
AI-Based Predictive Modelling of the Onset and Progression of Dementia

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Background
2.1. Ageing, Cognitive Decline, and Dementia
2.1.1. Physical Activity
2.1.2. Cardiovascular Risk Factors—Diabetes, Hypertension, Hypercholesterolaemia, and Obesity
2.1.3. Social Interaction
2.1.4. Nutrition
2.1.5. Cognitive Stimulating Activity
2.1.6. Sleep, Meditation and Relaxation
2.2. Predicting Dementia and Cognitive Decline
2.3. Sharing of Health Data
3. The LETHE Project Approach
- Using existing data from multinational, European clinical observational cohorts, and population-based observational and intervention studies (including the FINGER RCT, with data from an up to 11-year follow-up, assessing the long-term effects of a 2-year multidomain intervention) to develop initial prediction models for the progression of dementia and related risk factors;
- Using results from former ICT-based EU projects to implement a mainly automated ICT-based FINGER intervention model supported by validated sensing and interaction technology;
- Extending and validating the personalised prediction models using digital biomarkers collected in an 18-month validation trial in subjects at-risk of dementia, which will include two arms: ICT-assisted structured multimodal intervention and self-guided intervention group;
- Implementing a big data framework which allows a multicentre model optimisation and roll out;
- Providing knowledge for individuals and care professionals about dementia risk factors and risk of disease onset and progression, integrating information on lifestyle parameters, individual health data, and AD-related biomarkers, such as MRI (structural brain change) and blood-based biomarkers (APOE genotype, plasma markers related to AD: amyloid-42, amyloid-40, phosphorylated (p)-Tau181, p-Tau231, neurofilament light chain), thereby assessing their individual potential to benefit from multidomain preventive interventions.
