhibit prominent capillary vessels with microthrombi, the designation of angiolipoma may be applied [13].
6. Inflammatory Fibroid Polyp
Inflammatory fibroid polyp is a benign fibroblastic neoplasm. Typically polypoid in appearance, with some rare sessile lesions, they show a predilection for the stomach (antrum), followed by the ileum [47].
Usually, they are incidental findings, with large tumors being discovered in investigations due to abdominal pain, hemorrhage, or obstruction [48]. Some small lesions in the intestine may cause intussusception [49].
Most of the tumors are sporadic in origin, with some cases demonstrating a familial predilection due to germline PDGFRA mutations [50]. These mutations usually occur in exon 18 in the stomach and exon 12 in the small intestine [51].
The tumors vary in gross size; most are usually less than 3 cm, but in some cases they can be up to 7 cm [52].
Histological morphology is typical. The lesion is usually centered in the submucosa and composed of a proliferation of spindle and stellate cells in a haphazard distribution. The stroma is vaguely myxoid and contains inflammatory cells, namely eosinophils. Small to intermediate blood vessels with concentric fibrosis are also a characteristic part of the spectrum [13].
Immunohistochemistry demonstrates a consistent positivity for CD34 and PDGFRA [53]. Due to CD34 positivity, the main differential diagnosis is with GIST and SFT, but inflammatory fibroid polyp is negative for DOG-1 and STAT6.
7. Plexiform Fibromyxoma
This is a rare entity with benign behavior that arises in the antrum and pyloric region and, sometimes, in the duodenum [55]. Recently, a case was described in which the esophagus was affected [56]. Both sexes are equally affected, and the age range is wide, and includes children [57].
Symptoms are usually related to GI obstruction, with some being asymptomatic [58]. Grossly, this lesion appears as a gelatinous mass centered in the muscularis propria that can protrude to the serosa or to the mucosa with ulceration [59]. Lesions vary in size; with large lesions measuring up to 15 cm [60].
The histomorphology of these tumors is rather typical: bland spindle cells, supported by a myxoid/fibromyxoid/collagenous stroma and with a rich vascular network of thin-walled vessels in a multinodular pattern. Immunohistochemistry has a limited role; it is usually limited to smooth muscle actin positivity, and has more value in establishing the differential diagnosis [13].
8. Leiomyoma
Leiomyomas are benign mesenchymal tumors with smooth muscle differentiation. They are the second most common mesenchymal neoplasms of the GI tract [62], occurring more frequently in the esophagus (10%), colon, and rectum (together 80%); they are rarer in the stomach and the small intestine [63,64,65]. Data about prevalence are not known, but they are rare, and autopsy studies point to an incidence of 0.006–0.008% of esophageal leiomyomas [66]. Most commonly, they are found incidentally [62]. Depending on the location in which they arise, they can be polypoid or intramural.
Colorectal leiomyomas usually arise from the muscularis mucosae, are more frequently small-sized and pedunculated; rarely, they can appear as ulcerated lesions [62,67]. They are found more often in men (2.4:1 M:F) between the ages of 38 and 85 years, with a median of 62 years, and are located predominantly in the rectum and sigmoid colon [65]. The age of appearance may reflect when patients start to undergo colonoscopies. Rarely, they can be intramural in the colon and rectum [65].
Esophageal leiomyomas arise from the muscularis propria, and are intramural and larger [67]. Esophageal leiomyomas appear more frequently in younger men, with a median age of 30 to 35 years. They are more common in the lower third of the esophagus, are usually larger than colon leiomyomas because of their intramural origin, and they have a median size of 5.3 cm [63]. In a study of 342 patients whose esophagi were completely excised, 27 had leiomyomas, representing an incidence of 7.9%; none of them were clinically detected and more commonly arose from the inner circular layer of the muscularis propria [13].
Grossly, leiomyomas are white, well delimited, and have a firm consistency. Histologically, leiomyomas are composed of well-differentiated fascicles of bland, fusiform cells with elongated nuclei with tapered ends with eosinophilic cytoplasm. The histological features are similar, irrespective of where they arise. Mitotic activity and necrosis are absent. Atypia may be present in symplastic leiomyomas [65]. Leiomyomas stain positively for muscle markers—such as α-SMA, desmin, and h-caldesmon—and do not express S100, CD34, KIT, or DOG1, which is important in the differential diagnosis of other fusiform neoplasms in the GI tract, such as schwannoma, gastrointestinal stromal tumors, and inflammatory fibroid polyps [13].
These are benign neoplasms with no risk of recurrence or metastasis, and enucleation of the lesion is the treatment of choice [65].
9. Leiomyosarcoma
Leiomyosarcoma is a rare, malignant neoplasm with smooth muscle differentiation; in the GI, they are extremely rare. According to the SEER database [62], in a 15-year period (2001–2016) in the United States, a total of 523 patients were diagnosed with GI leiomyosarcoma. In a single institution study, Agaimy et al. [68] found three cases of leiomyosarcomas out of 262 mesenchymal lesions over 12 years.
According to one study, the median age at diagnosis is 58.5–66 years (18–94 years) [63,64]. It is most frequently found in the small intestine (31.7%), followed by the duodenum, the ileum and jejunum, the stomach (28.3%), and the colon (26.4%) [8]. It has an equal incidence in males and females [62].
In the largest study of LMS of the GI, the mean tumor size varied. In the esophagus it was 10.2 ± 4.5 cm, in the stomach it was 6.45 ±3.7 cm, in the small intestine it was 10.6 cm ± 6, and in the colorectum it was 6.7 ± 5 [64]. In a study by Yamamoto et al. [63], where they reported seven leiomyosarcomas of the GI, three were elevated and ulcerated with transmural involvement, two were in the submucosa with ulceration of the overlying mucosa, and two had extramural growth. Grossly, LMS are usually described as lobular masses, and are sometimes polypoid or ulcerated, with a grey, beige, or pink-tan mass [64,68].
Morphologically, they are composed of fascicles of spindle cells with atypia, centrally placed cigar-shaped nuclei, and eosinophilic fibrillary cytoplasm with high mitotic counts. LMS are positive for muscle markers, and α-smooth muscle actin closely followed by muscle-specific actin were reported to have the highest sensitivity (86% and 71%, respectively), these tumors are negative for c-kit and DOG1 [63]; however, desmin shows higher specificity as GISTs may have α-smooth muscle actin staining [65]. Loss of smooth muscle marker expression is associated with a worse prognosis [66,67].
In a study that involved multiple institutions, 407 smooth muscle tumors of the GI were studied, irrespective of whether they were initially diagnosed as leiomyoma or leiomyosarcoma, several pathological features were assessed, and some were found to be linked to a more aggressive course, such as moderate-to-severe atypia, high cellularity, abnormal or lack of differentiation, tumor necrosis mucosal ulceration, lamina propria involvement, and serosal involvement [65]. In another study, where only leiomyosarcomas were considered, tumors ≥ 5 cm were associated with shorter survival, and no association was found between the mitotic count and prognosis [63].
Usually, these patients present with unspecific symptoms; thus, around 40% have regional or distant involvement at diagnosis. Yamamoto et al. reported a 14% local recurrence rate and a 43% metastasis rate in their series; it is estimated that between 25 and 50% of patients died because of the disease [63]. In the analysis of the SEER data, the 5-year overall survival was 77.3%, and the cancer-specific survival was 90.3%. The grade and stage of the tumor were the only factors significantly affecting survival in the multivariate analysis [62].
The mainstay treatment for patients with resectable disease is surgery, as it is correlated with a better prognosis [64].
A typical morphology of a leiomyosarcoma can be observed in Figure 14.
10. Hemangioma
Hemangiomas of the GI are uncommon, they can appear as a single or multiple lesions, and occur anywhere throughout the GI tract [13,69]. Far more common are vascular malformations [70,71].
The most common location of hemangiomas is the small intestine [70]. The colorectum is a rare place of appearance and of all hemangiomas located here, about 50% appear in the rectum [13]. In the stomach, vascular malformations are more common than true hemangiomas [71]. There is a wide range of incidence for true hemangiomas, from being congenital to appearing in the eighth decade of life [71].
Clinically, the most common presentation is occult or acute GI bleeding; other presenting symptoms include abdominal pain, bowel obstruction, and perforation, but they can also be incidental. Grossly, the majority appear as intraluminal lesions, but polypoid lesions may occur [70].
11. Lymphangiomas
Lymphangiomas are benign mesenchymal tumors that, rarely, can be found throughout the GI tract, accounting for less than 5% of lymphangiomas [72]. They most commonly appear in the small intestine and less commonly in the colon and esophagus [13]. Usually, they occur in children and young adults and are equally distributed among genders [73].
Clinically, the patients may appear with anemia or acute abdomen. They can also be found incidentally during endoscopy or colonoscopy [74].
It has been suggested that these lesions may be congenital, or arise due to inflammation or trauma [73]. Grossly, they can range from small lesions to large masses [74].
Histologically, they are composed of thin-walled, cystically dilated lymphatic spaces lined by endothelial cells with lymph fluid [73] (see Figure 16). When lymphangiomas are multicentric or extensively infiltrating, this is called lymphangiomatosis [13]. Immunohistochemically, lymphangiomas stain for D2-40 and CD31 and show variable expression of CD34 [71].
12. Kaposi Sarcoma
Kaposi sarcoma (KS) is a vascular neoplasm derived from the lymphatic endothelium that can arise anywhere along the GI tract [13]. There are four different epidemiologic types: classic KS, iatrogenic/immunosuppressive KS, AIDS-related KS, and endemic KS [75].
Human herpesvirus 8 (HHV-8) has been identified as the causative agent. In Europe and the United States, KS usually manifests in the context of immunosuppression, such as post-transplantation or as a complication of AIDS. Between a quarter and half of AIDS patients can have visceral lesions, sometimes without cutaneous manifestations of KS [76,77,78] and it is frequently asymptomatic [78]. When symptomatic, the most common manifestations are diarrhea, abdominal pain, and GI bleeding [79]. The GI tract is the most common extracutaneous site for Kaposi in AIDS [13,75]. It stands out as the most prevalent gastrointestinal tumor in AIDS cases.
There is a wide age range for KS diagnosis. In a study by Zheng et al. [79], a multi-institutional analysis of 46 cases of KS of the GI was carried out; they found that incidence ranged from 25 to 72 years (median 34 years), with a male predominance.
Although it can involve any part of the GI tract, involvement of the upper tract is more common, especially the stomach, duodenum, and esophagus [78].
Macroscopically, KS in the GI typically presents as red, blue, or brown nodules/mass-like lesions, erythematous lesions, ulcers, and macules [13,79].
Histologically, KS is characterized by a proliferation of blood vessels and spindle cells with minimal atypia organized in vague fascicles, slit-like spaces with extravasated red blood cells with hemosiderin deposition, which is associated with lymphocytic and plasma cell infiltrate. The PAS shows hyaline globules, and there is a variable mitotic activity [75]. Multiple variants of KS have been reported, which may make the diagnosis considerably more difficult [79]. Seven morphologic patterns have been described as occurring in the GI tract, apart from the conventional KS morphology. Two are spindle cell patterns (GIST-like and inflammatory myofibroblastic tumor-like) and five patterns without spindle cells (lymphangioma/lymphangiectatic-like, mucosal hemorrhage/telangiectatic-like, mucosal inflammation-like, granulation tissue-like, and mucosal prolapse-like). The majority of cases were of the non-spindle variant [13].
Endothelial markers such as CD31, CD34, ERG, and D2-40 help ascertain a vascular differentiation of the neoplasm, and the antibody against the latent nuclear antigen 1 (LNA-1); a protein in HHV-8 confirms the diagnosis [75,80].
The differential diagnosis can include bacillary angiomatosis and angiosarcoma.
Enteric KS is usually clinically silent and has low morbidity, and the involvement of the GI tract does not influence survival [13].
13. Angiosarcoma
Angiosarcomas are malignant mesenchymal neoplasms that recapitulate endothelial cell differentiation [81]. Primary angiosarcomas are rare in the GI tract and are reported mainly in the setting of metastatic disease [13,82]. In an extensive review of the literature on primary angiosarcomas of the GI tract, Schizas et al. reported 110 cases published in the English literature [83].
Primary angiosarcomas present with non-specific symptoms such as GI bleeding, abdominal pain, mass or ascites, and acute abdomen, and the interval between the symptoms and the diagnosis is estimated to be greater than six months [83].
Grossly, angiosarcomas can have a variable appearance, from firm greyish-white tissue to markedly hemorrhagic tissue with cystic spaces; they form hemorrhagic, often ulcerating masses. The tumor size ranges from 1.5 to 19.5 cm (median 4–6 cm) [13,83]. Angiosarcomas in the GI tract have a male predominance and more commonly affect adults, with a peak in the seventh decade of life [83]; it can, rarely, affect children. The majority of cases are described in the small (44.5%) and large intestine (35.5%), and less commonly in the stomach (4.5%) and esophagus (2.7%) [83]. Predominantly, angiosarcomas are unifocal, but multifocality has also been described [83]. Angiosarcomas can arise de novo or can be secondary to radiation, most commonly after ten years.
Cytogenetically, angiosarcomas have complex karyotypes [84], which are usually aneuploid without any characteristic point mutation or gene fusion [13]. There are low levels of alterations in TP53 and the PIK3CA/AKT/mTOR pathway [85].
Recurrent somatic mutations involving genes that regulate the angiogenic signalling pathways and endothelial cell receptors are found in angiosarcomas [13,86], with increased expression of vascular endothelial growth factor and its receptors [87] and mutations in KDR, PTPRB, and PLCG1 [88,89]. KDR mutations have been reported in both primary and secondary angiosarcomas, and may be a target of specific kinase inhibitors. PLCG1/KDR mutations are mutually exclusive [88]. MYC amplification or high expression is seen in less than 10% of sporadic angiosarcomas [88]; it is much more common in secondary angiosarcoma related to breast cancer and lymphedema [88]. However, recent studies have detected MYC amplification in almost one-third of primary breast angiosarcomas [90] and 25% of visceral angiosarcomas [91]. Particularly in younger patients, CIC fusions have been described, and the presence of CIC alterations is associated with inferior disease-free survival [88]. Rare mutations have been described in RAS, PIK3CA, TP53, FLT4, and TIE1 [88].
There is a wide variation in morphology, from a well-formed network of vessels to sheets of epithelioid and spindle cells without a clear formation of vessels. The endothelial cells are often atypical. They are high-grade neoplasms with high mitotic activity and coagulative necrosis. The endothelial cells are spindled, hobnailed, or epithelioid, and may form papillary-like projections [13]. In the GI, a predominance of an epithelioid morphology is common [88]. Epithelioid angiosarcomas usually show a solid architecture and atypical epithelioid cells with abundant cytoplasm, mimicking carcinoma, melanoma, or lymphoma [13]. Less commonly, they can appear to be low-grade with well-formed vascular channels with minimally atypical spindled cells [13]. Endothelial markers are essential to establish the vascular nature of the tumor. Angiosarcomas usually show staining for vascular markers, such as CD31, factor VIII [92], FLI1, podoplanin [93], and ERG positivity [94]. The expression of CD34 is variable [13], and as it becomes more poorly differentiated, it is more probable to lose CD34, or for its expression to be decreased. The use of CD31 and CD34 identifies almost all angiosarcomas, even poorly differentiated ones [13]. FLI1 and ERG have a high specificity and sensitivity, although some carcinomas and melanomas may express them [94,95]. In angiosarcomas, especially epithelioid type, expression of keratins may be present [96].
Due to its epithelioid morphology, several differential diagnoses might be considered, including melanoma, sarcomas, and poorly differentiated carcinoma.
No association between angiosarcoma and immunosuppression or HIV positivity has been found [87].
Metastasis at presentation is found in primary angiosarcomas of the small intestine and colon in 44.9% and 53.8% of patients, respectively. The main sites involved are the liver and lungs [83]. Median survival varied between two and three months. The prognosis is unfavorable, with survival usually being below one year [97].
Local disease is treated with surgical resection, chemotherapy, and radiation therapy [13].
14. Glomus Tumor
Glomus tumors are composed of cells developed from the neuromyoarterial apparatus in the glomus body, representing less than 2% of soft tissue tumors [81]. Glomus tumors occur most commonly in the upper extremities in the subungual region. Rare cases can appear in the digestive tract and can be mistaken for neuroendocrine tumors, gastrointestinal stromal tumors, or metastasis [98]. They are rarer than GISTs, with an estimated incidence of one in 100 of that of GISTs [99]. Most glomus tumors are benign but they can exhibit malignant behavior with infiltrative growth and metastasis [100].
In the GI tract, they are most commonly found in the stomach [99] and can be found in the esophageal junction and duodenum. In a series by Miettinen et al. [99], just one out of 32 GI glomus tumor was not in the stomach, but was located in the cecum.
It probably has an equivalent incidence between genders. However, the paper by Miettinen showed a strong female predominance (72%) with a female–male ratio of 1.6:1, and the age of the patients ranged from 19 to 90 years (median age 55 years). Glomus tumors have been found in patients as young as 8 years [100].
The most common presenting symptom is upper GI bleeding, with melena being the most common consequence; other common symptoms are anemia and weakness. The tumor in the cecum mimicked appendicitis. Glomus tumor of the GI tract is typically a single lesion, but 10% of patients have a multifocal disease. Inactivating mutations of the glomulin gene are associated with multiple familial glomus tumors [81].
Grossly, they are reported as being circumscribed and intramural, with sizes varying between 1.3 and 7 cm (median 2.5 cm). The consistency is described as soft to rubbery and sometimes spongy. The color is white to pink and frequent hemorrhage occurs; ulceration of the mucosa is a common finding [99]. Presenting signs are non-specific with GI bleeding and ulcers.
Histologically, they involve the muscularis propria and are similar to the ones found in the soft tissue. Most are multinodular, separated by bands of smooth muscle. Dilated veins are present in the periphery of the lobules and the tumor periphery. A fibrous band of tissue around the tumor is a common finding. Surrounding the tumors is smooth muscle and a fibrous capsule [99]. The cells that make up these neoplasms have a distinct appearance, with a round and uniform shape and sharply defined borders that can be accentuated by PAS or toluidine blue [81]. They are organized in sheets and nests surrounding vascular spaces; cytoplasmatic clearing is a common finding. Mitotic activity is low, with less than five mitosis per 50 HPF. Foci of myxoid and hyaline change are common, especially in the center of the tumor. Vascular space involvement is also a common finding, especially at the periphery of the tumor; but this alone is not associated with metastasis [100].
The cells are positive for vimentin, smooth muscle actin, calponin [99], TLE1 [101], and often for h-caldesmon. Desmin is variable, and S100 and c-kit are absent [102]. Weak staining for synaptophysin is sometimes observed, which is important to keep in mind in the differential diagnosis of neuroendocrine tumor, paraganglioma, leiomyosarcoma, and lymphoma.
Fusions of CARMN::NOTCH with the partners NOTCH1 (3%), NOTCH2 (52%), and NOTCH3 (9%) genes have been described in both benign and malignant soft tissue glomus tumors [103]. This has also been confirmed in glomus tumors of the upper GI tract, where it was found at a higher incidence than the glomus tumors of the extremities, with the detection of the fusion transcript CARMN::NOTCH2 in 88% of cases [98]. In this series, the only two cases that did not have the CARMN::NOTCH2 had a specific morphology. All the cases with the fusion could be detected by the NOTCH2 antibody, which was negative for gastrointestinal stromal tumors, neuroendocrine tumors, desmoid tumors, inflammatory fibroid polyps, and leiomyosarcomas [98]. A small subset of angioleiomyomas and myofibromas harbors the same fusion [104]. BRAF V600E mutation and KRAS G12A mutation have been described in glomus tumors of the soft tissue [105]. In a subset of malignant glomus tumors, BRAF V600E expression has been noted [106]. Recurrent alterations in ATRX, CCND1, and CDKN2A were also described for malignant glomus tumors [107].
Papke et al. studied features associated with adverse outcomes in gastroesophageal glomus tumors. Glomus tumors with cytologic atypia, two or more mitoses per 10 HPF, and tumors 5 cm or bigger should be considered malignant. Complex copy number alterations were found in the malignant glomus tumors but not in the benign [107]. Folpe et al. previously had defined criteria for the classification of atypical and malignant glomus tumors in the soft tissue [108], which included deep location, a size ≥ 2 cm, moderate to high nuclear grade with ≥5 mitosis/50 HP.
The majority of glomus tumors are benign, and excision is the treatment of choice. A glomus tumor is represented in Figure 17.
15. Schwannoma
Schwannomas are benign lesions originating from the nerve sheath cells that are common in the soft tissue [81].
Regarding the GI tract, they usually form intramural masses and typically arise in the stomach [109]. Most commonly, they are incidental findings, although some may cause GI bleeding or mass-like symptoms [110]. Endoscopy has a pivotal role in the diagnosis and in obtaining tissue for pathology examination [111].
The majority are sporadic, but some cases may be associated with neurofibromatosis type 2; in these cases, they show loss of heterozygosity at NF2. The most frequent type of schwannoma in this context is the plexiform type [112].
On gross examination, they are well circumscribed, usually in the submucosa, with a wide size range; cases of lesions measuring up to 7 cm have been described [113].
Histologically, they are similar to the soft tissue counterpart, with spindle cells distributed in hypo- and hypercellular areas. Older lesions may show cystic changes, hemorrhage, and hyaline thick-walled blood vessels. A particular subtype of schwannomas in the GI tract is the reticular subtype. Schwannomas have a peculiar peripheral lymphoid cuff. Immunohistochemistry is consistent with Schwannian differentiation, with S100 and SOX10 positivity (Figure 18 and Figure 19).
16. Granular Cell Tumor
A granular cell tumor is a lesion with neuroectodermal differentiation, composed of cells with epithelioid morphology and granular cytoplasm due to a high quantity of lysosomes [13].
Up to 10% of the lesions arise in the GI tract; the esophagus being the most common location, especially in the lower part [114]. Some cases are described in other locations, namely the large bowel and perianal region [115].
The majority of cases are of small dimensions and, thus, are discovered incidentally. They can appear at any age but are more common around the sixth decade of life [114].
Most cases are sporadic, with some cases associated with neurofibromatosis type 1 [116], Noonan syndrome [117], and LEOPARD syndrome [118]. In syndromic cases, the granular cell tumor usually develops in a non-GI location.
Recent genetic studies have shown mutations (in circa 70% of cases) in ATP6AP1 and ATP6AP2; namely, inactivating mutations inducing an oncogenic driver and generating intracytoplasmatic granules [119].
Grossly, there are small yellowish nodules, usually under 3 cm. Histology exhibits a poorly defined lesion, with monotonous and epithelioid cells with abundant eosinophilic and granular cytoplasm. The cells are arranged into cords and nests, sometimes growing under the squamous epithelium of the esophagus, which shows pseudoepitheliomatous hyperplasia. The nucleus is frequently eccentric, small, and regular, as seen in Figure 20.
