
Aptamers as Theranostics in Cardiovascular Diseases
Department of Pharmacy, Central University of Rajasthan, NH-8, Bandar Sindri, Ajmer 305817, India
*
Author to whom correspondence should be addressed.
J. Nanotheranostics 2023, 4(3), 408-428; https://doi.org/10.3390/jnt4030018
Submission received: 26 July 2023
/
Revised: 19 August 2023
/
Accepted: 4 September 2023
/
Published: 6 September 2023
(This article belongs to the Special Issue Interventional Nanotheranostics for Translational Nano-Immunotherapy)
Abstract
:Cardiovascular disease (particularly atherosclerosis) is a leading cause of death around the world, and there still exists a need for improved diagnostic techniques and treatments to improve patient outcomes as well as minimize the disease’s global burden. Aptamers are short, single-stranded DNA or RNA molecules that are accompanied by unique characteristics such as specificity, high binding affinity, ease of cellular internalization, and rapid tissue accumulation capabilities, offering great potential as theranostic agents in cardiovascular diseases with significantly improved sensitivity and accuracy. These theranostic agents provide a combination of therapy and diagnostics in which aptamers may diagnose and treat disease simultaneously. Therefore, this review article summarizes the role of aptamer-based probes for imaging and theranostics in cardiovascular disease. It also provides insight into current research and future treatment techniques that are very relevant for future clinical practice with the aim of improving the quality of life of cardiovascular disease patients.
1. Introduction
Cardiovascular diseases (CVDs) affect the blood vessels and heart, including heart failure, peripheral artery disease, stroke, and coronary artery disease. It is the most prevalent cause of mortality worldwide, accounting for 17.7 million deaths every year. This figure will likely grow to 23.6 million by 2030, which is considerably more prevalent than cancer and other diseases [1]. The current diagnostic relies on imaging techniques that fail to reveal the nature and extent of plaque buildup. In contrast, the traditional treatment technique for CVD using diuretics, beta-blockers, hypolipidemic drugs, etc., exhibits non-targeted drug delivery to the site of action that produces potential side effects and toxicities [2]. Nanotechnology has the potential to revolutionize the field of CVDs by offering innovative solutions for diagnosis, treatment, and prevention. It is a multidisciplinary field that involves manipulating matter at the nanoscale (nanometers). The nanometric biomaterial can easily penetrate inside the cell through a tight junction; its smaller size enables exposure to a larger surface area and provides exhaustive binding affinity and surface modification. The knowledge and utilization of innovative nanotechnology will provide a safe and effective platform for diagnosing and treating CVDs [3]. Integrating diagnostic and therapeutic functions into a single platform is termed a theranostic system. These systems can provide real-time monitoring of the treatment response and adjust therapy accordingly. Theranostic agents have evolved into crucial mainstays for facilitating an effective treatment regimen for a wide range of serious illnesses due to the need for improved disease prognosis and advanced therapeutic decisions at the patient-specific level. Early disease identification will consequently enhance the probability of patient survival, and optimal treatment will result in the highest therapeutic efficacy and ideal safety profile [4].
Nanotheranostics is an emerging field combined with diagnostics, therapeutic, and nanotechnology. It is one of the newest and most technologically advanced branches of health care and medicine with intriguing ramifications. It entails using multifunctional nanostructures for diagnosis, treatment, and ongoing drug monitoring inside the body. This combined system of diagnosis and therapy helps to monitor the drug’s real-time response in a non-invasive way, which enhances the standard of care. Traditional diagnostic procedures like PET (positron emission tomography), MRI (magnetic resonance imaging), and NIR (near-infrared radiation) fluorescence have limitations such as low sensitivity, specificity, signal scattering, and low efficacy in terms of monitoring. The delivery of therapeutically effective regimens at the desired location is also made possible by nanotheranostics, which offer intriguing alternatives to the limitations of current traditional diagnostic methods [5]. Utilizing site-specific ligands for convenient surface modification, nanotheranostics enables disease-specific delivery without endangering nearby healthy tissues. Single-stranded DNA or RNA oligonucleotides known as “aptamers” have high affinity and specificity towards binding to a wide range of targets, including different small organic compounds, ions, large proteins, and living cells. They are called “chemical antibodies” because they can recognize their targets with high binding affinity and selectivity as they have distinct and stable three-dimensional shapes both in vitro and in vivo. These aptamers can specifically target critical molecules involved in the coagulation cascade, such as thrombin or factor Xa, providing a more targeted and potentially safer alternative to traditional anticoagulant drugs. Additionally, aptamers can also be designed to bind to specific receptors on endothelial cells, promoting vasodilation and improving blood flow in patients with conditions like hypertension or atherosclerosis. This targeted approach could help alleviate symptoms and reduce the need for invasive procedures like angioplasty or bypass surgery. Furthermore, aptamers can be utilized as diagnostic tools by conjugating them with fluorescent dyes or nanoparticles, allowing for detecting biomarkers associated with cardiovascular diseases. This non-invasive method could provide early detection and monitoring of disease progression, enabling timely intervention and personalized treatment plans [6]. Overall, this review is focused on the versatility and specificity of aptamers conjugated nanotheranostic-based advancement and approaches that can be promising candidates that effectively help diagnose and treat CVDs.
2. Cardiovascular Diseases
The term “cardiovascular disease” describes several ailments that impact the blood vessels and heart. Depending on the situation, it affects other organs and the heart. CVDs are the leading cause of morbidity and mortality worldwide with an estimated 17.9 million deaths each year (according to the WHO) [7]. CVDs encompass a range of conditions, including
- Strokes and transient ischemic attacks occur when the blood supply to the brain is temporarily reduced (in the case of a stroke) or wholly cut off [8].
- Coronary heart disease is caused by an imbalance between the oxygen supply and demand in the cardiac muscle.
- Peripheral arterial disease is caused by plaque buildup or decreased blood flow in the peripheral arteries (limbs).
- Aortic disease occurs when the blood supply to the aorta is interrupted or significantly reduced, resulting in potential side effects like aneurysms or aortic dissection [9].
- A blood clot blocking one of the pulmonary arteries results in a pulmonary embolism, which prevents blood from reaching the lungs [10].
- Another condition brought on by blood clots is deep vein thrombosis, which typically develops in the deep veins of the legs and may cause life-threatening complications if it spreads to the lungs [11].
- Coronary artery disease is characterized by the restriction or obstruction of the coronary arteries, which deliver oxygen-rich blood to the heart muscle and frequently cause chest pain or heart attacks.
- High blood pressure, or hypertension, can strain and harm blood vessels all over the body, raising the risk of developing several cardiovascular diseases.
- Heart valve abnormalities that affect proper blood flow and may result in heart failure or other complications, which are known as valvular heart disease.
- Congenital heart defects are structural flaws that can interfere with normal blood flow and are present at birth [12].
Cardiovascular diseases collectively contribute to a significant burden on healthcare systems. To address this challenge, researchers and healthcare professionals continuously strive to develop innovative strategies for preventing, detecting, and managing CVDs. These efforts involve a multidisciplinary approach integrating advances in imaging technologies and pharmacology. By understanding the complex interplay between genetic predisposition and environmental factors, personalized medicine holds promise for tailoring treatments to individual patients. Advancements in medical science and technology are revolutionizing the diagnosis and treatment of cardiovascular diseases. Machine learning and artificial learning are being integrated into medical imaging analysis to improve accuracy in diagnosing conditions and predicting outcomes. Liquid biopsies are being explored for non-invasive early detection of cardiovascular diseases using blood-based markers and genetic material [13]. Researchers are identifying novel biomarkers that can predict disease progression, risk of events, and response to treatment. High-sensitivity troponin assays, B-type natriuretic peptide (BNP), and other markers aid in diagnosis and prognosis [14]. Additionally, the advent of novel advanced imaging techniques like cutting-edge imaging technologies, including 3D echocardiography, cardiac computed tomography, and MRI, provide detailed anatomical and functional information, aiding in early disease detection and treatment planning and allowing for the precise identification of high-risk individuals and targeted interventions [15]. Precision medicine is gaining traction, tailoring treatment plans based on individual patient characteristics, genetics, and molecular profiles. Targeted therapies are being developed to target specific pathways and cellular processes involved in various heart diseases. Minimally invasive interventions like transcatheter aortic valve replacement and percutaneous coronary interventions are being developed, allowing for less invasive procedures and quicker recovery times. Regenerative medicine is being researched using stem cells, tissue engineering, and gene therapy to repair damaged cardiac tissue [16]. Digital health solutions, such as wearable devices, mobile apps, and remote monitoring tools, are being used to track patients’ cardiovascular health and enhance patient engagement. Telemedicine has gained prominence, especially during the COVID-19 pandemic, allowing patients to receive consultations, monitoring, and follow-up care remotely [17]. Pharmacogenomics is becoming increasingly important in tailoring drug therapies for cardiovascular conditions. Artificial intelligence algorithms are being developed to assist healthcare providers in making treatment decisions based on patient data, medical history, and current guidelines. Pharmacological advancements have led to the development of more effective drugs that target specific molecular pathways involved in CVD pathogenesis [18]. Theranostics is a new field of medicine that uses specific diagnostic tests to find the best way to diagnose and treat patients. Although theranostic research on CVDs is still in its infancy, nanotheranostic has advanced quickly over the past few decades because of the benefits of combining nanotechnology for diagnosis and treatment in a single agent [19].
3. Nanotheranostics and Their Role in CVDs
Nanotheranostics is an innovative method with numerous potential applications in treating cardiovascular diseases. Because nanotheranostics combine diagnostic and therapeutic capabilities into a single agent, they hold great promise for personalized medicine. These nanoscale systems enable early detection and diagnosis of CVDs due to their ability to target diseased tissues precisely. Additionally, they can deliver therapeutic payloads directly to the affected areas, minimizing off-target effects and enhancing the efficacy of the treatment. Development in nanotheranostics has accelerated because it can avoid the drawbacks of traditional techniques, such as low bioavailability and systemic toxicity [20]. To learn more about the detection of diseases, progression of conditions, effectiveness of the therapeutic molecule administered, and planning of improved or similar therapies in the future, nanotechnology aims to combine imaging, a therapeutic agent, and a biomarker. Near-infrared imaging, CT, fluorescence-based imaging agents, MRI, and other imaging agents are conjugated with nanostructure to enable early and precise diagnosis based on imaging systems [21]. Cardioprotective medications have disadvantages, such as poor bioavailability, nonspecific action, less precise targeting, and a shorter half-life. By creating a nanocarrier that can transport both the diagnostic and the therapeutic molecule, we can achieve selective targeting, tracking, or monitoring of the drug delivery, a higher drug load, increased penetration, controlled release, enhanced biocompatibility, tuneability, and surface functionalization [22]. Nanomaterials such as polymeric, metal, lipid, magnetic NPs, multifunctional nanocomposites, quantum dots (QDs), and other nanomaterials have been investigated to fabricate nanotheranostic systems. These systems exhibit specific applications in cardiovascular disorders to achieve early diagnosis and superior therapy (Figure 1) [23].
