
Efficacy and Effectiveness of Physical Agent Modalities in Complex Regional Pain Syndrome Type I: A Scoping Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
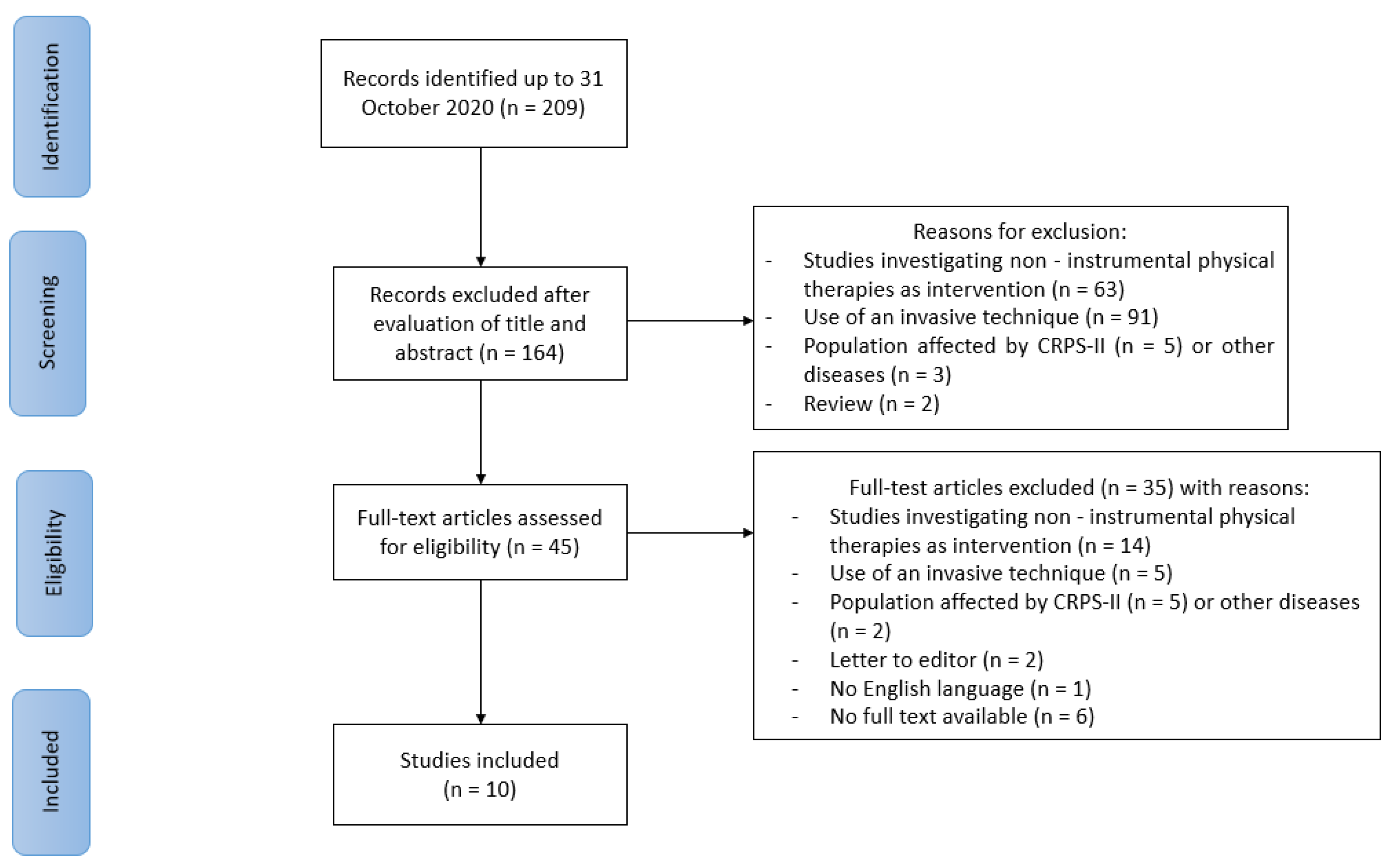
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Electromagnetic Field Therapy
3.2. Electrotherapy
3.2.1. TENS
3.2.2. Scrambler Therapy
3.3. Laser (or Light) Therapy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harden, R.N.; Bruehl, S.; Galer, B.S.; Saltz, S.; Bertram, M.; Backonja, M.; Gayles, R.; Rudin, N.; Bhugra, M.K.; Stanton-Hicks, M. Complex regional pain syndrome: Are the IASP diagnostic criteria valid and sufficiently comprehensive? Pain 1999, 83, 211–219. [Google Scholar] [CrossRef]
- Marinus, J.; Moseley, G.L.; Birklein, F.; Baron, R.; Maihöfner, C.; Kingery, W.S.; van Hilten, J.J. Clinical features and pathophysiology of complex regional pain syndrome. Lancet Neurol. 2011, 10, 637–648. [Google Scholar] [CrossRef] [Green Version]
- Ott, S.; Maihöfner, C. Signs and Symptoms in 1043 Patients with Complex Regional Pain Syndrome. J. Pain 2018, 19, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Pergolizzi, J.V.; LeQuang, J.A.; Nalamachu, S.; Taylor, R.; Bigelsen, R.W. The Budapest criteria for complex regional pain syndrome: The diagnostic challenge. Anaesthesiol. Clin. Sci. Res. 2018, 2, 1–10. [Google Scholar] [CrossRef]