Some malignant cases are described, usually presenting with nuclear pleomorphism, mitosis, necrosis, and sometimes sarcomatous transformation [13,81].
Immunohistochemistry shows positivity for S100 and calretinin [13]. Excision is the treatment of choice with good results. There are no established guidelines in malignant cases, but the use of pazopanib monotherapy, a potent oral tyrosine kinase inhibitor, has been reported with success in soft tissue tumors [120,121].
17. Perineurioma
Perineurioma is a benign lesion composed of cells with perineurial differentiation [13].
The majority of lesions are discovered incidentally during colorectal cancer screening, with the rectosigmoid colon being the most common location. Some cases may be identified in the stomach. They have a female predominance and appear in middle-aged adults [122].
Some cases have been associated with NF1/2 mutations [123] and serrated polyposis with BRAF V600E mutations [124].
They appear as small polypoid lesions. On microscopic evaluation, they show expansion of the lamina propria by uniform and bland spindle cells, entrapping colonic crypts. Some lesions can focally infiltrate the muscularis mucosa, but they are commonly well-defined. The cells have a whorled architecture and sometimes wavy nuclei. Mitosis and necrosis are absent. Immunohistochemistry reveals positivity for EMA, claudin-1, and GLUT1 [13].
18. Ganglioneuroma
The lesion encompasses a benign tumor composed of a mixture of mature ganglion cells, satellite cells, and nerves. In cases of multiple lesions or those associated with a syndrome, the term ganglioneuromatosis is employed [13].
Most cases occur in the large intestine, with a predilection for the left side and rectum. No gender preference is observed, and the age range is wide [125,126].
Usually, they present in colorectal cancer screening as small polypoid lesions (inferior to 2 cm) and can be solitary, multiple, or diffuse. Multiple and diffuse lesions have a strong association with multiple endocrine neoplasia (MEN) type 2B or neurofibromatosis type 1; the latter is less common [127]. Multiple ganglioneuromatosis polyposis is frequently associated with Cowden syndrome, with PTEN mutations [128].
Microscopically, the polypoid lesions show an expansion of the lamina propria by ganglion and Schwan cells, accompanied by eosinophils, sometimes with cystic colonic glands. Ganglioneuromatosis is characterized by an exuberant proliferation of nerves and ganglion cells. In these cases, the cells may also form nodules and have a transmural involvement. Immunohistochemistry is not contributive and shows neural and Schwann differentiation [13]. An example can be seen in Figure 21.
19. PEComa
The family of perivascular epithelioid cell tumors (PEComa) is a group of mesenchymal neoplasms composed of epithelioid cells that express both smooth muscle and melanocytic markers [81]. The term perivascular epithelioid cell was first suggested by Bonetti et al. to describe a cell type with both melanocytic and muscular characteristics [129].
PEComas are a family of tumors encompassing several entities that were once thought to be separate entities but are now considered related, including angiomyolipoma, lung lymphangioleiomyoma, and clear cell sugar tumor of the lung [81].
In patients with tuberous sclerosis, 80% of patients by the age of 10 develop renal angiomyolipomas, which are often multiple or bilateral, and almost 40% of women with this syndrome are affected with lymphangioleiomyomatosis. Other PEComas are usually sporadic [130].
PEComas are genetically heterogeneous [81]. About two-thirds of cases show deletions or mutations of the TSC2 gene or with a lower incidence TSC1 gene, leading to its inactivation; this can occur both in sporadic cases and in cases associated with tuberous sclerosis [131]. Of cases with TSC2 mutation, two-thirds have TP53 mutation [132]. TFE3 rearrangement may occur in 20% of the PEComas [132]. TFE3 rearrangements and TSC1/2 inactivation seem to be mutually exclusive [132].
They are rare neoplasms, and less than 100 cases have been reported in the GI tract [133]. The most common locations are the colon, liver, and small intestine. The stomach and other GI organs are rare sites for PEComas to arise [81]. The presenting symptoms are not specific, and include abdominal pain, GI bleeding, and weight loss.
Grossly, PEComas are circumscribed and encapsulated with a cut surface that varies from pale tan to greyish brown. Depending on their size, they can be intramural, and centered in the mucosa and submucosa; or transmural, involving the mesentery. Pedunculated PEComas have also been described [134,135,136].
In the biggest series conducted to date, Doyle et al. [133], reported a total of 35 cases of GI PEComas. The age at presentation varied between 7 and 70 years, with a median age of 45. The most common location was the colon (54%), more commonly the right colon, followed by the transverse, small bowel (35%), stomach (6%), gallbladder, and omentum (3% each). In this series, the tumor size ranged from 0.8 to 22 cm, with a median of 6.2 cm. In 31 patients, follow-up was available, with a median duration of 36 months. Local recurrence was not reported, but 13 patients developed metastatic disease. Five patients were reported to have died from the disease; the median time from the diagnosis to death was 22 months (ranging from 2–48 months).
There is uncertainty in how to predict the behavior of these neoplasms. They can have a benign behavior, uncertain malignant potential, or a malignant behavior. A risk stratification method has been proposed by Folpe et al. [108,137]. Some histological features have been associated with metastatic disease, such as marked nuclear atypia, diffuse pleomorphism, and ≥2 mitoses per 10 HPFs [133]. A tumor size above 6 cm seems to be associated with metastatic potential, but this finding did not reach statistical significance; the presence of atypical mitosis was not associated with metastasis [133].
Histologically, GI PEComas are morphologically similar to PEComas that develop elsewhere in the body. Most have a nested, trabecular, and alveolar architecture, surrounded by a delicate vasculature [81], with frequent perivascular condensation; however, PEComas can have a surprisingly diverse morphologic appearance. The cells are usually epithelioid with round to oval nuclei with a granular eosinophilic cytoplasm; a minority of spindle cells can be seen. Occasional multinucleated giant cells can be present [108]. The mitotic activity usually is low. The subset of PEComas associated with TFE3 translocation can have a striking similarity with alveolar soft part sarcoma, with a pseudoalveolar architecture.
PEComas are characterized by positivity for muscle markers (α-SMA and desmin) and melanocytic markers. HMB-45 is the most sensitive marker, followed by Melan-A, and MiTF as the least sensitive [108]. The epithelioid cells stain more extensively for melanocytic markers than the spindle cell component when present. In the TFE3-rearranged PEComa group, TFE3 expression is achieved by immunohistochemistry [138]. Up to one-third can stain for S100, and rare cells can stain for pancytokeratins and c-kit [108].
20. NUTM1-Rearranged Colorectal Sarcoma
NUT carcinomas are aggressive tumors that occur typically in the midline region in teens and young adults. They are commonly metastatic at the time of presentation, and are associated with a dismal prognosis [141].
Nuclear protein of the testis (NUT) carcinomas harbor fusions of NUTM with BRD4 (71%) and BRD3 (14%). Other uncommon partners are NSD3, ZNF532, and ZNF592. The cell of origin is unknown, and the most common locations are the head, neck, and thorax [142].
Rearrangements of NUTM1 are not limited to NUT carcinomas and have been described in poromas and porocarcinomas [143], embryonal tumors of the central nervous system [144], and undifferentiated sarcomas [145]. Sarcomas with NUTM1 rearrangements often show fusions involving the MAX family genes or CIC [146,147].
NUTM1-rearranged sarcoma is considered a distinct entity within the group of NUTM1-rearranged tumors. NUTM1-rearranged colorectal sarcoma is a recently described neoplasm with predominant spindle cell morphology and variable epithelioid/rhabdoid morphology with an MXD4::NUTM1 fusion [145]. In a paper by Van Treeck et al. [145], five patients with this rare entity were described. Four out of five patients were female, with age of presentation ranging from 38 to 67 years (median 51 years).
Grossly, the tumors were circumscribed, whorled, white to tan in color, with a size ranging from 2.5 to 20 cm. The tumors presented in the colon and the ileocecal valve region, and four had metastasis at presentation; three had lymph node involvement and one had liver involvement. Morphologically, the lesions were centered in the submucosa, infiltrated the mucosa and the muscularis propria, and were described as having three distinctive patterns: intersecting fascicles with uniform cells pattern, a hyalinized/nested pattern, and an epithelioid and rhabdoid pattern. Mitotic activity was low. Immunohistochemically, NUTM1-rearranged sarcomas have a nuclear expression of NUT, variable keratin expression and expression of CD117 and DOG1, and retained expression of SMARCB1 and SMARCA4 [148].
GIST, synovial sarcoma, sarcomatoid carcinomas, sarcomatoid mesothelioma, and rhabdoid tumors should be considered in the differential diagnosis. The expression of NUT or NUTM1 rearrangement is key for the diagnosis [146].
21. Mesenchymal Tumors Associated with NTRK Rearrangements
Eight cases of mesenchymal tumors with NTRK1 or NTRK3 rearrangements were described by Atiq et al., who identified three different groups of tumors. One was infantile fibrosarcoma with involvement of the GI tract, another was low-grade spindle cell S100+ and CD34+ neoplasms associated with NTRK1 fusions, and the third was unclassified high-grade spindle-cell sarcomas with NTRK1 fusions [149]. These tumors were morphologically and immunohistochemically different from GISTs, notably by the absence of DOG1 and KIT expression by immunohistochemistry [149].
22. Synovial Sarcoma
Synovial sarcoma is a high-grade lesion that is extremely rare in the GI tract. It has a morphological overlap with its soft tissue counterpart and is characterized by an SS18::SSX1/2/4 rearrangement [13].
In the GI tract, it is usually described in the stomach, albeit rarer cases were referred to in other locations. It appears in middle-aged to older adults, without gender predilection, and can be a polypoid or an ulcerated lesion [152].
Morphologically, they are monophasic with uniform spindle cells with scarce matrix or biphasic with glandular elements. High-grade sarcoma features with pleomorphic features and mitosis can be present and are associated with a poor prognosis [153].
Immunohistochemistry is similar to the soft tissue counterpart; tumors may have focal positivity for keratins and EMA in monophasic lesions and strong staining in the biphasic version [81]. A recent antibody for SS18/SSX has demonstrated excellent correlation with molecular findings.
Data are scarce, but small lesions with low-grade features seem to have an excellent prognosis after complete excision, while high-grade lesions are associated with aggressive behavior [154].
23. Gastrointestinal Clear Cell Sarcoma/Malignant Gastrointestinal Neuroectodermal Tumor
The last entry of this paper stands for a less common lesion with neuroectodermal differentiation and a gene fusion involving the ESWR1 gene.
This tumor usually arises in young adults but can appear in older age groups. It is highly aggressive, with a tendency for metastases in the lymph nodes and the liver, which are frequently present at diagnosis. The size of the tumor varies, and tumors of up to 15 cm, polypoid or mural in appearance, with ulceration resembling carcinomas have been reported.
Histology shows a nested or pseudopapillary pattern and sometimes a spindle phenotype. Nuclei are large with prominent nucleoli, and cytoplasm is eosinophilic and, in rare cases, clear. Osteclastic-like giant cells are present in 50% of cases. Mitotic activity is common.
Immunohistochemistry shows a neuroectodermic differentiation with S100 and SOX10 positivity. It is a matter of debate whether the gastrointestinal clear cell sarcoma/and the malignant gastrointestinal neuroectodermal tumor are different tumors or the same tumor with two faces. Tumors with positive melanocytic markers (Melan-A, HMB45, or MiTF) are considered clear cell sarcomas, while tumors with negativity for these markers are called malignant gastrointestinal neuroectodermal tumors.
Most cases contain EWSR1 fusions, namely EWSR1::ATF1 or EWSR1::CREB1. This gene alteration allows the differential diagnosis of metastatic melanoma.
A summary of the lesion features is displayed in Table 1.
24. Conclusions
Gastrointestinal sarcomas exhibit significant diversity in their characteristics and morphology. While GIST is the most common mesenchymal tumor of the GI tract, it is crucial to recognize the broader spectrum of entities. Awareness of the various entities and diagnostic options is challenging.
Although morphology remains fundamental, the considerable morphological similarities make it challenging to achieve precise diagnoses based solely on morphology. Acknowledging this, incorporating an updated immunohistochemical panel, and considering molecular markers have become essential components of the diagnosis.
Author Contributions
J.M.G. and R.C.O. both contributed equally to this manuscript, namely in the conceptualization, data acquisition, manuscript drafting and reviewing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| a-SMA | Alpha-smooth muscle actin |
| APC | Adenomatous polyposis coli |
| FISH | Fluorescence In Situ Hybridization |
| GI | Gastro intestinal |
| GIST | Gastrointestinal stromal tumor |
| IMT | inflammatory myofibroblastic tumor |
| LMS | Leiomyosarcoma |
| MEN | Multiple endocrine neoplasia |
| PEComas | Perivascular epithelioid cell tumors |
| VM | Vascular Malformations |
References
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA A Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Waidhauser, J.; Bornemann, A.; Trepel, M.; Märkl, B. Frequency, localization, and types of gastrointestinal stromal tumor-associated neoplasia. World J. Gastroenterol. 2019, 25, 4261–4277. [Google Scholar] [CrossRef] [PubMed]
- Güller, U.; Tarantino, I.; Cerny, T.; Schmied, B.M.; Warschkow, R. Population-based SEER trend analysis of overall and cancer-specific survival in 5138 patients with gastrointestinal stromal tumor. BMC Cancer 2015, 15, 557. [Google Scholar] [CrossRef] [PubMed]
- Sbaraglia, M.; Businello, G.; Bellan, E.; Fassan, M.; Tos, A.P.D. Mesenchymal tumours of the gastrointestinal tract. Pathologica 2021, 113, 230–251. [Google Scholar] [CrossRef]
- Shi, H.; Wei, L.; Sun, L.; Guo, A. Primary gastric inflammatory myofibroblastic tumor: A clinicopathologic and immunohistochemical study of 5 cases. Pathol. Res. Pract. 2010, 206, 287–291. [Google Scholar] [CrossRef]
- Cheng, B.; Yang, C.; Liu, Z.; Liu, L.; Zhou, L. Primary gastric inflammatory myofibroblastic tumor. Medicine 2018, 97, e13423. [Google Scholar] [CrossRef]
- Antonescu, C.R.; Suurmeijer, A.J.; Zhang, L.; Sung, Y.-S.; Jungbluth, A.A.; Travis, W.D.; Al-Ahmadie, H.; Fletcher, C.D.; Alaggio, R. Molecular Characterization of Inflammatory Myofibroblastic Tumors With Frequent ALK and ROS1 Gene Fusions and Rare Novel RET Rearrangement. Am. J. Surg. Pathol. 2015, 39, 957–967. [Google Scholar] [CrossRef]
- Lee, C.-J.; Schöffski, P.; Modave, E.; van Wezel, T.; Boeckx, B.; Sufliarsky, J.; Gelderblom, H.; Blay, J.-Y.; Debiec-Rychter, M.; Sciot, R.; et al. Comprehensive Molecular Analysis of Inflammatory Myofibroblastic Tumors Reveals Diverse Genomic Landscape and Potential Predictive Markers for Response to Crizotinib. Clin. Cancer Res. 2021, 27, 6737–6748. [Google Scholar] [CrossRef]
- Harada, R.; Ohtaki, M.; Hashizume, N.; Takeshi, A.; Murai, E.; Shirahata, Y.; Suzuki, S.; Uchigasaki, S.; Yoshida, H. Inflammatory myofibroblastic tumor of the small intestine with intussusception in a child: Case report and literature review. J. Pediatr. Surg. Case Rep. 2020, 56, 101423. [Google Scholar] [CrossRef]
- Ribeiro, M.C.B.; Lopes, L.R.; Neto, J.C.d.S.; Meirelles, L.R.; de Carvalho, R.B.; Andreollo, N.A. Rare Gastric Inflammatory Myofibroblastic Tumor in an Adult Woman: A Case Report with Review of the Literature. Case Rep. Med. 2012, 2012, 374070. [Google Scholar] [CrossRef]
- Abrantes, C.F.C.; Silva, M.R.; Oliveira, R.C.; Eloy, C.; Cipriano, M.A.; Castro, L.P. Inflammatory myofibroblastic tumour arising incidentally as a polypoid lesion in the gallbladder Tumor miofibroblástico inflamatório surgindo incidentalmente como lesão polipoide na vesícula biliar. J. Bras. Patol. Med. Lab. 2015, 51, 422–426. [Google Scholar] [CrossRef]
- Siemion, K.; Reszec-Gielazyn, J.; Kisluk, J.; Roszkowiak, L.; Zak, J.; Korzynska, A. What do we know about inflammatory myofibroblastic tumors?—A systematic review. Adv. Med. Sci. 2022, 67, 129–138. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Gros, L.; Tos, A.P.D.; Jones, R.L.; Digklia, A. Inflammatory Myofibroblastic Tumour: State of the Art. Cancers 2022, 14, 3662. [Google Scholar] [CrossRef]
- Xu, P.; Shen, P.; Jin, Y.; Wang, L.; Wu, W. Epithelioid inflammatory myofibroblastic sarcoma of stomach: Diagnostic pitfalls and clinical characteristics. Int. J. Clin. Exp. Pathol. 2019, 12, 1738–1744. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6947137/ (accessed on 6 December 2023).
- Ganeshan, D.; Amini, B.; Nikolaidis, P.; Assing, M.; Vikram, R. Current Update on Desmoid Fibromatosis. J. Comput. Assist. Tomogr. 2019, 43, 29–38. [Google Scholar] [CrossRef]
- Xiao, J.; Mao, J.; Li, B. Clinical Characteristics and Treatment of Intra-abdominal Aggressive Fibromatosis: A Retrospective Study of 16 Patients. Front. Med. 2020, 7, 2. [Google Scholar] [CrossRef]
- Lips, D.; Barker, N.; Clevers, H.; Hennipman, A. The role of APC and beta-catenin in the aetiology of aggressive fibromatosis (Desmoid tumors). Eur. J. Surg. Oncol. (EJSO) 2009, 35, 3–10. [Google Scholar] [CrossRef]
- Sioda, N.A.; Wakim, A.A.; Wong, T.; Patel, S.; Coan, K.; Row, D. A Large Sporadic Intra-abdominal Desmoid-Type Fibromatosis in a Young Male: A Case Report. Front. Surg. 2020, 7, 60. [Google Scholar] [CrossRef]
- Enzo, M.; Rastrelli, M.; Rossi, C.; Hladnik, U.; Segat, D. The Wnt/β-catenin pathway in human fibrotic-like diseases and its eligibility as a therapeutic target. Mol. Cell. Ther. 2015, 3, 1. [Google Scholar] [CrossRef]
- McLean, T.D.; Duchi, S.; Di Bella, C. Molecular Pathogenesis of Sporadic Desmoid Tumours and Its Implications for Novel Therapies: A Systematised Narrative Review. Target. Oncol. 2022, 17, 223–252. [Google Scholar] [CrossRef]
- Zreik, R.T.; Fritchie, K.J. Morphologic Spectrum of Desmoid-Type Fibromatosis. Am. J. Clin. Pathol. 2016, 145, 332–340. [Google Scholar] [CrossRef]
- Bhattacharya, B.; Dilworth, H.P.; Iacobuzio-Donahue, C.; Ricci, F.; Weber, K.; A Furlong, M.; Fisher, C.M.; Montgomery, E. Nuclear β-Catenin Expression Distinguishes Deep Fibromatosis From Other Benign and Malignant Fibroblastic and Myofibroblastic Lesions. Am. J. Surg. Pathol. 2005, 29, 653–659. [Google Scholar] [CrossRef]
- Gao, C.; Wang, Y.; Broaddus, R.; Sun, L.; Xue, F.; Zhang, W. Exon 3 mutations of CTNNB1 drive tumorigenesis: A review. Oncotarget 2017, 9, 5492–5508. [Google Scholar] [CrossRef]
- Sturt, N.J.H.; Gallagher, M.C.; Bassett, P.; Philp, C.R.; Neale, K.F.; Tomlinson, I.P.M.; Silver, A.R.J.; Phillips, R.K.S. Evidence for genetic predisposition to desmoid tumours in familial adenomatous polyposis independent of the germline APC mutation. Gut 2004, 53, 1832–1836. [Google Scholar] [CrossRef]
- Howard, J.H.; Pollock, R.E. Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis. Oncol. Ther. 2016, 4, 57–72. [Google Scholar] [CrossRef]
- Ghert, M.; Yao, X.; Corbett, T.; Gupta, A.; Kandel, R.; Verma, S.; Werier, J. Treatment and Follow-Up Strategies in Desmoid Tumours: A Practice Guideline. Curr. Oncol. 2014, 21, 642–649. [Google Scholar] [CrossRef]
- Zhang, Z.; Shi, J.; Yang, T.; Liu, T.; Zhang, K. Management of aggressive fibromatosis (Review). Oncol. Lett. 2020, 21, 1. [Google Scholar] [CrossRef]
- Testa, S.; Bui, N.Q.; Charville, G.W.; Avedian, R.S.; Steffner, R.; Ghanouni, P.; Mohler, D.G.; Ganjoo, K.N. Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting. Cancers 2022, 14, 3907. [Google Scholar] [CrossRef]
- Van Broekhoven, D.L.M.; Verhoef, C.; Grünhagen, D.J.; van Gorp, J.M.H.H.; Bakker, M.A.D.; Hinrichs, J.W.J.; de Voijs, C.M.A.; van Dalen, T. Prognostic Value of CTNNB1 Gene Mutation in Primary Sporadic Aggressive Fibromatosis. Ann. Surg. Oncol. 2014, 22, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Martin-Broto, J.; Mondaza-Hernandez, J.L.; Moura, D.S.; Hindi, N. A Comprehensive Review on Solitary Fibrous Tumor: New Insights for New Horizons. Cancers 2021, 13, 2913. [Google Scholar] [CrossRef] [PubMed]
- Inayat, F.; Hussain, Q.; Shafique, K.; Hurairah, A.; Grossman, E.B. Solitary Fibrous Tumor of the Stomach. ACG Case Rep. J. 2017, 4, e35. [Google Scholar] [CrossRef]
- Kimmel, J.; Dikman, A.; Hajdu, C. Gastric Solitary Fibrous Tumor Causing Upper Gastrointestinal Bleeding. ACG Case Rep. J. 2019, 6, e00005. [Google Scholar] [CrossRef]
- Vogels, R.J.; Vlenterie, M.; Versleijen-Jonkers, Y.M.; Ruijter, E.; Bekers, E.M.; Verdijk, M.A.; Link, M.M.; Bonenkamp, J.J.; van der Graaf, W.T.; Slootweg, P.J.; et al. Solitary fibrous tumor—Clinicopathologic, immunohistochemical and molecular analysis of 28 cases. Diagn. Pathol. 2014, 9, 224. [Google Scholar] [CrossRef]
- Park, H.K.; Yu, D.B.; Sung, M.; Oh, E.; Kim, M.; Song, J.-Y.; Lee, M.-S.; Jung, K.; Noh, K.-W.; An, S.; et al. Molecular changes in solitary fibrous tumor progression. J. Mol. Med. 2019, 97, 1413–1425. [Google Scholar] [CrossRef] [PubMed]
- Georgiesh, T.; Namløs, H.M.; Sharma, N.; Lorenz, S.; Myklebost, O.; Bjerkehagen, B.; Meza-Zepeda, L.A.; Boye, K. Clinical and molecular implications of NAB2-STAT6 fusion variants in solitary fibrous tumour. Pathology 2021, 53, 713–719. [Google Scholar] [CrossRef]
- Lee, J.-C.; Fletcher, C.D. Malignant Fat-Forming Solitary Fibrous Tumor (so-called “Lipomatous Hemangiopericytoma”). Am. J. Surg. Pathol. 2011, 35, 1177–1185. [Google Scholar] [CrossRef]
- A Doyle, L.; Vivero, M.; Fletcher, C.D.; Mertens, F.; Hornick, J.L. Nuclear expression of STAT6 distinguishes solitary fibrous tumor from histologic mimics. Mod. Pathol. 2014, 27, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Demicco, E.G.; Wagner, M.J.; Maki, R.G.; Gupta, V.; Iofin, I.; Lazar, A.J.; Wang, W.-L. Risk assessment in solitary fibrous tumors: Validation and refinement of a risk stratification model. Mod. Pathol. 2017, 30, 1433–1442. [Google Scholar] [CrossRef]
- Salas, S.; Resseguier, N.; Blay, J.Y.; Le Cesne, A.; Italiano, A.; Chevreau, C.; Rosset, P.; Isambert, N.; Soulie, P.; Cupissol, D.; et al. Prediction of local and metastatic recurrence in solitary fibrous tumor: Construction of a risk calculator in a multicenter cohort from the French Sarcoma Group (FSG) database. Ann. Oncol. 2017, 28, 1779–1787. [Google Scholar] [CrossRef]
- Voth, E.; Serio, S.; Gross, J.; Singh, A.; Dietz, N.; Nandipati, K. Solitary fibrous tumor of the stomach with high-grade sarcomatous dedifferentiation. J. Surg. Case Rep. 2018, 2018, rjy307. [Google Scholar] [CrossRef] [PubMed]
- Davanzo, B.; Emerson, R.E.; Lisy, M.; Koniaris, L.G.; Kays, J.K. Solitary fibrous tumor. Transl. Gastroenterol. Hepatol. 2018, 3, 94. [Google Scholar] [CrossRef]
- Kumar, S.; Harisankar, A.; Singh, R.; Kumar, A.; Kumar, B.; Mandal, M. Lipoma of the gastrointestinal tract: A tertiary care centre experience. Ind. Mark. Manag. 2023. [Google Scholar] [CrossRef]
- Caliskan, A.; Kohlmann, W.K.; E Affolter, K.; Downs-Kelly, E.; Kanth, P.; Bronner, M.P. Intramucosal lipomas of the colon implicate Cowden syndrome. Mod. Pathol. 2018, 31, 643–651. [Google Scholar] [CrossRef]
- Kastanakis, M.; Anyfantakis, D.; Symvoulakis, E.K.; Katsougris, N.; Papadomichelakis, A.; Kokkinos, I.; Petrakis, G.; Bobolakis, E. Cecal Lipoma Presenting as Acute Intestinal Obstruction in an Elderly Woman: A Case Report. Case Rep. Surg. 2013, 2013, 1–3. [Google Scholar] [CrossRef]
- Rezaii, S.; Enshaii, A.; Zahedi, A.; Amestejani, M.; Herik Dizaji, M. Gastrointestinal bleeding due to gastrointestinal lipoma: A case report. Casp. J. Intern. Med. 2021, 12, 622. [Google Scholar] [CrossRef]
- Garmpis, N.; Damaskos, C.; Garmpi, A.; Georgakopoulou, V.E.; Sakellariou, S.; Liakea, A.; Schizas, D.; Diamantis, E.; Farmaki, P.; Voutyritsa, E.; et al. Inflammatory Fibroid Polyp of the Gastrointestinal Tract: A Systematic Review for a Benign Tumor. In Vivo 2021, 35, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Klingbeil, K.D.; Balaban, A.; Fertig, R.M.; Gamret, A.C.; Gong, Y.; Torres, C.; Satahoo, S.S. Inflammatory fibroid polyp of the gastric antrum presenting as hypovolemic shock: Case report and literature review. Intractable Rare Dis. Res. 2017, 6, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Gadoura, A.; Mohammed, F.; Abdulkarim, M.; Ibn Yasir, A.; Shani, D.; Salih, N. Inflammatory fibroid polyp (Vanek’s tumor) causing double compound ileo-ileal intussusception in an adult patient, a case report. Int. J. Surg. Case Rep. 2022, 93, 106947. [Google Scholar] [CrossRef]