Wu et al. (2021) prepared chitosan nanococktails entrapped with iron oxide nanoparticles and nanoceria. Cerium oxide was used as self-regenerating anti-ROS therapeutics with chemically transitioning to tetravalence from trivalent states, and iron oxide was used as a contrast agent for MRI. An in vitro study of the chitosan nanococktail revealed a reduction in the ROS level and less toxicity to LPS macrophage (J774A) [24]. Ma et al. (2021) developed lipid-specific fluorophores (LSP) and prednisolone-loaded RBC-coated micelles as atherosclerosis theranostics. Copolymers PMPCP (MEMA-co-PDMA) were used to achieve self-assembled micelles, and RBC coating was used to achieve biomimetic action (for more extended circulation and evading the phagocytic system). The micelles were found to be stable, and minimum leakage was traced using LSP, offering orange-red fluorescent in blood. As LSP micelles resulted in higher affinity to lipids, they accumulated in atherosclerotic lesions, presenting fluorescent green, and released prednisolone to achieve anti-inflammatory activity. The shift in fluorescence from green to blue revealed ROS-responsive and anti-inflammatory activity [25]. Obstructive thrombosis can be prevented by targeting FTIAN nanoparticles as a fibrin targeting and imaging agent and tirofiban as an antiplatelet therapeutic. FTIAN is a near-infrared fluorescent dye (IR820) conjugated with boronate antioxidant polymers and fibrin-targeting pentapeptides. It can target accumulated fibrin, scavenge hydrogen peroxide, and help in preventing platelet activation. The active targeting of nanoparticles demonstrates site-specific binding of CD40 ligand, inhibition of H2O2 generation, and suppression of TNF-α. FTIAN-targeted nanoparticles imaged usinga photoacoustic signal exhibit excellent antiplatelet, antioxidant, and anti-inflammatory activity in a ferric chloride-induced carotid thrombosis mouse model [26]. Photodynamic selenium nanoparticles (Se-NPs) were prepared by Lu et al. (2017) to target inflammatory macrophages using a multilayer coating strategy. Initially, NPs were coated with chitosan-conjugated rose bengal and glutathione (via Se-S bond); lastly, the surface was modified with catalase enzymes (first coating). The second coating was performed by conjugating hyaluronic acid, ethylenediamine, and folic acid. The second negatively charged coating showed electrostatic interaction with positively charged chitosan-rose bengal-catalase while loading into selenium NPs. The HA and FA coatings on Se-NPs showed specific binding to active macrophages during in vitro studies. According to phototoxicity studies, Se-NPs can kill catalase-activated macrophages by converting H2O2 to the toxic singlet oxygen 1O2, which kills cells. Transferring H2O2 to the harmful singlet oxygen, 1O2 reduced the H2O2 level in LPS-stimulated macrophages to 85%. As a result, the lesions showed lower levels of released NO and H2O2 and activated macrophage, preventing the escalation of inflammation [27]. To treat myocardial infarction, Somasuntharam et al. (2016) created Cy5-labeled, DNAzyme surface-modified gold nanoparticles. They used TNF-mRNA and DNAzyme to knock down TNF-gene expression in macrophage RAW 264.7 before testing the nanoparticles on adult Sprague Dawley rats. These nanoparticles significantly reduced TNF expression in LPS-stimulated macrophages. In addition, exvivofluorescence images of the mouse heart showed that the nanoparticles could be found for at least three days after injection. Overall, the gold nanoparticles mentioned above are promising therapeutic agents [28]. Various other nanotheranostic are mentioned in Table 1.
4. Aptamer Nanoconjugates for Theranostic Applications in Cardiovascular Diseases
4.1. Aptamers
Aptamers are short chains of oligonucleotides that have the ability to identify and bind targets having a specific sequence shown in Figure 2 [36]. Aptamers are commonly classified into DNA or RNA aptamers and oligopeptide aptamers. Single-stranded DNA/RNA oligonucleotides (5–40 kDa) called DNA/RNA aptamers can fold into distinct 3-dimensional structures and attach to their target molecules very specifically and with high affinity. The process of obtaining aptamers is typically done through a technique called Systematic Evolution of Ligand via Exponential enrichment (SELEX), discovered by Tuerk, Gold, Ellington, and Szostak in the late 1990s. Followed by this, Sullenger laboratory demonstrated that nucleic acids that bind proteins could serve potentially as therapeutic agents [6]. Recent advancements in the SELEX process involved exposing a large collection of random nucleotide sequences (containing 1013 to 1015 sequences) that exhibit the highest precision and overall affinity toward the desired target, which is further amplified for examination and application. A revolutionary selection method, called free selection (FRELEX) does not involve the immobilization of the target protein or the oligonucleotide repository, in contrast with the popular SELEX method. It is important to note that the restricted movement of targeted molecules signifies the potential of aptamers to restrain the expression of crucial sequences that would otherwise be available in their free state and play a defining role in oligonucleotide binding interactions [37,38].
In addition to the widely used antibodies, aptamers offer significant promise as diagnostic toolkits and therapeutic agents. A larger size of antibodies makes them impractical for targeting various sites, while aptamers provide an advantage over this because their smaller size provides greater access to a larger number of epitopes. Aptamers are chemically easy to synthesize in vitro with a rapid diffusion rate in solution, providing rapid measurements during end-to-end batch variations. Additionally, aptamers are stable over higher temperatures with less toxicity and immunogenicity, which makes them suitable for the development of different diagnostic and therapeutic applications [39].
Single-stranded DNA (ssDNA)-based aptamers have been successfully used to target a wide variety of targets, including small molecules, amino acid sequences, and carbohydrates [40]. These aptamers are utilized as biosensors to detect the targets in various complex matrices, including body fluids and food samples. The design of these aptasensors enables attachment to the target of interest, resulting in a detectable alteration in the electrophysiological and optical signaling [41].
To successfully target various cardiovascular diseases, a variety of nano-structures functionalized with aptamers are used as theranostics [42]. Additionally, while aptamers can be easily conjugated to nanoparticle surfaces, conjugation seldom alters their natural affinity for the target site or organ, indicating the high applicability of these nanoconjugates in disease imaging and site-specific drug delivery [43].
4.2. Aptamers for Diagnosis of Cardiovascular Diseases
4.2.1. Troponin I
Troponin I, a well-researched cardiac biomarker, plays a crucial role in assessing myocardial damage. When the heart muscle is injured, troponin is released into the bloodstream within a relatively short timeframe of 1 to 3 h [44]. The concentration of troponin reaches its peak, at a level of 100 ng/mL, between 1 and 2 days after the onset of a heart attack. Subsequently, the elevated levels of troponin persist for approximately 10 to 12 days.
Troponin is made up of mainly three subunits includingtroponin I, troponin C, and troponin T. Troponin I (cTnI) and troponin T (cTnT) are found in three isoforms in humans with slow and fast skeletal cardiovascular isform. As a result, it has been found that cTn-I and cTn-T are extremely susceptible and precise indicators for identifying cardiac damage [45,46].
In recent times, the integration of nanotechnology with biosensing platforms has proven to be highly advantageous. Nanostructures, when used to restrict the movement of drugs, transduction, or signal creation and processing, significantly enhance the analytical capabilities of biosensors. Numerous research laboratories have successfully developed electrochemical-based aptasensors in conjunction with nanomaterials for sensitive detection of myocardial problems associated with troponin I [47].
In a study conducted by Jo et al., a novel amperometric biosensor was developed. This biosensor utilized dual aptamers and a nanocomposite consisting of gold-conjugated nanoparticles-TTCA (5,2′:5′2′′-terthiophene-3′-carboxylic acid) [48]. To construct the sensing platform, screen-printed carbon electrodes were used and subsequently electrodeposited with AuNPs. The conductive monomer TTCA was then electropolymerized onto the electrodes. Certain groups containing carboxylic moiety in TTCA facilitated the covalent bonding of the amino-modified Tro4 aptamer, which played a crucial role in target recognition [49].
Subsequently, additional aptasensors utilizing sandwich-based configurations were developed to detect troponin I. A group from China devised distinct electrochemical biosensing techniques for troponin I utilizing ssDNA nanotetrahedrons (NTH) connected to dual-aptamers. NTHs are nucleic acids with a highly rigid framework consisting of four single-stranded DNA molecules, which may be uniformly assembled on the electrode plane surface. NTHs improve the aptamers’ distribution and orientation by serving as a divider between them and the surface [50]. As a result, they improve the accessibility and recognition efficiency of the target, leading to enhanced analytical performance of the aptasensor.
Another study showed the development of an aptamer-based dual-biosensor utilizing an amalgam of tetrahedron cage and nanohybrid electrochemicalcatalysts for labeling purposes. The innovative approach involved replacing natural enzymes with enzymes for signal amplification. The utilization of nanocatalysts proved advantageous due to their enhanced stability and cost-effectiveness over naturally occurring enzymes. These nanoprobes were created by incorporating dual-metal copper-augmented Au nanoparticles with troponin 4 and troponin 6 aptamers onto Fe3O4@UiO-66 nanozymes. These nanoprobes were successfully used to catalyze the oxidation of hydroquinone, resulting in amplified electrochemical signals and improved detection sensitivity [51].
A recent study introduced a novel approach for the amperometric determination of cTnI using sandwich-based architecture. In this method, an aptasensing surface was created by applying it to an SPCE variant of graphene-oxide (GO) modified via carboxyethylsilanetriol [52]. This carboxylic acid-enriched surface was then used to immobilize an amino-modified troponin I aptamer, which served as the recognition probe. The novelty of this strategy lies in the dramatically enhanced and improved loading capacity of aptamers, which also probed a sensitivity limit of 0.8 pg/mL.
Chekin et al. also explored a similar approach by functionalizing N-pr-GO (porous reduced graphene oxide doped with nitrogen) with 1-pyrenecarboxylic acid (pyCOOH) to elevate the inclining endurance of the troponin4-based aptamer. In order to mitigate imprecise interactions commonly observed on graphene-operated surfaces, the researchers integrated pyrene modified with polyethylene glycol (py-PEG) into the system through non-covalent interactions. Additionally, the density of the aptamer and pyCOOH over N-pr-GO complex interaction was also altered with the addition of py-PEG, boosting the aptasensor’s sensitivity [53].
In addition, aptamer-MIP (molecular imprinted polymerization) hybrid receptors have been developed as dual-operatedaptsensorsin order to detect troponinI. In this approach, an amino-derived aptamer was restricted on a glassy carbon electrode (GCE) altered with ZnO-NPs (zinc oxide nanoparticles) in order to obtain acTnI sequence template. These troponin–aptamer complexes were then encapsulated in electropolymerized methylene blue monomer units. The resulting cavities developed the aptamer-MIP hybrid receptor, with electrochemical probing via polymerized MB (methylene blue). This hybrid receptor approach exhibited exponential targeting for troponin I determination. By combining the advantages of MIPs cavities and aptamers, these hybrid receptor sensors offer enhanced selectivity for the recognition sites, overcoming potential interference from other proteins [54].
Overall, the use of dual aptamers, where the first aptamer is immobilized and the second aptamer is labeled for signal generation, can be further enclosed with entrapped drug delivery to enhance sensitivity and specific treatment simultaneously.
4.2.2. Myoglobin
Myoglobin is a relatively small protein that weighs 16 kDa and plays a crucial role in binding, storing, and transporting oxygen molecules. It may be present in both cardiac and skeletal muscles. Myoglobin levels in the blood are commonly range between 6 and 85 ng/mL. However, in cases of muscle cell injury, such as acute myocardial infarction (AMI), myoglobin is released into the bloodstream, causing its levels to rise to 75–200 ng/mL, serving as the diagnostic cutoff value [55,56].
As a gold standard in diagnosing acute myocardial infarction, myoglobin has been the subject of some research on electrochemical aptasensing. One study by Ghafori et al. focused on synthesizing a nanocomposite of carbon nanotubes (PtSnNP/CNTs) and polytungstate (PtSn) nanoparticles to serve as a nanocarrier for the immobilization and signal amplification of myoglobin aptamers [57]. The following composite allowed the protein-modified aptamer to be immobilized over the electrode surface, hindering electron transfer upon target binding. The electrochemical probe hexacyanoferrate was then used to detect myoglobin with differential pulse voltammetry in specimens of serum, yielding attractive performance with a level of detection of 2.0 pM and a varying range of 10–200 nM [58].
In another study, an electrode made of tin oxide doped with fluorine (FTO) was substituted with boron nitride nanosheets (BNNs), permitting the chemical accumulating of gold-surfaced nanoparticles (Au-NPs) using a seed-associated chemical minimization method. BNNs possess a broader surface area, which easily becomes functionalized with metal-based nanoparticles, resulting in advanced catalytic nanohybrids. The functionalized BNNs-AuNPs-FTO surface served as the site for immobilizing aptamer with disulfide functionality. The resulting aptasensor exhibited a high signaling responsiveness within a fluctuating response ranging from 100 to 100,000 ng/mL as the process of aptamer–myoglobin complex reduced the electrical characteristics [59].
Anotherstudy reported using cationic polyethyleneimine (PEI) as a reductant for graphene oxide (GO). By increasing the positive charges on graphene oxide using this technique, the negatively charged DNA aptamer was directly immobilized without the use of linkers or coupling chemicals. Additionally, the nanocomposite facilitated quick electron transferring and enabled signal amplification [60]. Using this customized surface, the researchers achieved label-free electrolytic identification of myoglobin by monitoring the change in current result from direct electron transfer between the electrodes and the target. The constructed aptasensor demonstrated the ability to detect myoglobin between the range of 0.01 and 1000 ng/mL, which aligns well with clinical values [61].
