
COVID-19 Vaccine Acceptance and Hesitancy among Teachers and Students: A Scoping Review of Prevalence and Risk Factors


1
Department of Health, Physical Education and Recreation, University of Cape Coast, Cape Coast CC 3321, Ghana
2
Neurocognition and Action-Biomechanics-Research Group, Faculty of Psychology and Sports Science, Bielefeld University, Postfach 10 01 31, 33501 Bielefeld, Germany
*
Author to whom correspondence should be addressed.
COVID 2024, 4(4), 557-570; https://doi.org/10.3390/covid4040037
Submission received: 7 February 2024
/
Revised: 12 April 2024
/
Accepted: 15 April 2024
/
Published: 19 April 2024
Abstract
:Students’ and teachers’ acceptance of the COVID-19 vaccination may help boost the uptake of the vaccines in the general population because teachers and students serve as a source of information and campaign mechanisation for vaccination. This review aimed to map evidence on the prevalence and predictors of COVID-19 vaccine acceptance and hesitancy among teachers and students. After removing duplicates, a search in several databases (Dimensions, PubMed Central, JSTOR, Google Scholar, Google, the WHO Library, and HINARI) produced 2060 records. Through screening based on the inclusion criteria, 27 records were used for this review. A relatively high prevalence of vaccine hesitancy was found among teachers and students. Teachers and students in countries such as China, Egypt, the USA, and India however, reported relatively low levels of COVID-19 vaccine acceptance. Vaccine hesitancy depends on perceived adverse effects, safety, efficacy, and benefits among teachers and students, with male teachers and male students being more likely to accept the COVID-19 vaccine than their female counterparts. Moreover, we found that vaccine acceptance could result from trust in the healthcare system and pharmaceutical companies, sources of COVID-19 information, and trust in healthcare providers. Public health experts, academics, other scientists, and health practitioners are required to take a more distinctive, multidisciplinary, and structured approach that focused on communicating effective evidence-based information to combat misinformation concerning COVID-19 vaccines.
1. Introduction
Three years have passed since the coronavirus disease 2019 (COVID-19) pandemic surprised the world. So far, 775,132,086 COVID-19 cases, including 7,042,222 COVID-19 deaths, have been confirmed globally by the World Health Organisation (WHO) as of 24 March 2024 [1]. Several remedies, including vaccination against COVID-19, were widely recommended. Consequently, about 13.59 billion vaccines have been administered globally [1]. Globally, there are about 63% and 28% coverage rates of full primary and booster vaccination, respectively. However, the recurrent and continuous outbreak of waves has shown that it would be practically impossible to stop the COVID-19 pandemic by gaining herd immunity [2]. Meanwhile, the protective effect of vaccinations is to prevent COVID-19-related complications and mortality rather than preventing the spread of the virus [3]. Thus, COVID-19, like the influenza virus, will co-exist with humans for a long time, especially with the emergence of new variants [1]. Hence, until vaccines that stop the spread of COVID-19 are developed and made available globally, complete vaccination and boosters remain vital to prevent COVID-19-related complications, hospitalisation, and mortality [4,5].
The argument is that the public acceptance of the COVID-19 vaccination safeguards public health and eases the burden on the healthcare system, particularly in resource-limited environments. However, the unwillingness to receive the COVID-19 vaccine is a widespread problem [1,6,7]. It is considered one of the top ten global public health concerns, although vaccination has been one of the most significant initiatives in the field of public health in the 21st century [6]. The term “vaccine hesitancy”, according to Coustasse et al. [7], describes the hesitation or unwillingness to receive a vaccination against an infectious disease even when the safety and efficacy of the vaccine have been confirmed and proven. Vaccine uptake greatly depends on trust [7], which is related to personal beliefs, motivation, perceived risk of exposure, knowledge, and vaccination awareness [8]. Evidence shows that a safe and efficacious vaccine has widespread acceptability [9], whereas a vaccine with low efficacy and safety issues may have a low acceptance rate [9,10]. According to a recent systematic review and meta-analysis, the acceptance rate of the COVID-19 vaccination was only 61% [10]. These findings show that people are showing hesitation toward COVID-19 vaccination.
To boost public confidence in COVID-19 vaccines and to encourage the acceptance it is important to identify and resolve knowledge gaps and myths about these vaccines, especially among critical populations such as teachers and students that serve as a knowledge source for most people in society [11]. Schools are privileged operational environments that disseminate health information and educational messages [11]. Schools’ health education programmes, a medium for health communication, can accurately transmit health and medical knowledge among young people and society. Teachers and students may also influence how communities and families decide whether to vaccinate their children against vaccine-preventable infections. Yet, there are a lot of variations in teachers’ and students’ intentions to receive or accept the COVID-19 vaccine in various countries [12,13,14,15,16]. To close the gap and encourage the uptake of vaccines in such a crucial population, it may be important to map the evidence to understand the prevalence of COVID-19 vaccine acceptance and hesitancy and explore the protective and risk factors of COVID-19 vaccine acceptance and hesitancy among students and teachers.
2. Methods
Study Design, Data Source, and Search Strategy
This scoping review was conducted following the recommendations of Arksey and O’Malley [17], i.e., (1) identifying the objectives or research questions, (2) identifying relevant studies, (3) selecting the studies, (4) collecting data, (5) data summary and synthesis of the results, and (6) consultation. This review was guided by two research questions: (1) What is the prevalence of COVID-19 vaccine acceptance and hesitancy among teachers and students? (2) What are the protective and risk factors of COVID-19 vaccine acceptance and hesitancy among teachers and students?
Several meta databases, like Dimensions, JSTOR, and PubMed Central, were searched for peer-reviewed articles. First, Medical Subject Headings (MeSH) words were used for the PubMed search. These terms were then modified for the search conducted in the other databases. Table 1 presents the search approach, exclusion and inclusion criteria. Further searches for peer-reviewed articles were conducted in Google Scholar, Google, the WHO Library, and HINARI. The last search was conducted on 27 March 2024. The authors carefully examined the records they had obtained, and duplicates were merged using the Mendeley v1.19.8 software. Twelve graduate students were trained and supervised to screen tittles and abstracts for full-text eligible papers using the eligibility criteria. The reference lists of these full-text eligible records were further checked for additional eligible full-text records. MA and JOS independently screen full-text eligible records using the eligibility criteria presented in Table 1.