- Maccagno, A.; Sander, B.; Dintner, S.; Harloff, M.; Füzesi, L.; Märkl, B. Inflammatory fibroid polyp: A series of 29 cases and a systematic review of the literature. Hum. Pathol. Rep. 2023, 32. [Google Scholar] [CrossRef]
- Huss, S.; Wardelmann, E.; Goltz, D.; Binot, E.; Hartmann, W.; Merkelbach-Bruse, S.; Büttner, R.; Schildhaus, H. Activating PDGFRA mutations in inflammatory fibroid polyps occur in exons 12, 14 and 18 and are associated with tumour localization. Histopathology 2012, 61, 59–68. [Google Scholar] [CrossRef]
- Almaghrabi, H.; Almaghrabi, M.; Al-Maghrabi, H. Giant Ileocecal Inflammatory Fibroid Polyp: Unique Clinical Presentation. Case Rep. Surg. 2020, 2020, 8811404. [Google Scholar] [CrossRef]
- Lasota, J.; Wang, Z.-F.; Sobin, L.H.; Miettinen, M. Gain-of-function PDGFRA mutations, earlier reported in gastrointestinal stromal tumors, are common in small intestinal inflammatory fibroid polyps. A study of 60 cases. Mod. Pathol. 2009, 22, 1049–1056. [Google Scholar] [CrossRef]
- Tang, Y.-S.; Liu, L.; Gao, Y.; He, Q.-C.; Guo, H.-M.; Zhao, Z.-F. Minimally invasive colonoscopy treatment of inflammatory fibroid polyps in the terminal ileum. Sci. Rep. 2023, 13, 4929. [Google Scholar] [CrossRef]
- Lin, M.M.; Song, L.M.; Qin, S.M.; Li, D.M.; Hou, G.B.; Li, X. Plexiform fibromyxoma. Medicine 2021, 100, e27164. [Google Scholar] [CrossRef]
- Higashi, M.; Hamada, T.; Sasaki, K.; Tsuruda, Y.; Shimonosono, M.; Kitazono, I.; Kirishima, M.; Tasaki, T.; Noguchi, H.; Tabata, K.; et al. Esophageal plexiform fibromyxoma: A case report with molecular analysis for MALAT1-GLI1 fusion. Pathol. - Res. Pract. 2022, 233, 153878. [Google Scholar] [CrossRef]
- Arslan, M.E.; Li, H.; Fu, Z.; A Jennings, T.; Lee, H. Plexiform fibromyxoma: Review of rare mesenchymal gastric neoplasm and its differential diagnosis. World J. Gastrointest. Oncol. 2021, 13, 409–423. [Google Scholar] [CrossRef]
- Sugimura, N.; Kubota, E.; Sasaki, M.; Fukusada, S.; Mizuno, Y.; Iwasaki, H.; Tanaka, M.; Ozeki, K.; Shimura, T.; Kataoka, H. A case of asymptomatic gastric plexiform fibromyxoma followed up for 3 years. DEN Open 2023, 4, e291. [Google Scholar] [CrossRef] [PubMed]
- Altameemi, H.; A Asghar, I. Gastric Plexiform Fibromyxoma: A Rare Clinical Entity. Am. J. Clin. Pathol. 2022, 158, S55–S56. [Google Scholar] [CrossRef]
- Miettinen, M.; Makhlouf, H.R.; Sobin, L.H.; Lasota, J. Plexiform fibromyxoma: A distinctive benign gastric antral neoplasm not to be confused with a myxoid GIST. Am. J. Surg. Pathol. 2009, 33, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Su, H.-A.; Yen, H.-H.; Chen, C.-J. An Update on Clinicopathological and Molecular Features of Plexiform Fibromyxoma. Can. J. Gastroenterol. Hepatol. 2019, 2019, 3960920. [Google Scholar] [CrossRef]
- Senapathi, H.; Morada, A.; Perry, M.; Bertram, C.; Yeung, E.; Sultany, M.; Bertsch, D.; Cagir, B. Prognostic Factors in Gastrointestinal Leiomyosarcomas: An Analysis Using the Surveillance, Epidemiology, and End Results (SEER) Database. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Yamamoto, H.; Handa, M.; Tobo, T.; Setsu, N.; Fujita, K.; Oshiro, Y.; Mihara, Y.; Yoshikawa, Y.; Oda, Y. Clinicopathological features of primary leiomyosarcoma of the gastrointestinal tract following recognition of gastrointestinal stromal tumours. Histopathology 2013, 63, 194–207. [Google Scholar] [CrossRef]
- Hilal, L.; Barada, K.; Mukherji, D.; Temraz, S.; Shamseddine, A. Gastrointestinal (GI) leiomyosarcoma (LMS) case series and review on diagnosis, management, and prognosis. Med. Oncol. 2016, 33, 20. [Google Scholar] [CrossRef]
- Alpert, L.; Al-Sabti, R.; Graham, R.P.; Pai, R.K.; Gonzalez, R.S.; Zhang, X.; Smith, V.; Wang, H.L.; Westbrook, L.; Goldblum, J.R.; et al. Smooth muscle tumors of the gastrointestinal tract: An analysis of prognostic features in 407 cases. Mod. Pathol. 2020, 33, 1410–1419. [Google Scholar] [CrossRef]
- Demicco, E.G.; Boland, G.M.; Savannah, K.J.B.; Lusby, K.; Young, E.D.; Ingram, D.; Watson, K.L.; Bailey, M.; Guo, X.; Hornick, J.L.; et al. Progressive loss of myogenic differentiation in leiomyosarcoma has prognostic value. Histopathology 2014, 66, 627–638. [Google Scholar] [CrossRef]
- Aggarwal, G.; Sharma, S.; Zheng, M.; Reid, M.D.; Crosby, J.H.; Chamberlain, S.M.; Nayak-Kapoor, A.; Lee, J.R. Primary leiomyosarcomas of the gastrointestinal tract in the post–gastrointestinal stromal tumor era. Ann. Diagn. Pathol. 2012, 16, 532–540. [Google Scholar] [CrossRef]
- Agaimy, A.; Wünsch, P.H. True smooth muscle neoplasms of the gastrointestinal tract: Morphological spectrum and classification in a series of 85 cases from a single institute. Langenbeck’s Arch. Surg. 2006, 392, 75–81. [Google Scholar] [CrossRef]
- Mellish, R. Multiple hemangiomas of the gastrointestinal tract in children. Am. J. Surg. 1971, 121, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S. GI-Associated Hemangiomas and Vascular Malformations. Clin. Colon Rectal Surg. 2011, 24, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Handra-Luca, A.; Montgomery, E. Vascular malformations and hemangiolymphangiomas of the gastrointestinal tract: Morphological features and clinical impact. Int. J. Clin. Exp. Pathol. 2011, 4, 430–443. [Google Scholar]
- Roisman, I.; Manny, J.; Fields, S.; Shiloni, E. Intra-abdominal lymphangioma. Br. J. Surg. 1989, 76, 485–489. [Google Scholar] [CrossRef]
- Wiegand, S.; Eivazi, B.; Barth, P.J.; von Rautenfeld, D.B.; Folz, B.J.; Mandic, R.; Werner, J.A. Pathogenesis of lymphangiomas. Virchows Arch. 2008, 453, 1–8. [Google Scholar] [CrossRef]
- Hornick, J.L.; Fletcher, C.D. Intraabdominal cystic lymphangiomas obscured by marked superimposed reactive changes: Clinicopathological analysis of a series. Hum. Pathol. 2005, 36, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Ho-Yen, C.; Chang, F.; van der Walt, J.; Lucas, S. Gastrointestinal Malignancies in HIV-infected or Immunosuppressed Patients. Adv. Anat. Pathol. 2007, 14, 431–443. [Google Scholar] [CrossRef]
- Hengge, U.R.; Ruzicka, T.; Tyring, S.K.; Stuschke, M.; Roggendorf, M.; A Schwartz, R.; Seeber, S. Update on Kaposi’s sarcoma and other HHV8 associated diseases. Part 1: Epidemiology, environmental predispositions, clinical manifestations, and therapy. Lancet Infect. Dis. 2002, 2, 281–292. [Google Scholar] [CrossRef]
- Barrison, I.G.; Foster, S.; Harris, J.W.; Pinching, A.J.; Walker, J.G. Upper gastrointestinal Kaposi’s sarcoma in patients positive for HIV antibody without cutaneous disease. BMJ 1988, 296, 92–93. [Google Scholar] [CrossRef]
- Nagata, N.; Shimbo, T.; Yazaki, H.; Asayama, N.; Akiyama, J.; Teruya, K.; Igari, T.; Ohmagari, N.; Oka, S.; Uemura, N. Predictive Clinical Factors in the Diagnosis of Gastrointestinal Kaposi’s Sarcoma and Its Endoscopic Severity. PLoS ONE 2012, 7, e46967. [Google Scholar] [CrossRef]
- Zheng, W.; Obeng, R.C.; Graham, R.P.M.; Lui, S.; Cheng, J.; Alexiev, B.A.; Quigley, B.; Krasinskas, A.; Yang, G.-Y.; Escobar, D.; et al. Histologic Variants of Kaposi Sarcoma in the Gastrointestinal Tract. Am. J. Surg. Pathol. 2022, 46, 1500–1506. [Google Scholar] [CrossRef] [PubMed]
- Robin, Y.-M.; Guillou, L.; Michels, J.-J.; Coindre, J.-M. Human Herpesvirus 8 Immunostaining: A Sensitive and Specific Method for Diagnosing Kaposi Sarcoma in Paraffin-Embedded Sections. Am. J. Clin. Pathol. 2004, 121, 330–334. [Google Scholar] [CrossRef]
- IARC. WHO Classification of Soft Tissue and Bone Tumours; IARC: Geneva, Switzerland, 2020. [Google Scholar]
- Allison, K.H.; Yoder, B.J.; Bronner, M.P.; Goldblum, J.R.; Rubin, B.P. Angiosarcoma Involving the Gastrointestinal Tract. Am. J. Surg. Pathol. 2004, 28, 298–307. [Google Scholar] [CrossRef]
- Schizas, D.; Mastoraki, A.; Giannakodimos, I.; Giannakodimos, A.; Ziogou, A.; Katsaros, I.; Frountzas, M.; Koutelidakis, I.; Vassiliu, P.; Pikoulis, E. Primary Angiosarcoma of the Gastrointestinal Tract: A Systematic Review of the Literature. J. Investig. Surg. 2020, 35, 400–408. [Google Scholar] [CrossRef]
- Guillou, L.; Aurias, A. Soft tissue sarcomas with complex genomic profiles. Virchows Arch. 2009, 456, 201–217. [Google Scholar] [CrossRef]
- Italiano, A.; Chen, C.; Thomas, R.; Breen, M.; Bonnet, F.; Sevenet, N.; Longy, M.; Maki, R.G.; Coindre, J.; Antonescu, C.R. Alterations of the p53 and PIK3CA/AKT/mTOR pathways in angiosarcomas: A pattern distinct from other sarcomas with complex genomics. Cancer 2012, 118, 5878–5887. [Google Scholar] [CrossRef]
- Itakura, E.; Yamamoto, H.; Oda, Y.; Tsuneyoshi, M. Detection and characterization of vascular endothelial growth factors and their receptors in a series of angiosarcomas. J. Surg. Oncol. 2007, 97, 74–81. [Google Scholar] [CrossRef]
- Young, R.J.; Brown, N.J.; Reed, M.W.; Hughes, D.; Woll, P.J. Angiosarcoma. Lancet Oncol. 2010, 11, 983–991. [Google Scholar] [CrossRef]
- Huang, S.-C.; Zhang, L.; Sung, Y.-S.M.; Chen, C.-L.M.; Kao, Y.-C.; Agaram, N.P.M.; Singer, S.; Tap, W.D.; D’angelo, S.; Antonescu, C.R. Recurrent CIC Gene Abnormalities in Angiosarcomas. Am. J. Surg. Pathol. 2016, 40, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Behjati, S.; Tarpey, P.S.; Sheldon, H.; Martincorena, I.; Van Loo, P.; Gundem, G.; Wedge, D.C.; Ramakrishna, M.; Cooke, S.L.; Pillay, N.; et al. Recurrent PTPRB and PLCG1 mutations in angiosarcoma. Nat. Genet. 2014, 46, 376–379. [Google Scholar] [CrossRef]
- Hogeboom-Gimeno, A.; van Ravensteijn, S.; Desar, I.; Hillebrandt-Roeffen, M.; van Cleef, P.; Bonenkamp, J.; Flucke, U.; Versleijen-Jonkers, Y. MYC amplification in angiosarcoma depends on etiological/clinical subgroups–Diagnostic and prognostic value. Ann. Diagn. Pathol. 2023, 63, 152096. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gong, H.; Wang, Y.; Zhang, G.; Hou, P. Angiosarcoma of the visceral organs: A morphological, immunohistochemical, and C-MYC status analysis. Pathol.-Res. Pract. 2022, 238, 154118. [Google Scholar] [CrossRef]
- Meis-Kindblom, J.M.; Kindblom, L.-G. Angiosarcoma of Soft Tissue. Am. J. Surg. Pathol. 1998, 22, 683–697. [Google Scholar] [CrossRef]
- Pusztaszeri, M.P.; Seelentag, W.; Bosman, F.T. Immunohistochemical Expression of Endothelial Markers CD31, CD34, von Willebrand Factor, and Fli-1 in Normal Human Tissues. J. Histochem. Cytochem. 2006, 54, 385–395. [Google Scholar] [CrossRef]
- Miettinen, M.; Wang, Z.-F.; Paetau, A.; Tan, S.-H.; Dobi, A.; Srivastava, S.; Sesterhenn, I. ERG Transcription Factor as an Immunohistochemical Marker for Vascular Endothelial Tumors and Prostatic Carcinoma. Am. J. Surg. Pathol. 2011, 35, 432–441. [Google Scholar] [CrossRef]
- Folpe, A.L.; Chand, E.M.; Goldblum, J.R.; Weiss, S.W. Expression of Fli-1, a Nuclear Transcription Factor, Distinguishes Vascular Neoplasms from Potential Mimics. Am. J. Surg. Pathol. 2001, 25, 1061–1066. [Google Scholar] [CrossRef]
- Alles, J.U.; Bosslet, K. Immunocytochemistry of Angiosarcomas: A Study of 19 Cases with Special Emphasis on the Applicability of Endothelial Cell Specific Markers to Routinely Prepared Tissues. Am. J. Clin. Pathol. 1988, 89, 463–471. [Google Scholar] [CrossRef]
- Fayette, J.; Martin, E.; Piperno-Neumann, S.; Le Cesne, A.; Robert, C.; Bonvalot, S.; Ranchère, D.; Pouillart, P.; Coindre, J.M.; Blay, J.Y. Angiosarcomas, a heterogeneous group of sarcomas with specific behavior depending on primary site: A retrospective study of 161 cases. Ann. Oncol. 2007, 18, 2030–2036. [Google Scholar] [CrossRef]
- Girard, N.; Marin, C.; Hélias-Rodzewicz, Z.; Villa, C.; Julié, C.; de Lajarte-Thirouard, A.; de Beauce, S.M.; Lagorce-Pages, C.; Renaud, F.; Cazals-Hatem, D.; et al. CARMN-NOTCH2 fusion transcript drives high NOTCH2 expression in glomus tumors of the upper digestive tract. Genes Chromosom. Cancer 2021, 60, 723–732. [Google Scholar] [CrossRef]
- Miettinen, M.M.; Paal, E.M.; Lasota, J.M.; Sobin, L.H.M. Gastrointestinal glomus tumors: A clinicopathologic, immunohistochemical, and molecular genetic study of 32 cases. Am. J. Surg. Pathol. 2002, 26, 301–311. [Google Scholar] [CrossRef]
- Folpe, A.L.M.; Fanburg–Smith, J.C.M.; Miettinen, M.M.; Weiss, S.W.M. Atypical and malignant glomus tumors: Analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am. J. Surg. Pathol. 2001, 25, 1–12. [Google Scholar] [CrossRef]
- Bozdogan, N.; Dilek, G.B.; Benzer, E.; Karadeniz, M.; Bozdogan, O. Transducing-Like Enhancer of Split 1: A Potential Immunohistochemical Marker for Glomus Tumor. Am. J. Dermatopathol. 2017, 39, 524–527. [Google Scholar] [CrossRef]
- Dervan, P.A.; Tobbia, I.N.; Casey, M.; O’Loughlin, J.; O’Brien, M. Glomus tumours: An immunohistochemical profile of 11 cases. Histopathology 1989, 14, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Mosquera, J.; Sboner, A.; Zhang, L.; Chen, C.; Sung, Y.; Chen, H.; Agaram, N.P.; Briskin, D.; Basha, B.M.; Singer, S.; et al. Novel MIR143-NOTCH fusions in benign and malignant glomus tumors. Genes, Chromosom. Cancer 2013, 52, 1075–1087. [Google Scholar] [CrossRef]
- Agaram, N.P.M.; Zhang, L.; Jungbluth, A.A.; Dickson, B.C.; Antonescu, C.R. A Molecular Reappraisal of Glomus Tumors and Related Pericytic Neoplasms with Emphasis on NOTCH-gene Fusions. Am. J. Surg. Pathol. 2020, 44, 1556–1562. [Google Scholar] [CrossRef]
- Chakrapani, A.; Warrick, A.; Nelson, D.; Beadling, C.; Corless, C.L. BRAF and KRAS Mutations in Sporadic Glomus Tumors. Am. J. Dermatopathol. 2012, 34, 533–535. [Google Scholar] [CrossRef]
- Dashti, N.K.; Bahrami, A.; Lee, S.J.; Jenkins, S.M.; Rodriguez, F.J.; Folpe, A.L.; Boland, J.M. BRAF V600E Mutations Occur in a Subset of Glomus Tumors, and Are Associated With Malignant Histologic Characteristics. Am. J. Surg. Pathol. 2017, 41, 1532–1541. [Google Scholar] [CrossRef]
- Papke, D.J.J.; Sholl, L.M.; Doyle, L.A.; Fletcher, C.D.M.; Hornick, J.L. Gastroesophageal Glomus Tumors: Clinicopathologic and Molecular Genetic Analysis of 26 Cases with a Proposal for Malignancy Criteria. Am. J. Surg. Pathol. 2022, 46, 1436–1446. [Google Scholar] [CrossRef]
- Folpe, A.L.; Mentzel, T.; Lehr, H.-A.; Fisher, C.; Balzer, B.L.; Weiss, S.W. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: A clinicopathologic study of 26 cases and review of the literature. Am. J. Surg. Pathol. 2005, 29, 1558–1575. [Google Scholar] [CrossRef]
- Lomdo, M.; Setti, K.; Oukabli, M.; Moujahid, M.; Bounaim, A. Gastric schwannoma: A diagnosis that should be known in 2019. J. Surg. Case Rep. 2020, 2020, rjz382. [Google Scholar] [CrossRef]
- Mekras, A.; Krenn, V.; Perrakis, A.; Croner, R.S.; Kalles, V.; Atamer, C.; Grützmann, R.; Vassos, N. Gastrointestinal schwannomas: A rare but important differential diagnosis of mesenchymal tumors of gastrointestinal tract. BMC Surg. 2018, 18, 47. [Google Scholar] [CrossRef]
- Crinò, S.; Bernardoni, L.; Manfrin, E.; Parisi, A.; Gabbrielli, A. Endoscopic ultrasound features of pancreatic schwannoma. Endosc. Ultrasound 2016, 5, 396–398. [Google Scholar] [CrossRef]
- Kudose, S.; Kyriakos, M.; Awad, M.M. Gastric plexiform schwannoma in association with neurofibromatosis type 2. Clin. J. Gastroenterol. 2016, 9, 352–357. [Google Scholar] [CrossRef]
- Yoon, H.Y.; Kim, C.B.; Lee, Y.H.; Kim, H.G. Gastric Schwannoma. Yonsei Med. J. 2008, 49, 1052–1054. [Google Scholar] [CrossRef]
- Radaelli, F.; Minoli, G. Granular Cell Tumors of the Gastrointestinal Tract: Questions and Answers. Gastroenterol. Hepatol. 2009, 5, 798. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2886372/ (accessed on 9 December 2023).
- Chen, Y.; Chen, Y.; Chen, X.; Chen, L.; Liang, W. Colonic granular cell tumor: Report of 11 cases and management with review of the literature. Oncol. Lett. 2018, 16, 1419–1424. [Google Scholar] [CrossRef]
- Marcoval, J.; Bauer-Alonso, A.; Llobera-Ris, C.; Moreno-Vílchez, C.; Penín, R.; Bermejo, J. Granular Cell Tumor: A Clinical Study of 81 Patients. Actas Dermo-Sifiliográficas 2021, 112, 441–446. [Google Scholar] [CrossRef]
- Castagna, J.; Clerc, J.; Dupond, A.-S.; Laresche, C. Multiple granular cell tumours in a patient with Noonan’s syndrome and juvenile myelomonocytic leukemia. Ann. Dermatol. Venereol. 2017, 144, 705–711. [Google Scholar] [CrossRef]
- Schrader, K.; Nelson, T.; De Luca, A.; Huntsman, D.; McGillivray, B. Multiple granular cell tumors are an associated feature of LEOPARD syndrome caused by mutation in PTPN11. Clin. Genet. 2009, 75, 185–189. [Google Scholar] [CrossRef]
- Pareja, F.; Brandes, A.H.; Basili, T.; Selenica, P.; Geyer, F.C.; Fan, D.; Da Cruz Paula, A.; Kumar, R.; Brown, D.N.; Gularte-Mérida, R.; et al. Loss-of-function mutations in ATP6AP1 and ATP6AP2 in granular cell tumors. Nat. Commun. 2018, 9, 3533. [Google Scholar] [CrossRef]
- Katiyar, V.; Vohra, I.; Uprety, A.; Yin, W.; Gupta, S. Recurrent Unresectable Malignant Granular Cell Tumor with Response to Pazopanib. Cureus 2020, 12, e8287. [Google Scholar] [CrossRef]
- Morita, S.; Hiramatsu, M.; Sugishita, M.; Gyawali, B.; Shibata, T.; Shimokata, T.; Urakawa, H.; Mitsuma, A.; Moritani, S.; Kubota, T.; et al. Pazopanib monotherapy in a patient with a malignant granular cell tumor originating from the right orbit: A case report. Oncol. Lett. 2015, 10, 972–974. [Google Scholar] [CrossRef]
- van Wyk, A.C.; van Zyl, H.; Rigby, J. Colonic perineurioma (benign fibroblastic polyp): Case report and review of the literature. Diagn. Pathol. 2018, 13, 16. [Google Scholar] [CrossRef]
- Tsuchiya, T.; Iwaya, Y.; Iwaya, M.; Okamura, T.; Nagaya, T.; Umemura, T. A Case of Multiple Perineuriomas in the Colon with Underlying Neurofibromatosis Type I. ACG Case Rep. J. 2021, 8, e00665. [Google Scholar] [CrossRef]
- Agaimy, A.; Stoehr, R.; Vieth, M.; Hartmann, A. Benign Serrated Colorectal Fibroblastic Polyps/Intramucosal Perineuriomas Are True Mixed Epithelial-stromal Polyps (Hybrid Hyperplastic Polyp/Mucosal Perineurioma) With Frequent BRAF Mutations. Am. J. Surg. Pathol. 2010, 34, 1663–1671. [Google Scholar] [CrossRef]
- Baiomi, A.; Abbas, H.; Niazi, M.; Remotti, H.; Daniel, M.; Balar, B. Colonic Ganglioneuroma: A Rare Lesion with Extremely Different Presentations and Outcomes in Two Patients. Gastroenterol. Res. 2021, 14, 194–198. [Google Scholar] [CrossRef]
- Mauro, A.; Zenzeri, L.; Esposito, F.; Gaglione, G.; Strisciuglio, C.; Pilozzi, E.; Corleto, V.D.; Ziparo, C.; Di Nardo, G. Isolated intestinal Ganglioneuromatosis: Case report and literature review. Ital. J. Pediatr. 2021, 47, 80. [Google Scholar] [CrossRef]
- Lu, C.; Qiu, Y.; Lu, X.; Li, G.; Bu, H. Synchronous diffuse ganglioneuromatosis and multiple schwannomas of the colon: A case report and literature review. Exp. Ther. Med. 2015, 9, 733–736. [Google Scholar] [CrossRef]
- Pistorius, S.; Klink, B.; Pablik, J.; Rump, A.; Aust, D.; Garzarolli, M.; Schröck, E.; Schackert, H.K. An unusual case of Cowden syndrome associated with ganglioneuromatous polyposis. Hered. Cancer Clin. Pract. 2016, 14, 11. [Google Scholar] [CrossRef]
- Bonetti, F.M.; Pea, M.M.; Martignoni, G.M.; Zamboni, G.M. PEC and Sugar. Am. J. Surg. Pathol. 1992, 16, 307–308. [Google Scholar] [CrossRef]
- Thway, K.; Fisher, C. PEComa: Morphology and genetics of a complex tumor family. Ann. Diagn. Pathol. 2015, 19, 359–368. [Google Scholar] [CrossRef]
- Pan, C.; Chung, M.; Ng, K.; Liu, C.; Wang, J.; Chai, C.; Huang, S.; Chen, P.; Ho, D. Constant allelic alteration on chromosome 16p (TSC2 gene) in perivascular epithelioid cell tumour (PEComa): Genetic evidence for the relationship of PEComa with angiomyolipoma. J. Pathol. 2008, 214, 387–393. [Google Scholar] [CrossRef]
- Agaram, N.P.; Sung, Y.-S.; Zhang, L.; Chen, C.-L.; Chen, H.-W.; Singer, S.; Dickson, M.A.; Berger, M.F.; Antonescu, C.R. Dichotomy of Genetic Abnormalities in PEComas With Therapeutic Implications. Am. J. Surg. Pathol. 2015, 39, 813–825. [Google Scholar] [CrossRef]
- Doyle, L.A.; Hornick, J.L.; Fletcher, C.D. PEComa of the Gastrointestinal tract: Clinicopathologic study of 35 cases with evaluation of prognostic parameters. Am. J. Surg. Pathol. 2013, 37, 1769–1782. [Google Scholar] [CrossRef]
- Park, S.J.; Han, D.K.; Baek, H.J.; Chung, S.Y.; Nam, J.H.; Kook, H.; Hwang, T.J. Perivascular epithelioid cell tumor (PEComa) of the ascending colon: The implication of IFN-α2b treatment. Korean J. Pediatr. 2010, 53, 975–978. [Google Scholar] [CrossRef]
- Baek, J.-H.; Chung, M.G.; Jung, D.H.; Oh, J.H. Perivascular Epithelioid Cell Tumor (Pecoma) in the Transverse Colon of an Adolescent: A Case Report. Tumori J. 2007, 93, 106–108. [Google Scholar] [CrossRef]
- Pereira, K.; Inamdar, A.A.; Zaveri, A.; Teitelbaum, J.E.; Shertz, W.; Belitsis, K. A Rare Case of a Translocation-Associated Perivascular Epithelioid Cell Neoplasm (PEComa). Case Rep. Pediatr. 2022, 2022, 7519456. [Google Scholar] [CrossRef]
- Bleeker, J.S.; Quevedo, J.F.; Folpe, A.L. “Malignant” Perivascular Epithelioid Cell Neoplasm: Risk Stratification and Treatment Strategies. Sarcoma 2012, 2012, 541626. [Google Scholar] [CrossRef]
- Argani, P.; Aulmann, S.; Illei, P.B.; Netto, G.J.; Ro, J.; Cho, H.-Y.; Dogan, S.; Ladanyi, M.; Martignoni, G.; Goldblum, J.R.; et al. A Distinctive Subset of PEComas Harbors TFE3 Gene Fusions. Am. J. Surg. Pathol. 2010, 34, 1395–1406. [Google Scholar] [CrossRef]
- Italiano, A.; Delcambre, C.; Hostein, I.; Cazeau, A.L.; Marty, M.; Avril, A.; Coindre, J.-M.; Bui, B. Treatment with the mTOR inhibitor temsirolimus in patients with malignant PEComa. Ann. Oncol. 2010, 21, 1135–1137. [Google Scholar] [CrossRef]
- Wagner, A.J.; Malinowska-Kolodziej, I.; Morgan, J.A.; Qin, W.; Fletcher, C.D.; Vena, N.; Ligon, A.H.; Antonescu, C.R.; Ramaiya, N.H.; Demetri, G.D.; et al. Clinical Activity of mTOR Inhibition with Sirolimus in Malignant Perivascular Epithelioid Cell Tumors: Targeting the Pathogenic Activation of mTORC1 in Tumors. J. Clin. Oncol. 2010, 28, 835–840. [Google Scholar] [CrossRef]
- French, C.A. NUT Carcinoma: Clinicopathologic features, pathogenesis, and treatment. Pathol. Int. 2018, 68, 583–595. [Google Scholar] [CrossRef]
- Dickson, B.C.; Sung, Y.-S.M.; Rosenblum, M.K.; Reuter, V.E.; Harb, M.; Wunder, J.S.; Swanson, D.B.; Antonescu, C.R. NUTM1 Gene Fusions Characterize a Subset of Undifferentiated Soft Tissue and Visceral Tumors. Am. J. Surg. Pathol. 2018, 42, 636–645. [Google Scholar] [CrossRef]
- Sekine, S.; Kiyono, T.; Ryo, E.; Ogawa, R.; Wakai, S.; Ichikawa, H.; Suzuki, K.; Arai, S.; Tsuta, K.; Ishida, M.; et al. Recurrent YAP1-MAML2 and YAP1-NUTM1 fusions in poroma and porocarcinoma. J. Clin. Investig. 2019, 129, 3827–3832. [Google Scholar] [CrossRef]
- Le Loarer, F.; Pissaloux, D.; Watson, S.; Godfraind, C.; Galmiche-Rolland, L.; Silva, K.; Mayeur, L.; Italiano, A.; Michot, A.; Pierron, G.; et al. Clinicopathologic Features of CIC-NUTM1 Sarcomas, a New Molecular Variant of the Family of CIC-Fused Sarcomas. Am. J. Surg. Pathol. 2019, 43, 268–276. [Google Scholar] [CrossRef]
- Van Treeck, B.J.; Thangaiah, J.J.; Torres-Mora, J.; Stevens, T.M.; Rothermundt, C.; Fassan, M.; Loupakis, F.; Diebold, J.; Hornick, J.L.; Halling, K.C.; et al. NUTM1-rearranged colorectal sarcoma: A clinicopathologically and genetically distinctive malignant neoplasm with a poor prognosis. Mod. Pathol. 2021, 34, 1547–1557. [Google Scholar] [CrossRef]
- Folpe, A.L. ‘I Can’t Keep Up!’: An update on advances in soft tissue pathology occurring after the publication of the 2020 World Health Organization classification of soft tissue and bone tumours. Histopathology 2021, 80, 54–75. [Google Scholar] [CrossRef]
- Yoshida, A. NUT carcinoma and thoracic SMARCA4-deficient undifferentiated tumour: Facts and controversies. Histopathology 2023, 84, 86–101. [Google Scholar] [CrossRef]
- Luo, W.; Stevens, T.M.; Stafford, P.; Miettinen, M.; Gatalica, Z.; Vranic, S. NUTM1-Rearranged Neoplasms—A Heterogeneous Group of Primitive Tumors with Expanding Spectrum of Histology and Molecular Alterations—An Updated Review. Curr. Oncol. 2021, 28, 4485–4503. [Google Scholar] [CrossRef]
- Atiq, M.A.; Davis, J.L.; Hornick, J.L.; Dickson, B.C.; Fletcher, C.D.M.; Fletcher, J.A.; Folpe, A.L.; Mariño-Enríquez, A. Mesenchymal tumors of the gastrointestinal tract with NTRK rearrangements: A clinicopathological, immunophenotypic, and molecular study of eight cases, emphasizing their distinction from gastrointestinal stromal tumor (GIST). Mod. Pathol. 2020, 34, 95–103. [Google Scholar] [CrossRef]
- Brenca, M.; Rossi, S.; Polano, M.; Gasparotto, D.; Zanatta, L.; Racanelli, D.; Valori, L.; Lamon, S.; Tos, A.P.D.; Maestro, R. Transcriptome sequencing identifies ETV6–NTRK3 as a gene fusion involved in GIST. J. Pathol. 2015, 238, 543–549. [Google Scholar] [CrossRef]
- Shi, E.; Chmielecki, J.; Tang, C.-M.; Wang, K.; Heinrich, M.C.; Kang, G.; Corless, C.L.; Hong, D.; Fero, K.E.; Murphy, J.D.; et al. FGFR1 and NTRK3 actionable alterations in “Wild-Type” gastrointestinal stromal tumors. J. Transl. Med. 2016, 14, 339. [Google Scholar] [CrossRef]
- Sinniah, R.P.; Roche, E.; Cameron, D. GI Synovial Sarcomas. Clin. Transl. Gastroenterol. 2012, 3, e11. [Google Scholar] [CrossRef]
- Romeo, S.; Rossi, S.; Marín, M.A.; Canal, F.; Sbaraglia, M.; Laurino, L.; Mazzoleni, G.; Montesco, M.C.; Valori, L.; Dell’orto, M.C.; et al. Primary Synovial Sarcoma (SS) of the digestive system: A molecular and clinicopathological study of fifteen cases. Clin. Sarcoma Res. 2015, 5, 7. [Google Scholar] [CrossRef]
- Requena, D.O.; Longacre, T.A.; Rosenberg, A.E.; Torres, J.M.V.; Yanchenko, N.; Garcia-Buitrago, M.T.; Voltaggio, L.; Montgomery, E.A. Synovial Sarcoma of the Gastrointestinal Tract. Mod. Pathol. 2024, 37, 100383. [Google Scholar] [CrossRef]
Figure 1.
An example of an inflammatory myofibroblastic tumor: uniform, spindle, and plump cells form randomly oriented fascicles. Stroma is vaguely myxoid, without necrosis.
Figure 1.
An example of an inflammatory myofibroblastic tumor: uniform, spindle, and plump cells form randomly oriented fascicles. Stroma is vaguely myxoid, without necrosis.