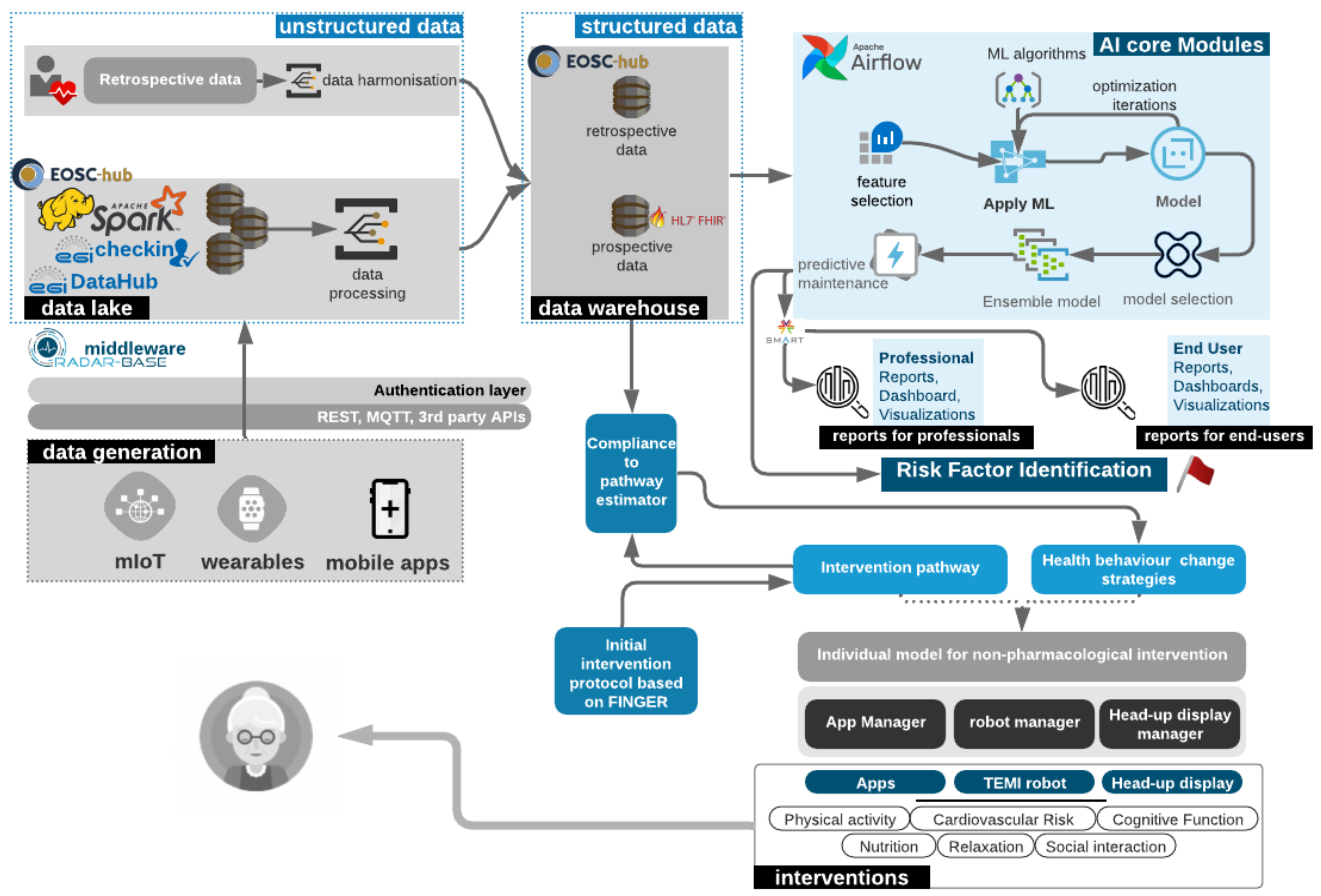
3.1. Technical Architecture of LETHE
3.2. Prediction Models
4. Discussion
4.1. Leveraging Big Data Analytics, AI and Biomarkers for Personalised Early Risk Prediction of Cognitive Decline
- Scalability and adaptation to data growth;
- Generation of information and insights on the temporal evolution of cognitive decline in predementia stages;
- Integration of heterogeneous sources of structured and unstructured data;
- Acquisition of high-quality data, their validation and verification;
- Securing of health data and anonymisation despite personalisation.
4.2. Long Term Disease Knowledge
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on the Public Health Response to Dementia; WHO: Geneva, Switzerland, 2021.
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Andrieu, S.; Guyonnet, S.; Coley, N.; Cantet, C.; Bonnefoy, M.; Bordes, S.; Bories, L.; Cufi, M.N.; Dantoine, T.; Dartigues, J.F.; et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): A randomised, placebo-controlled trial. Lancet Neurol. 2017, 16, 377–389. [Google Scholar] [CrossRef]
- Moll van Charante, E.P.; Richard, E.; Eurelings, L.S.; van Dalen, J.W.; Ligthart, S.A.; van Bussel, E.F.; Hoevenaar-Blom, M.P.; Vermeulen, M.; van Gool, W.A. Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): A cluster-randomised controlled trial. Lancet 2016, 388, 797–805. [Google Scholar] [CrossRef] [Green Version]
- WHO. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; WHO: Geneva, Switzerland, 2019.