The characteristics of the peer-reviewed papers extracted during the data charting process included the authors, year of the publication, country where the study was conducted, study design, population, sample size, prevalence, risk and protective factors of vaccine acceptance/hesitancy. The data were extracted independently by MA and JOS and reviewed by EWA and JEH. This process was conducted to improve the reliability and accuracy of the data extracted. Table 2 presents the details of the extracted data from the reviewed studies. In addition, experts were consulted on the search (chartered librarians) and review process to ensure the accuracy and depth of the data for this scoping review. Consequently, a thematic analysis of the extracted data and synthesis was conducted, and the findings are presented below.
3. Results
3.1. Search Results
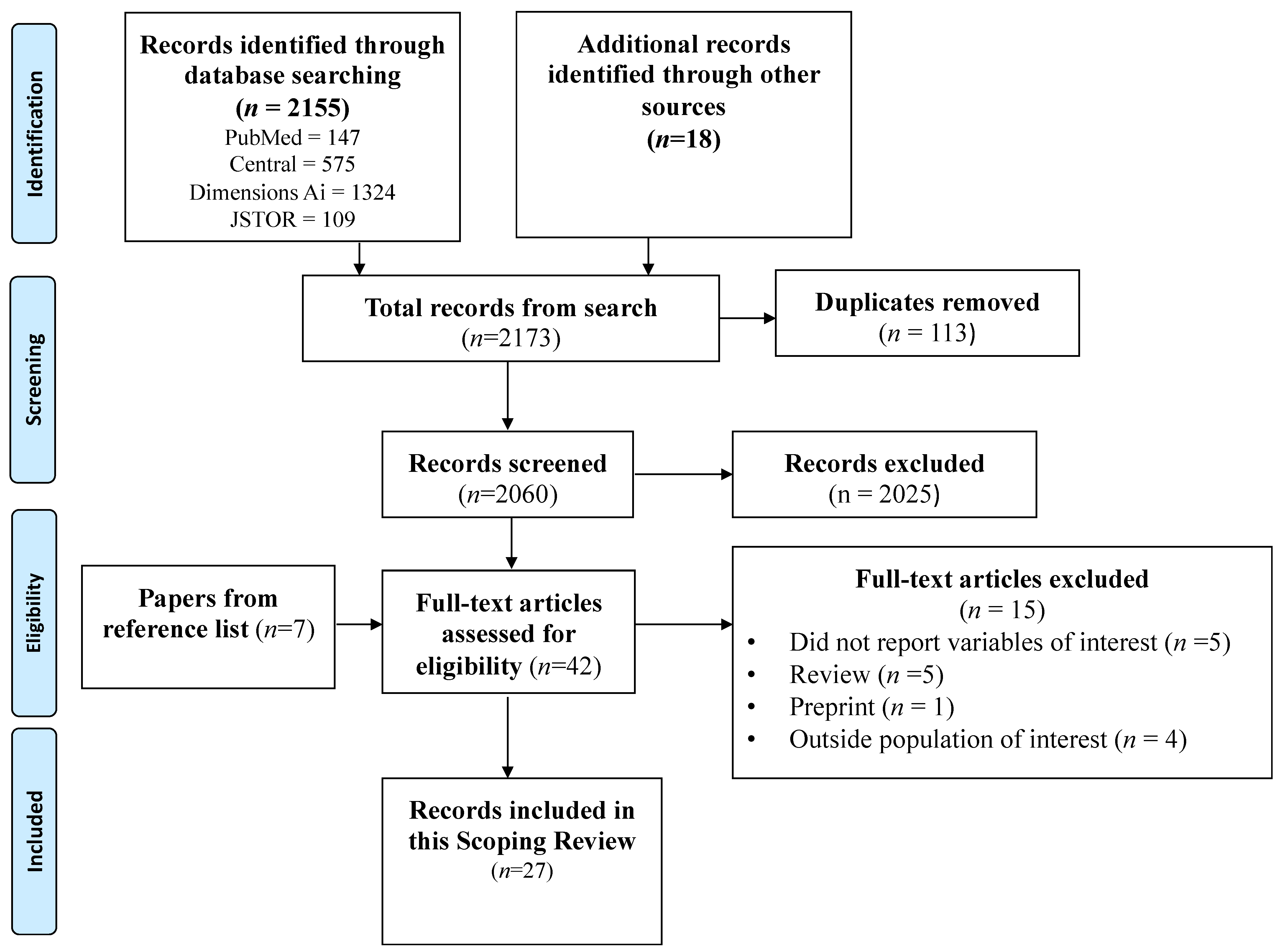
The search in the four meta-databases databases (PubMed, Central, JSTOR, and Dimensions) produced 2155 records. An additional search in Google Scholar and Google produced an extra 18 records. Thus, 2173 records were produced from the search conducted. A total of 113 duplicates were merged in the Mendeley tool. Also, 2025 records were not relevant to this review and were removed. We further scrutinised 35 full-text records using the eligibility criteria. Moreover, 7 records were additionally identified by checking the reference lists of the selected full-text records, resulting in 42 records. Finally, out of the 42 records, 15 were excluded. Thus, 27 full-text articles were included in the thematic synthesis for this review (see details in Figure 1).
3.2. Characteristics of the Reviewed Studies
All the reviewed studies adopted the cross-sectional survey design. Moreover, all 27 articles were conducted in only 19 countries across the globe(see details in Figure 2). In addition, 13 of the reviewed studies reported on both vaccine acceptance and hesitancy. Furthermore, two studies [15,18] sampled both teachers and students, whereas 10 and 15 studies sampled only teachers and students, respectively (see details in Table 2). However, 17 of the reviewed studies reported COVID-19 vaccine hesitancy (see Table 3), whereas 23 reported acceptance.