Figure 2.
Gross picture of mesenteric fibromatosis, showing a white/pink mass with moderately defined borders.
Figure 2.
Gross picture of mesenteric fibromatosis, showing a white/pink mass with moderately defined borders.

Figure 3.
The lesion has poorly defined boundaries and entraps local adipose tissue.

Figure 4.
Spindle cells without atypia, sometimes with small nucleoli.

Figure 5.
A nuclear beta-catenin immunohistochemistry stain is the hallmark of pathological diagnosis.
Figure 5.
A nuclear beta-catenin immunohistochemistry stain is the hallmark of pathological diagnosis.

Figure 6.
Low-power view of a solitary fibrous tumor with central cystic spaces.

Figure 7.
Higher power shows oval to spindle cells in a background of a mild fibrotic stroma and with hyalinized blood wall vessels.
Figure 7.
Higher power shows oval to spindle cells in a background of a mild fibrotic stroma and with hyalinized blood wall vessels.

Figure 8.
A typical submucosal lipoma in the colon. Note the colonic normal mucosa in the right part of the figure.
Figure 8.
A typical submucosal lipoma in the colon. Note the colonic normal mucosa in the right part of the figure.

Figure 9.
A typical angiolipoma with small blood vessels and thrombi. Some myxoid changes are also apparent.
Figure 9.
A typical angiolipoma with small blood vessels and thrombi. Some myxoid changes are also apparent.

Figure 10.
A typical inflammatory fibroid polyp in the stomach. Notice the lesion centered in the submucosa.
Figure 10.
A typical inflammatory fibroid polyp in the stomach. Notice the lesion centered in the submucosa.

Figure 11.
A high-power view shows spindle cells associated with eosinophils and concentric perivascular fibrosis, imparting an “onion skin” morphology.
Figure 11.
A high-power view shows spindle cells associated with eosinophils and concentric perivascular fibrosis, imparting an “onion skin” morphology.

Figure 12.
A submucosal leiomyoma of the ampulla of Vater.

Figure 13.
Leiomyoma composed of well-differentiated fascicles of bland, fusiform cells with elongated nuclei with eosinophilic cytoplasm.
Figure 13.
Leiomyoma composed of well-differentiated fascicles of bland, fusiform cells with elongated nuclei with eosinophilic cytoplasm.

Figure 14.
Leiomyosarcoma. When compared to the benign counterpart (leiomyoma), there is more cellular density and nuclear atypia.
Figure 14.
Leiomyosarcoma. When compared to the benign counterpart (leiomyoma), there is more cellular density and nuclear atypia.

Figure 15.
A cavernous hemangioma; notice the large and dilated vessels with thin walls.

Figure 16.
Cystic lesion with spaces lined by a layer of endothelial cells located in the duodenum; notice the normal duodenal mucosa in the upper part of the picture.
Figure 16.
Cystic lesion with spaces lined by a layer of endothelial cells located in the duodenum; notice the normal duodenal mucosa in the upper part of the picture.

Figure 17.
Glomus tumor. There is a proliferation of glomus cells in the perivascular compartment.

Figure 18.
The lesion is composed of spindle cells with dilated blood vessels and hyalinized walls.

Figure 19.
The lesion has a diffuse staining for S100.

Figure 20.
In this case, the lesion has a nested appearance. The cells have a large, eosinophilic, and granular cytoplasm.
Figure 20.
In this case, the lesion has a nested appearance. The cells have a large, eosinophilic, and granular cytoplasm.

Figure 21.
Ganglion cells with eosinophilic cytoplasm dispersed among a background of Schwann cells.
Figure 21.
Ganglion cells with eosinophilic cytoplasm dispersed among a background of Schwann cells.

Figure 22.
PEComa. The tumor is composed of cells with eosinophil cytoplasm, with evident lipomatous and vascular elements.
Figure 22.
PEComa. The tumor is composed of cells with eosinophil cytoplasm, with evident lipomatous and vascular elements.

Figure 23.
On higher magnification, some cells are mildly pleomorphic; sometimes with clear cytoplasm.
Figure 23.
On higher magnification, some cells are mildly pleomorphic; sometimes with clear cytoplasm.

Figure 24.
The lesions can have a diffuse staining for muscular markers (α-SMA).

Figure 25.
Lesions usually exhibit heterogeneous staining for melanocytic marker (Melan-A).

Figure 26.
A low-power view showing a dense cellular lesion in a haphazard pattern.

Figure 27.
The lesion is composed of spindle cells, somehow monotonous in a fibrous stroma background.
Figure 27.
The lesion is composed of spindle cells, somehow monotonous in a fibrous stroma background.

Figure 28.
Mitotic activity is evident.

Figure 29.
A break-apart FISH probe exhibits the typical translocation, leading to the correct diagnosis.
Figure 29.
A break-apart FISH probe exhibits the typical translocation, leading to the correct diagnosis.

Figure 30.
Ileum with ulceration and submucosal involvement by a solid and nested tumor.

Figure 31.
The tumor is composed of cells with clear or eosinophilic cytoplasm and rather monotonous nuclei.
Figure 31.
The tumor is composed of cells with clear or eosinophilic cytoplasm and rather monotonous nuclei.