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Bateman, R.J.; Xiong, C.; Benzinger, T.L.S.; Fagan, A.M.; Goate, A.; Fox, N.C.; Marcus, D.S.; Cairns, N.J.; Xie, X.; Blazey, T.M.; et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 2012, 367, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Mattsson, N.; Andreasson, U.; Zetterberg, H.; Blennow, K.; Alzheimer’s Disease Neuroimaging Initiative. Association of Plasma Neurofilament Light with Neurodegeneration in Patients with Alzheimer Disease. JAMA Neurol. 2017, 74, 557–566. [Google Scholar] [CrossRef]
- Verberk, I.M.W.; Slot, R.E.; Verfaillie, S.C.J.; Heijst, H.; Prins, N.D.; van Berckel, B.N.M.; Scheltens, P.; Teunissen, C.E.; van der Flier, W.M. Plasma Amyloid as Prescreener for the Earliest Alzheimer Pathological Changes. Ann. Neurol. 2018, 84, 648–658. [Google Scholar] [CrossRef]
- Anstey, K.J.; Zheng, L.; Peters, R.; Kootar, S.; Barbera, M.; Stephen, R.; Dua, T.; Chowdhary, N.; Solomon, A.; Kivipelto, M. Dementia Risk Scores and Their Role in the Implementation of Risk Reduction Guidelines. Front. Neurol. 2022, 12, 765454. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; Macchi, C. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2009, 39, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Arenaza-Urquijo, E.M.; Vemuri, P. Improving the resistance and resilience framework for aging and dementia studies. Alzheimer’s Res. Ther. 2020, 12, 41. [Google Scholar] [CrossRef] [Green Version]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for persons with mild to moderate dementia of the Alzheimer’s or vascular type: A review. Alzheimer’s Res. Ther. 2013, 5, 35. [Google Scholar] [CrossRef]
- Irwin, M.R.; Vitiello, M.V. Implications of sleep disturbance and inflammation for Alzheimer’s disease dementia. Lancet Neurol. 2019, 18, 296–306. [Google Scholar] [CrossRef]
- Bubu, O.M.; Brannick, M.; Mortimer, J.; Umasabor-Bubu, O.; Sebastião, Y.V.; Wen, Y.; Schwartz, S.; Borenstein, A.R.; Wu, Y.; Morgan, D.; et al. Sleep, Cognitive impairment, and Alzheimer’s disease: A Systematic Review and Meta-Analysis. Sleep 2016, 40, zsw032. [Google Scholar] [CrossRef]
- Shi, L.; Chen, S.J.; Ma, M.Y.; Bao, Y.P.; Han, Y.; Wang, Y.M.; Shi, J.; Vitiello, M.V.; Lu, L. Sleep disturbances increase the risk of dementia: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 40, 4–16. [Google Scholar] [CrossRef]
- Khalsa, D.S.; Newberg, A.B. Spiritual Fitness: A New Dimension in Alzheimer’s Disease Prevention. J. Alzheimer’s Dis. 2021, 80, 505–519. [Google Scholar] [CrossRef]
- Tang, E.Y.H.; Harrison, S.L.; Errington, L.; Gordon, M.F.; Visser, P.J.; Novak, G.; Dufouil, C.; Brayne, C.; Robinson, L.; Launer, L.J.; et al. Current Developments in Dementia Risk Prediction Modelling: An Updated Systematic Review. PLoS ONE 2015, 10, e0136181. [Google Scholar] [CrossRef] [Green Version]
- Kivipelto, M. Midlife vascular risk factors and Alzheimer’s disease in later life: Longitudinal, population based study. BMJ 2001, 322, 1447–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, A.; Ngandu, T.; Soininen, H.; Hallikainen, M.M.; Kivipelto, M.; Laatikainen, T. Validity of dementia and Alzheimer’s disease diagnoses in Finnish national registers. Alzheimer’s Dement. 2013, 10, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Pekkala, T.; Hall, A.; Lötjönen, J.; Mattila, J.; Soininen, H.; Ngandu, T.; Laatikainen, T.; Kivipelto, M.; Solomon, A. Development of a Late-Life Dementia Prediction Index with Supervised Machine Learning in the Population-Based CAIDE Study. J. Alzheimer’s Dis. 2017, 55, 1055–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamate, D.; Smith, R.; Tsygancov, R.; Vorobev, R.; Langham, J.; Stahl, D.; Reeves, D. Applying Deep Learning to Predicting Dementia and Mild Cognitive Impairment. In IFIP Advances in Information and Communication Technology; Springer International Publishing: Cham, Switzerland, 2020; pp. 308–319. [Google Scholar]