3.3. Prevalence of COVID-19 Vaccine Hesitancy
Generally, the prevalence of COVID-19 vaccine hesitancy reported by the reviewed studies included 4.7% in China [27] and 54.4% in Egypt [25]. COVID-19 vaccine hesitancy among teachers was between 10% among preschool and college teachers in Portugal [23] and 54.4% among college teachers in Egypt [25]. Among students, COVID-19 vaccine hesitancy was between 4.7% among nursing students in China [27] and 46% among medical students in Egypt [16]. The highest hesitancy among teachers (54.4%) and students (46%) were all from Africa [16,25]. Studies conducted in Europe produced hesitancy below 20%, except in Slovenia, where students reported a hesitancy prevalence of 29.2% [24]. In Asia, China (42.2%) [20] and India (36.2%) [31] recorded relatively higher rates of COVID-19 vaccine hesitancy. In two studies from the United States, all medical students reported 23% [19] and 34.9% [19] prevalence of COVID-19 vaccine hesitancy. Teachers recorded a higher prevalence than students across various geographical areas. Details of the prevalence of vaccine hesitancy are presented in Table 3.

{kind=link}
{kind=link}
Table 3.
COVID-19 vaccine hesitancy prevalence among the reviewed studies.
| Authors | Country | Population | Hesitancy (%) |
|---|---|---|---|
| Zhou et al. [27] | China | Nursing students | 4.7 |
| Chen et al. [15] | China | College students | 23.8 |
| Chen et al. [15] | China | College teachers | 31.8 |
| Xu et al. [20] | China | College teachers | 42.2 |
| Riad et al. [34] | Czech Republic | College students | 7.4 |
| Saied et al. [16] | Egypt | Medical students | 46 |
| Sharaf et al. [25] | Egypt | College teachers | 54.4 |
| Tavolacci et al. [30] | France | College students | 17 |
| Scharff et al. [32] | Germany | Secondary school students | 7 |
| Jain et al. [31] | India | College students | 36.2 |
| Hamdan et al. [36] | Lebanon | College teachers | 10 |
| Montvidas et al. [33] | Lithuania | Health science students | 10 |
| Estrela et al. [23] | Portugal | Preschool to higher education teachers | 10 |
| Šorgo et al. [24] | Slovenia | Post-secondary school students | 29.2 |
| Lucia et al. [28] | USA | Medical students | 23 |
| Kelekar et al. [19] | USA | Dental and medical students | 34.9 |
| Khuc et al. [35] | Vietnam | College students | 16.6 |
3.4. Prevalence of COVID-19 Vaccine Acceptance
Studies on COVID-19 vaccine acceptance intentions found a prevalence between 6% [16] among medical students in Egypt and 92% [38] among public school teachers in Canada. In Africa, all studies reported COVID-19 vaccine acceptance rate above 40% [14,25,26,29], except that by Saied et al. [16], which reported 6% among medical students in Egypt. In Asia, all studies, which were conducted on students, reported COVID-19 vaccine acceptance above 50%, with 51.9% in China [27], 63.8% in India [31], 72.5% in Pakistan [39], 83.4% in Vietnam [35], and 87% in Lebanon [36]. Moreover, students in Asia were more likely to accept the vaccine than those from Africa. Only students in Italy [37] and teachers in Canada [38] recorded COVID-19 vaccine acceptance above 90%. See Table 4 for summary details.
3.5. Risk Factors for COVID-19 Vaccine Hesitancy among Teachers and Students
The evidence shows that female teachers [25] and female students [30] were more likely to refuse COVID-19 vaccines. Also, lower education status predicted COVID-19 vaccine hesitancy [32]. Furthermore, teachers with no intentions of travelling internationally were more hesitant to vaccinate against COVID-19-related complications [25]. In China, it was reported that students and teachers suffering from chronic diseases or with a history of chronic illness were more hesitant to accept the COVID-19 vaccine. Moreover, university students in Lebanon who refused the flu vaccine were more likely to reject the COVID-19 vaccine as well, despite the availability of the vaccine [36]. In addition, the perceived high risk of side effects [16,18,35], low safety [15,23,27,30], and low efficacy [16,23,30] of the COVID-19 vaccine were predictors of hesitancy among teachers and students. Hence, insufficient or lack of data regarding the side effects of the COVID-19 vaccine fueled hesitancy among teachers and students [16,27,35]. Meanwhile, agreeing to COVID-19 vaccine-related conspiracy also accounted for the refusal of the COVID-19 vaccine among college students in Lebanon [36].
3.6. Predictors of COVID-19 Vaccine Acceptance among Teachers and Students
Being a male [13,14,21], knowing a family member who has received the COVID-19 vaccine [22], and having a high income [21] and attaining graduate-level education [21,29,39] were associated with the willingness and intentions to accept the COVID-19 vaccine. Also, medical students [33] and student healthcare workers [22], especially students who volunteered to work in COVID-19 wards [33], were more likely to accept COVID-19 vaccines. Furthermore, teachers and students with high perceived susceptibility to COVID-19 [12,13,14,23,24,27,29] and benefits [14,29], efficacy [23], and few side effects [26,27,28,36] of the COVID-19 vaccine were more likely to accept the vaccine. In addition, teachers and students who trusted the health system [31,34], the pharmaceutical industry [34], COVID-19 information sources [13,23], and domestic vaccines [31] were willing to accept the COVID-19 vaccine. Meanwhile, teachers and students with high level of knowledge of COVID-19 [13,30,34,37] and those with adequate information on the COVID-19 vaccine [26] were more likely to be vaccinated against COVID-19-related diseases and complications. Finally, teachers and students who received seasonal flu vaccines [12,22,37] and hepatitis B vaccine [26] and believed the vaccine was mandatory [12,39] were more likely to accept the COVID-19 vaccine.