A recent development in myoglobin biomarker targeting and diagnosis involved the screening of aptamers using a microfluidic SELEX system. This method allowed for the generation of the Myo040-7-27 aptamer specific within a rangeof dissociation values (4.3–6.8 nM) after seven phases of choosing negative and positive selection components [61]. The chosen 40mer aptamer was subsequently used to build a highly sensitive, label-free electrochemical biosensor that used the target-activated aptamer displacement technique in order to detect myoglobin biomarkers for cardiovascular disease treatment, achieving a sensitivity of 10 pM [62].
Wang et al. (2015) proposed a new investigation for detecting particular myoglobinusing a customized glucometer as an indicator for acute myocardial infarction. This assay involved the non-covalent immobilization of the anti-myoglobin antibody on a polystyrene microplate to target and bind myoglobin [63]. Subsequently, myoglobin-specific aptamer-invertase conjugates were immobilized onto the myoglobin as their cognate targets. The invertase conjugates then hydrolyzed sucrose into glucose, reflecting the correlation between myoglobin and the proportion of glucose. Analytical results demonstrated that this novel assay could measure even trace amounts (approximately 50 pM, which is lower than the healthy clinical myoglobin cutoff point) of serum myoglobin [64].
4.2.3. Creatine Kinase
Creatine phosphokinase is an enzyme that exists in three different forms, known as isoenzymes, in humans—CK-BB, CK-MM, and CK-MB. These abbreviations are derived from the amalgamation of the M and B isoforms. Among these isoenzymes, CK-MB is predominantly found in the myocardium (heart muscle). An elevated volume of CK-MB in the bloodstream is a highly selective and sensitive indicator of myocardial injury and inflammation [65]. The permissible standards for serum CK-MB range between 3.0 and 5.0% (percentage of CK activity) or 5.0 and 25.0 IU/L. Following a myocardial infarction, CK-MB activity reaches its peak level within 3 to 8 h and remains elevated for 24–48h. Despite the availability of troponins T and I assay, which allows for slightly more immediate identification of acute coronary syndrome (ACS) and better specificity compared with CK-MB, the evaluation of CK and CK-MB still has a significant role in diagnosing clinical conditions.
In a recent study, new single-stranded DNA aptamers, namely, c.pt.1 and c.pt.0, were identified for their profound selectivity and binding affinity to CK-MB. A lateral flow assay based on c.pt.0 and fluorescent microspheres was performed using serum samples of artificial origin. The level of detection (LOD) for CK-MB was comparably lower at 0.3 ng/mL. This encouraging outcome suggests this assay has potential use in clinical diagnostics. Another study utilized c.pt.1 to create a hybrid microfluidic chipset packed with DNA-based hydrogel for the purpose of detecting CK-MB. Therefore, the signal produced from this chip showed a linear correlation with the magnitude of CK-MB concentration in the spectrum of 0.1–750 nM [66].
4.2.4. Cardiac-Related Fatty Acid Membrane-Bound Protein
Heart-located fatty acid binding protein (HFABP) is a protein weighing 15 kDa, which plays a role in the transport, metabolism, and absorption of long-chain fatty acids by cells. HFABP is a distinct form of fatty acid-binding protein found predominantly in cardiomyocytes. In cases of cardiac injury, HFABP levels in the blood rise within 30–90 min and return to baseline between 24 and 36 h. As a result of its immediate release into the bloodstream, HFABP serves as a potential biomarker for acute coronary syndrome (ACS). Its faster release and cardiac specificity make it superior in myoglobin detection in myocardial infarction [67,68].
To date, only one research paper has been published on the development of aptamers targeting HFABP. Two distinct DNA aptamers, namely, N13 and N53, were isolated, each with its own binding site. N13 exhibited a KD value of 74.nM, while N53 had a KD value of 334 nM. These aptamers were used in an AuNP aggregation-based colorimetric assay for HFABP detection, which yielded a limit of detection (LOD) of 54 ng/mL. However, this LOD falls short of practical usage requirements.
Moving forward, future research on aptamers for HFABP aims to isolate novel aptamers specific to HFABP and develop novel detection techniques and treatments, such as nanomedicine sandwich detection aptasensors.
4.2.5. C-Reactive Protein
C-reactive protein (CRP) is produced by the liver and other cell sections in reaction to inflammation, which includes heart damage. While CRP is not specific to any particular condition, it is widely recognized due to its important role as a cardiac biomarker. Elevated levels of CRP are associated with an increased risk of atherothrombotic events, such as cardiac death, ischemic stroke, and myocardial infarction. Human CRP is a significant inflammatory marker that provides a valuable diagnosis of serious heart disorders like ischemic stroke, myocardial infarction, and sudden cardiac death [69].
Researchers have developed a CRP-based aptasensor for potential cardiovascular diagnosis. Using a screening method involving graphene oxide, two DNA aptamers were selected that could bind to a monomeric form of CRP, rather than the pentameric form. The aptamers demonstrated a low dissociation constant of 3 nM, indicating high selectivity and affinity for CRP. The aptamers were immobilized through the 3′ terminus, which facilitated their specific folding into a three-dimensional conformation for CRP binding [70].
It is worth noting that there are very few aptasensors developed for detecting myoglobin in comparison to troponin I.
4.2.6. Other Diagnostic Aptasensors
Researchers mounted both BNP and cTnI aptamers towards gold-plated imprinted electrodes to enable electrochemical measurement at the same time. Propargyl acetic acid and polyethyleneimine/reduced graphene oxide sheets were used to modify these electrodes. The aptamers were then immobilized over the surface using Cu(I)-catalyzed click chemistry. The working of this technique was verified by analyzing serum samples from patients with suspected coronary artery disease in its early stages [71]. The results from the aptasensor showed good agreement with those from the standard kits used in hospitals. The aptasensor also demonstrated reusability up to ten times without losing its sensitivity. This method yields a stable and accurate electrochemical system with a threshold of 0.9 ng/mL, without any signal amplification or labels [72].
Another electrochemical sensing platform based on a platinum multiarray, was designed for the detection of cTnI and BNP. These cardiac biomarkers are widely used in the detection of congestive cardiac failure and acute myocardial infarction. The multi-array aptasensoris based on platinum wires, which allows tiny devices because it enables the quick, inexpensive, and label-filtered monitoring of several indicators in biological fluids. The label-free aptasensor successfully achieved impedimetric detection of cTn-I and BNP with high susceptibility and sensitivity [73].
Wang et al. created a novel heteronanostructure, as a dimetric aptasensing device that enables highly sensitive detection of troponin I and myoglobin. The researchers synthesized nanospheres measuring 200 to 500 nm, consisting of nanostructures embedded-graphdiyne with a hydrogen substitution (HsGDY). The combination of HsGDY showed chemical robustness and three-dimensional porous networks with nanodiamonds along with biological compatibility and electrochemical activity resulting in enhanced sensitivity. The limit of detection for troponinI was 9.4 fg/mL, while for myoglobin, it was 6.9 ng/mL [74]. Table 2 discusses the aptamers nanoconjugates used for the diagnosis of CVDs.
4.3. Aptamers for the Treatment of Cardiovascular Diseases with Clinical Trial Pipelines
Aptamers have a wide range of uses in the treatment of cardiovascular disorders as medicinal agents. Currently, there are ongoing clinical trials to evaluate the effectiveness of aptamers in various diagnostics and treatments, as summarized in the table provided.
One particular blood glycoprotein, known as von Willebrand factor (VWF), is produced by endothelial cells, megakaryocytes, and subendothelial connective tissues. VWF plays a crucial role in blood clotting in veins and arteries. There are several aptamers that have been extensively studied for their ability to bind with the platelet’s A1 domain of activated VWF, which acts as an anti-platelet therapeutic agent. ARC1779 and ARC1172, 41mer DNA aptamers, are two examples of anti-platelet aptamers [86,87].
Other aptamers have been found to interact with the thrombin that promotes platelet activation and aggregation, making them useful in the management of clotting disorders of the heart. Additionally, certain aptamers have shown potential as anti-coagulants and direct thrombin inhibitors in cardiovascular treatment. Aptamer–antidote pairs that bind particularly to proteases serine-like factor-IX have also been investigated for cardiovascular treatment strategies [6,88].
A recent development reported that aptamer oligonucleotides have gained attention as anticoagulant and antithrombotic agents for the treatment of cardiovascular diseases. Aptamers that target factors like factor XII, tissue factor, vasopressin-binding, mesenchymal stem cells, and auto-antibodies in cardiomyopathies provide potential use as therapeutics for different heart disorders [89,90].
Additionally, several aptamers have been explored for their potential use in intracoronary stent coating to improve reendothelialization. However, it is important to note that while aptamers have shown promise for the effective treatment of cardiac disorders, their potency in this regard is currently less than their diagnostic capabilities. Figure 3 represents the aptamers nanoconjugates as an effective thernaostic therapy in the treatment of cardiovascular diseases.
4.3.1. Aptamers Binding von Willebrand Factor (vWF)
One specific area of focus in aptamer research is the binding of aptamers to the von Willebrand Factor (VWF). It is a massive multimeric glycoprotein that plays an essential role in platelet attachment to sites of arterial damage and thrombus development. Conventional treatments for ischemic disorders primarily focus on the accumulation of platelets and activation, rather than VWF activity. However, VWF has been identified as a potential emerging target in cardiac disorders.
Several aptamers have been developed with the attachment of the A1 domain of VWF. ARC1172, a 41mer DNA aptamer, has shown promise in inhibiting carotid artery thrombosis and VWF-dependent platelet aggregation [91]. Derived from ARC1172, ARC1779 has been modified to enhance its inhibitory effect on VWF platelet function. According to clinical studies, ARC1779 lowers cerebral thrombo-embolism in people having carotid artery endarterectomy, with fewer bleeding complications compared with anti-platelet aggregation [92].
The second-generation anti-VWF aptamer demonstrated strong inhibitory effects on platelet accumulation, prompting various agonist actions in both healthy individuals and patients with myocardial infarction. Compared with ARC1779, ARC15105 has a greater bioavailability and an extended half-life [93].
Another aptamer, BT100, has been developed with additional base pairs and conjugated with polyethylene glycol to create BT200. BT200 efficiently blocks the VWF, favoring the arterial bloodstream system. Specific medications, like BT101, can quickly reverse it. BT200 has shown promise in lowering increased VWF levels in patients with stroke from major artery atherosclerosis and is a possible candidate for subsequent stroke prevention [94,95].
DTRI-031, an optimized VWF aptamer, was developed to avoid platelet-rich thromboembolism and restore circulation after ischemic occlusion. It showed higher anti-thrombotic efficacy and reversibility when compared with alteplase, an FDA-approved therapeutic drug for arterial recanalization [96].
In conclusion, aptamers that bind to VWF have shown promise as medicinal substances for the treatment of heart disorders. Further research and development are needed to optimize their efficacy and explore their full potential in clinical applications.
4.3.2. Aptamers Binding Thrombin
Thrombus formation is a common factor in many events of the cardiac system and occurs through two main coagulation routes involving thrombosis and coagulation of proteins. Abciximab, Aspirin, and tirofiban are examples of antiplatelet medicines, whereas warfarin, heparin, and apixaban are examples of anticoagulants [97]. The coagulation cascade key enzyme, thrombin, is a prime candidate for the creation of anticoagulant therapeutic drugs.
In 2002, RNA aptamers were introduced as reversible antagonists. Rusconi et al. successfully inhibited the anticoagulant effects of aptamers by choosing oligonucleotides against FIXa. One such novel FIXa inhibitor based on RNA aptamers, called Pegnivacogin, has been found to reduce platelet activity in patients with acute coronary syndromes (ACS) [98]. A serine protease plasma kallikrein, involved in blood coagulation, amplifies the production of activated factor XIIa (FXIIa), which results in the production of fibrin clots and thrombin synthesis. Furthermore, it was discovered that an RNA aptamer that targets kallikrein can suppress the intrinsic pathway of thrombosis and minimize the production of bradykinin [99].