- Walters, K.; Hardoon, S.; Petersen, I.; Iliffe, S.; Omar, R.Z.; Nazareth, I.; Rait, G. Predicting dementia risk in primary care: Development and validation of the Dementia Risk Score using routinely collected data. BMC Med. 2016, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Sciarrone, A.; Bisio, I.; Garibotto, C.; Lavagetto, F.; Staude, G.H.; Knopp, A. Leveraging IoT Wearable Technology Towards Early Diagnosis of Neurological Diseases. IEEE J. Sel. Areas Commun. 2021, 39, 582–592. [Google Scholar] [CrossRef]
- Arabia, G.; Lupo, A.; Manfredini, L.I.; Vescio, B.; Nisticò, R.; Barbagallo, G.; Salsone, M.; Morelli, M.; Novellino, F.; Nicoletti, G.; et al. Clinical, electrophysiological, and imaging study in essential tremor-Parkinson’s disease syndrome. Park. Relat. Disord. 2018, 56, 20–26. [Google Scholar] [CrossRef]
- Li, Z.; Lian, L.; Pei, J.; She, Y. Design and implementation of wearable medical monitoring system on the internet of things. J. Ambient. Intell. Humaniz. Comput. 2021, 1–14. [Google Scholar] [CrossRef]
- Wang, F.; Casalino, L.P.; Khullar, D. Deep Learning in Medicine—Promise, Progress, and Challenges. JAMA Intern. Med. 2019, 179, 293–294. [Google Scholar] [CrossRef]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef]
- Peiffer-Smadja, N.; Maatoug, R.; Lescure, F.X.; D’Ortenzio, E.; Pineau, J.; King, J.R. Machine Learning for COVID-19 needs global collaboration and data-sharing. Nat. Mach. Intell. 2020, 2, 293–294. [Google Scholar] [CrossRef]
- Van Panhuis, W.G.; Paul, P.; Emerson, C.; Grefenstette, J.; Wilder, R.; Herbst, A.J.; Heymann, D.; Burke, D.S. A systematic review of barriers to data sharing in public health. BMC Public Health 2014, 14, 1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pezoulas, V.C.; Exarchos, T.P.; Fotiadis, D.I. (Eds.) Chapter 3—Medical data sharing. In Medical Data Sharing, Harmonization and Analytics; Academic Press: Cambridge, MA, USA, 2020; pp. 67–104. [Google Scholar]
- Hulsen, T. Sharing Is Caring-Data Sharing Initiatives in Healthcare. Int. J. Environ. Res. Public Health 2020, 17, 3046. [Google Scholar] [CrossRef] [PubMed]
- Pezoulas, V.C.; Exarchos, T.P.; Fotiadis, D.I. (Eds.) Chapter 4—Data protection. In Medical Data Sharing, Harmonization and Analytics; Academic Press: Cambridge, MA, USA, 2020; pp. 105–136. [Google Scholar]
- Pezoulas, V.C.; Exarchos, T.P.; Fotiadis, D.I. (Eds.) Chapter 5—Medical data harmonization. In Medical Data Sharing, Harmonization and Analytics; Academic Press: Cambridge, MA, USA, 2020; pp. 137–183. [Google Scholar]
- McMahan, H.B.; Moore, E.; Ramage, D.; Hampson, S.; y Arcas, B.A. Communication-Efficient Learning of Deep Networks from Decentralized Data. arXiv 2017, arXiv:cs.LG/1602.05629. [Google Scholar]
- Nori, V.S.; Hane, C.A.; Sun, Y.; Crown, W.H.; Bleicher, P.A. Deep neural network models for identifying incident dementia using claims and EHR datasets. PLoS ONE 2020, 15, e0236400. [Google Scholar] [CrossRef] [PubMed]