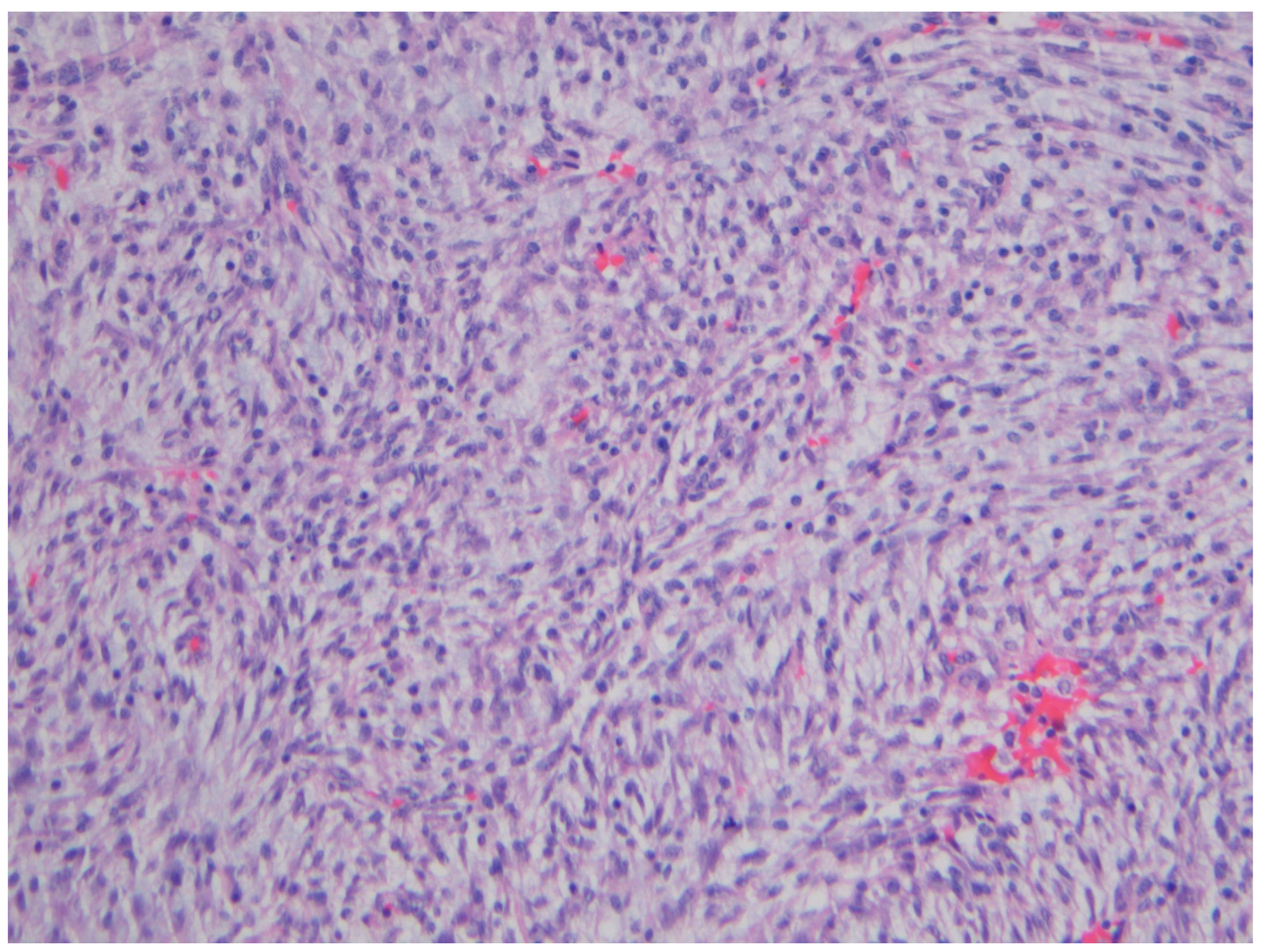{kind=link}
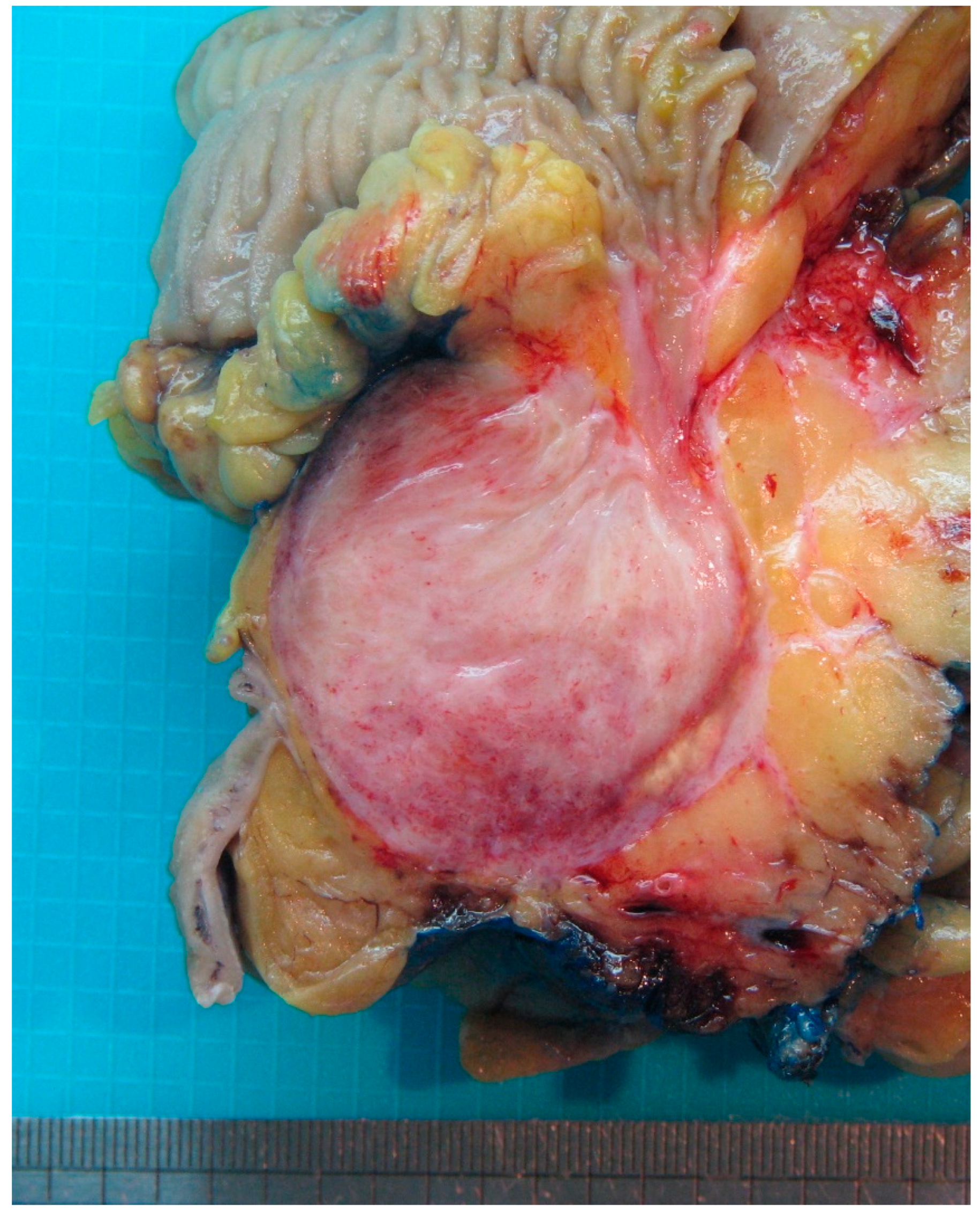{kind=link}
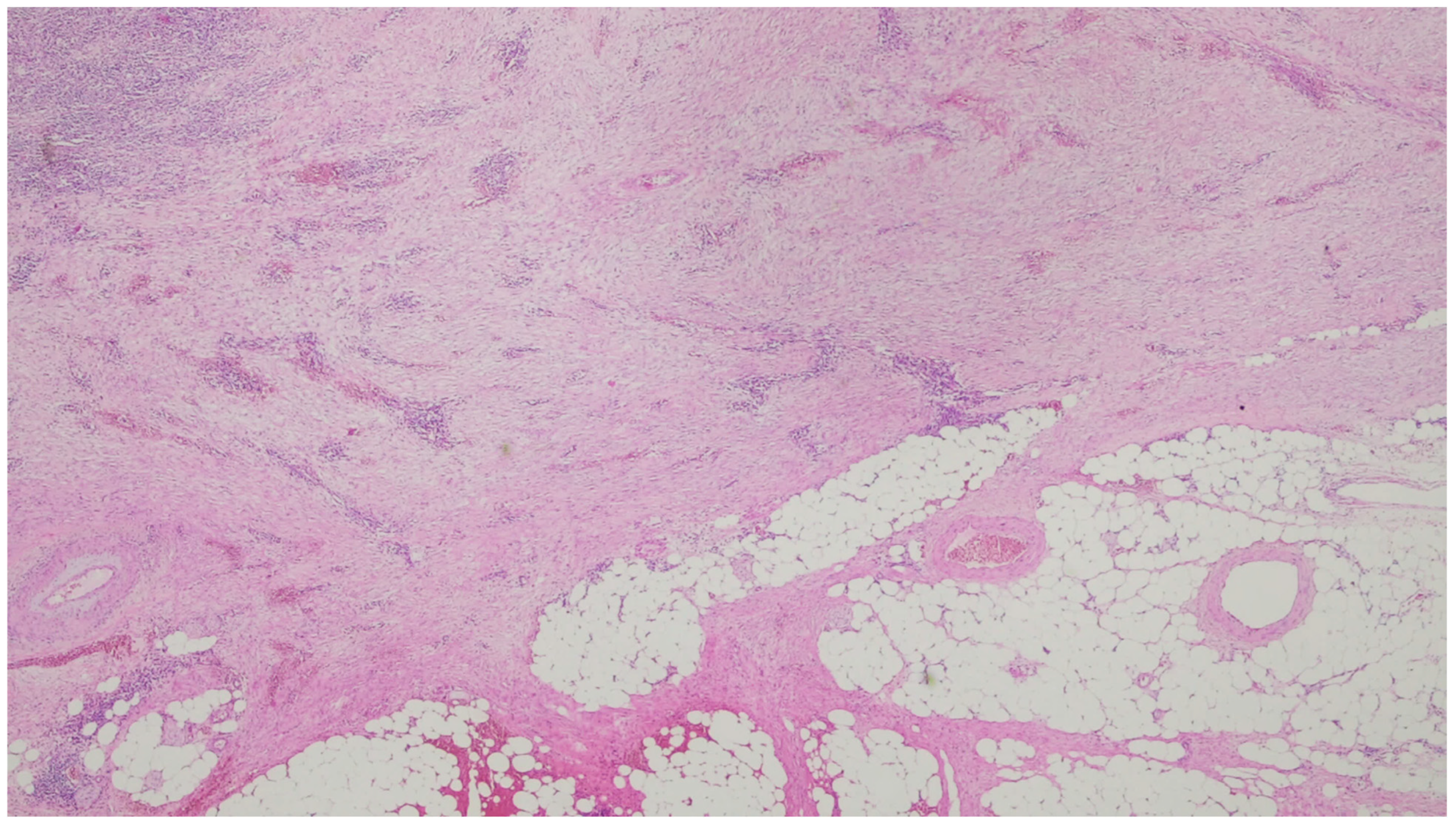{kind=link}
{kind=link}
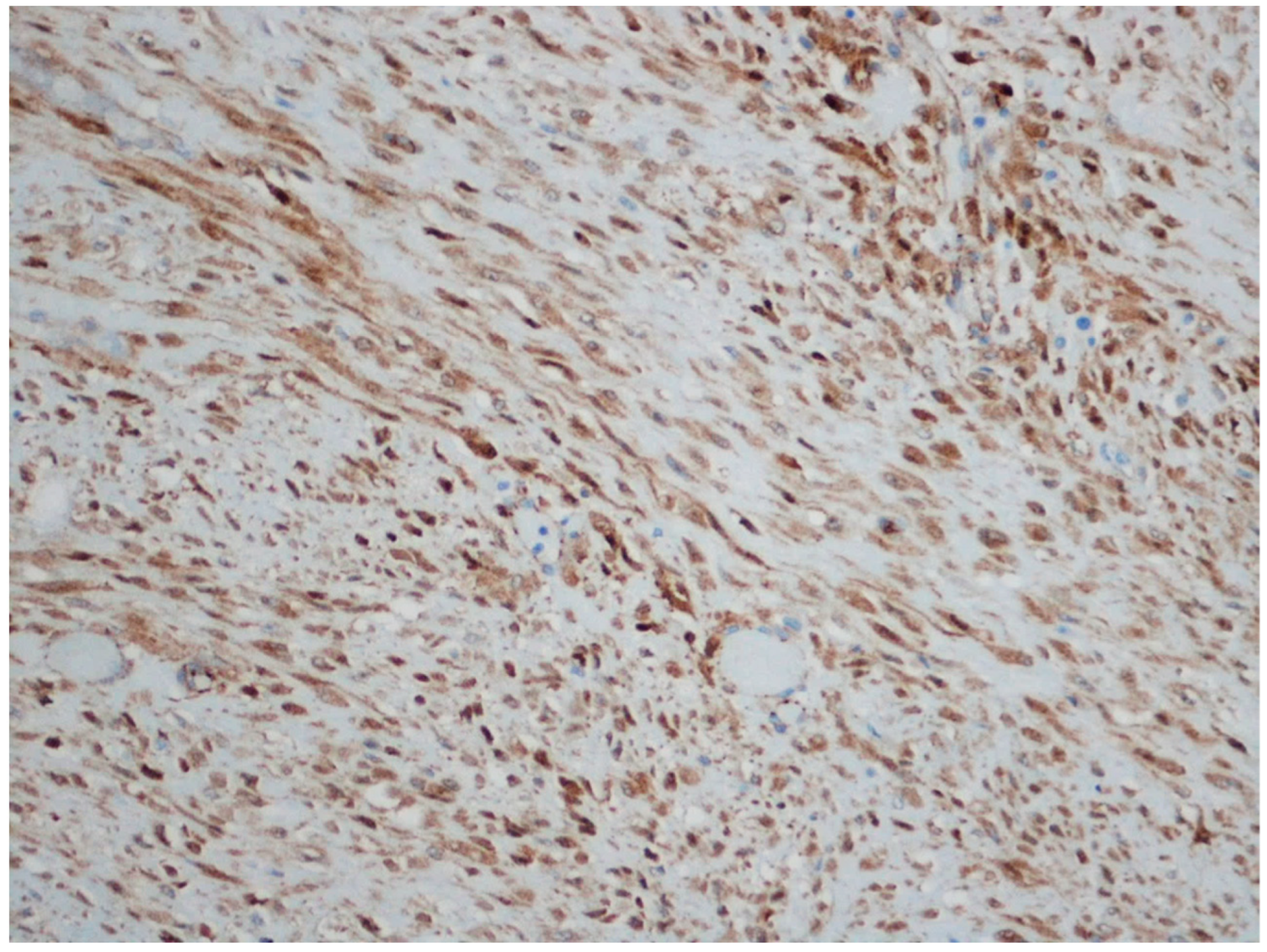{kind=link}
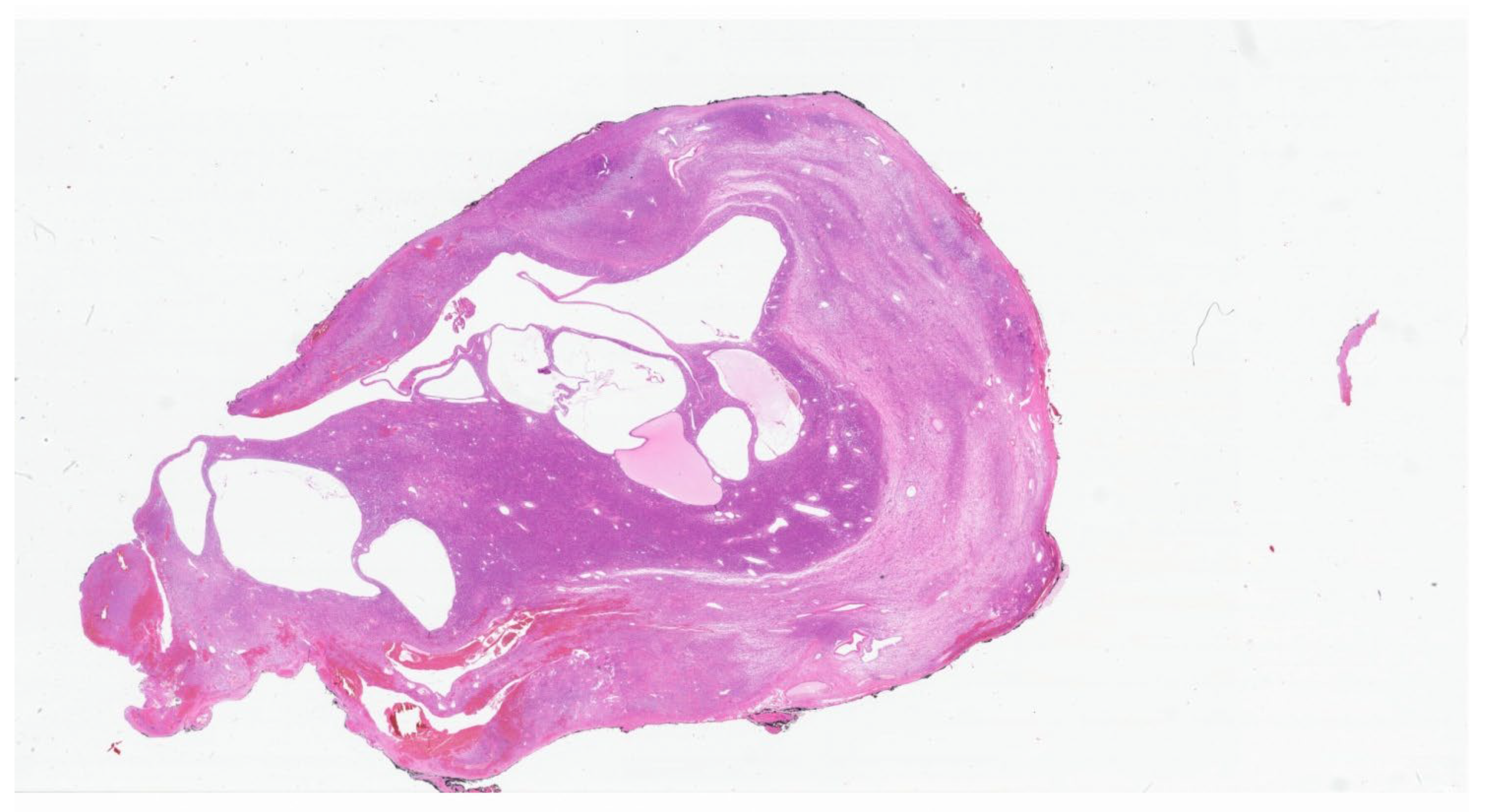{kind=link}
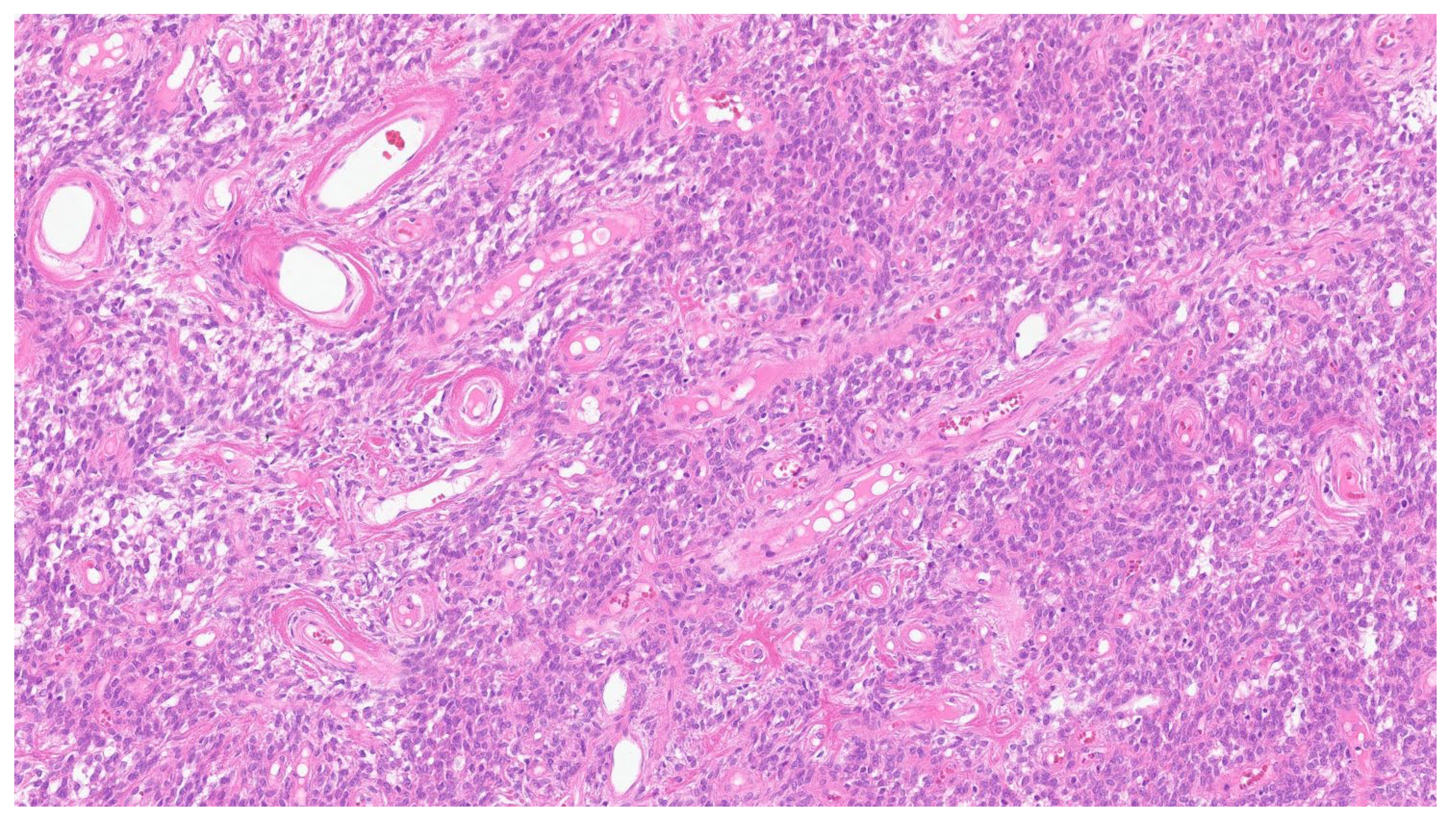{kind=link}
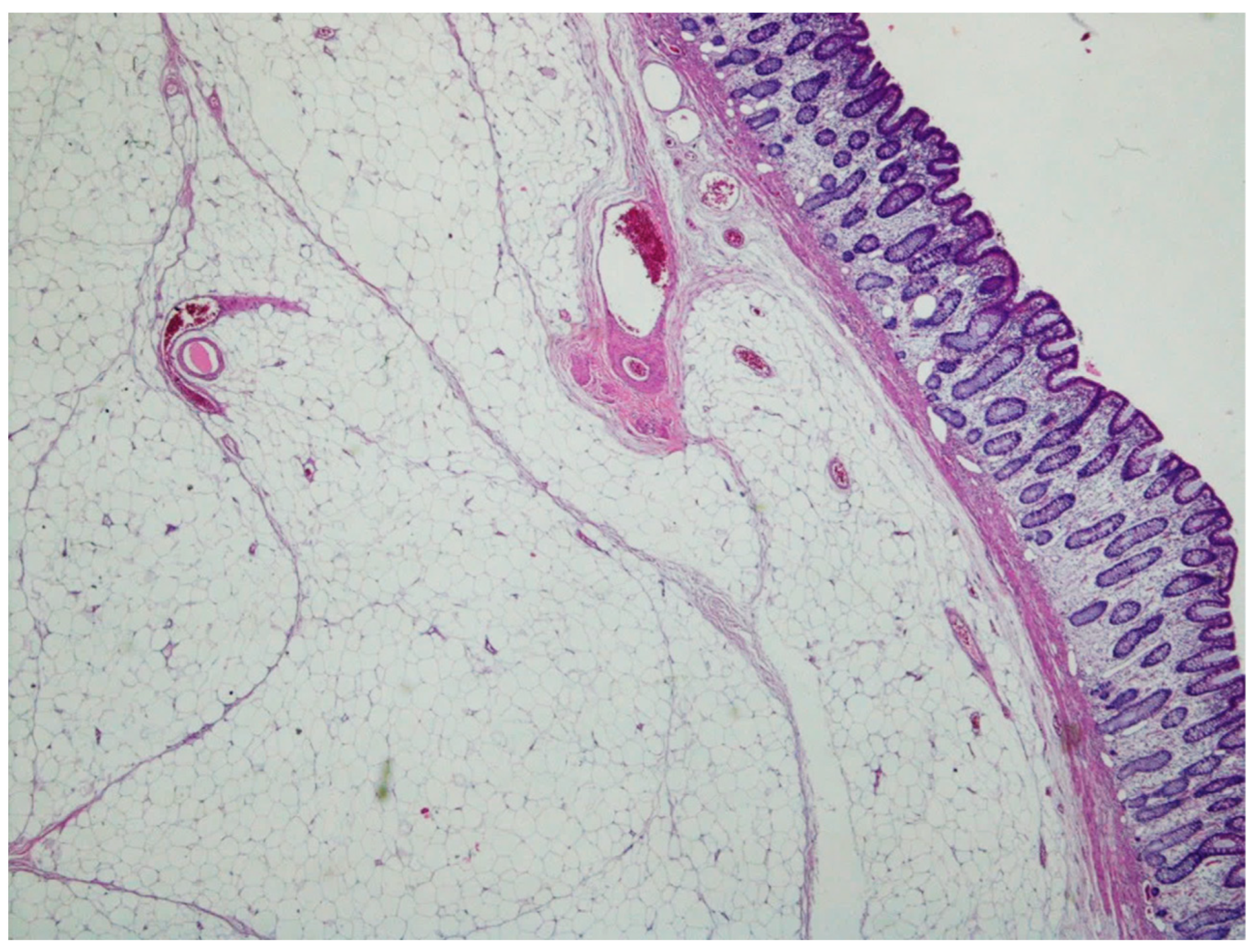{kind=link}
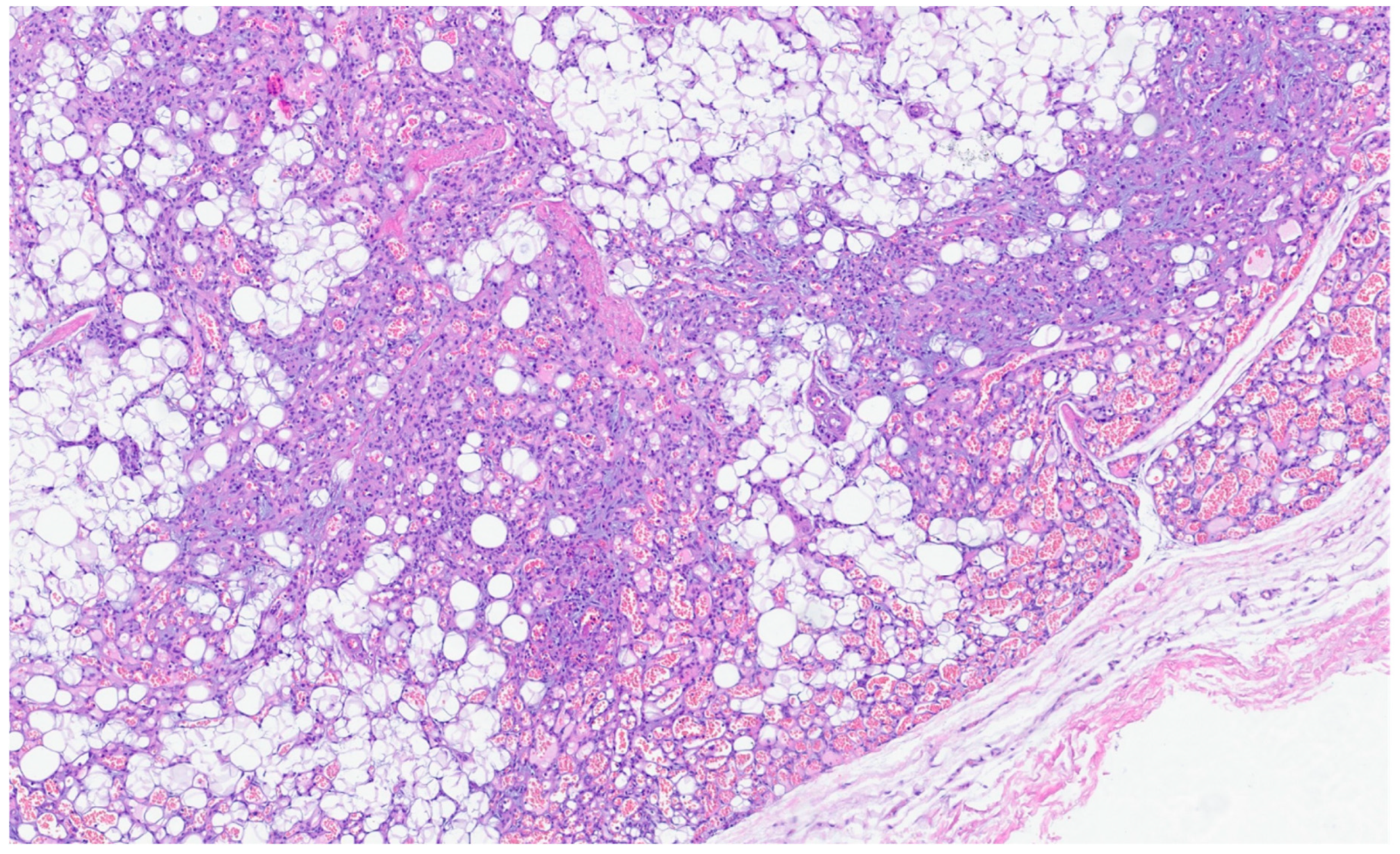{kind=link}
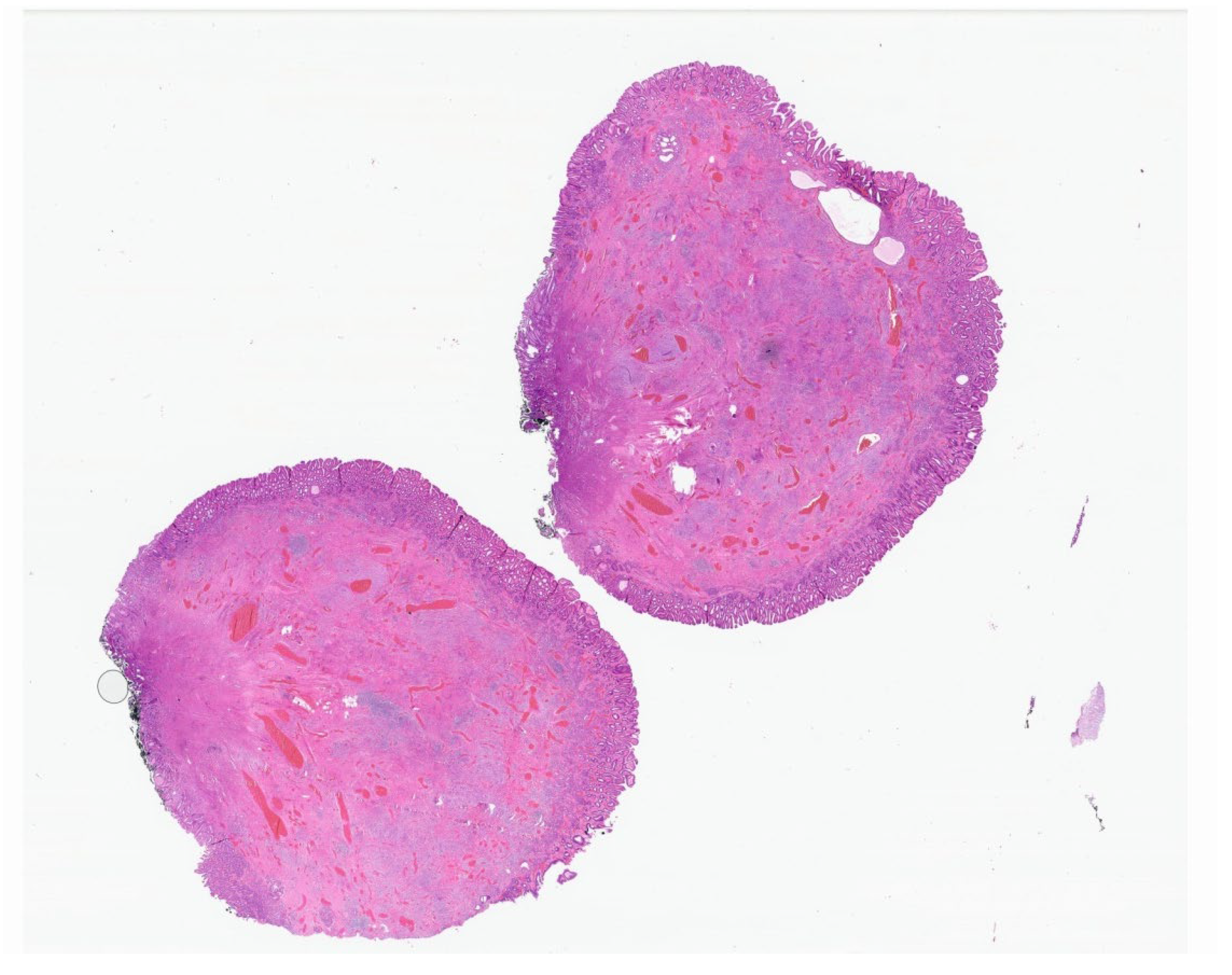{kind=link}
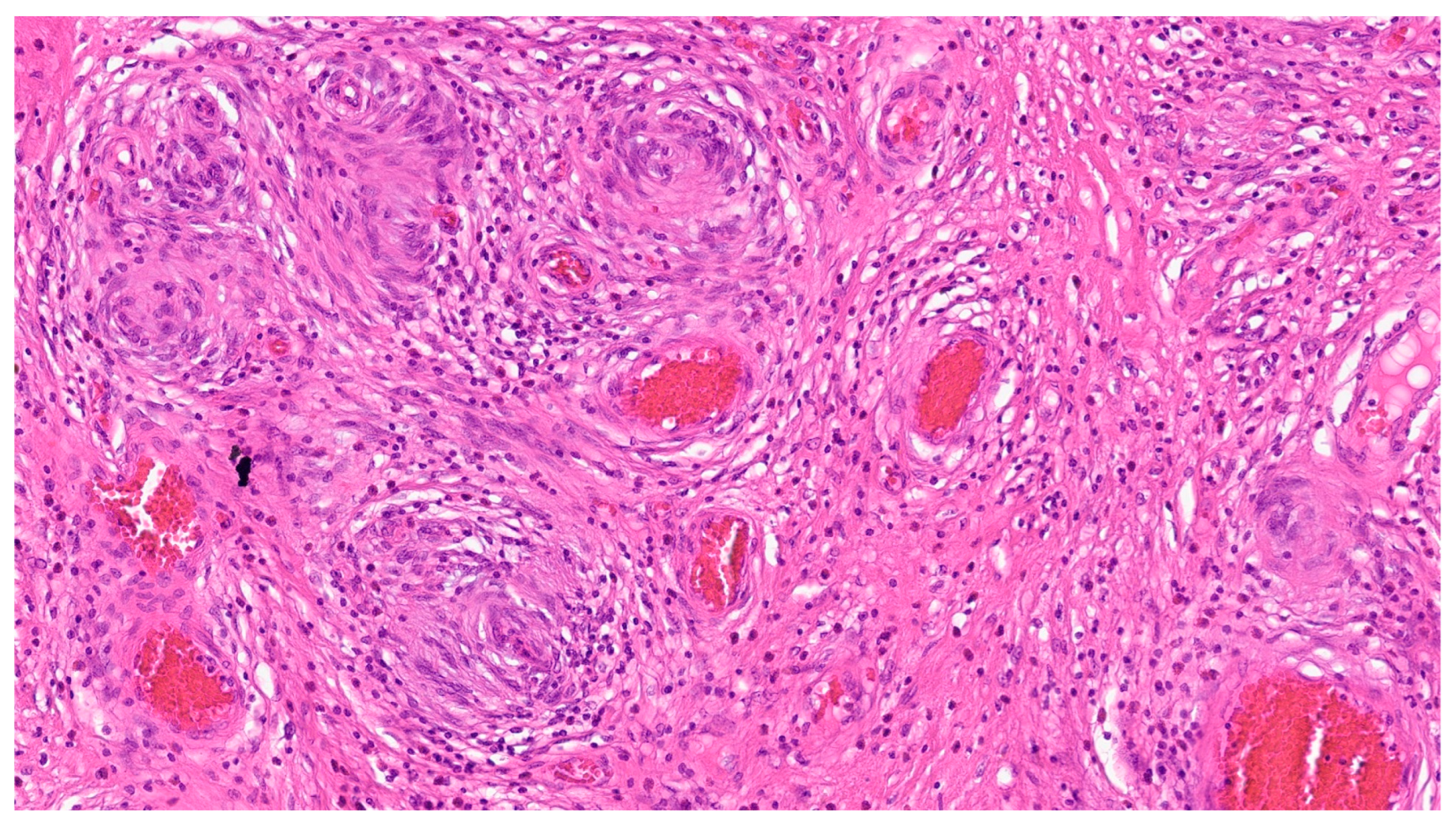{kind=link}
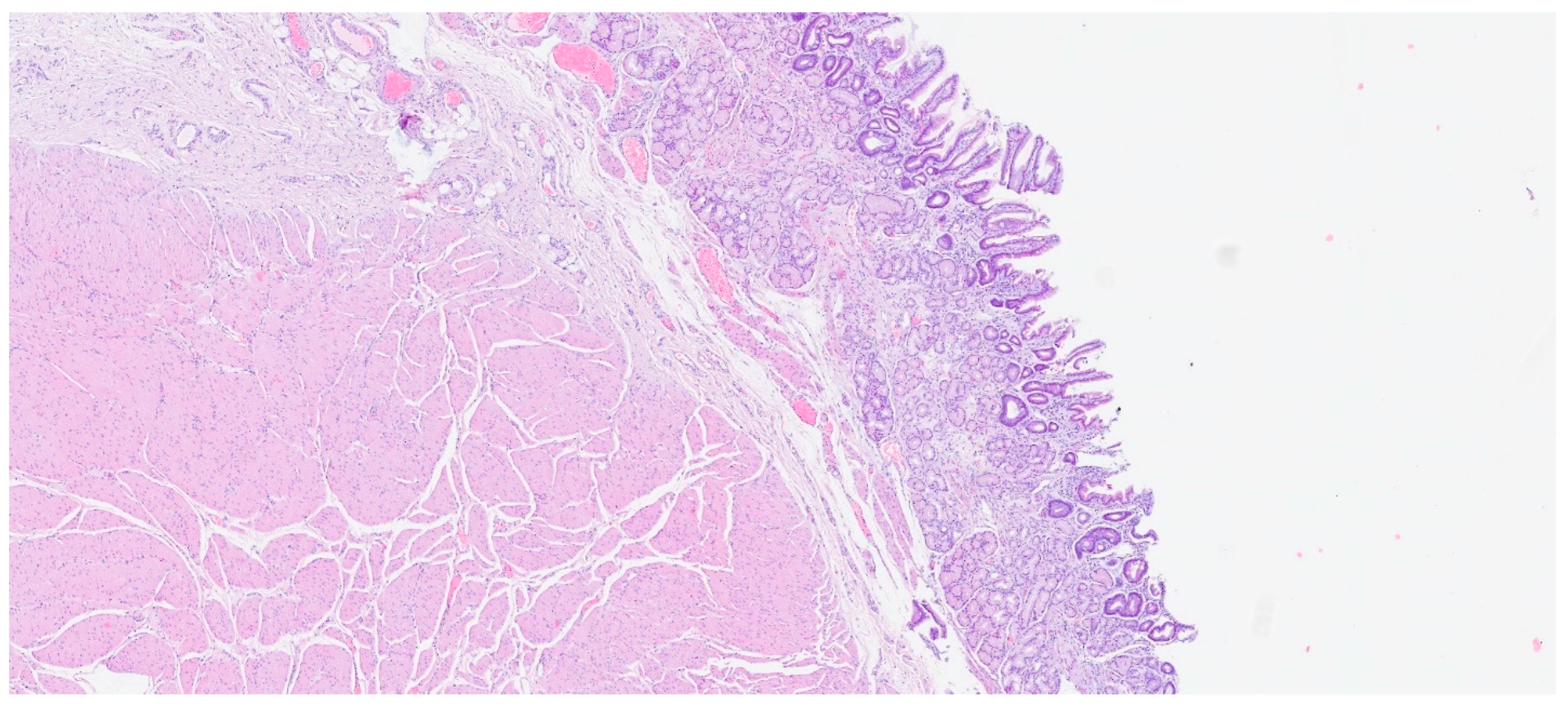{kind=link}
{kind=link}
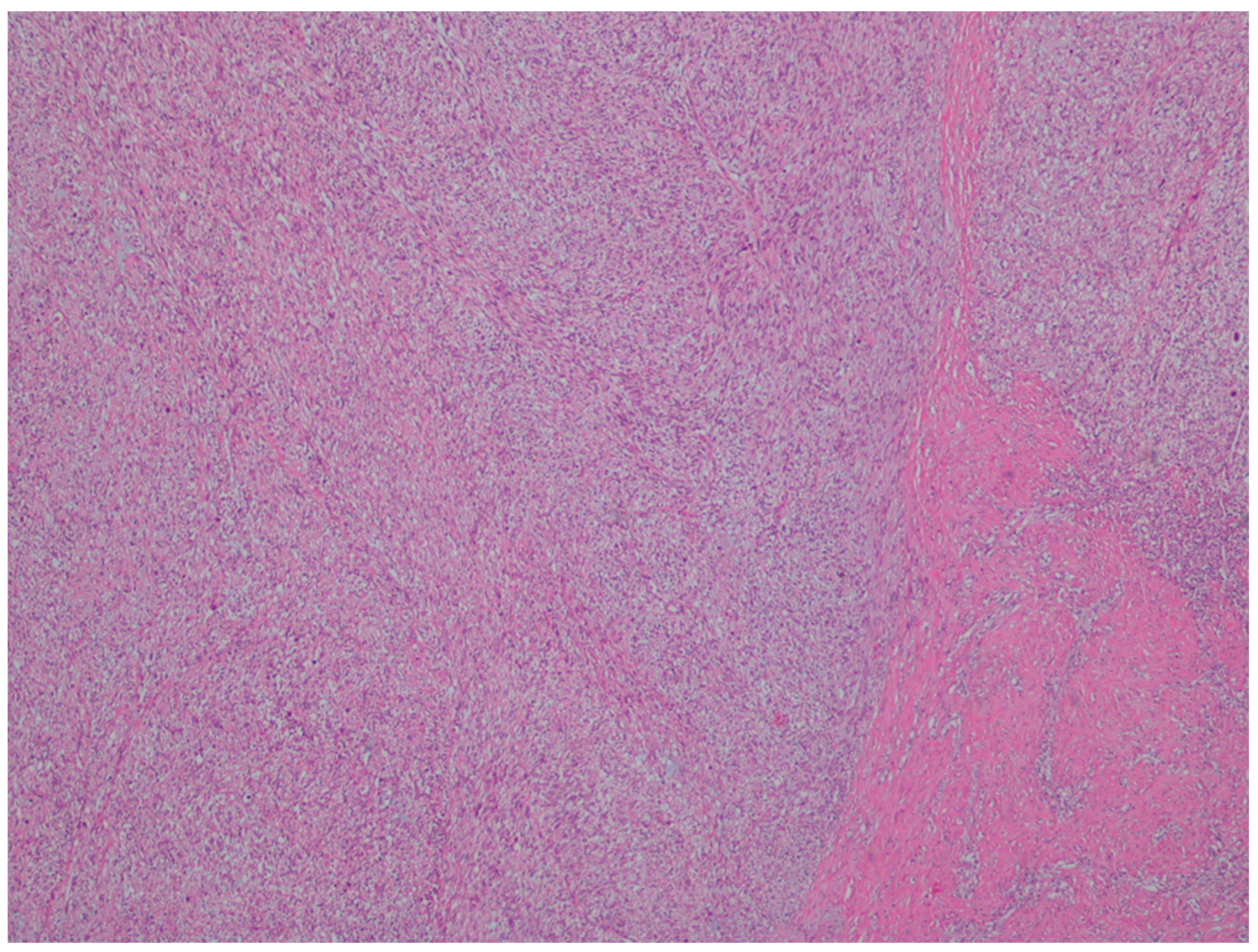{kind=link}
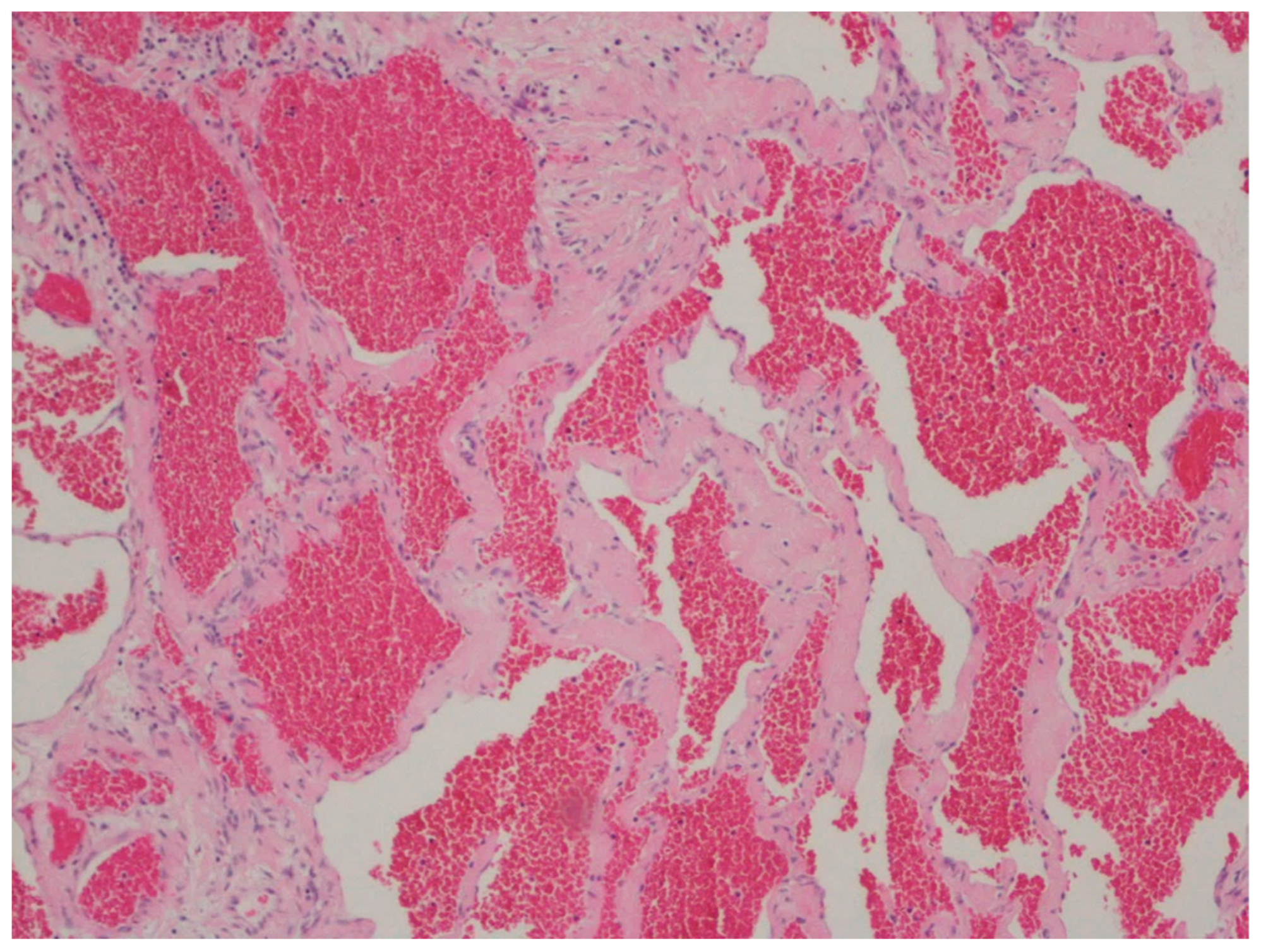{kind=link}
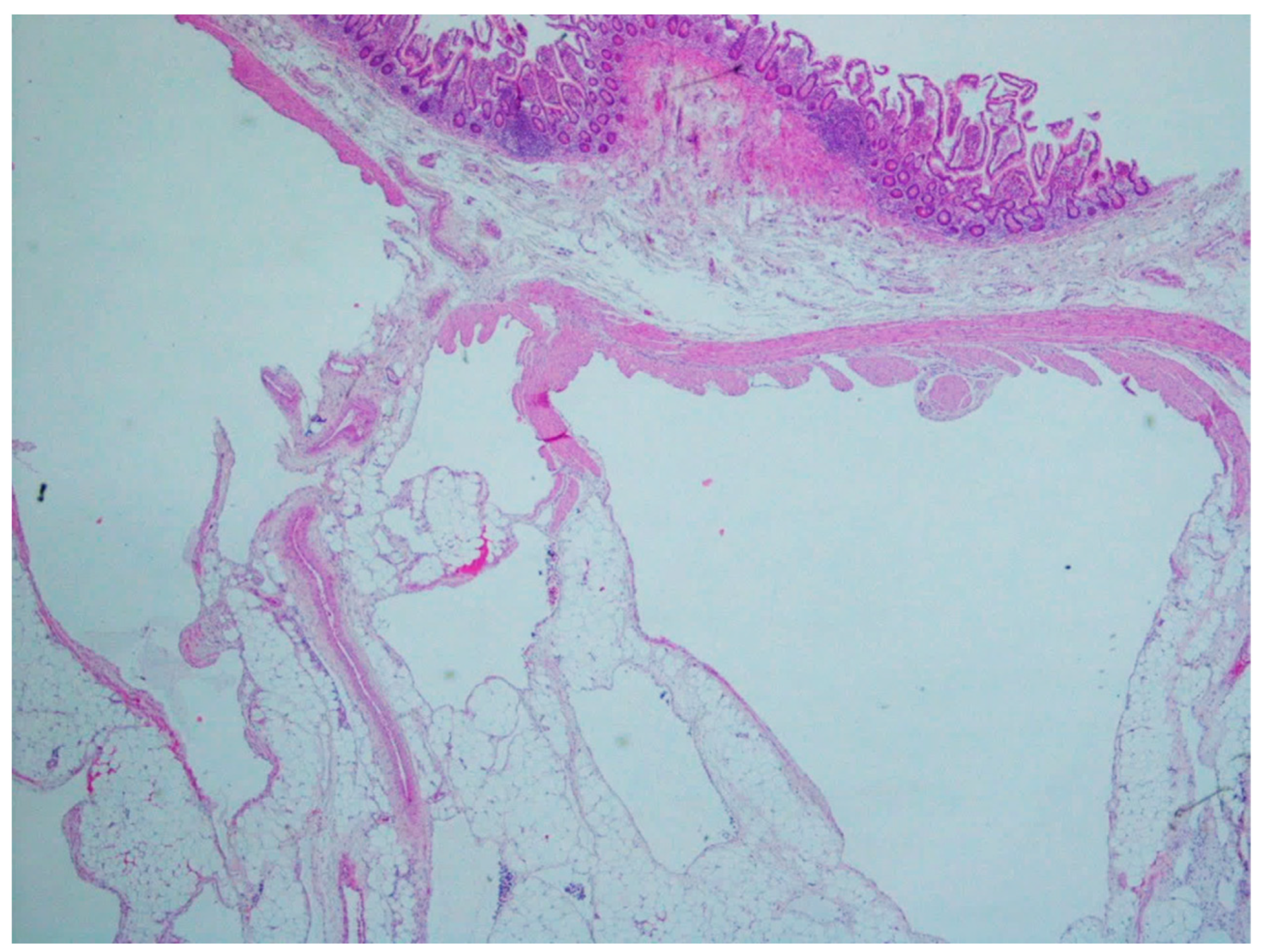{kind=link}
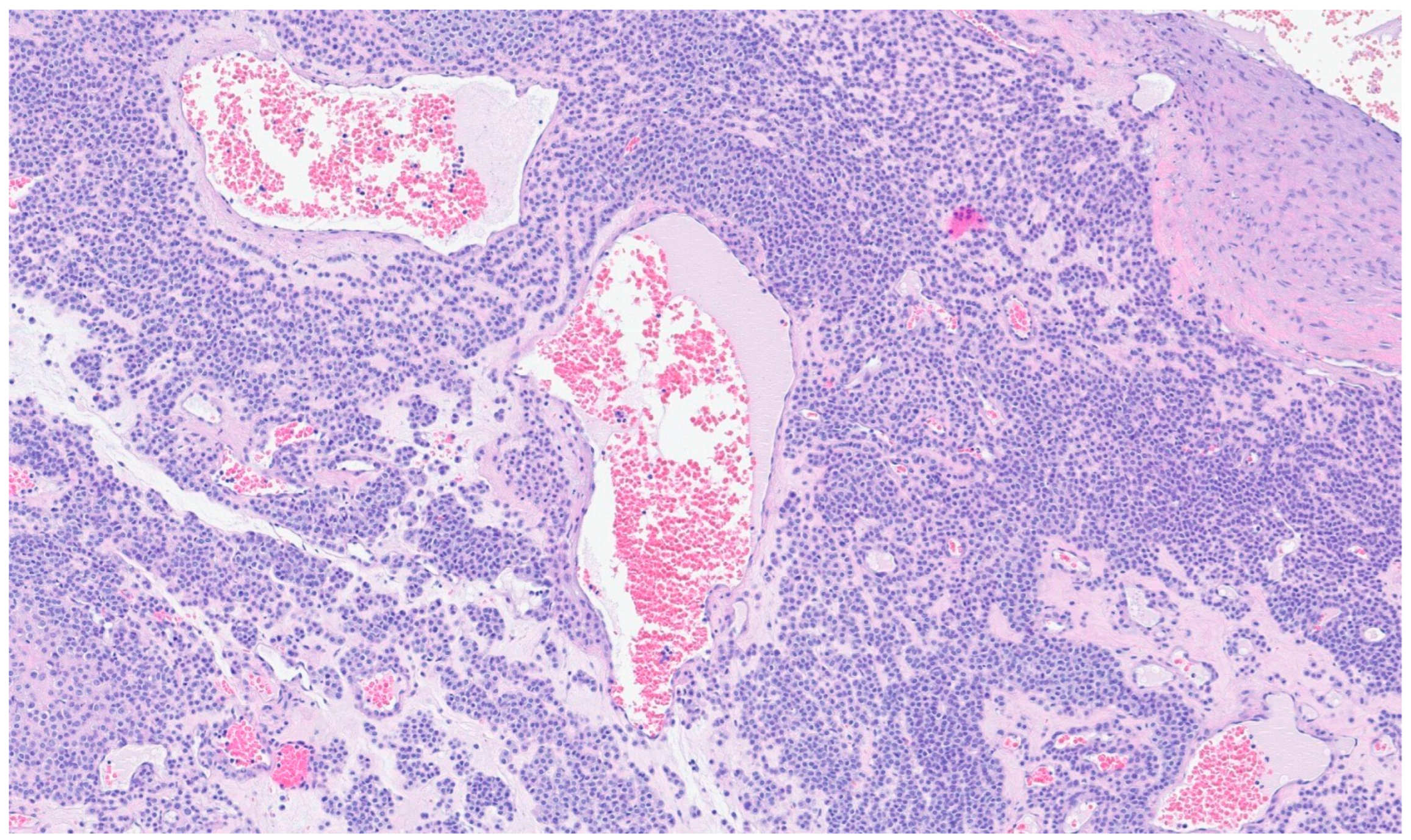{kind=link}
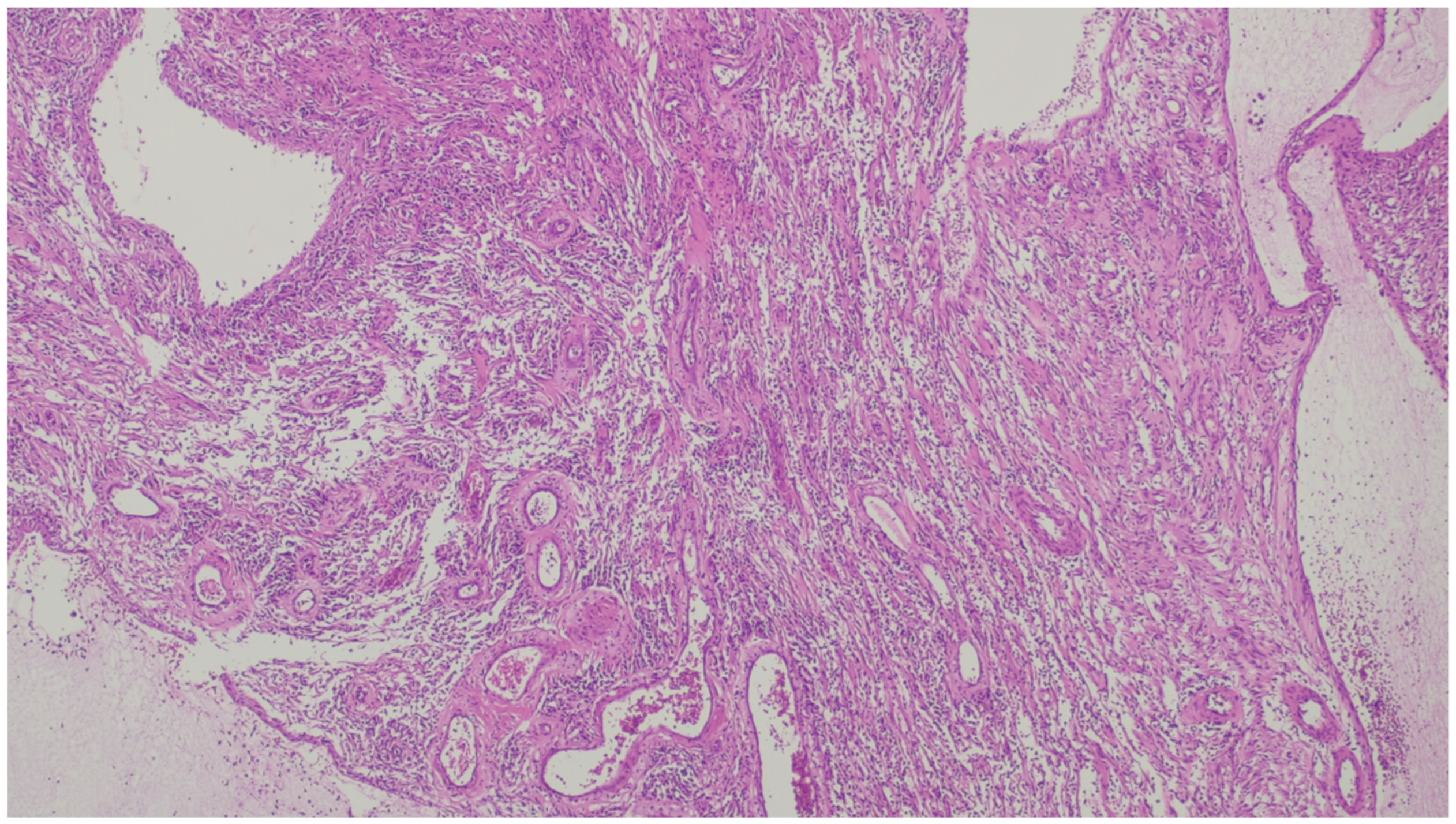{kind=link}
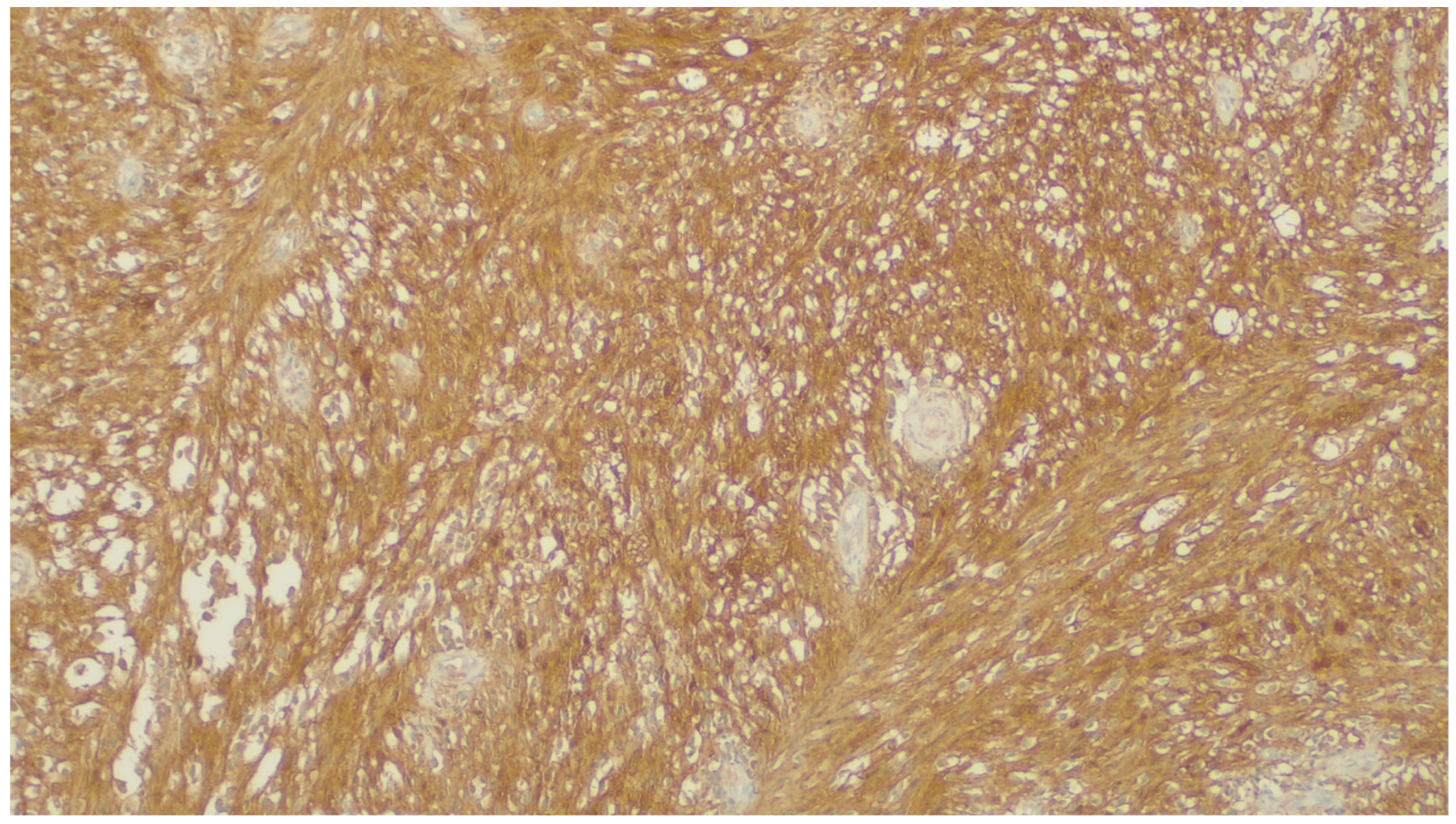{kind=link}
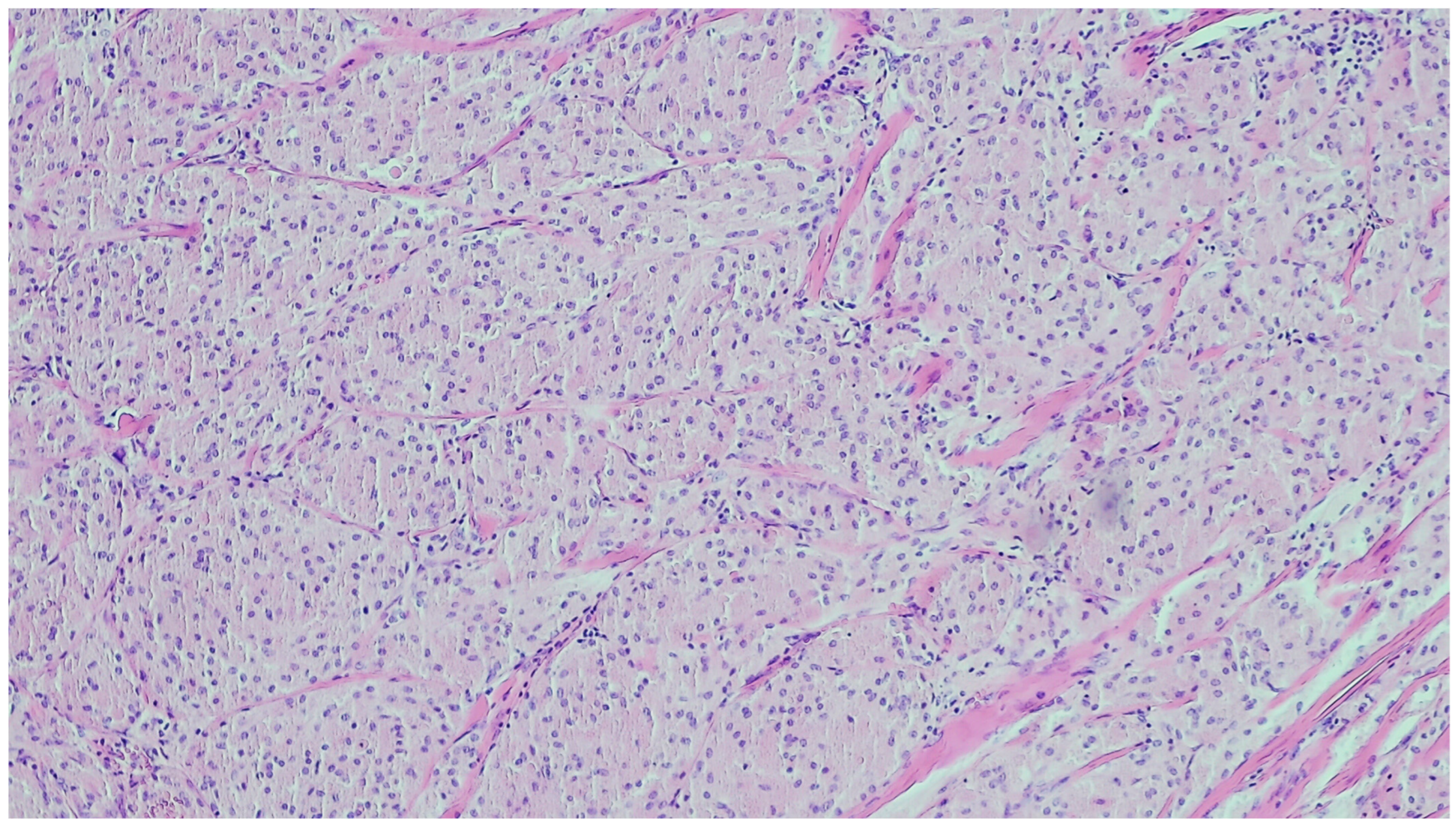{kind=link}
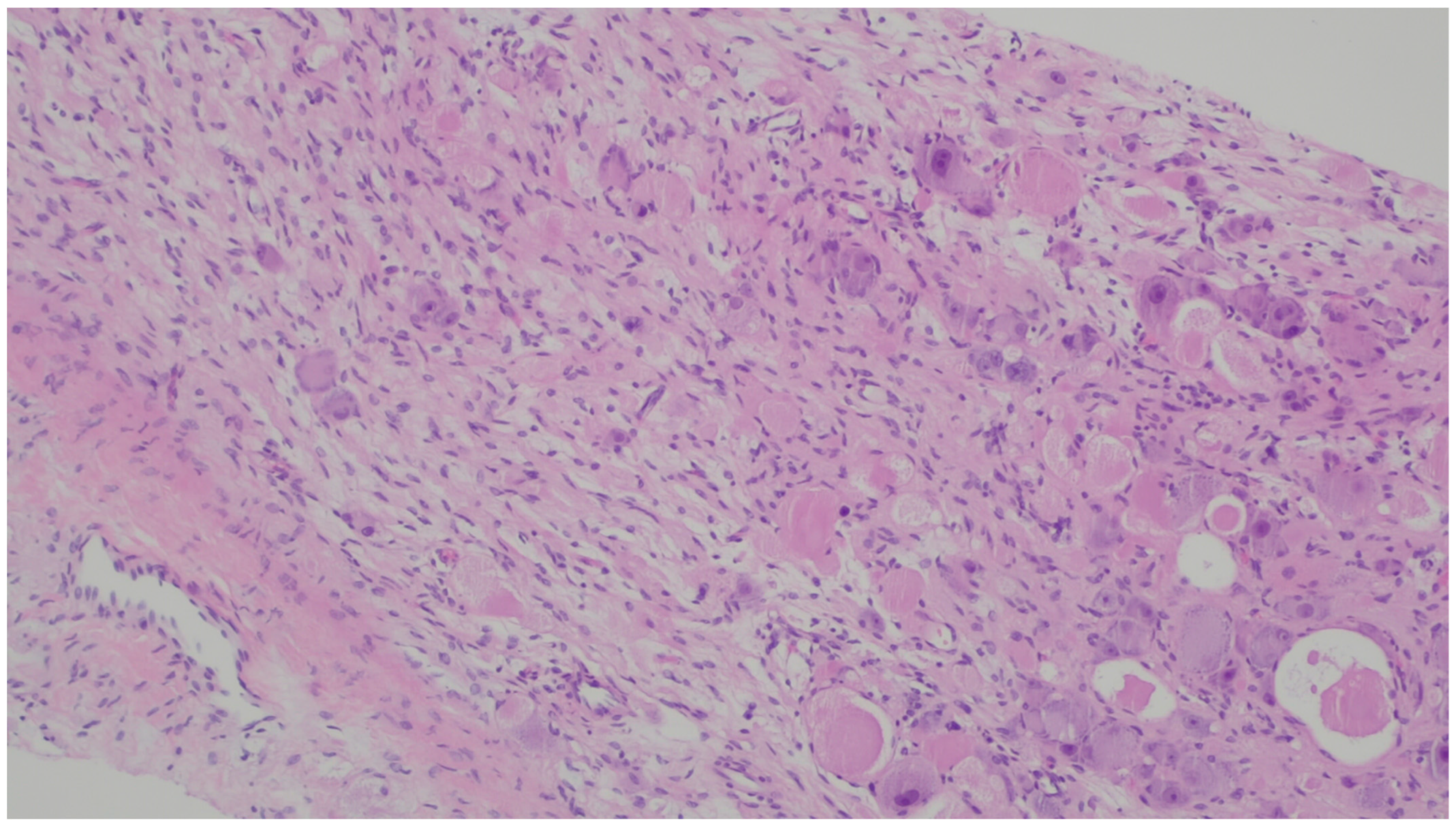{kind=link}
{kind=link}
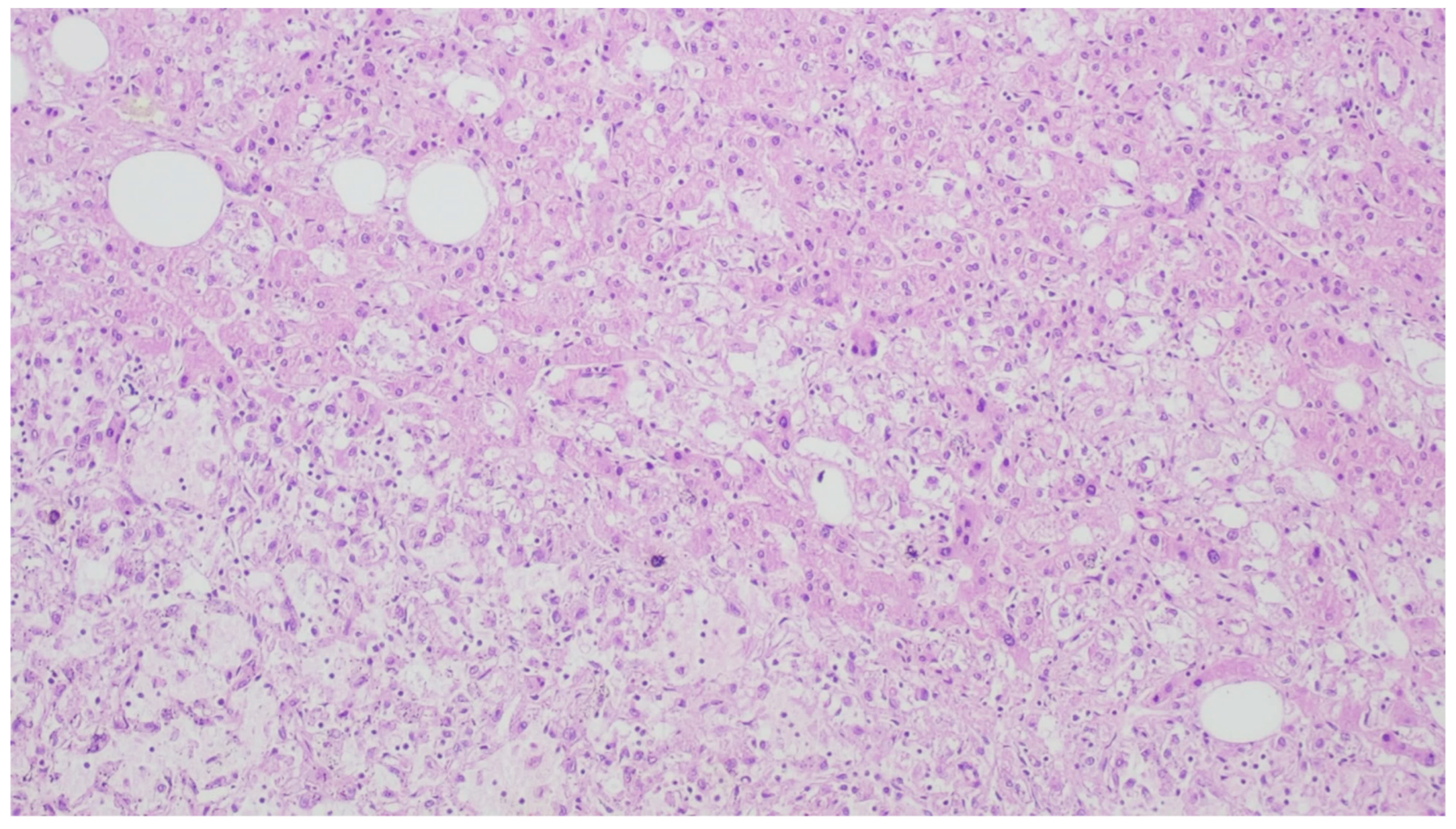{kind=link}
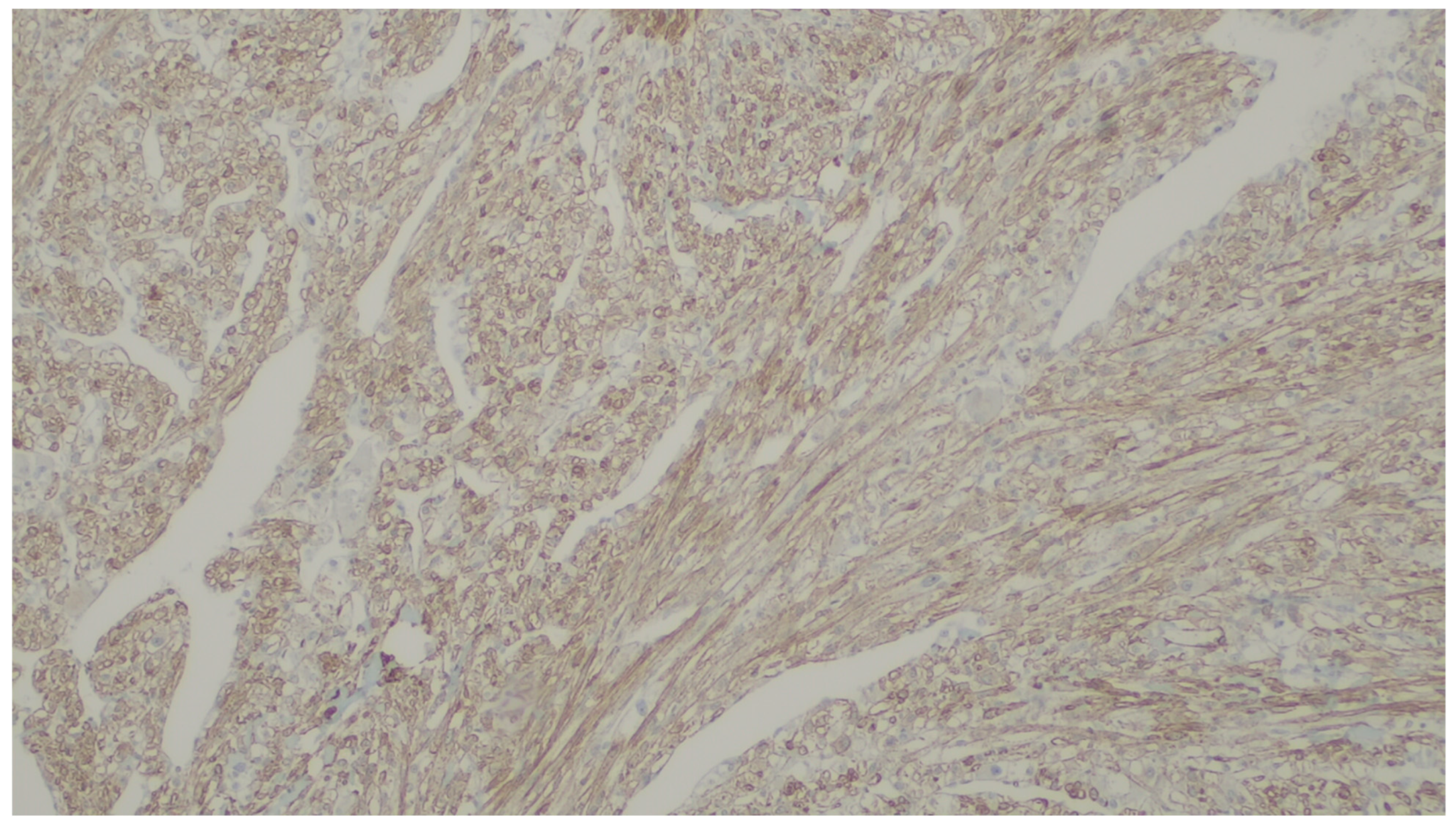{kind=link}
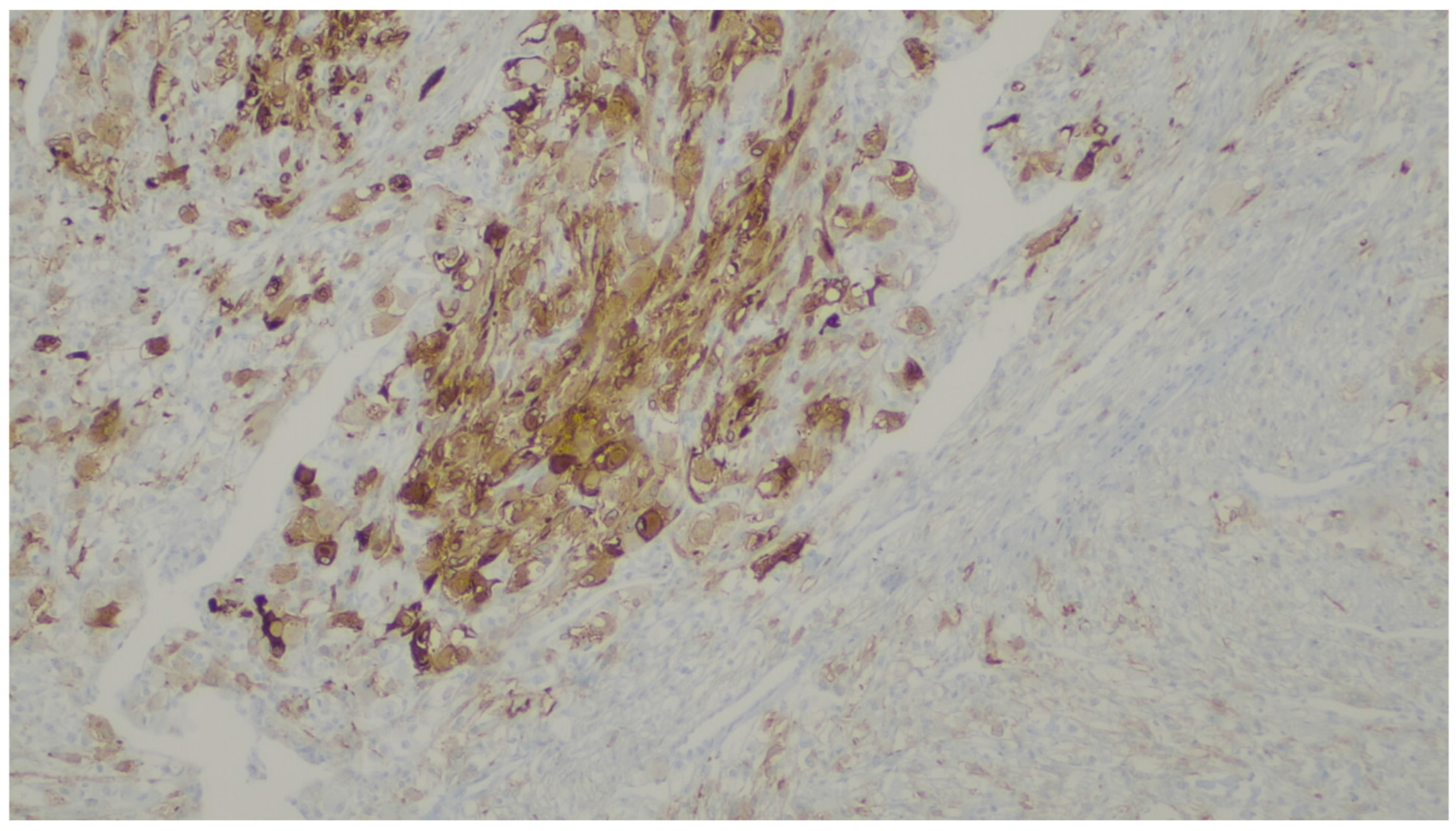{kind=link}
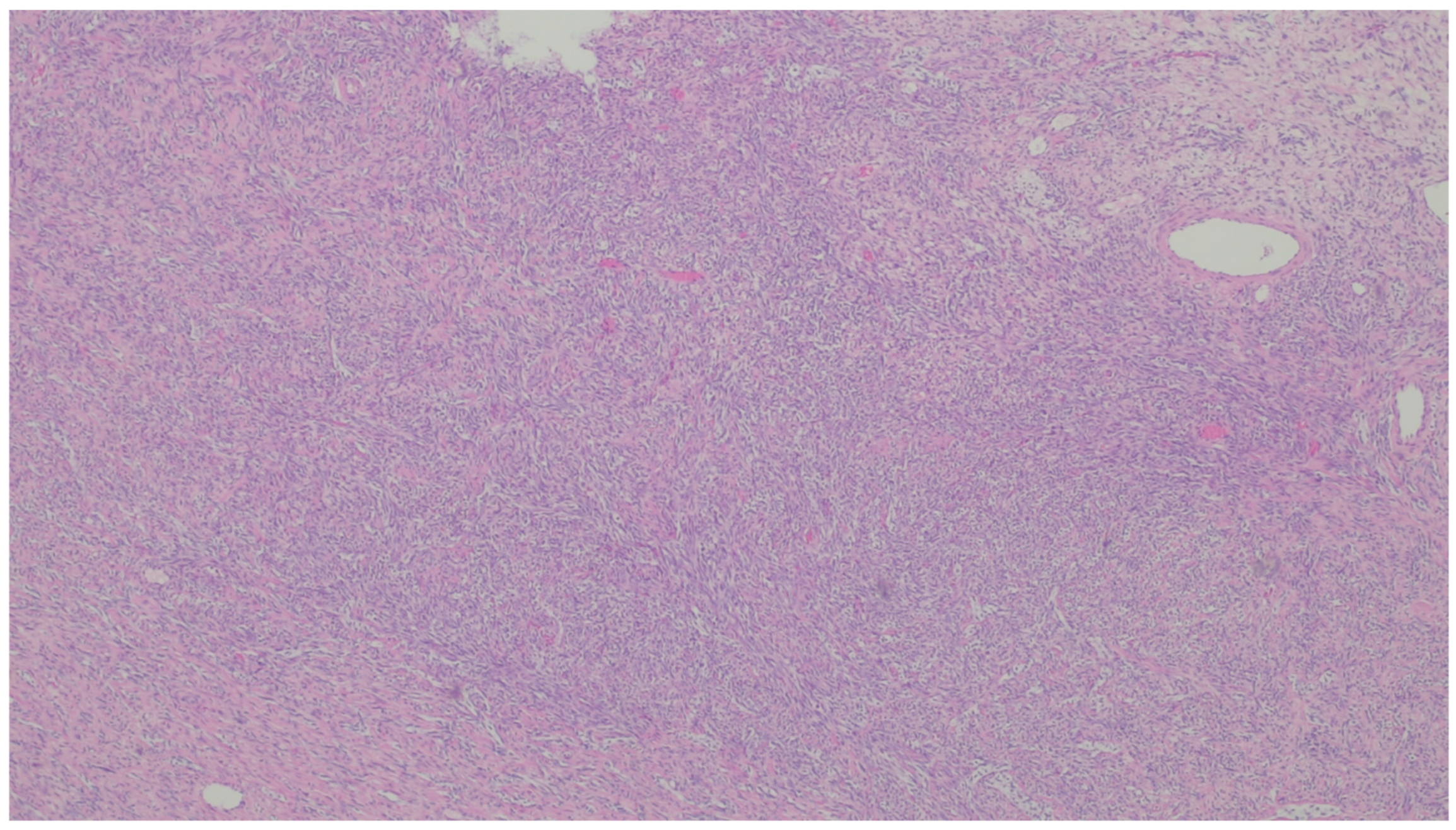{kind=link}
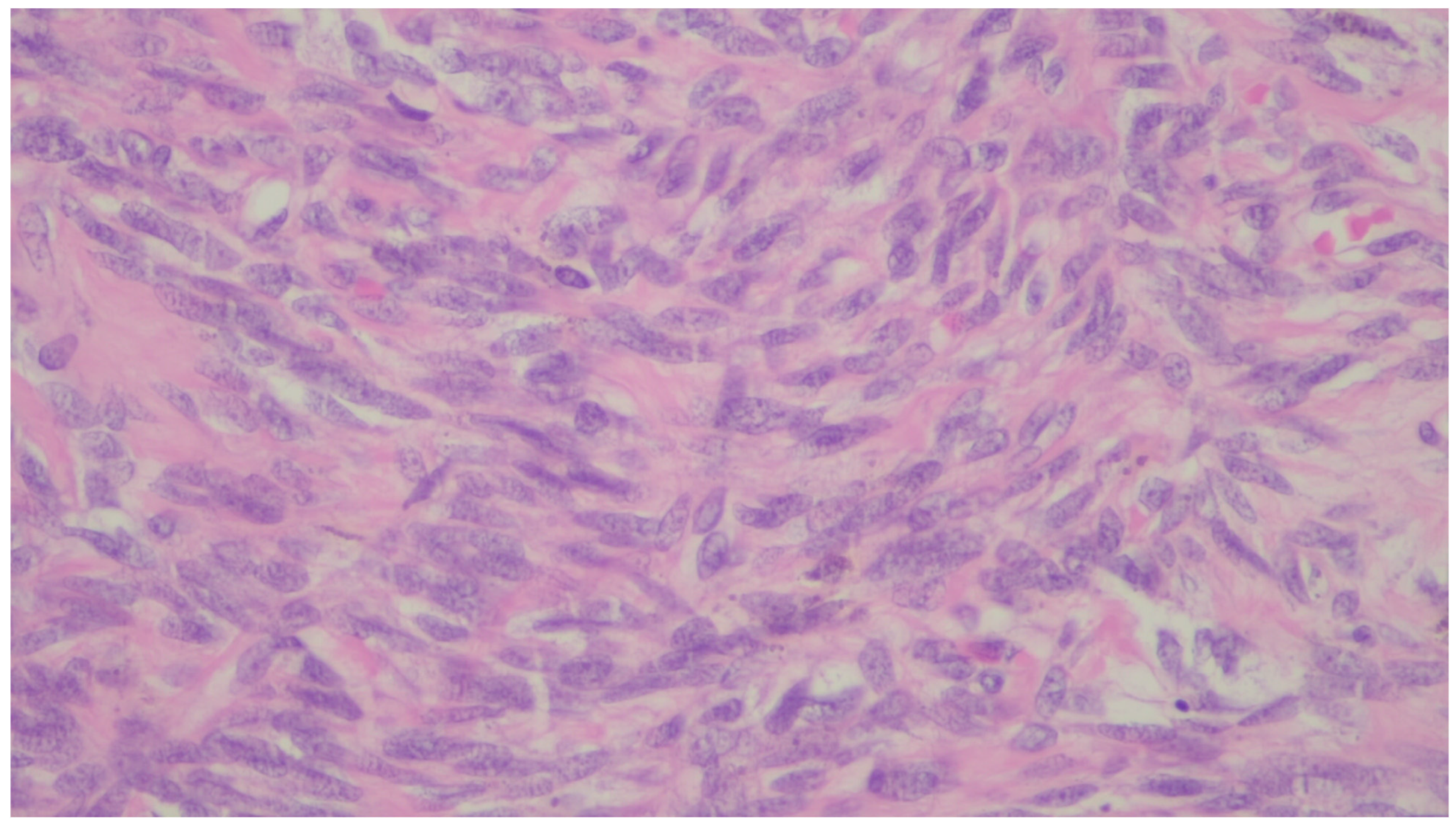{kind=link}
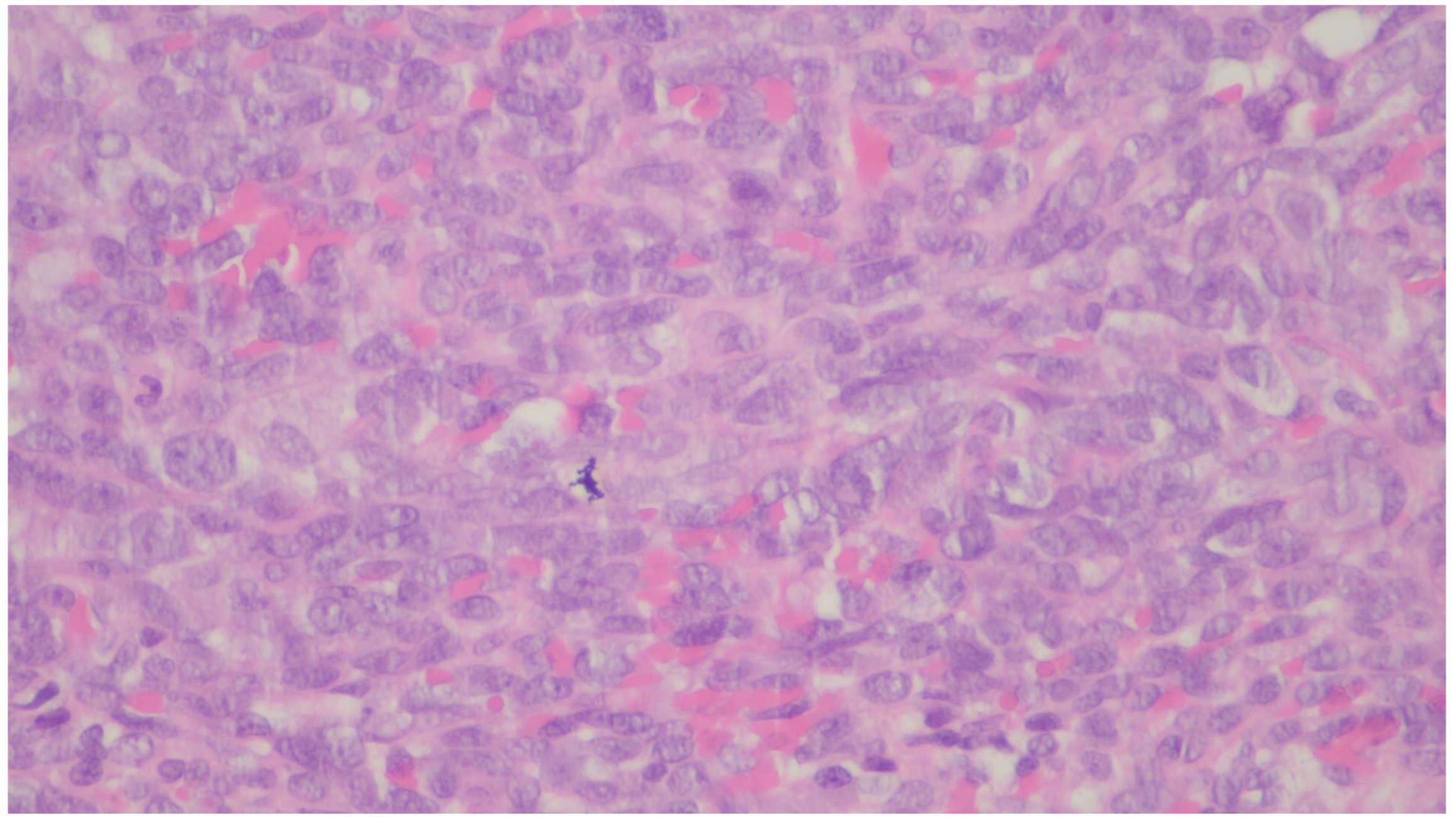{kind=link}
{kind=link}
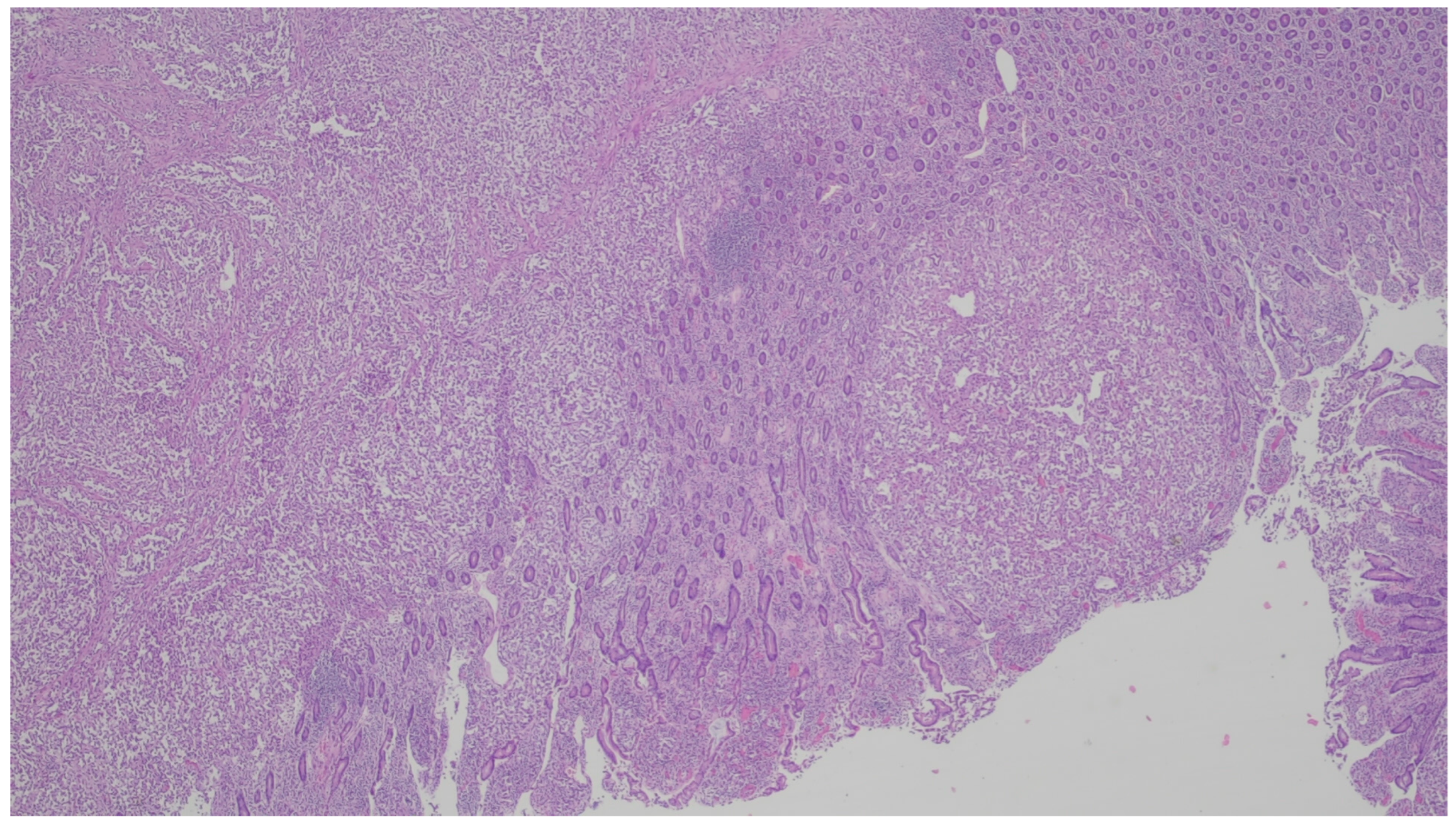{kind=link}
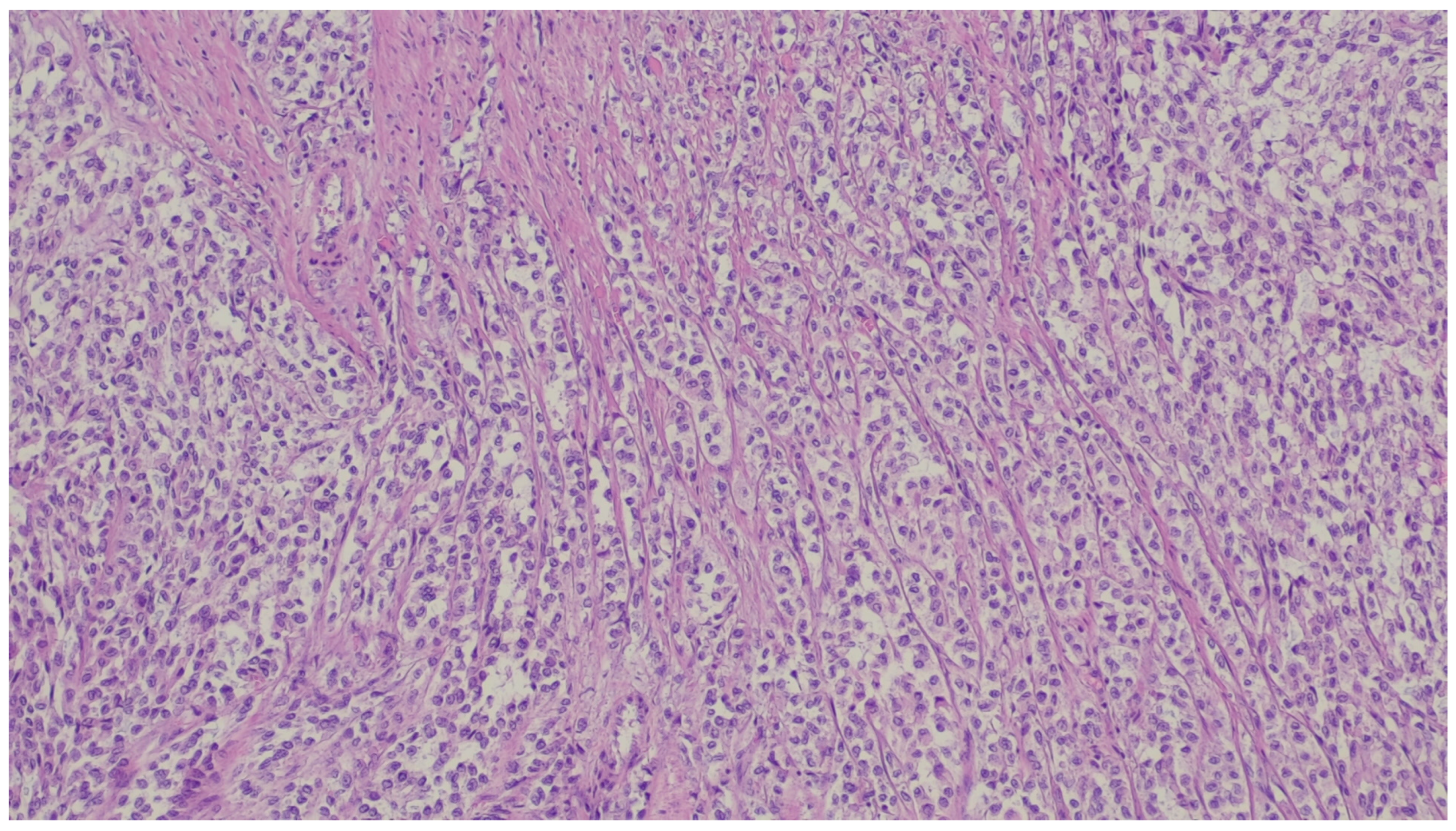{kind=link}
Table 1.
Summary of the lesions, with focus on demographics, site, clinical presentation, histology and relevant immunohistochemistry.
Table 1.
Summary of the lesions, with focus on demographics, site, clinical presentation, histology and relevant immunohistochemistry.
| Entity | Demographics | Site | Clinical Presentation | Histology | Immunohistochemistry |
|---|---|---|---|---|---|
| Inflammatory myofibroblastic tumor | Children and young adults | Colon and small intestine | Variable, from abdominal pain to obstruction | Uniform, plump spindle cells with pale cytoplasm organized into loose fascicles; colagenous or myxoid stroma with inflammation, mainly lymhocytes and plasma cells | α-SMA, ALK positive |