Moreover, aptamers producedusing CE-SELEX target polypeptide convertase subtilisin/kexin9 (PCSK9). These aptamers have been shown to effectively restrain PCSK9 and serve as viable treatments for people with high cholesterol levels in coronary artery disease (CAD) [100]. However, traditional anti-thrombosis medications increase the threat of bleeding, and there are few antagonists readily available. Notably, single-stranded DNA aptamers that target Dabigatran Etexilate, a low molecular weight anticoagulant drug, have been developed with a dissociation constant (Kd) leveling from 46 to 208 nM. These aptamers could be a valuable option for detecting Dabigatran’s effects and managing the risk of bleeding after therapeutics [37].
Thrombin, a serine protease, plays a critical role in activating several proteins in the coagulation cascade. Nu172 is a DNA aptamer specifically designed to bind to and inhibit thrombin [101]. Nu172 was discovered from a degenerate DNA library using SELEX and subsequently modified to a length of 26 nucleotides without any additional chemical alterations. Intravenous administration of Nu172 during acute cardiovascular surgical procedures effectively prevents the formation of blood clots [101,102].
The thrombin-binding aptamer (TBA) is an artificial DNA sequence that inhibits the formation of fibrin clots. Bao et al. successfully synthesized oligonucleotide 8-trifluoromethyl-2’-deoxyguanosine (FG), which enhanced the stability and antithrombotic activity of TBA by incorporating it into the TBA sequence [103].
Together, these investigations demonstrated the potential of thrombin-specific aptamers as anti-thrombotic medicines.
4.3.3. Aptamers Binding to Factor IX
A serine protease called factor IX is a valuable target in cardiovascular diseases. It plays a crucial role in the coagulation process by generating the necessary amount of thrombin. Initially produced as an inactive precursor called a zymogen, it can be activated in the presence of factor IXa, calcium ions, membrane phospholipids, and a cofactor for factor VIII. Factor IXa disintegrates a specific bond in factor X, resulting in the formation of factor Xa. This thrombin can be produced by factor Xa from prothrombin, a key step in coagulation [104].
One anti-coagulation system called REG1 consists of a factor IXa-selective aptamer called RB006 and its oligonucleotide antidote, RB007. SELEX, which makes use of a 2′-ribo purine/2′-fluoro pyrimidine transcript library, was utilized to develop RB006. The aptamer was subsequently modified by truncating it to 34 nucleotides, conjugating it to a PEG of 40 kDa to decrease kidney clearance, and adding an inverted nucleotide to the 3′-terminus to prevent degradation by 3′-exonucleases [105]. RB006 binds to factor IXa with a dissociation constant (Kd) of 2 nM. On the other hand, the 17mer oligonucleotide RB007 is entirely 2′-O-methyl substituted and completes the 5′-terminal sections of RB006. As an antidote, RB007 effectively alters the structure of RB006, reducing its ability to prevent coagulation [99,105].
Another aptamer, R39, was selected using Cell-SELEX against immortalized endothelial cells. This aptamer may identify and internalize primary endothelial cells through endocytosis. Additionally, R39 can carry siVEGFR2, a gene-targeting molecule, in the shape of a lengthy polymeric structure to effectively inhibit the expressions of the target gene [106]. The avβ3 aptamer, which targets the endothelial cells that express integrin avβ3, has shown inhibitory effects on affecting the migration and proliferation of smooth muscle cells. By affecting the signaling pathway for Ras-PI3K/MAPK, it holds promise as a therapeutic agent for treating post-PTCA vascular restenosis, a condition associated with vascular remodeling and atherosclerosis [107].
We presume that upcoming research mentioned in Table 3 on aptamer nanoconjugates will identify a positive perspective for developing potential therapeutic outcomes in the case of cardiovascular disorders.
5. Challenges and Future Aspects of Aptamers as Theranosticsin CVDs
The interaction of aptamers with cell surface receptors can hinder their ability to deliver drug compounds to the nucleus, limiting access to intracellular target molecules. To overcome this challenge, it is recommended to use compounds that induce cell surface receptor-dependent endocytosis on the drug carrier. Developing aptamers against specific targets relevant to CVDs can be difficult, which limits their use as theranostics. Aptamers can also exhibit off-target effects when they interact with structures similar to the target molecule, which can pose a significant challenge for aptamer-based therapies. The complex and time-consuming production process of aptamers, along with the difficulties in purification, adds to the challenges. Although aptamers offer better stability compared with antibodies, they can still be degraded by enzymes in the body, impacting their effectiveness and durability. The rapid clearance of aptamers from the blood and other biological environments due to the activity of endonucleases has also posed challenges for their diagnostic and drug delivery applications. Changing the conformational structure of aptamers can increase their shelf life, but time is still a limiting factor, and reducing the retention time is not desirable in medical practice. Despite these limitations, ongoing research aims to address these challenges and improve the clinical applicability of aptamers as theranostics in cardiovascular disorders.
The spectrum of overall vascular disease has been established, despite certain limits in diagnosis and treatment, as etiological mechanisms of cardiovascular diseases, particularly our understanding of pan-vascular disorders, continue to progress. In-stent thrombosis and bleeding issues in the body are the most common side effects of current cardiovascular disease treatment methods including stent implantation and balloon dilatation [110]. A lot of attention has recently been paid to aptamers in the areas of biosensing and targeted medication delivery. As opposed to proteinaceous targeting ligands, aptamers do not run the risk of inducing unfavorable immunological reactions. Furthermore, they can be easily modified without compromising their biological roles, giving aptamers a great opportunity to conjugate or combine with other components such as cardio-therapeutics for targeted therapies, vehicles for drug delivery, nanomaterials for biosensing, and detection of interested analytes using various methods and disease diagnostics. NPs would improve aptamer in vivo stability, thus increasing target selectivity and sensitivity. NPs have high surface-to-volume ratios, which would allow for more targeted interactions. Even supramolecular structures resulting from the effective combination of aptamers and delivery agents have been tested and examined in vivo and can be fine-tuned further to pave the path for clinical use [111,112]. As previously stated, targeted treatment with aptamer nanoconjugates has also been undertaken. Aptamer nanoconjugates have proved useful in achieving enhanced amounts of payloads/cargoes in certain cells and tissues in the field of cardiovascular treatment. Finally, as we obtain a better knowledge of the underlying inflammatory and immune-mediated responses that occur in CVD, we may investigate the application of immunotherapy to reduce overall inflammation and immune-mediated damage, therefore reducing the progression of CVD states. Increasing our knowledge of the molecular and pathophysiological mechanisms that underpin CVD is critical because it will allow us to design timely, targeted, specific, and effective treatment modalities and drug-delivery platforms.
6. Conclusions