- Mayo Clinic. Complex Regional Pain Syndrome—Symptoms and Causes. Available online: https://www.mayoclinic.org/diseases-conditions/crps-complex-regional-pain-syndrome/symptoms-causes/syc-20371151 (accessed on 3 December 2020).
- Merskey, H.; Addison, R.G.; Beric, A.; Blumberg, H.; Bogduk, N.; Boivie, J.; Bond, M.R.; Bonica, J.J.; Boyd, D.B.; Deathe, A.B.; et al. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms, 2nd ed.; Merskey, H., Bogduk, N., Eds.; IASP Press: Seattle, DC, USA, 1994; pp. 40–43. [Google Scholar]
- Pons, T.; Shipton, E.A.; Williman, J.; Mulder, R.T. Potential risk factors for the onset of complex regional pain syndrome type 1: A systematic literature review. Anesthesiol. Res. Pract. 2015, 2015, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urits, I.; Shen, A.H.; Jones, M.R.; Viswanath, O.; Kaye, A.D. Complex Regional Pain Syndrome, Current Concepts and Treatment Options. Curr. Pain Headache Rep. 2018, 22, 10. [Google Scholar] [CrossRef]
- Harden, N.R.; Bruehl, S.; Perez, R.S.G.M.; Birklein, F.; Marinus, J.; Maihofner, C.; Lubenow, T.; Buvanendran, A.; Mackey, S. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain 2010, 150, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Physichians. Complex Regional Pain Syndrome in Adults (2nd Edition), UK Guidelines for Diagnosis, Referral and Management in Primary and Secondary Care. 2018. Available online: https://www.rcplondon.ac.uk/guidelines-policy/complex-regional-pain-syndrome-adults (accessed on 3 December 2020).