4. Discussion
Public reactions and behaviours to uptake a new vaccine and gain protection from a specific pandemic disease are the same [40]. Vaccine hesitancy and low or poor initial vaccine uptake prevalence for a particular vaccine, such as the COVID-19 vaccine, are serious threats to global health. This situation may result in complex behavioural patterns. Besides, similar factors were reported during measles outbreaks [41] and flu vaccination [42]. Although introducing and distributing a new vaccine is expensive and time-consuming, vaccine acceptability is the primary factor determining the success of vaccination campaigns as a whole [43]. Hence, understanding the rates and predictors of vaccine acceptance and hesitancy may help develop robust public health vaccination campaigns and policies to reduce vaccine hesitancy gaps affecting existing COVID-19 vaccination programmes and new vaccines that may emerge.
This scoping review reported a relatively high prevalence of COVID-19 vaccine hesitancy in Africa (Egypt). Also, low hesitancy was reported in China and some European countries [44,45]. This high refusal of the COVID-19 vaccine in Egypt may be due to the low prevalence of COVID-19 cases in the country, including fatalities in Africa compared to Asia and Europe [44,45]. Thus, a lack of trust in the health system and pharmaceutical industries in Africa and trust in conspiracy theories against the COVID-19 vaccine may account for high levels of hesitancy in Africa [34]. Inconsistent messages from various sources and health organisations may also have led to the high prevalence of vaccine hesitation among teachers and students in Egypt [46]. Also, the relatively high COVID-19 vaccine acceptance in some African countries, such as Ghana and Ethiopia, may be due to active public health systems and vaccination campaigns and the sufficiency of COVID-19 vaccine-related information [26]. Moreover, in Canada and some parts of Europe, like Italy, Lithuania, and the Czech Republic, the COVID-19 vaccine was made mandatory, and restrictions placed on unvaccinated people may have resulted in the relatively high acceptance rate reported in reviewed studies [37,38]. In addition, in these areas, teachers and students were required to take the vaccine in schools [38]. However, regardless of how COVID-19 took a toll on China, India, and the USA, COVID-19 vaccine acceptance among teachers and students was relatively low due to the negative attitudes towards vaccination and poor confidence in COVID-19 vaccine safety and efficacy [22,30,31].
Furthermore, students did not demonstrate a notable variation in their attitudes towards vaccine acceptance or hesitancy. In some cases, medical students [33] and student healthcare workers [22], particularly students who volunteered to work in COVID-19 wards [33], were more likely to accept COVID-19 vaccines. Nevertheless, COVID-19 vaccine hesitancy was reported among nursing [27] and medical students [16,28]. This observation underscores the complexity of factors influencing vaccine-related attitudes and suggests that professional training in healthcare disciplines may not inherently lead to an increase in vaccination among students [28]. Thus, factors beyond professional training may play a vital role in shaping vaccine beliefs and behaviours among students. Thus, further exploration is needed into the multifaceted influences on vaccine acceptance within educational settings.
From the synthesis of the reviewed studies, female teachers and female students were more likely to refuse COVID-19, whereas male teachers and male students were more likely to accept the vaccine. This finding may be due to males’ greater awareness and perceived susceptibility to COVID-19 risks and hesitancy to agree to COVID-19-related conspiracy theories [44,47]. Moreover, sampling bias regarding sex distribution found in reviewed studies can alter the reported rates. Thus, these characteristics should be considered for an appropriate interpretation of COVID-19 acceptance rates or when gender is being considered as a predictor of hesitancy and acceptance of the COVID-19 vaccine.
The reviewed articles reported that perceived side effects, efficacy, and safety are strong predictors of COVID-19 vaccine acceptance among teachers and students. The evidence shows that the most common influencing factors of vaccine hesitancy in early part of COVID-19 vaccination campaigns are perceived high vaccine safety and efficacy [48,49]. Furthermore, reports of side effects of previous vaccinations hamper the uptake of new vaccines [50]. Then, clear and sufficient information regarding side effects, efficacy, and safety of such vaccines would help boost teachers’ and students’ trust in COVID-19 vaccines. The trust teachers and students have in the COVID-19 vaccine is necessary to help disseminate accurate, reliable, and sufficient information on COVID-19 vaccines to families, relatives, and the general public. This is because the public relies on teachers and students, especially medical and nursing students, for high vaccine uptake intentions [22,30,31]. Thus, restoring public trust in COVID-19 vaccines may begin with providing teachers and students with enough reliable data on the vaccines’ side effects and efficacy.
Conspiracy theories targeting COVID-19 vaccines, a lack of information and trust in vaccine benefits, and a lack of trust in health systems and pharmaceutical and healthcare providers are additional key elements that may interfere with conducting successful vaccination programmes in various nations [46,51,52,53,54]. Also, unreliable and incomplete health information may fuel rumours and conspiracy theories against COVID-19 vaccinations among teachers and students [49]. The communication strategies and vaccine delivery methods targeting teachers and students during COVID-19 vaccination and any future vaccination should be transparent, accurate, frequent, and multimodal to ensure vaccine confidence among teachers and students. This is because the general public can source their information from teachers and students [49].
It is also evident that teachers and students who received flu vaccines and hepatitis B vaccines were more likely to accept COVID-19 vaccines. The perceived benefits of vaccines and high susceptibility to COVID-19 and related complications, just as in flu and hepatitis B, have drawn attention to accepting COVID-19 vaccines [53]. Moreover, teachers and students who have received previous vaccines, such as seasonal flu and hepatitis B vaccines, may have a generally positive attitude toward vaccination [52].
4.1. Limitations and Recommendations for Future Research
This review used papers sourced from several databases. However, the included studies in this scoping review were all cross-sectional surveys, whose findings are affected mainly by response bias. In addition, the results of this review might not hold after a specific amount of time because vaccine hesitation and acceptance may alter over time as vaccine efficacy and safety and adverse effects of vaccines manifest among teachers and students. Authors did not carry out quality appraisal of the included articles, which may limit the validity and reliability of our findings. A longitudinal study that accounts for confounders may help explore changes in teachers’ and students’ attitudes toward COVID-19 vaccine hesitancy and acceptance over time. It is equally important to explore how vaccination status affects long COVID status.