Aptamers are single-stranded DNA or RNA molecules that can bind to specific target molecules with high affinity and selectivity. By selecting aptamers that specifically recognize biomarkers associated with cardiovascular diseases, such as proteins or receptors, aptamer nanoconjugates can be designed to selectively target diseased cells or tissues. Aptamer nanoconjugates hold great potential for theranostic applications in cardiovascular diseases. These nanoconjugates, aptamers with nanoparticles, offer a multifunctional platform for targeted therapy and diagnostic imaging. Therapeutically, aptamer nanoconjugates can deliver drugs or therapeutic agents directly to the site of cardiovascular disease. The nanoparticles used in the nanoconjugates can encapsulate or conjugate with therapeutic molecules, protecting them from degradation and improving their delivery efficiency. This targeted approach minimizes off-target effects and reduces systemic toxicity. Moreover, aptamer nanoconjugates can serve as theranostic agents by combining therapeutic and diagnostic functions. By incorporating imaging agents into the nanoconjugates, they can enable non-invasive imaging of cardiovascular lesions, allowing for early detection and monitoring of disease progression. Additionally, the aptamers themselves can serve as diagnostic probes, selective binding of disease-specific biomarkers and facilitating the identification of cardiovascular abnormalities. The use of aptamer nanoconjugates in cardiovascular theranostics offers several advantages over conventional approaches. They provide targeted drug delivery, enhance therapeutic efficacy, minimize side effects, and enable real-time imaging and diagnostics. However, further research is needed to optimize the design, stability, and delivery efficiency of these nanoconjugates, as well as to evaluate their safety and long-term effects in preclinical and clinical settings.
Author Contributions
Conceptualization & writing-original draft preparation, M.R. and P.K.; supervision: A.K.G. All authors have read and agreed to the published version of the manuscript.
Funding
ICMR-SRF fellowship (RBMH/FW/2021/9).
Acknowledgments
The authors acknowledge support from ICMR-SRF fellowship (RBMH/FW/2021/9).
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Wang, Y.; Li, G.; Yang, L.; Luo, R.; Guo, G. Development of Innovative Biomaterials and Devices for the Treatment of Cardiovascular Diseases. Adv. Mater. 2022, 34, 2201971. [Google Scholar] [CrossRef]
- Chopra, H.; Bibi, S.; Mishra, A.K.; Tirth, V.; Yerramsetty, S.V.; Murali, S.V.; Ahmad, S.U.; Mohanta, Y.K.; Attia, M.S.; Algahtani, A.; et al. Nanomaterials: A Promising Therapeutic Approach for Cardiovascular Diseases. J. Nanomater. 2022, 2022, 4155729. [Google Scholar] [CrossRef]
- Rhee, J.W.; Wu, J.C. Advances in nanotechnology for the management of coronary artery disease. Trends Cardiovasc. Med. 2013, 23, 39–45. [Google Scholar] [CrossRef]
- Kelkar, S.S.; Reineke, T.M. Theranostics: Combining Imaging and Therapy. Bioconjug Chem. 2011, 22, 1879–1903. [Google Scholar] [CrossRef]
- Cherry, S.R.; Louie, A.Y.; Jacobs, R.E. The Integration of Positron Emission Tomography with Magnetic Resonance Imaging. Proc. IEEE 2008, 96, 416–438. [Google Scholar] [CrossRef]
- Wang, P.; Yang, Y.; Hong, H.; Zhang, Y.; Cai, W.; Fang, D. Aptamers as Therapeutics in Cardiovascular Diseases. Curr. Med. Chem. 2011, 18, 4169–4174. [Google Scholar] [CrossRef]
- Nawaz, M.S.; Shoaib, B.; Ashraf, M.A. Intelligent Cardiovascular Disease Prediction Empowered with Gradient Descent Optimization. Heliyon 2021, 7, e06948. [Google Scholar] [CrossRef]
- Easton, J.D.; Saver, J.L.; Albers, G.W.; Alberts, M.J.; Chaturvedi, S.; Feldmann, E.; Hatsukami, T.S.; Higashida, R.T.; Johnston, S.C.; Kidwell, C.S.; et al. Definition and evaluation of transient ischemic attack: A scientific statement for healthcare professionals from the American heart association/American stroke association stroke council; council on cardiovascular surgery and anesthesia; council on cardio. Stroke 2009, 40, 2276–2293. [Google Scholar] [CrossRef]
- Choi, D.; Hwang, K.C.; Lee, K.Y.; Kim, Y.H. Ischemic heart diseases: Current treatments and future. J. Control Release 2009, 140, 194–202. [Google Scholar] [CrossRef]
- Amorim, B.J.; Rigolon, M.Y.; Ramos, C.D. Diagnosis of pulmonary embolism. Nucl. Cardiol. Basic. Adv. Concepts Clin. Pract. 2021, 168, 723–739. [Google Scholar]
- Esmon, C.T. Inflammation and thrombosis. J. Thromb. Haemost. 2003, 1, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Ghofrani, H.A.; Grünig, E.; Klose, H.; Olschewski, H.; Rosenkranz, S. Pulmonary hypertension. Dtsch. Arztebl. Int. 2017, 114, 73–84. [Google Scholar] [CrossRef]
- Choy, G.; Khalilzadeh, O.; Michalski, M.; Do, S.; Samir, A.E.; Pianykh, O.S.; Geis, J.R.; Pandharipande, P.V.; Brink, J.A.; Dreyer, K.J. Current Applications and Future Impact of Machine Learning in Radiology. Radiology 2018, 288, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tan, G.J.; Han, L.N.; Bai, Y.Y.; He, M.; Liu, H.B. Novel biomarkers for cardiovascular risk prediction. J. Geriatr. Cardiol. 2017, 14, 135–150. [Google Scholar]
- Counseller, Q.; Aboelkassem, Y. Recent technologies in cardiac imaging. Front. Med. Technol. 2023, 4, 984492. [Google Scholar] [CrossRef] [PubMed]
- Tobis, J.M.; Abudayyeh, I. New devices and technology in interventional cardiology. J. Cardiol. 2015, 65, 5–16. [Google Scholar] [CrossRef]
- Xie, Y.; Lu, L.; Gao, F.; He, S.J.; Zhao, H.J.; Fang, Y.; Yang, J.M.; An, Y.; Ye, Z.W.; Dong, Z. Integration of Artificial Intelligence, Blockchain, and Wearable Technology for Chronic Disease Management: A New Paradigm in Smart Healthcare. Curr. Med. Sci. 2021, 41, 1123–1133. [Google Scholar] [CrossRef]
- Zaiou, M.; El Amri, H. Cardiovascular pharmacogenetics: A promise for genomically-guided therapy and personalized medicine. Clin. Genet. 2017, 91, 355–370. [Google Scholar] [CrossRef]
- Shrivastava, S.; Jain, S.; Kumar, D.; Soni, S.L.; Sharma, M. A Review on Theranostics: An Approach to Targeted Diagnosis and Therapy. Asian J. Pharm. Res. Dev. 2019, 7, 63–69. [Google Scholar] [CrossRef]
- Mura, S.; Couvreur, P. Nanotheranostics for personalized medicine. Adv. Drug Deliv. Rev. 2012, 64, 1394–1416. [Google Scholar] [CrossRef]
- Hahn, M.A.; Singh, A.K.; Sharma, P.; Brown, S.C.; Moudgil, B.M. Nanoparticles as contrast agents for in-vivo bioimaging: CNanoparticles as contrast agents for in-vivo bioimaging: Current status and future perspectivesCardioprotective medications have disadvantages, such as poor bioavailability, nonspecific action, les. Anal. Bioanal. Chem. 2011, 399, 3–27. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Y.; Liu, Y.; Huang, H.; Roy, S.; Song, Z.; Guo, B. Recent advances in nanomedicines for imaging and therapy of myocardial ischemia-reperfusion injury. J. Control Release 2023, 353, 563–590. [Google Scholar] [CrossRef]
- Siafaka, P.I.; Okur, N.Ü.; Karantas, I.D.; Okur, M.E.; Gündoğdu, E.A. Current update on nanoplatforms as therapeutic and diagnostic tools: A review for the materials used as nanotheranostics and imaging modalities. Asian J. Pharm. Sci. 2021, 16, 24–46. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, R.; Tran, H.D.N.; Kurniawan, N.D.; Moonshi, S.S.; Whittaker, A.K.; Ta, H.T. Chitosan Nanococktails Containing Both Ceria and Superparamagnetic Iron Oxide Nanoparticles for Reactive Oxygen Species-Related Theranostics. ACS Appl. Nano Mater. 2021, 4, 3604–3618. [Google Scholar] [CrossRef]
- Ma, B.; Xu, H.; Wang, Y.; Yang, L.; Zhuang, W.; Li, G.; Wang, Y. Biomimetic-Coated Nanoplatform with Lipid-Specific Imaging and ROS Responsiveness for Atherosclerosis-Targeted Theranostics. ACS Appl. Mater. Interfaces 2021, 13, 35410–35421. [Google Scholar] [CrossRef]
- Kang, C.; Gwon, S.; Song, C.; Kang, P.M.; Park, S.C.; Jeon, J.; Hwang, D.W.; Lee, D. Fibrin-Targeted and H2O2-Responsive Nanoparticles as a Theranostics for Thrombosed Vessels. ACS Nano 2017, 11, 6194–6203. [Google Scholar] [CrossRef]
- Lu, K.Y.; Lin, P.Y.; Chuang, E.Y.; Shih, C.M.; Cheng, T.M.; Lin, T.Y.; Sung, H.W.; Mi, F.L. H2O2-Depleting and O2-Generating Selenium Nanoparticles for Fluorescence Imaging and Photodynamic Treatment of Proinflammatory-Activated Macrophages. ACS Appl. Mater. Interfaces 2017, 9, 5158–5172. [Google Scholar] [CrossRef]
- Somasuntharam, I.; Yehl, K.; Carroll, S.L.; Maxwell, J.T.; Martinez, M.D.; Che, P.L.; Brown, M.E.; Salaita, K.; Davis, M.E. Knockdown of TNF-α by DNAzyme gold nanoparticles as an anti-inflammatory therapy for myocardial infarction. Biomaterials 2016, 83, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Oumzil, K.; Ramin, M.A.; Lorenzato, C.; Hémadou, A.; Laroche, J.; Jacobin-Valat, M.J.; Mornet, S.; Roy, C.-E.; Kauss, T.; Gaudin, K.; et al. Solid Lipid Nanoparticles for Image-Guided Therapy of Atherosclerosis. Bioconjug Chem. 2016, 27, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.B.; Yao, R.; Akurathi, V.; Snay, E.R.; Thedsanamoorthy, J.K.; Zurakowski, D.; Ericsson, M.; Friehs, I.; Wu, Y.; Levitsky, S.; et al. Intracoronary delivery of mitochondria to the ischemic heart for cardioprotection. PLoS ONE 2016, 11, e0160889. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Cheng, A.; Jia, Y.; Yang, L.; Ning, Y.; Xu, L.; Zhong, Y.; Zhuang, Z.; Guan, J.; Zhang, X.; et al. PH-Responsive Multifunctional Theranostic Rapamycin-Loaded Nanoparticles for Imaging and Treatment of Acute Ischemic Stroke. ACS Appl. Mater. Interfaces 2021, 13, 56909–56922. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Liu, Y.; Chen, J.; Liu, T.; Gu, Z.; Zhang, J.; Gu, X.; Teng, G.; Yang, F.; Gu, N. Platelet bio-nanobubbles as microvascular recanalization nanoformulation for acute ischemic stroke lesion theranostics. Theranostics 2018, 8, 4870–4883. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Yang, J.; Liu, R.; Qiao, C.; Lu, Z.; Shi, Y.; Fan, Z.; Zhang, Z.; Zhang, X. Dual-targeting theranostic system with mimicking apoptosis to promote myocardial infarction repair via modulation of macrophages. Theranostics 2017, 7, 4149. [Google Scholar] [CrossRef]