- Vescio, A.; Testa, G.; Culmone, A.; Sapienza, M.; Valenti, F.; Di Maria, F.; Pavone, V. Treatment of Complex Regional Pain Syndrome in Children and Adolescents: A Structured Literature Scoping Review. Children 2020, 7, 245. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.E.; Bialocerkowski, A.E. Does evidence support physiotherapy management of adult Complex Regional Pain Syndrome Type One? A systematic review. Eur. J. Pain 2009, 13, 339–353. [Google Scholar] [CrossRef]
- Rakel, B.; Barr, J.O. Physical modalities in chronic pain management. Nurs. Clin. North Am. 2003, 38, 477–494. [Google Scholar] [CrossRef]
- Maher, C.G. Effective physical treatment for chronic low back pain. Orthop. Clin. North Am. 2004, 35, 57–64. [Google Scholar] [CrossRef]
- Ferronato, L.; Cunha, H.M.; Machado, P.M.; Souza, G.D.; Limana, M.D.; Avelar, N.C. Phisical modalities on the functional performance in knee osteoarthritis: A sytematic review. Fisioter. Mov. 2017, 30, 607–623. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Durmus, A.; Cakmak, A.; Disci, R.; Muslumanoglu, L. The efficiency of electromagnetic field treatment in Complex Regional Pain Syndrome Type I. Disabil. Rehabil. 2004, 26, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Cavazzuti, L.; Mosca, M.; Fusaro, I.; Zati, A. Bio-Electro-Magnetic-Energy-Regulation (BEMER) for the treatment of type I complex regional pain syndrome: A pilot study. Physiother. Theory Pract. 2018, 36, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Karabegović, A.; Kapidzić-Duraković, S.; Ljuca, F. Laser therapy of painful shoulder and shoulder-hand syndrome in treatment of patients after the stroke. Bosn. J. Basic Med. Sci. 2009, 9, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodenheim, R.; Bennett, J.H. Reversal of a Sudeck’s atrophy by the adjunctive use of transcutaneous electrical nerve stimulation. A case report. Phys. Ther. 1983, 63, 1287–1288. [Google Scholar] [CrossRef]
- Bukhalo, Y.; Mullin, V. Presentation and Treatment of Complex Regional Pain Syndrome Type 1 in a 3-Year-Old. Anesthesiology 2004, 101, 542–543. [Google Scholar] [CrossRef]
- Anandkumar, S.; Manivasagam, M. Multimodal physical therapy management of a 48-year-old female with post-stroke complex regional pain syndrome. Physiother. Theory Pract. 2014, 30, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Ashwal, S.; Tomasi, L.; Neumann, M.; Schneider, S. Reflex sympathetic dystrophy syndrome in children. Pediatr. Neurol. 1988, 4, 38–42. [Google Scholar] [CrossRef]
- Bilgili, A.; Çakır, T.; Doğan, Ş.K.; Erçalık, T.; Filiz, M.B.; Toraman, F. The effectiveness of transcutaneous electrical nerve stimulation in the management of patients with complex regional pain syndrome: A randomized, double-blinded, placebo-controlled prospective study. J. Back Musculoskelet. Rehabil. 2016, 29, 661–671. [Google Scholar] [CrossRef]
- Cimaz, R.; Matucci-Cerinic, M.; Zulian, F.; Falcini, F. Reflex Sympathetic Dystrophy in Children. J. Child. Neurol. 1999, 14, 363–368. [Google Scholar] [CrossRef]
- Raucci, U.; Tomasello, C.; Marri, M.; Salzano, M.; Gasparini, A.; Conicella, E. Scrambler Therapy (®) MC-5A for Complex Regional Pain Syndrome: Case Reports. Pain Pract. 2016, 16, 103–109. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Paoletta, M.; Moretti, A.; Brandi, M.L.; Iolascon, G. Complex regional pain syndrome: Facts on causes, diagnosis and therapy. Clin. Cases Miner. Bone Metab. 2018, 15, 166–172. [Google Scholar] [CrossRef]
- Iolascon, G.; Moretti, A. Pharmacotherapeutic options for complex regional pain syndrome. Expert Opin. Pharmacother. 2019, 20, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Smart, K.M.; Wand, B.M.; O’Connell, N.E. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database Syst. Rev. 2016, 2, CD010853. [Google Scholar] [CrossRef] [Green Version]
- Tashani, O.; Johnson, M. Transcutaneous Electrical Nerve Stimulation (TENS) A Possible Aid for Pain Relief in Developing Countries? Libyan J. Med. 2009, 4, 62–65. [Google Scholar] [CrossRef] [Green Version]
- Köke, A.J.; Schouten, J.S.; Lamerichs-Geelen, M.J.; Lipsch, J.S.; Waltje, E.M.; van Kleef, M.; Patijn, J. Pain reducing effect of three types of transcutaneous electrical nerve stimulation in patients with chronic pain: A randomized crossover trial. Pain 2004, 108, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Great Ormond Street Hospital for Children NHS Foundation Trust. Pain Relief Using Transcutaneous Electrical Nerve Stimulation (TENS). Available online: https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/pain-relief-using-transcutaneous-electrical-nerve-stimulation-tens (accessed on 21 December 2020).