4.2. Policy Recommendations
Teachers and students, just like many educated people, are more worried about the possibility of contracting COVID-19, and many such individuals are more receptive to vaccination [55]. Also, teachers and students have access to various information sources, including social media, academia, personal networks, and health organisations, which are crucial for influencing vaccination in the general public [56]. Teachers and students frequently work to protect vulnerable populations and spread accurate information about vaccinations. Hence, public health systems should focus on these demographics because many teachers and students belong to communities and would be able to improve COVID-19 vaccination uptake [55]. In addition, reputable public health specialists, academics, other scientists, and health practitioners need to take more distinctive, multidisciplinary, and structured approaches that focused on communicating effective evidence-based information to combat misinformation to teachers and students. Perhaps, these are some quick ways to reduce vaccine hesitancy in this population.
5. Conclusions
A relatively high prevalence of vaccine hesitancy was identified among teachers and students. However, teachers and students in countries such as China, the USA, and India reported relatively low levels of COVID-19 vaccine acceptance. Vaccine hesitancy in some African countries, like Egypt, is also high. The high level of vaccine hesitancy may result from perceived adverse effects, challenges with safety, efficacy, and doubt about the benefits of the COVID-19 vaccine. Moreover, male teachers and male students, compared to their female counterparts, were more likely to accept the COVID-19 vaccine. Trust in the healthcare system, pharmaceutical companies, sources of COVID-19 vaccine information, and healthcare providers influence how teachers and students accept COVID-19 vaccines. Finally, clear and sufficient information about the side effects of the COVID-19 vaccine could enhance COVID-19 vaccine uptake intentions. Hence, reputable public health specialists, academics, scientists, and health practitioners should take a more distinctive, multidisciplinary, structured approach focused on communicating effective evidence-based information to these teachers and their students. The need to combat misinformation to teachers and students would be a quick way to reduce vaccine hesitancy and improve vaccine acceptance among these categories of stakeholders in education.
Author Contributions
J.O.S. and M.A. conceived and designed this study, collected and analysed the data, and wrote the initial manuscript. E.W.A. reviewed and supervised the review process. J.E.H.J. reviewed the manuscript and provided funding for publication. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. However, the authors sincerely thank Bielefeld University, Germany, for providing financial support through the Institutional Open Access Publication Fund.
Data Availability Statement
All data generated or analysed during this study are included in this published article.
Acknowledgments
We appreciate the authors for making their works available to our team. We are also grateful to all the chartered librarians at the Sam Jonah Library, University of Cape Coast, for their support. We thank the Centre for Behaviour and Wellness Advocacy, Ghana, for their professional editing services.
Conflicts of Interest
The authors declare that they have no competing interests.
Abbreviations
WHO: World Health Organisation; MeSH: Medical Subject Headings.
References
- WHO. WHO Coronavirus (COVID-19) Dashboard 2024. Available online: https://data.who.int/dashboards/covid19/cases?n=c (accessed on 11 April 2024).
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The Concept of Classical Herd Immunity May Not Apply to COVID-19. J. Infect. Dis. 2022, 226, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nat. Med. 2021, 27, 2136–2143. [Google Scholar] [CrossRef] [PubMed]
- Vilches, T.N.; Sah, P.; Moghadas, S.M.; Shoukat, A.; Fitzpatrick, M.C.; Hotez, P.J.; Schneider, E.C.; Galvani, A.P. COVID-19 hospitalizations and deaths averted under an accelerated vaccination program in northeastern and southern regions of the USA. Lancet Reg. Health Am. 2022, 6, 100147. [Google Scholar] [CrossRef] [PubMed]
- Shoukat, A.; Vilches, T.N.; Moghadas, S.M.; Sah, P.; Schneider, E.C.; Shaff, J.; Ternier, A.; Chokshi, D.A.; Galvani, A.P. Lives saved and hospitalizations averted by COVID-19 vaccination in New York City: A modeling study. Lancet Reg. Health Am. 2022, 5, 100085. [Google Scholar] [CrossRef] [PubMed]
- Omar, D.I.; Hani, B.M. Attitudes and intentions towards COVID-19 vaccines and associated factors among Egyptian adults. J. Infect. Public Health 2021, 14, 1481–1488. [Google Scholar] [CrossRef]
- Coustasse, A.D.; Kimble, C.P.; Maxik, K.M. COVID-19 and Vaccine Hesitancy. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Wagner, A.L.; Ji, J.; Huang, Z.; Zikmund-Fisher, B.J.; Boulton, M.L.; Ren, J.; Prosser, L.A. A conjoint analysis of stated vaccine preferences in Shanghai, China. Vaccine 2020, 38, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Norhayati, M.N.; Yusof, R.C.; Azman, Y.M. Systematic Review and Meta-Analysis of COVID-19 Vaccination Acceptance. Front. Med. 2022, 8, 783982. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; D’egidio, V.; Sestili, C.; Cocchiara, R.A.; Cianfanelli, S.; Di Bella, O.; Lia, L.; Dorelli, B.; Cammalleri, V.; Backhaus, I.; et al. ImmunizziAMO: A School-Based Field Trial to Teach New Generations the Importance of Vaccination through Games and to Fight Vaccine Hesitancy in Italy. Vaccines 2020, 8, 280. [Google Scholar] [CrossRef]
- Gkentzi, D.; Benetatou, E.; Karatza, A.; Kanellopoulou, A.; Fouzas, S.; Lagadinou, M.; Marangos, M.; Dimitriou, G. Attitudes of school teachers toward influenza and COVID-19 vaccine in Greece during the COVID-19 pandemic. Hum. Vaccines Immunother. 2021, 17, 3401–3407. [Google Scholar] [CrossRef] [PubMed]