- Vazquez-Prada, K.X.; Moonshi, S.S.; Wu, Y.; Akther, F.; Tse, B.W.C.; Sokolowski, K.A.; Peter, K.; Wang, X.; Xu, G.; Ta, H.T. A Spiky Silver-Iron Oxide Nanoparticle for Highly Efficient Targeted Photothermal Therapy and Multimodal Imaging of Thrombosis. Small 2023, 19, 2205744. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Bao, Q.; Miao, Y.; Cheng, Q.; Chen, Y.; Yang, S.; Mao, C.; Yang, M. Peptide-Enabled Thrombus-Targeting Nanoparticles for Highly Effective Targeted CT Imaging and Eradication of Thrombi. Adv. Funct. Mater. 2023, 2303331, early view. [Google Scholar] [CrossRef]
- Jin, H. Perspectives of Aptamers for Medical Applications. In Aptamers for Medical Applications From Diagnosis to Therapeutics; Dong, Y., Ed.; Springer: Singapore, 2021; pp. 405–462. [Google Scholar]
- Aljohani, M.M.; Chinnappan, R.; Eissa, S.; Alsager, O.A.; Weber, K.; Cialla-May, D.; Popp, J.; Zourob, M. In Vitro Selection of Specific DNA Aptamers Against the Anti-Coagulant Dabigatran Etexilate. Sci. Rep. 2018, 8, 13290. [Google Scholar] [CrossRef]
- Wu, L.; Wang, Y.; Xu, X.; Liu, Y.; Lin, B.; Zhang, M.; Zhang, J.; Wan, S.; Yang, C.; Tan, W. Aptamer-Based Detection of Circulating Targets for Precision Medicine. Chem. Rev. 2021, 121, 12035–12105. [Google Scholar] [CrossRef]
- Liu, M.; Wang, L.; Lo, Y.; Shiu, S.C.C.; Kinghorn, A.B.; Tanner, J.A. Aptamer-Enabled Nanomaterials for Therapeutics, Drug Targeting and Imaging. Cells 2022, 11, 159. [Google Scholar] [CrossRef]
- Hong, K.L.; Sooter, L.J. Single-Stranded DNA Aptamers against Pathogens and Toxins: Identification and Biosensing Applications. Biomed. Res. Int. 2015, 2015, 419318. [Google Scholar] [CrossRef]
- Wang, K.; Wang, M.; Ma, T.; Li, W.; Zhang, H. Review on the Selection of Aptamers and Application in Paper-Based Sensors. Biosensors 2023, 13, 39. [Google Scholar] [CrossRef]
- MacRitchie, N.; Di Francesco, V.; Ferreira, M.F.M.M.; Guzik, T.J.; Decuzzi, P.; Maffia, P. Nanoparticle theranostics in cardiovascular inflammation. Semin. Immunol. 2021, 56, 101536. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Chen, J.; Wu, M.; Zhao, J.X. Aptamers: Active targeting ligands for cancer diagnosis and therapy. Theranostics 2015, 5, 322–344. [Google Scholar] [CrossRef] [PubMed]
- Babuin, L.; Jaffe, A.S. Troponin: The biomarker of choice for the detection of cardiac injury. Can. Med. Assoc. J. 2005, 173, 1191–1202. [Google Scholar] [CrossRef] [PubMed]
- Korff, S.; Katus, H.A.; Giannitsis, E. Differential diagnosis of elevated troponins. Heart 2006, 92, 987–993. [Google Scholar] [CrossRef]
- Teekakirikul, P.; Ho, C.Y.; Seidman, C.E. Chapter 47—Inherited Cardiomyopathies. In Korf BBTE and RP and P of MG; Rimoin, D., Pyeritz, R., Sixth, E., Eds.; Academic Press: Oxford, UK, 2013; pp. 1–38. [Google Scholar]
- Malik, P.; Gupta, R.; Malik, V.; Ameta, R.K. Emerging nanomaterials for improved biosensing. Meas. Sensors 2021, 16, 100050. [Google Scholar] [CrossRef]
- Nooranian, S.; Mohammadinejad, A.; Mohajeri, T.; Aleyaghoob, G.; Kazemi Oskuee, R. Biosensors based on aptamer-conjugated gold nanoparticles: A review. Biotechnol. Appl. Biochem. 2022, 69, 1517–1534. [Google Scholar] [CrossRef]
- Jo, H.; Her, J.; Lee, H.; Shim, Y.B.; Ban, C. Highly sensitive amperometric detection of cardiac troponin I using sandwich aptamers and screen-printed carbon electrodes. Talanta 2017, 165, 442–448. [Google Scholar] [CrossRef]
- Schlapak, R.; Danzberger, J.; Armitage, D.; Morgan, D.; Ebner, A.; Hinterdorfer, P.; Pollheimer, P.; Gruber, H.J.; Schäffler, F.; Howorka, S. Nanoscale DNA tetrahedra improve biomolecular recognition on patterned surfaces. Small 2012, 8, 89–97. [Google Scholar] [CrossRef]
- Sun, D.; Luo, Z.; Lu, J.; Zhang, S.; Che, T.; Chen, Z.; Zhang, L. Electrochemical dual-aptamer-based biosensor for nonenzymatic detection of cardiac troponin I by nanohybrid electrocatalysts labeling combined with DNA nanotetrahedron structure. Biosens. Bioelectron. 2019, 134, 49–56. [Google Scholar] [CrossRef]
- Villalonga, A.; Estabiel, I.; Pérez-Calabuig, A.M.; Mayol, B.; Parrado, C.; Villalonga, R. Amperometric aptasensor with sandwich-type architecture for troponin I based on carboxyethylsilanetriol-modified graphene oxide coated electrodes. Biosens. Bioelectron. 2021, 183, 113203. [Google Scholar] [CrossRef]
- Yan, P.; Shu, S.; Zou, L.; Liu, Y.; Li, J.; Wei, F. Density functional theory study of active sites on nitrogen-doped graphene for oxygen reduction reaction. R. Soc. Open Sci. 2021, 8, 210272. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, Z.; Khajehsharifi, H.; Hashemnia, S.; Solati, Z.; Azimpanah, R.; Shahrokhian, S. Evaluation of molecular imprinted polymerized methylene blue/aptamer as a novel hybrid receptor for Cardiac Troponin I (cTnI) detection at glassy carbon electrodes modified with new biosynthesized ZnONPs. Sens. Actuators B Chem. 2020, 320, 128316. [Google Scholar] [CrossRef]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, İ.; Yardim, M. Biomarkers in acute myocardial infarction: Current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H. Traditional and novel diagnostic biomarkers for acute myocardial infarction. Egypt. J. Intern. Med. 2022, 34, 87. [Google Scholar] [CrossRef]
- Rabai, S.; Teniou, A.; Catanante, G.; Benounis, M.; Marty, J.L.; Rhouati, A. Fabrication of AuNPs/MWCNTS/chitosan nanocomposite for the electrochemical aptasensing of cadmium in water. Sensors 2022, 22, 105. [Google Scholar] [CrossRef]
- Gomes, E.S.; Leite, F.R.F.; Ferraz, B.R.L.; Mourão, H.A.J.L.; Malagutti, A.R. Voltammetric sensor based on cobalt-poly(methionine)-modified glassy carbon electrode for determination of estriol hormone in pharmaceuticals and urine. J. Pharm. Anal. 2019, 9, 347–357. [Google Scholar] [CrossRef]
- Bagheri, H.; Talemi, R.P.; Afkhami, A. Gold nanoparticles deposited on fluorine-doped tin oxide surface as an effective platform for fabricating a highly sensitive and specific digoxin aptasensor. RSC Adv. 2015, 5, 58491–58498. [Google Scholar] [CrossRef]
- Sharma, A.; Bhardwaj, J.; Jang, J. Label-Free, Highly Sensitive Electrochemical Aptasensors Using Polymer-Modified Reduced Graphene Oxide for Cardiac Biomarker Detection. ACS Omega 2020, 5, 3924–3931. [Google Scholar] [CrossRef]
- Radi, A.E.; Abd-Ellatief, M.R. Electrochemical aptasensors: Current status and future perspectives. Diagnostics 2021, 11, 104. [Google Scholar] [CrossRef]
- Lou, X.; Oh, S.S.; Zhang, Y.; Xiao, Y.; Soh, H.T.; Qian, J. Generation of Highly Specific Aptamers via Micromagnetic Selection. Anal. Chem. 2011, 83, 1866. [Google Scholar]
- Wang, Q.; Liu, F.; Yang, X.; Wang, K.; Wang, H.; Deng, X. Sensitive point-of-care monitoring of cardiac biomarker myoglobin using aptamer and ubiquitous personal glucose meter. Biosens. Bioelectron. 2015, 64, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Zhang, T.T.; Huang, Z.F.; Hu, S.W.; Zhao, W.; Xu, J.J.; Chen, H.-Y. An exploration of nucleic acid liquid biopsy using a glucose meter. Chem. Sci. 2018, 9, 3517–3522. [Google Scholar] [CrossRef] [PubMed]
- Takagi, Y.; Yasuhara, T.; Gomi, K. Creatine kinase and its isozymes. Rinsho Byori. 2001, 185, 1–8. [Google Scholar]
- Zhang, J.; Lv, X.; Feng, W.; Li, X.; Li, K.; Deng, Y. Aptamer-based fluorometric lateral flow assay for creatine kinase MB. Microchim. Acta 2018, 185, 364. [Google Scholar] [CrossRef]
- Rezar, R.; Jirak, P.; Gschwandtner, M.; Derler, R.; Felder, T.K.; Haslinger, M.; Kopp, K.; Seelmaier, C.; Granitz, C.; Hoppe, U.C.; et al. Heart-type fatty acid-binding protein (H-FABP) and its role as a biomarker in heart failure: What do we know so far? J. Clin. Med. 2020, 9, 164. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Sanders, L.; Lawler, O.; Riley, T.; Maki, K. Hyperlipidemia. In Caballero BBTE of HN; Fourth, E., Ed.; Academic Press: Oxford, UK, 2023; pp. 361–379. [Google Scholar]
- Sproston, N.R.; Ashworth, J.J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, N.; Taghdisi, S.M.; Yazdian-Robati, R.; Mansouri, A.; Abnous, K.; Ahmad Mohajeri, S. Selection of DNA aptamers for tramadol through the systematic evolution of ligands by exponential enrichment method for fabrication of a sensitive fluorescent aptasensor based on graphene oxide. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 259, 119840. [Google Scholar] [CrossRef]