- Marineo, G. Inside the Scrambler Therapy, a Noninvasive Treatment of Chronic Neuropathic and Cancer Pain: From the Gate Control Theory to the Active Principle of Information. Integr. Cancer Ther. 2019, 18, 1534735419845143. [Google Scholar] [CrossRef]
- Pagani, S.; Veronesi, F.; Aldini, N.N.; Fini, M. Complex Regional Pain Syndrome Type I, a Debilitating and Poorly Understood Syndrome. Possible Role for Pulsed Electromagnetic Fields: A Narrative Review. Pain Physician 2017, 20, E807–E822. [Google Scholar]
- Markov, M.S. Magnetic Field Therapy: A Review. Electromagn. Biol. Med. 2007, 26, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.L.; Wong-Gibbons, D.; Maultsby, J. Microcirculatory effects of pulsed electromagnetic fields. J. Orthop. Res. 2004, 22, 80–84. [Google Scholar] [CrossRef]
- Groeneweg, G.; Huygen, F.J.; Coderre, T.J.; Zijlstra, F.J. Regulation of peripheral blood flow in complex regional pain syndrome: Clinical implication for symptomatic relief and pain management. BMC Musculoskelet. Disord. 2009, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ide, Y. Phototherapy for chronic pain treatment. Masui 2009, 58, 1401–1406. [Google Scholar] [PubMed]
- Huang, Z.; Ma, J.; Chen, J.; Shen, B.; Pei, F.; Kraus, V.B. The effectiveness of low-level laser therapy for nonspecific chronic low back pain: A systematic review and meta-analysis. Arthritis Res. Ther. 2015, 17, 360. [Google Scholar] [CrossRef] [Green Version]
- Farivar, S.; Malekshahabi, T.; Shiari, R. Biological effects of low level laser therapy. J. Lasers Med. Sci. 2014, 5, 58–62. [Google Scholar]
- De Andrade, A.R.; Meireles, A.; Artifon, E.L.; Brancalhão, R.M.C.; Ferreira, J.R.L.; Bertolini, G.R.F. The Effects of Low-Level Laser Therapy, 670 nm, on Epiphyseal Growth in Rats. Sci. World J. 2012, 1–5. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Search Strategy |
|---|
| (“Electric Stimulation Therapy”[Mesh] OR “Pulsed electromagnetic field” OR “Low-Level Light Therapy”[Mesh] OR “Laser Therapy”[Mesh] OR “Magnetic Field Therapy”[Mesh] OR “Extracorporeal Shockwave Therapy”[Mesh] OR “Hyperthermia, Induced”[Mesh] OR “Cryotherapy”[Mesh] OR “Physical Therapy Modalities”[Mesh] NOT “Spinal Cord Stimulation”[Mesh]) AND (“Reflex Sympathetic Dystrophy”[Mesh] OR “Complex Regional Pain Syndromes”[Mesh]) |
| Eligibility Criteria |
|---|
| Inclusion criteria: |
|
| Exclusion criteria: |
|
| Author, Year | Physical Therapy Modality | Study Design | Sample Size: Total (group) | Administration | Main Findings |
|---|---|---|---|---|---|
| Durmus A. et al. 2004 | PEMF | Randomized double-blind, placebo-controlled study | n = 40 PEMF Group: n = 20 Placebo Group: n = 20 | Both groups: Calcitonin (100 units ampoule for 6 weeks) and active/active assistive ROM exercises (three times a day for a period of 30 min per session for 6 weeks). PEMFs: intensity 100 Gauss, frequency 50 Hertz (5 times a week for 6 weeks, 30 sessions). Placebo treatment: device turned off (60 min per session). | No additional benefits were observed to PEMFs associated to calcitonin and exercise therapy in improving pain (measured by VAS score), swelling, instrumental (bone scan), and laboratory values. |