| Fibromatosis | 30 and 40 years | Mesentery of the small bowel | Abdominal pain | Long fascicles of spindle cells with ovoid nuclei without atypia or necrosis | Β-catenin |
| Solitary fibrous tumor | Adults, with a wide range of ages | Anywhere in the GI tract | Symptoms are unspecific, usually associated with compression and, sometimes, hemorrhage | Ovoid/spindle cells arranged in poorly defined fascicles, supported by thin-walled vessels, dilated in a staghorn pattern | STAT6 |
| Lipoma | Adults | Anywhere in the GI tract | Asymptomatic; some cases in the ileocecal valve with obstruction | Mature adipose tissue | S100, Rb1 is retaned, CD34 is negative |
| Inflammatory fibroid polyp | Adults | Stomach | Incidental findings; some cases with abdominal pain, hemorrhage, or obstruction | Proliferation of spindle and stellate cells in haphazard distribution in the submucosa | CD34; PDGFRA |
| Plexiform fibromyxoma | Wide range of age | Antrum and pyloric region | Asymptomatic; some cases with ulceration | Bland spindle cells, supported by a myxoid/fibromyxoid/collagenous stroma and with a rich vascular network of thin-walled vessels in a multinodular pattern | SMA and, occasionally desmin positive. ALK, CD34, keratins, KIT, and DOG1 are negative |
| Leiomyoma | Wide range of age | Esophagus, colon, and rectum | Asympromatic | Well-differentiated fascicles of bland, fusiform cells with elongated nuclei with tapered ends with eosinophilic cytoplasm | α-SMA, desmin, caldesmon |
| Leiomyosarcoma | Very rare in the GI tract | Small intestine | Abdominal pain, obstruction | Of fascicles of spindle cells with atypia, centrally placed cigar-shaped nuclei, and eosinophilic fibrillary cytoplasm with high mitotic counts | α-sma, desmin, caldesmon |
| Hemangioma | Uncommon | Anywhere in the GI tract | Occult or acute GI bleeding | Large and dilated vessels with a thin wall | CD31, CD34 and ERG |
| Lymphangiomas | Children and young adults | Small intestine | Anemia or acute abdomen | Thin-walled, cystically dilated lymphatic spaces lined by endothelial cells with lymph fluid | D2-40, CD31, CD34 |