- Racey, C.S.; Donken, R.; Porter, I.; Albert, A.; Bettinger, J.A.; Mark, J.; Bonifacio, L.; Dawar, M.; Gagel, M.; Kling, R.; et al. Intentions of Public School Teachers in British Columbia, Canada to Receive a COVID-19 Vaccine. Vaccine X 2021, 8, 100106. [Google Scholar] [CrossRef] [PubMed]
- Shitu, K.; Wolde, M.; Handebo, S.; Kassie, A. Correction to: Acceptance and willingness to pay for COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. Trop. Med. Health 2021, 49, 65. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, M.-X.; Lin, X.-Q.; Wu, H.; Tung, T.-H.; Zhu, J.-S. COVID-19 vaccine hesitancy between teachers and students in a college, a cross-sectional study in China. Hum. Vaccines Immunother. 2022, 18, 2082171. [Google Scholar] [CrossRef] [PubMed]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Dafogianni, C.; Mangoulia, P.; Pappa, D.; Xanthopoulou, P.; Koutelekos, I.; Zografakis-Sfakianakis, M.; Ferentinou, E.; Fountouki, A.; Drakopoulou, M.; Giga, A.; et al. COVID-19 Vaccination Intention Associated with Behaviors towards Protection and Perceptions Regarding the Pandemic. J. Pers. Med. 2022, 12, 295. [Google Scholar] [CrossRef] [PubMed]
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Shi, G.; Zheng, S.; Tung, T.-H.; Zhang, M. COVID-19 vaccine hesitancy between family decision-makers and non-decision-makers among college teachers. Ann. Med. 2023, 55, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Cahapay, M.B. To get or not to get: Examining the intentions of Philippine teachers to vaccinate against COVID-19. J. Hum. Behav. Soc. Environ. 2022, 32, 325–335. [Google Scholar] [CrossRef]
- Kecojevic, A.; Basch, C.H.; Sullivan, M.; Chen, Y.-T.; Davi, N.K. COVID-19 Vaccination and Intention to Vaccinate Among a Sample of College Students in New Jersey. J. Community Health 2021, 46, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Estrela, M.; Silva, T.M.; Roque, V.; Gomes, E.R.; Figueiras, A.; Roque, F.; Herdeiro, M.T. Unravelling the drivers behind COVID-19 vaccination hesitancy and refusal among teachers: A nationwide study. Vaccine 2022, 20, 5464–5470. [Google Scholar] [CrossRef] [PubMed]
- Šorgo, A.; Crnkovič, N.; Cesar, K.; Selak, Š.; Vrdelja, M.; Gabrovec, B. The influence of anxiety and fear of COVID-19 on vaccination hesitancy among postsecondary students. Sci. Rep. 2022, 12, 20564. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, M.; Taqa, O.; Mousa, H.; Badran, A. COVID-19 vaccine acceptance and perceptions among dental teaching staff of a governmental university in Egypt. J. Egypt. Public Health Assoc. 2022, 97, 9. [Google Scholar] [CrossRef]
- Dubik, S.D. Understanding the Facilitators and Barriers to COVID-19 Vaccine Uptake Among Teachers in the Sagnarigu Municipality of Northern Ghana: A Cross-Sectional Study. Risk Manag. Health Policy 2022, 15, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, Y.; Li, Z. Intention to get vaccinated against COVID-19 among nursing students: A cross-sectional survey. Nurse Educ. Today 2021, 107, 105152. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Handebo, S.; Wolde, M.; Shitu, K.; Kassie, A. Determinant of intention to receive COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. PLoS ONE 2021, 16, e0253499. [Google Scholar] [CrossRef] [PubMed]
- Tavolacci, M.P.; Dechelotte, P.; Ladner, J. COVID-19 vaccine acceptance, hesitancy, and resistancy among university students in France. Vaccines 2021, 9, 654. [Google Scholar] [CrossRef] [PubMed]
- Jain, L.; Vij, J.; Satapathy, P.; Chakrapani, V.; Patro, B.; Kar, S.S.; Singh, R.; Pala, S.; Sankhe, L.; Modi, B.; et al. Factors Influencing COVID-19 Vaccination Intentions Among College Students: A Cross-Sectional Study in India. Front. Public Health 2021, 9, 735902. [Google Scholar] [CrossRef] [PubMed]
- Scharff, A.Z.; Paulsen, M.; Schaefer, P.; Tanisik, F.; Sugianto, R.I.; Stanislawski, N.; Blume, H.; Schmidt, B.M.W.; Heiden, S.; Stiesch, M.; et al. Students’ age and parental level of education influence COVID-19 vaccination hesitancy. Eur. J. Pediatr. 2022, 181, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Montvidas, J.; Basevičiūtė, M.; Burokaitė, K.; Adomaitienė, V.; Lesinskienė, S. COVID-19 vaccine hesitancy and psychosocial effects of the COVID-19 pandemic among health-science students of Lithuania—A national cross-sectional online survey. Int. J. Environ. Res. Public Health 2021, 18, 12870. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Antalová, N.; Krobot, M.; Zviadadze, N.; Serdiuk, I.; Koščík, M.; Klugar, M. Prevalence and drivers of COVID-19 vaccine hesitancy among Czech university students: National cross-sectional study. Vaccines 2021, 9, 948. [Google Scholar] [CrossRef] [PubMed]
- Van Khuc, Q.; Nguyen, T.; Nguyen, T.; Pham, L.; Le, D.-T.; Ho, H.-H.; Truong, T.-B.; Tran, Q.-K. Young adults’ intentions and rationales for covid-19 vaccination participation: Evidence from a student survey in Ho chi minh city, Vietnam. Vaccines 2021, 9, 794. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, M.B.; Singh, S.; Polavarapu, M.; Jordan, T.R.; Melhem, N.M. COVID-19 vaccine hesitancy among university students in Lebanon. Epidemiol. Infect. 2021, 149, 1–32. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Watts, A.W.; Hutchison, S.M.; Bettinger, J.A.; Gadermann, A.; Oberle, E.; Oberlander, T.F.; Goldfarb, D.M.; Lavoie, P.M.; Mâsse, L.C. COVID-19 Vaccine Intentions and Perceptions Among Public School Staff of the Greater Vancouver Metropolitan Area, British Columbia, Canada. Front. Public Health 2022, 10, 832444. [Google Scholar] [CrossRef] [PubMed]
- Hossian, M.; Khan, A.S.; Nazir, A.; Nabi, M.H.; Hasan, M.; Maliha, R.; Hossain, M.A.; Rashid, U.; Itrat, N.; Hawlader, M.D.H. Factors affecting intention to take COVID-19 vaccine among Pakistani University Students. PLoS ONE 2022, 17, e0262305. [Google Scholar] [CrossRef] [PubMed]