- Almubark, I.; Chang, L.C.; Shattuck, K.F.; Nguyen, T.; Turner, R.S.; Jiang, X. A 5-min Cognitive Task with Deep Learning Accurately Detects Early Alzheimer’s Disease. Front. Aging Neurosci. 2020, 12, 603179. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.R.; Gill, A.Q. Towards an IoT Big Data Analytics Framework: Smart Buildings Systems. In Proceedings of the 2016 IEEE 18th International Conference on High Performance Computing and Communications; IEEE 14th International Conference on Smart City; IEEE 2nd International Conference on Data Science and Systems (HPCC/SmartCity/DSS), Sydney, Australia, 12–14 December 2016; pp. 1325–1332. [Google Scholar]
- Zhang, Q.; Zhang, X.; Zhang, Q.; Shi, W.; Zhong, H. Firework: Big Data Sharing and Processing in Collaborative Edge Environment. In Proceedings of the 2016 Fourth IEEE Workshop on Hot Topics in Web Systems and Technologies (HotWeb), Washington, DC, USA, 24–25 October 2016; pp. 20–25. [Google Scholar]
- Rathore, M.M.; Ahmad, A.A.; Paul, A. IoT-based smart city development using big data analytical approach. In Proceedings of the 2016 IEEE International Conference on Automatica (ICA-ACCA), Curico, Chile, 19–21 October 2016. [Google Scholar]
- Kivipelto, M.; Ngandu, T.; Laatikainen, T.; Winblad, B.; Soininen, H.; Tuomilehto, J. Risk score for the prediction of dementia risk in 20 years among middle aged people: A longitudinal, population-based study. Lancet Neurol. 2006, 5, 735–741. [Google Scholar] [CrossRef]
- Hall, A.; Pekkala, T.; Polvikoski, T.; van Gils, M.; Kivipelto, M.; Lötjönen, J.; Mattila, J.; Kero, M.; Myllykangas, L.; Mäkelä, M.; et al. Prediction models for dementia and neuropathology in the oldest old: The Vantaa 85+ cohort study. Alzheimer’s Res. Ther. 2019, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Tolppanen, A.M.; Solomon, A.; Soininen, H.; Kivipelto, M. Midlife vascular risk factors and Alzheimer’s disease: Evidence from epidemiological studies. J. Alzheimer’s Dis. 2012, 32, 531–540. [Google Scholar] [CrossRef]
- Goerdten, J.; Čukić, I.; Danso, S.O.; Carrière, I.; Muniz-Terrera, G. Statistical methods for dementia risk prediction and recommendations for future work: A systematic review. Alzheimer’s Dement. 2019, 5, 563–569. [Google Scholar] [CrossRef]
- Solomon, A.; Turunen, H.; Ngandu, T.; Peltonen, M.; Levälahti, E.; Helisalmi, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; et al. Effect of the Apolipoprotein E Genotype on Cognitive Change During a Multidomain Lifestyle Intervention: A Subgroup Analysis of a Randomized Clinical Trial. JAMA Neurol. 2018, 75, 462–470. [Google Scholar] [CrossRef]
- De Wolf, F.; Ghanbari, M.; Licher, S.; McRae-McKee, K.; Gras, L.; Weverling, G.J.; Wermeling, P.; Sedaghat, S.; Ikram, M.K.; Waziry, R.; et al. Plasma tau, neurofilament light chain and amyloid-β levels and risk of dementia; a population-based cohort study. Brain 2020, 143, 1220–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Mielke, M.M.; Bell, W.R.; Reilly, C.; Zhang, L.; Lin, F.V.; Yu, F. Blood biomarkers as surrogate endpoints of treatment responses to aerobic exercise and cognitive training (ACT) in amnestic mild cognitive impairment: The blood biomarkers study protocol of a randomized controlled trial (the ACT Trial). Trials 2020, 21, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, J.M.; Cronk, B.B.; Anderson, H.S.; Donnelly, J.E.; Thomas, G.P.; Harsha, A.; Brooks, W.M.; Swerdlow, R.H. Cardiorespiratory Fitness and Brain Atrophy in Early Alzheimer’s Disease. Neurology 2008, 71, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, F.; Heffner, K.L.; Ren, P.; Tivarus, M.E.; Brasch, J.; Chen, D.G.; Mapstone, M.; Porsteinsson, A.P.; Tadin, D. Cognitive and Neural Effects of Vision-Based Speed-of-Processing Training in Older Adults with Amnestic Mild Cognitive Impairment: A Pilot Study. J. Am. Geriatr. Soc. 2016, 64, 1293–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, R.; Liu, Y.; Ngandu, T.; Antikainen, R.; Hulkkonen, J.; Koikkalainen, J.; Kemppainen, N.; Lötjönen, J.; Levälahti, E.; Parkkola, R.; et al. Brain volumes and cortical thickness on MRI in the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER). Alzheimer’s Res. Ther. 2019, 11, 53. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Phase I | Phase II | Acquisition Type | Data Source | |