| Kaposi sarcoma | 25 to 72 years (median 34 years), with a male predominance | Stomach, duodenum, and esophagus | Frequently asymptomatic, when symptomatic, the most common manifestations are diarrhea, abdominal pain, and gi bleeding | Proliferation of blood vessels and spindle cells with minimal atypia organized in vague fascicles, slit-like spaces with extravasated red blood cells with hemosiderin deposition, associated with lymphocytic and plasma cell infiltrate | CD31, CD34, ERG, D2-40, HHV-8 |
| Angiosarcoma | Male predominance and more commonly affect adults with a peak in the seventh decade | Small and large intestine | GI bleeding, abdominal pain, mass or ascites | A wide variation in morphology, from a well-formed network of vessels to sheets of epithelioid and spindle atypical cells without a clear formation of vessels, with necrosis | CD31, CD34, ERG, D2-40 |
| Glomus tumor | Equal predominance, with a paper showing female predominance | Stomach | Upper GI bleeding | Cells with a round and uniform shape and sharply defined borders organized in sheets and nests surrounding vascular spaces | SMA, calponin, TLE1, caldesmon. Variable desmin. S100 and c-kit are absent. |
| Schwannoma | Marked female predominance | Stomach | Mass-like symptoms | Spindle cells distributed in hypo and hypercellular areas; older lesions may show cystic changes, hemorrhage, and hyaline thick- walled blood vessels | S100, SOX-10 |
| Granular cell tumor | Sixth decade of life | Esophagus | Asymptomatic | Monotonous and epithelioid cells with abundant eosinophilic and granular cytoplasm | S100 and calretinin |
| Perineurioma | Female predominance and appear in middle-aged adults | Rectosigmoid colon | Asymptomatic, GI bleeding | Show expansion of the lamina propria by uniform and bland spindle cells, entrapping colonic cripts | EMA, claudin-1, and GLUT1 |
| Ganglioneuroma | Wide age range | Large intestine, with a predilection for the left side and rectum | They present in colorectal cancer screening as small polypoid lesions (inferior to 2 cm) and can be solitary, multiple, or diffuse; however symptms are not specific | Expansion of the lamina propria by ganglion and schwan cells, accompanied by eosinophils, sometimes with cystic colonic glands | S100, SOX10 |