- Determann, D.; Korfage, I.J.; Lambooij, M.S.; Bliemer, M.; Richardus, J.H.; Steyerberg, E.W.; de Bekker-Grob, E.W. Acceptance of Vaccinations in Pandemic Outbreaks: A Discrete Choice Experiment. PLoS ONE 2014, 9, e102505. [Google Scholar] [CrossRef]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States A review of measles and pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Nan, X.; Xie, B.; Madden, K. Acceptability of the H1N1 Vaccine Among Older Adults: The Interplay of Message Framing and Perceived Vaccine Safety and Efficacy. Health Commun. 2012, 27, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. Worldwide Vaccine Hesitancy. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Biswas, M.R.; Alzubaidi, M.S.; Shah, U.; Abd-Alrazaq, A.A.; Shah, Z. A Scoping Review to Find out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants. Vaccines 2021, 9, 1243. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef] [PubMed]
- Sweileh, W.M. Bibliometric analysis of global scientific literature on vaccine hesitancy in peer-reviewed journals (1990–2019). BMC Public Health 2020, 20, 1252. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [PubMed]
- D’onofrio, A.; Manfredi, P. Vaccine demand driven by vaccine side effects: Dynamic implications for SIR diseases. J. Theor. Biol. 2010, 264, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Haroon, N.; Venkatesan, K.; Menon, S. COVID-19 vaccine hesitancy among medical students: A systematic review. J. Educ. Health Promot. 2022, 11, 218. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.N.; Biswas, M.; Islam, E.; Azam, S. Potential factors influencing COVID-19 vaccine acceptance and hesitancy: A systematic review. PLoS ONE 2022, 17, e0265496. [Google Scholar] [CrossRef] [PubMed]
- Ackah, M.; Ameyaw, L.; Salifu, M.G.; Asubonteng, D.P.A.; Yeboah, C.O.; Annor, E.N.; Ankapong, E.A.K.; Boakye, H. COVID-19 vaccine acceptance among health care workers in Africa: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268711. [Google Scholar] [CrossRef] [PubMed]
- AlShurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What Demographic, Social, and Contextual Factors Influence the Intention to Use COVID-19 Vaccines: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow chart of the screening process.

Figure 2.
Countries and continents where the reviewed studies were conducted.

Table 1.
Planned Search Strategy.
| Item | Search Strategy |
|---|---|
| Database | Dimensions, PubMed, JSTOR, Google Scholar, Google, the WHO Library, and HINARI |
| Language filter | English |
| Date filter | No limits |
| Spatial filter | Global |
| Keywords |
|
| Inclusion criteria | The paper should be:
|
| Exclusion criteria | The paper should be:
|
Table 2.
Characteristics of the Reviewed Studies.
| Authors and Country | Population | Sample Size | Prevalence (%) | Acceptance/Hesitancy Predictors | |
|---|---|---|---|---|---|
| Acceptance | Hesitancy | ||||
| Dafogianni et al. [18] Greece | Students, teachers, and professors | 3697 | NA | NA | Lower personal and general perceived risk due to side effects of the COVID-19 vaccine was significantly associated with lower intention to be vaccinated. |
| Chen et al. [15] China | College students and teachers | 835 | NA | 31.8 Teachers 23.8 Students | Believed that vaccine safety was low and did not give any attention to vaccine news, with those who suffered from chronic diseases being more hesitant. |
| Kelekar et al. [19] USA | Dental and medical students | 415 | NA | 34.9 | |
| Xu et al. [20] China | College teachers | 251 | NA | 42.2 | Non-decision makers in the family were more hesitant. |
| Saied et al. [16] Egypt | Medical students | 2133 | 6 | 46 | Concerns for the vaccine’s adverse effects, ineffectiveness, deficient data regarding the vaccine’s adverse effects, and insufficient information regarding the vaccine itself. |
| Cahapay [21] Philippine | High school teachers | 1070 | 20.7 | NA | Male gender, high income, and education (graduate level) were associated with intentions to accept vaccines. |
| Kecojevic et al. [22] USA | College students | 457 | 23 | NA | Student healthcare workers, who had a family member who had received the COVID-19 vaccine, had greater positive attitudes towards vaccination, and received the seasonal flu vaccine were more likely to have received the vaccine. |
| Estrela et al. [23] Portugal | Preschool to higher education teachers | 1062 | 30 | 10 | Concerns about vaccine efficacy and safety increase the risk of hesitancy; a higher perceived risk of being infected, trust in the effectiveness of the vaccine in protecting them against complications of COVID-19, and a higher trust level of information sources were associated with decreased hesitancy. |
| Gkentzi et al. [12] Greece | Elementary school teachers | 399 | 38.1 | NA | Previous influenza vaccine uptake, believing COVID-19 vaccination was mandatory, and believing teachers were at high risk of being infected. |
| Šorgo et al. [24] Slovenia | Post-secondary school students | 5999 | 39.7 | 29.2 | Fear of COVID-19 played a significant role in the intention to vaccinate. |
| Shitu et al. [14] Ethiopia | Primary and secondary school teachers | 301 | 40.8 | NA | Being a male, a private school teacher, having high perceived susceptibility, high perceived seriousness, and perceived benefits of the vaccine were significant predictors of acceptance. |
| Sharaf et al. [25] Egypt | Teaching staff of a public university | 171 | 45.6 | 54.4 | Being a female, not intending to travel internationally, and being more anxious about COVID-19 were significantly associated with hesitancy. |
| Dubik [26] Ghana | Basic and senior high school teachers | 421 | 49 | NA | Unconfident about the COVID-19 vaccine, perception of not being susceptible to COVID-19, and feeling uncomfortable to receive the vaccine were associated with unwillingness to take the vaccine. Vaccination against hepatitis B, adequacy of information about the expectation of the COVID-19 vaccine, and not believing that the COVID-19 vaccine will cause illness were facilitators of vaccine acceptance. |