|---|---|---|---|---|
| Clinical Parameter | Anthropometric data | Anthropometric measures | time-discrete | |
| Blood markers | Blood markers | time-discrete | ||
| Blood pressure | Blood pressure | time-discrete | ||
| - | Genetic markers | time-discrete | ||
| Physical Activity and Health | Medication | Medication | time-discrete | |
| Heart diseases | Heart diseases | time-discrete | ||
| Diabetes | Diabetes | time-discrete | ||
| Injuries | Injuries | time-discrete | ||
| Family history | Family history | time-discrete | ||
| Falls/injury | Falls/injury | time-discrete | ||
| Exercise/Activity | continuous | Sensor | ||
| Heart rate | continuous | Sensor | ||
| SpO2 | continuous | Sensor | ||
| Gait characteristics | continuous | App | ||
| Cardio- vascular risk | Alcohol | time-discrete | ||
| Alcohol | continuous | App | ||
| Smoking | - | time-discrete | ||
| Smoking | continuous | App | ||
| Social interaction | Marriage status | Marriage status | time-discrete | |
| Education level | Education level | time-discrete | ||
| Occupation | Occupation | time-discrete | ||
| Living alone | Living alone | time-discrete | ||
| Location change | continuous | Sensor | ||
| Social Apps | continuous | App | ||
| Time spent outside | continuous | Sensor | ||
| Chatbot | continuous | App | ||
| Nutrition | Weight | - | time-discrete | |
| Weight | continuous | App | ||
| Meals | continuous | App | ||
| Calorie intake | continuous | App | ||
| Water intake | continuous | App | ||
| Cognition | Dementia (type) | Dementia (type) | time-discrete | |
| Impairment state | Impairment state | time-discrete | ||
| Dementia ratings | Dementia ratings | time-discrete | ||
| MRI | MRI | time-discrete | ||
| CSF | CSF | time-discrete | ||
| ApoE | ApoE | time-discrete | ||
| Cognitive games | continuous | App | ||
| Tapping/typing games | continuous | App | ||
| Eye movement | continuous | App | ||
| Meditation and Sleep | Depression/GDS | Depression/GDS | time-discrete | |
| Sleep quality | - | time-discrete | ||
| Sleep quality | continuous | Sensor | ||
| Meditation | continuous | App | ||
| Pulse, HRV | continuous | Sensor | ||
| Emotion recording | continuous | App |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanke, S.; Mangialasche, F.; Bödenler, M.; Neumayer, B.; Ngandu, T.; Mecocci, P.; Untersteiner, H.; Stögmann, E. AI-Based Predictive Modelling of the Onset and Progression of Dementia. Smart Cities 2022, 5, 700-714. https://doi.org/10.3390/smartcities5020036
Hanke S, Mangialasche F, Bödenler M, Neumayer B, Ngandu T, Mecocci P, Untersteiner H, Stögmann E. AI-Based Predictive Modelling of the Onset and Progression of Dementia. Smart Cities. 2022; 5(2):700-714. https://doi.org/10.3390/smartcities5020036
Chicago/Turabian StyleHanke, Sten, Francesca Mangialasche, Markus Bödenler, Bernhard Neumayer, Tiia Ngandu, Patrizia Mecocci, Helena Untersteiner, and Elisabeth Stögmann. 2022. "AI-Based Predictive Modelling of the Onset and Progression of Dementia" Smart Cities 5, no. 2: 700-714. https://doi.org/10.3390/smartcities5020036