| PEComa | Rare | Colon and small intestine | Symptoms are not specific | Nested, trabecular, and alveolar architecture, surrounded by a delicate vasculature; the cells are usually epithelioid with round to oval nuclei with a granular eosinophilic cytoplasm, but a minority of spindle cells can be seen | α-SMA, desmin, HMB-45 Melan-A, MiTF |
| NUTM1-rearranged colorectal sarcoma | Teens and young adults; more common in females | Colorectal | Symptoms are not specific | Three distinctive patterns: intersecting fascicles with uniform cells pattern, a hyalinized/nested pattern, and an epithelioid and rhabdoid pattern | nuclear expression of NUT, variable keratin expression and expression of CD117 and DOG1, retained expression of SMARCB1 and SMARCA4 |
| Mesenchymal tumors associated with NTRK rearrangements | - | - | Symptoms are not specific | Spindle cells tumors | CD34, S100, NTRK |
| Synovial sarcoma | Middle-aged to older adults | Stomach | Polypoid or an ulcerated lesion | Monophasic with uniform spindle cells with scarce matrix or biphasic with glandular elements | SS18/SSX positivity. Focal positivity for keratins and EMA in monophasic lesions and strong staining in the biphasic version |
| Gastrointestinal clear cell sarcoma/malignant gastrointestinal neuroectodermal tumor | Young adults | More common in the small intestine, stomach, and colon | Polypoid or mural in appearance, with ulceration resembling carcinomas | Nested or pseudopapillary pattern and sometimes a spindle phenotype | S100, SOX-10, Melan-A, HMB45, MiTF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gama, J.M.; Oliveira, R.C. Mesenchymal Tumors of the Gastrointestinal Tract—Beyond GIST—A Review. Gastrointest. Disord. 2024, 6, 257-291. https://doi.org/10.3390/gidisord6010019
AMA Style
Gama JM, Oliveira RC. Mesenchymal Tumors of the Gastrointestinal Tract—Beyond GIST—A Review. Gastrointestinal Disorders. 2024; 6(1):257-291. https://doi.org/10.3390/gidisord6010019
Chicago/Turabian StyleGama, João Martins, and Rui Caetano Oliveira. 2024. "Mesenchymal Tumors of the Gastrointestinal Tract—Beyond GIST—A Review" Gastrointestinal Disorders 6, no. 1: 257-291. https://doi.org/10.3390/gidisord6010019