| Zhou et al. [27] China | Nursing students | 1070 | 51.9 | 4.7 | Positive beliefs towards general vaccination and COVID-19 vaccination, perception of less adverse effects following vaccination, and greater impact of COVID-19 on daily life were associated with intentions to vaccinate. Concerns about the safety of the vaccines and efficacy, the belief that vaccination was unnecessary, and less information about COVID-19 were associated with hesitancy. |
| Lucia et al. [28] USA | Medical students | 168 | 53 | 23 | Being public health experts and having fewer concerns about side effects increased the willingness to take the vaccine. |
| Handebo et al., [29] Ethiopia | Primary and secondary school teachers | 301 | 54.8 | NA | Education (a Bachelor’s degree), perceived susceptibility, perceived benefits, and cues to action significantly influenced intentions to receive vaccines. |
| Tavolacci et al. [30] France | College students | 3089 | 58 | 17 | The female gender and those studying science were at higher risk of vaccine hesitancy. Knowledge about conventional vaccination and the COVID-19 vaccine and confidence in safety and efficacy were associated with a lower risk of vaccine hesitancy. |
| Jain et al. [31] India | College students | 655 | 63.8 | 36.2 | Trust in the healthcare system and trust in domestic vaccines were significantly associated with vaccine acceptance. |
| Scharff et al. [32] Germany | Secondary school students | 903 | 68.3 | 7 | Students under 16 years and at lower education levels showed significantly higher vaccine hesitancy. |
| Montvidas et al. [33] Lithuania | Health science students | 1545 | 72.6 | 10 | Medicine students, non-infected students, and students who volunteered in COVID-19 wards were more willing to take the vaccine. Negative effects of the vaccine on their income and belief in the future were associated with vaccine hesitancy. |
| Riad et al. [34] Czech Republic | College students | 1351 | 73.3 | 7.4 | Trust in the pharmaceutical industry, trust in healthcare providers, and perceived knowledge sufficiency predicted higher odds of vaccine acceptance. |
| Khuc et al. [35] Vietnam | College students | 398 | 83.41 | 16.59 | Concerns about the vaccine’s side effects and lack of information were associated with hesitancy. |
| Hamdan et al. [36] Lebanon | University students | 3805 | 87 | 10 | Perceived vaccine safety was associated with vaccine acceptance or less hesitancy. Those who did not receive the flu vaccine and agreed with the conspiracy theory were more hesitant. |
| Racey et al. [13] Canada | Public school teachers | 5076 | 89.7 | NA | The male gender, a science or engineering education background, the belief that COVID-19 is a serious illness, higher vaccine knowledge, and reliable information sources on vaccination predicted intentions for vaccine acceptance. |
| Galle et al. [37] Italy | College students | 3226 | 91.9 | NA | Previous vaccination against influenza and knowledge were associated with the intention to receive the vaccine. |
| Watts et al. [38] Canada | Public school teachers | 2393 | 92.7 | NA | Valued expert recommendations, perceived susceptibility, accepted routine vaccines, and the perception of higher benefits were associated with vaccine acceptance. |
| Hossian et al. [39] Pakistan | College students | 2865 | 72.5 | NA | Higher education was associated with vaccine acceptance. |
Note. NA = not available. All studies adopted the cross-sectional survey design.
Table 4.
COVID-19 vaccine acceptance prevalence among reviewed studies.
| Authors | Country | Population | Acceptance (%) |
|---|---|---|---|
| Racey et al. [13] | Canada | Public school teachers | 89.7 |
| Watts et al. [38] | Canada | Public school teachers | 92.7 |
| Zhou et al. [27] | China | Nursing students | 51.9 |
| Riad et al. [34] | Czech Republic | College students | 73.3 |
| Saied et al. [16] | Egypt | Medical students | 6 |
| Sharaf et al. [25] | Egypt | College teachers | 45.6 |
| Shitu et al. [14] | Ethiopia | Primary and secondary school teachers | 40.8 |
| Handebo et al. [29] | Ethiopia | Primary and secondary school teachers | 54.8 |
| Tavolacci et al. [30] | France | College students | 58 |
| Scharff et al. [32] | Germany | Secondary school students | 68.3 |
| Dubik [26] | Ghana | Basic and senior high school teachers | 49 |
| Gkentzi et al. [12] | Greece | Elementary school teachers | 38.1 |
| Jain et al. [31] | India | College students | 63.8 |
| Galle et al. [37] | Italy | College students | 91.9 |
| Hamdan et al. [36] | Lebanon | College students | 87 |
| Montvidas et al. [33] | Lithuania | Health science students | 72.6 |
| Hossian et al. [39] | Pakistan | College students | 72.5 |
| Cahapay [21] | Philippine | High school teachers | 20.7 |
| Estrela et al. [23] | Portugal | Preschool to college education teachers | 30 |
| Šorgo et al. [24] | Slovenia | Post-secondary school students | 39.7 |
| Kecojevic et al. [22] | USA | College students | 23 |
| Lucia et al. [28] | USA | Medical students | 53 |
| Khuc et al. [35] | Vietnam | College students | 83.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sarfo, J.O.; Amoadu, M.; Ansah, E.W.; Hagan Jnr, J.E. COVID-19 Vaccine Acceptance and Hesitancy among Teachers and Students: A Scoping Review of Prevalence and Risk Factors. COVID 2024, 4, 557-570. https://doi.org/10.3390/covid4040037
AMA Style
Sarfo JO, Amoadu M, Ansah EW, Hagan Jnr JE. COVID-19 Vaccine Acceptance and Hesitancy among Teachers and Students: A Scoping Review of Prevalence and Risk Factors. COVID. 2024; 4(4):557-570. https://doi.org/10.3390/covid4040037
Chicago/Turabian StyleSarfo, Jacob Owusu, Mustapha Amoadu, Edward Wilson Ansah, and John Elvis Hagan Jnr. 2024. "COVID-19 Vaccine Acceptance and Hesitancy among Teachers and Students: A Scoping Review of Prevalence and Risk Factors" COVID 4, no. 4: 557-570. https://doi.org/10.3390/covid4040037