- Grabowska, I.; Sharma, N.; Vasilescu, A.; Iancu, M.; Badea, G.; Boukherroub, R.; Ogale, S.; Szunerits, S. Electrochemical Aptamer-Based Biosensors for the Detection of Cardiac Biomarkers. ACS Omega 2018, 3, 12010–12018. [Google Scholar] [CrossRef]
- Omage, J.I.; Easterday, E.; Rumph, J.T.; Brula, I.; Hill, B.; Kristensen, J.; Ha, D.T.; Galindo, C.L.; Danquah, M.K.; Sims, N.; et al. Cancer Diagnostics and Early Detection Using Electrochemical Aptasensors. Micromachines 2022, 13, 522. [Google Scholar] [CrossRef]
- Shanmugam, N.R.; Muthukumar, S.; Tanak, A.S.; Prasad, S. Multiplexed electrochemical detection of three cardiac biomarkers cTnI, cTnT and BNP using nanostructured ZnO-sensing platform. Future Cardiol. 2018, 14, 131–141. [Google Scholar] [CrossRef]
- Qiao, X.; Li, K.; Xu, J.; Cheng, N.; Sheng, Q.; Cao, W.; Yue, T.; Zheng, J. Novel electrochemical sensing platform for ultrasensitive detection of cardiac troponin I based on aptamer-MoS2 nanoconjugates. Biosens. Bioelectron. 2018, 113, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Dorraj, G.S.; Rassaee, M.J.; Latifi, A.M.; Pishgoo, B.; Tavallaei, M. Selection of DNA aptamers against Human Cardiac Troponin I for colorimetric sensor based dot blot application. J. Biotechnol. 2015, 208, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Krasitskaya, V.V.; Goncharova, N.S.; Biriukov, V.V.; Bashmakova, E.E.; Kabilov, M.R.; Baykov, I.K.; Sokolov, A.E.; Frank, L.A. The Ca2+-Regulated Photoprotein Obelin as a Tool for SELEX Monitoring and DNA Aptamer Affinity Evaluation. Photochem. Photobiol. 2020, 96, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Torrini, F.; Palladino, P.; Brittoli, A.; Baldoneschi, V.; Minunni, M.; Scarano, S. Characterization of troponin T binding aptamers for an innovative enzyme-linked oligonucleotide assay (ELONA). Anal. Bioanal. Chem. 2019, 411, 7709–7716. [Google Scholar] [CrossRef]
- Ara, M.N.; Hyodo, M.; Ohga, N.; Hida, K.; Harashima, H. Development of a novel DNA aptamer ligand targeting to primary cultured tumor endothelial cells by a cell-based SELEX method. PLoS ONE 2012, 7, e50174. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, W.; Xing, Y.; Yang, X.; Wang, K.; Jiang, R.; Wang, P.; Zhao, Q. Screening of DNA aptamers against myoglobin using a positive and negative selection units integrated microfluidic chip and its biosensing application. Anal. Chem. 2014, 86, 6572–6579. [Google Scholar] [CrossRef]
- Sharma, A.; Jang, J. Flexible electrical aptasensor using dielectrophoretic assembly of graphene oxide and its subsequent reduction for cardiac biomarker detection. Sci Rep. 2019, 9, 5970. [Google Scholar] [CrossRef]
- Lai, X.H.; Liang, R.L.; Liu, T.C.; Dong, Z.N.; Wu, Y.S.; Li, L.H. A fluorescence immunochromatographic assay using europium (III) chelate microparticles for rapid, quantitative and sensitive detection of creatine kinase MB. J. Fluoresc. 2016, 26, 987–996. [Google Scholar] [CrossRef]
- Kakoti, A.; Goswami, P. Multifaceted analyses of the interactions between human heart type fatty acid binding protein and its specific aptamers. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 3289–3299. [Google Scholar] [CrossRef]
- Yang, X.; Wang, Y.; Wang, K.; Wang, Q.; Wang, P.; Lin, M.; Chen, N.; Tan, Y. DNA aptamer-based surface plasmon resonance sensing of human C-reactive protein. RSC Adv. 2014, 4, 30934–30937. [Google Scholar] [CrossRef]
- Wu, B.; Jiang, R.; Wang, Q.; Huang, J.; Yang, X.; Wang, K.; Li, W.; Chen, N.; Li, Q. Detection of C-reactive protein using nanoparticle-enhanced surface plasmon resonance using an aptamer-antibody sandwich assay. Chem. Commun. 2016, 52, 3568–3571. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, J.; Chen, Y.; Xue, F.; Teng, J.; Cao, J.; Lu, C.; Chen, W. Magnetic microparticle-based SELEX process for the identification of highly specific aptamers of heart marker--brain natriuretic peptide. Microchim. Acta 2015, 182, 331–339. [Google Scholar] [CrossRef]
- Huang, R.H.; Fremont, D.H.; Diener, J.L.; Schaub, R.G.; Sadler, J.E. A Structural Explanation for the Antithrombotic Activity of ARC1172, a DNA Aptamer that Binds von Willebrand Factor Domain A1. Structure 2009, 17, 1476–1484. [Google Scholar] [CrossRef]
- Liu, M.; Zaman, K.; Fortenberry, Y.M. Overview of the therapeutic potential of aptamers targeting coagulation factors. Int. J. Mol. Sci. 2021, 22, 3897. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wang, K.; Zhao, M.; Yang, X.; Chen, M.; Lan, X. Development of aptamer oligonucleotides as anticoagulants and antithrombotics for cardiovascular diseases: Current status. Thromb. Res. 2014, 134, 769–773. [Google Scholar] [CrossRef]
- Mittal, R.; Jhaveri, V.M.; McMurry, H.S.; Kay, S.I.S.; Sutherland, K.J.; Nicole, L.; Mittal, J.; Jayant, R.D. Recent treatment modalities for cardiovascular diseases with a focus on stem cells, aptamers, exosomes and nanomedicine. Artif. CellsNanomed. Biotechnol. 2018, 46, 831–840. [Google Scholar] [CrossRef]
- Diener, J.L.; Daniel Lagassé, H.A.; Duerschmied, D.; Merhi, Y.; Tanguay, J.F.; Hutabarat, R.; Gilbert, J.; Wagner, D.D.; Schaub, R. Inhibition of von Willebrand factor-mediated platelet activation and thrombosis by the anti-von Willebrand factor A1-domain aptamer ARC1779. J. Thromb. Haemost. 2009, 7, 1155–1162. [Google Scholar]
- Sakai, K.; Someya, T.; Harada, K.; Yagi, H.; Matsui, T.; Matsumoto, M. Novel aptamer to Von Willebrand factor A1 domain (TAGX-0004) shows total inhibition of thrombus formation superior to ARC1779 and comparable to caplacizumab. Haematologica 2020, 105, 2631–2638. [Google Scholar] [CrossRef]
- Siller-Matula, J.M.; Merhi, Y.; Tanguay, J.F.; Duerschmied, D.; Wagner, D.D.; McGinness, K.E.; Pendergrast, P.S.; Chung, J.-K.; Tian, X.; Schaub, R.G.; et al. ARC15105 is a potent antagonist of von Willebrand factor mediated platelet activation and adhesion. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 902–909. [Google Scholar] [CrossRef]
- Zhu, S.; Gilbert, J.C.; Liang, Z.; Kang, D.; Li, M.; Tarantino, P.M.; Jilma, B. Potent and rapid reversal of the von Willebrand factor inhibitor aptamer BT200. J. Thromb. Haemost. 2020, 18, 1695–1704. [Google Scholar] [CrossRef]
- Kovacevic, K.D.; Greisenegger, S.; Langer, A.; Gelbenegger, G.; Buchtele, N.; Pabinger, I.; Petroczi, K.; Zhu, S.; Gilbert, J.C.; Jilma, B. The aptamer BT200 blocks von Willebrand factor and platelet function in blood of stroke patients. Sci. Rep. 2021, 11, 3092. [Google Scholar] [CrossRef]
- Nimjee, S.M.; Dornbos, D.; Pitoc, G.A.; Wheeler, D.G.; Layzer, J.M.; Venetos, N.; Huttinger, A.; Talentino, S.E.; Musgrave, N.J.; Moody, H.; et al. Preclinical Development of a vWF Aptamer to Limit Thrombosis and Engender Arterial Recanalization of Occluded Vessels. Mol. Ther. 2019, 27, 1228–1241. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Hirsh, J.; Spencer, F.A.; Baglin, T.P.; Weitz, J.I. Antiplatelet drugs—Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012, 141, e89S–e119S. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ma, Y.; Xie, Y.; Pu, J. Aptamer-based applications for cardiovascular disease. Front. Bioeng. Biotechnol. 2022, 10, 1002285. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Rossi, J.; Biology, C.; Rd, E.D. Aptamers as targeted therapeutics: Current potential and challenges. Nat. Rev. Drug Discov. 2017, 8, 181–202. [Google Scholar] [CrossRef] [PubMed]
- Sattari, R.; Palizban, A.; Khanahmad, H. Single-Strand DNA-Like Oligonucleotide Aptamer Against Proprotein Convertase Subtilisin/Kexin 9 Using CE-SELEX: PCSK9 Targeting Selection. Cardiovasc. Drugs Ther. 2020, 34, 475–485. [Google Scholar] [CrossRef]
- Yu, H.; Frederiksen, J.; Sullenger, B.A. Applications and future of aptamers that achieve rapid-onset anticoagulation. RNA 2023, 29, 455–462. [Google Scholar] [CrossRef]
- Ni, X.; Castanares, M.; Mukherjee, A.; Lupold, S.E. Nucleic Acid Aptamers: Clinical Applications and Promising New Horizons. Curr. Med. Chem. 2011, 18, 4206–4214. [Google Scholar] [CrossRef]
- Riccardi, C.; Meyer, A.; Vasseur, J.J.; Cavasso, D.; Krauss, I.R.; Paduano, L.; Morvan, F.; Montesarchio, D. Design, synthesis and characterization of cyclic nu172 analogues: A biophysical and biological insight. Int. J. Mol. Sci. 2020, 21, 3860. [Google Scholar] [CrossRef]
- Pasternak, A.; Hernandez, F.J.; Rasmussen, L.M.; Vester, B.; Wengel, J. Improved thrombin binding aptamer by incorporation of a single unlocked nucleic acid monomer. Nucleic Acids Res. 2011, 39, 1155–1164. [Google Scholar] [CrossRef]
- Palta, S.; Saroa, R.; Palta, A. Overview of the coagulation system. Indian. J. Anaesth. 2014, 58, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Burnett, J.C.; Rossi, J.J. RNA-based therapeutics: Current progress and future prospects. Chem. Biol. 2012, 19, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Schneider, P.N.; Olthoff, J.T.; Matthews, A.J.; Houston, D.W. Use of fully modified 2′-O-methyl antisense oligos for loss-of-function studies in vertebrate embryos. Genesis 2012, 49, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Hahn, U.; Rentmeister, A. Cell-specific aptamers as emerging therapeutics. J. Nucleic Acids 2011, 2011, 904750. [Google Scholar] [CrossRef] [PubMed]
- Mi, J.; Zhang, X.; Giangrande, P.H.; McNamara, J.O.; Nimjee, S.M.; Sarraf-Yazdi, S.; Sullenger, B.A.; Clary, B.M. Targeted inhibition of αvβ3 integrin with an RNA aptamer impairs endothelial cell growth and survival. Biochem. Biophys. Res. Commun. 2005, 338, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Kara, N.; Ayoub, N.; Ilgu, H.; Fotiadis, D.; Ilgu, M. Aptamers Targeting Membrane Proteins for Sensor and Diagnostic Applications. Molecules 2023, 28, 3728. [Google Scholar] [CrossRef]
- Vater, A.; Klussmann, S. Turning mirror-image oligonucleotides into drugs: The evolution of Spiegelmer® therapeutics. Drug Discov. Today 2015, 20, 147–155. [Google Scholar] [CrossRef]
- Torrado, J.; Buckley, L.; Durán, A.; Trujillo, P.; Toldo, S.; Valle Raleigh, J.; Abbate, A.; Biondi-Zoccai, G.; Guzmán, L.A. Restenosis, Stent Thrombosis, and Bleeding Complications: Navigating Between Scylla and Charybdis. J. Am. Coll. Cardiol. 2018, 71, 1676–1695. [Google Scholar] [CrossRef]
- Fathi-Karkan, S.; Mirinejad, S.; Ulucan-Karnak, F.; Mukhtar, M.; Ghahramani Almanghadim, H.; Sargazi, S.; Rahdar, A.; Díez-Pascual, A.M. Biomedical applications of aptamer-modified chitosan nanomaterials: An updated review. Int. J. Biol. Macromol. 2023, 238, 124103. [Google Scholar] [CrossRef]
Figure 1.
Nanotheranostic application for the treatment of CVDs.

Figure 2.
Aptamer as ssRNA/ssDNA targeting mechanism.

Figure 3.
Aptamer nanoconjugates as effective thernaostic therapy in the treatment of cardiovascular diseases.
Figure 3.
Aptamer nanoconjugates as effective thernaostic therapy in the treatment of cardiovascular diseases.


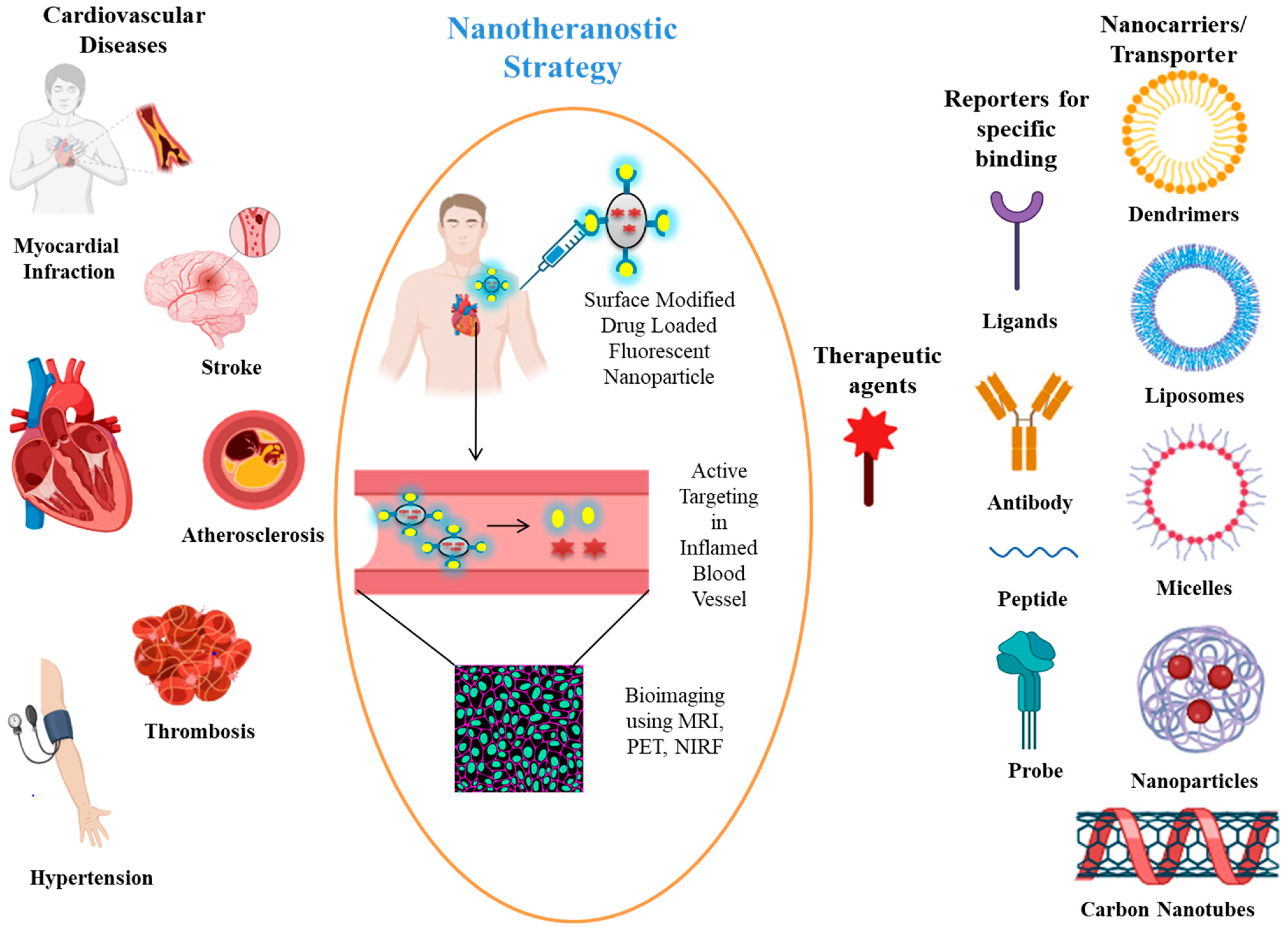{kind=link}
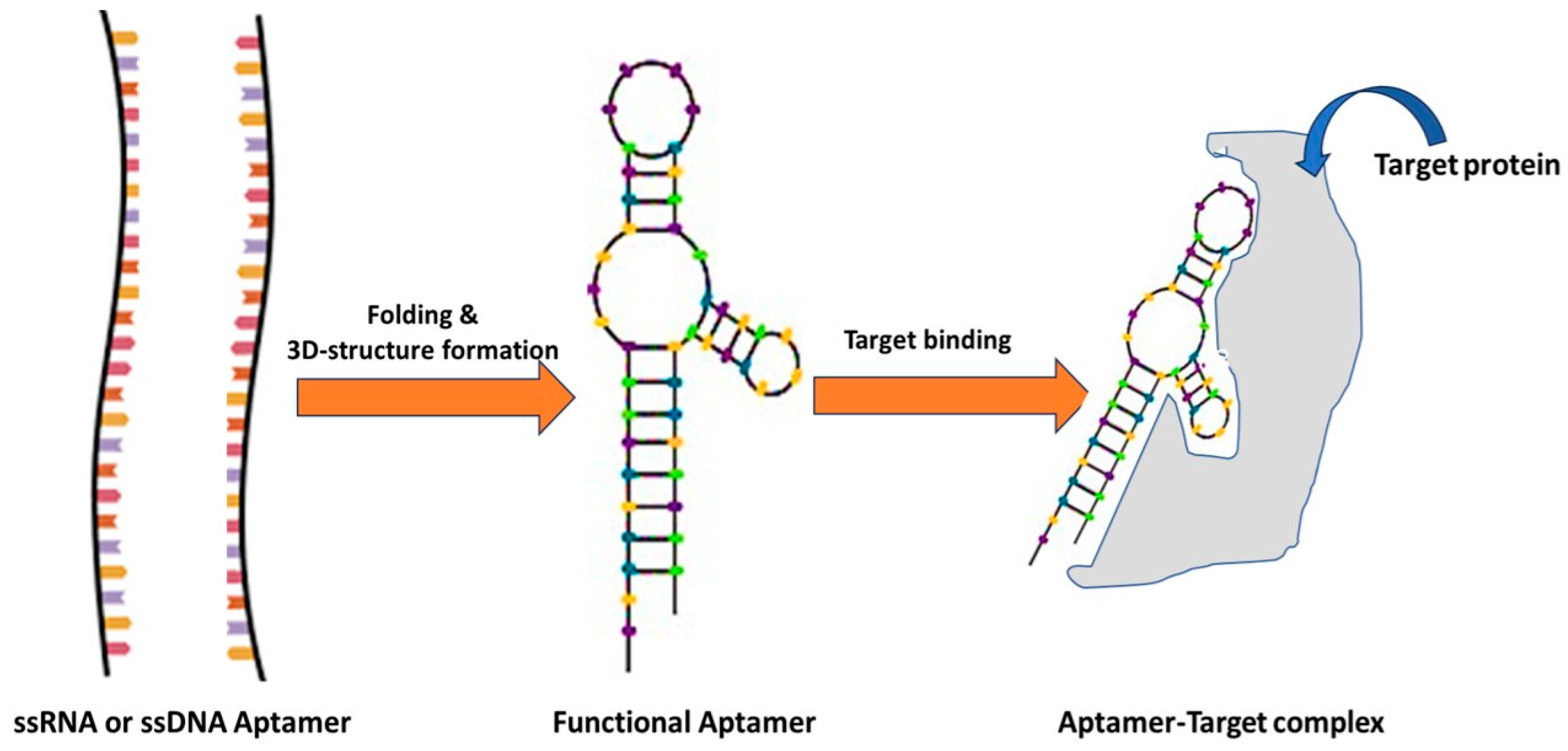{kind=link}
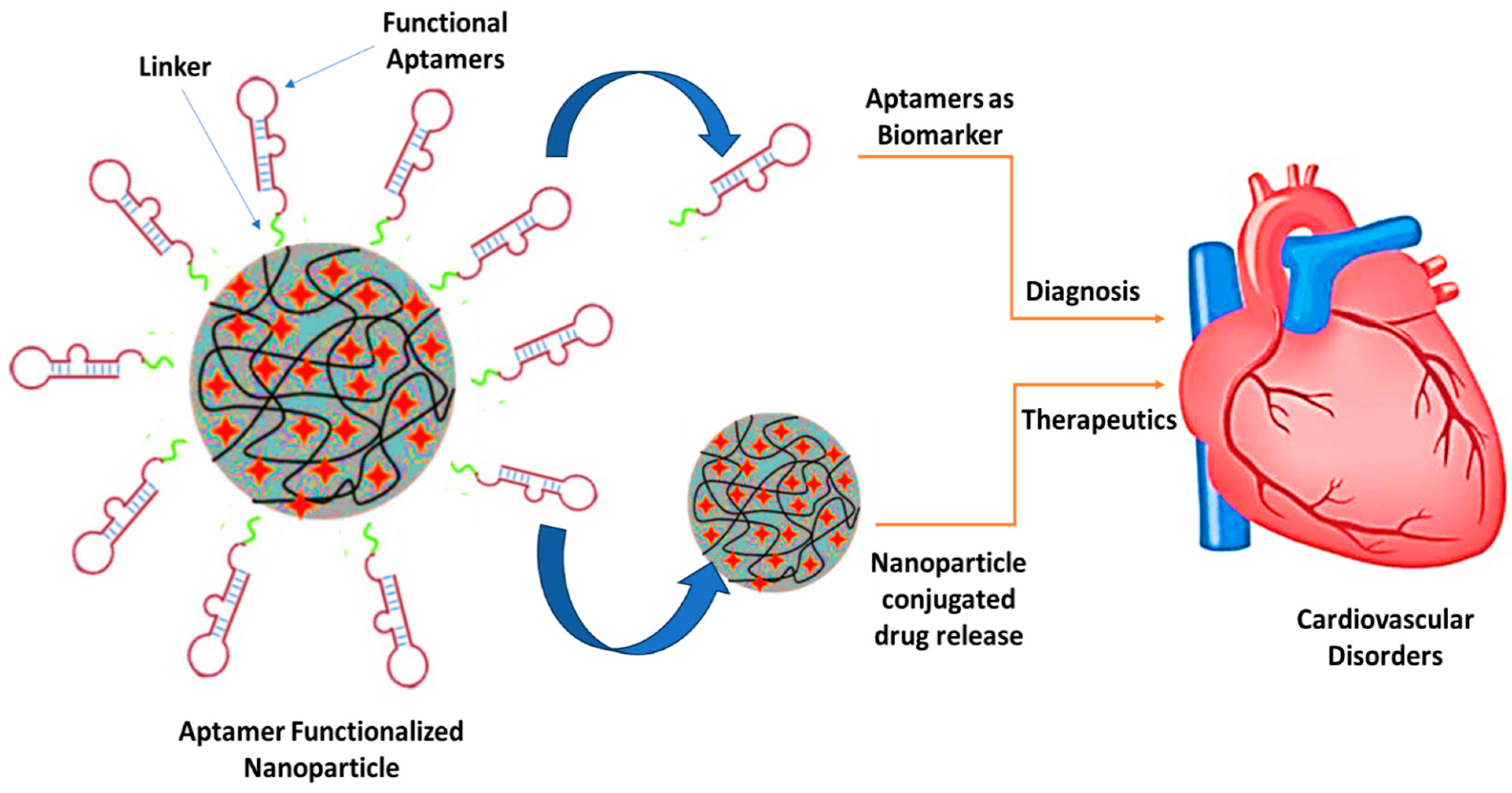{kind=link}
Table 1.
Nanotheranostic developed as diagnostic and therapeutic for cardiovascular diseases.
| Carrier | Bioimaging Mode | Therapeutic Agent | Target | Disease | References |
|---|---|---|---|---|---|
| Mesoporous silica-coated conversion nanoparticles | NIR fluorescence | Chlorin e6 (Photosensitiser) | THP-1 Macrophage apoptosis | Atherosclerosis | [29] |
| Nanoparticles | NIR fluorescence | Cathepsin-B activated (L-SR15) | Cathepsin-B plaque destabilizing by eliminating macrophage | Atheroma | [27] |
| Single-walled carbon nanotubes | NIR fluorescence | Carbon nanotube | Macrophage-rich atherosclerotic lesions | Atherosclerosis | [28] |
| Gold nanorods | Micro-computed tomography (CT) imaging | Gold nanorods | Inflammatory macrophage | Atherosclerosis | [30] |
| Magnetic nanostructure | MRI | High-density lipoprotein | Cholesterol-rich macrophage | Atherosclerotic vascular lesions | [31] |
| Solid lipid NPs | MRI | α-tocopherol or prostacyclin PGI2 | Platelet activation and aggregation | Atherosclerosis | [32] |
| Iron NPs | Micro-CT, PET, MRI | Mitochondria loaded with 18F-R6G | Mitochondria | Ischemic heart disease | [32] |
| Nanoparticles | MRI, NIRF | Rapamycin | Ischemic Lesions | Acute ischemic stroke | [33] |
| BiomemticNanobubbles | NIRF | Platelets | Platelet aggreagation | Acute ischemic stroke | [34] |
| Magnetic iron oxide nanocubes | MRI | Poly(lactide)-polycarboxybetaine coated iron oxide nanocubes | Phosphatidylserine receptor | Myocardial infarction | [34] |
| Silver oxide NPs | MRI, NIRF | Silver oxide NPs | Activated platelets | Thrombosis | [34] |
| GK coated macroporus silica-Bi core shell NPs | CT | Urokinase | Enriched thrombus | Thrombotic disease | [35] |
Table 2.
Aptamers Nano conjugates in the diagnosis of cardiovascular diseases.
| Biomarker | Aptamer | Disease Diagnosis | Binding Affinity(KD) | Method for Affinity | Reference |
|---|---|---|---|---|---|
| cTnT | TnIApt23 | Acute coronary syndrome (ACS), AMI, acute chest pain | 2.7 nM | Fluorescence | [75] |
| TnIApt19 | 6.3 nM | Fluorescence | [75] | ||
| TnIApt18 | 9 nM | Fluorescence | [75] | ||
| TnIApt11 | 10.25 nM | Fluorescence | [75] | ||
| Troponin | TnApt.1 | Acute myocardial infarction | 61.51 nM | Bioluminescence | [76] |
| TnApt.2 | 42.01 nM | Bioluminescence | [76] | ||
| TnApt.4 | 167.1 nM | Bioluminescence | [76] | ||
| TnApt.5 | 255.7 nM | Bioluminescence | [76] | ||
| TnApt.10 | 121.4 nM | Bioluminescence | [76] | ||
| TnApt.12 | 24.16 nM | Bioluminescence | [76] | ||
| TnApt.14 | 79.04 nM | Bioluminescence | [76] | ||
| TnAp2t1 | 39.06 nM | Bioluminescence | [76] | ||
| TnAp2t2 | 24.93 nM | Bioluminescence | [76] | ||
| TnAp2t3 | 80.6 nM | Bioluminescence | [76] | ||
| cTnI | Apt.1 | Acute coronary syndromes, venous thrombosis | 122 nM | SPR | [77] |
| Apt.2 | 190 nM | SPR | [77] | ||
| AraHH001 | 43 nM | Flowcytometry | [78] | ||
| Myoglobin | Myo40-7-27 | Acute myocardial infarction | 4.93 nM | SPR | [79] |
| Myo40-7-69 | 6.38 nM | SPR | [79] | ||
| Myo40-7-34 | 5.58 nM | SPR | [79] | ||
| Mb 089 | 65 pM | SPR | [80] | ||
| Creatine Kinase | C.Apt.21 | Chronic heart failure, hypertension | 255.7 nM | Bioluminescence | [81] |
| C.Apt.30 | 121.4 nM | Bioluminescence | [81] | ||
| HFABP | N13 | Heart failure, myocardial infarction | 24.16 nM | Bioluminescence | [82] |
| N53 | 79.04 nM | Bioluminescence | [82] | ||
| C-Reactive Protein | CRP-80-17 | Atherothrombotic, cardiac death, ischemic stroke, myocardial infarction | 3.9 nM | Bioluminescence | [83] |
| CRP-40-17 | 16.2 nM | Bioluminescence | [83] | ||
| CRP-62-40 | 16.2 nM | Bioluminescence | [84] | ||
| BNP | A10 | von Willebrand disease, atherosclerosis, stroke, arterial thrombosis | 12 nM | Fluorescence | [85] |
| A8 | 139.4 nM | Fluorescence | [85] | ||
| A11 | 28 nM | Fluorescence | [85] | ||
| A14-1 | 22.4 nM | Fluorescence | [85] | ||
| A14-5 | 104.6 nM | Fluorescence | [85] |
cTnI—cardiac troponin I; cTnT—cardiac troponin T; BNP—B-type natriuretic peptide; CRP—C-reactive protein.
Table 3.
Current status of aptamers in cardiovascular diseases.
| Drug | Composition | Target | Condition | Current Phase | Reference |
|---|---|---|---|---|---|
| ARC1779 | DNA and 2′-O-methyl, coupled to a 20 kDa PEG, 3′ inverted dT | Willebrand factor (vWF) | Carotid artery disease and thrombotic microangiopathies | Phase II | [91,92] |
| ARC1172 | Biotin-41-mer DNA aptamer complex | Willebrand factor (vWF) | Vascular injury | Phase I | [86] |
| ARC183 | 15-nucleotide single-stranded DNA aptamer without modifications | Thrombin | Coronary artery disease and cardiac surgery | Phase I | [108] |
| REG1 | 2′-O-methyl antidote in addition to 2′-ribo purine/2′-fluoro pyrimidine (RB006)/40 kDa PEG | Coagulation factor IXa | Percutaneous coronary interventions | Phase I, IIa, and IIb | [105] |
| NU172 | Unmodified-DNA aptamer | Thrombin or coagulation factor II | Cardiopulmonary bypass | Phase II | [101,102] |
| Rondoraptivon pegol (BT 200) | PEGylated RNA aptamer | von Willebrand factor | Arterial thrombosis, atherosclerosis, stroke, hemophilia A, and von Willebrand disease | Phase II, Phase I, and Preclinical | [94,95] |
| Anivamersenpegnivacogin | RNA aptamer made of 31 nucleotides and PEGylated | Factor IXa | Vascular thrombosis and acute coronary syndromes | Phase I | [98] |
| Egaptivon pegol | RNA aptamer linked with polyethylene glycol | von Willebrand factor | Thrombosis, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, and von Willebrand disease | Phase I | [109] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ramchandani, M.; Kumari, P.; Goyal, A.K. Aptamers as Theranostics in Cardiovascular Diseases. J. Nanotheranostics 2023, 4, 408-428. https://doi.org/10.3390/jnt4030018
AMA Style
Ramchandani M, Kumari P, Goyal AK. Aptamers as Theranostics in Cardiovascular Diseases. Journal of Nanotheranostics. 2023; 4(3):408-428. https://doi.org/10.3390/jnt4030018
Chicago/Turabian StyleRamchandani, Manish, Priyanka Kumari, and Amit K. Goyal. 2023. "Aptamers as Theranostics in Cardiovascular Diseases" Journal of Nanotheranostics 4, no. 3: 408-428. https://doi.org/10.3390/jnt4030018