| Bilgili A. et al. 2016 | TENS | Randomized, double-blind, placebo-controlled prospective study | n = 30 Experimental group (conventional TENS + contrast bath + whirlpool bath+ exercise program) n = 15 Control group (sham TENS + contrast bath + whirlpool bath + exercise program) n = 15 | Conventional TENS: frequency 100 Hertz, pulse duration 50–100 milliseconds. Duration: 20 min for session. Sharm TENS: device turned off. Contrast bath: immersion in hot water (38 °C) for 4 min followed by cold water (4 °C) for 1 min. Overall duration 20 min. Whirlpool bath: immersion in a whirlpool tank containing hot water (37 °C) for 15 min. Exercise program: daily active, active assistive and passive ROM exercises (3 sets of 10 repeats for 15 sessions). All interventions were administered for 15 sessions. | Additional TENS reduces spontaneous pain (measured by VAS), neuropathic pain (measured by DN-4 and LANSS scores), volumetric oedema, and improves ROM. |
| Benedetti M.G. et al. 2018 | PEMF | Randomized controlled double-blind pilot study | n = 30 Experimental group (rehabilitation program + BEMER EMFs) N = 15 Control group (rehabilitation program + placebo BEMER treatment) n = 15 | BEMER PEMFs: frequency < 33.3 Hertz, intensity (total body: 7–35 microTesla, pad: 60–100 microTesla). Duration: daily 20-min session for 10 days. BEMER placebo treatment: device turned off. Rehabilitation program: information on the pathology, contrast of kinesiophobia, psychological support, kinesiotherapy with active/active/assisted/passive mobilization, desensitization techniques, proprioceptive feedback, gait rehabilitation for lower limb; perceptive motor therapy and occupational therapy for upper limb. Duration: 2-h sessions per day, for 10 days. | BEMER PEMFs combined with other rehabilitation interventions reduce pain (measured by VAS score) and improves strength and function (measured by HGS and DASH scores for the upper limb and by MFS for the lower limb) in the short term (1 month). |
| Author, Year | Physical Therapy Modality | Study Design | Sample Size: Total (Group) | Administration | Main Findings |
|---|---|---|---|---|---|
| Bohednim R. et al. 1983 | TENS | Case report | n = 1 | Pulse rate: 20 pulses per second Width: 100 microseconds Intensity depending on patient tolerance. Duration: one hour, three times a week for 2 months. | TENS improved pain relief and stimulated weight acceptance on the involved limb. There was an increase in bone stock and atrophy resolution in a short time. |
| Bukhalo J. et al. 2004 | TENS | Case report | n = 1 | TENS: no data available. Naproxen: 125 mg orally twice daily. Physical therapy: massage using lymphedema techniques of skin stretching, along with active and passive range of motion exercises. Duration: 3 times a week. | TENS remarkably improved pain, swelling, and oedema two weeks after the beginning of therapy. At 1 month, symptoms completely resolved. |
| Anandkumar S. et al. 2014 | TENS | Case report | n = 1 | TENS: high frequency (100 Hertz), pulse width 150 milliseconds, 4 channels. Kinesio Tape: ‘‘I’’ strips measuring 15 cm and 25 cm applied for about 48 h. PEPT: daily bi-manual activities such as cutting vegetables, etc. Exercise therapy: scapular setting exercises using a Swiss ball (10 times, 3 sets) and rotator cuff strengthening exercises using a Thera-Band latex free resistance band (10 times, 3 sets). Duration: 8 weeks. | Intervention resolved pain (measured by VAS), improved upper limb physical function (measured by DASH) and kinesiophobia (measured by TSK) after 7 weeks and maintained at six months. |
| Ashwal S. et al. 1988 | TENS | Case series | n = 3 | Case 1: TENS (no data available). Case 2: sympathectomy. Case 3: TENS (no data available). | Case 1: immediate decrease in hyperesthesia. Symptoms resolved within 3 months. Case 2: normal strength and sensation was achieved 30 months after initial symptoms. Case 3: reduction of pain after 5 days. |
| Cimaz R. et al. 1999 | Electrotherapy (TENS, electrical stimulation), laser therapy | Case series | n = 6 | Case 1: naproxen and physical therapy (passive movements). Case 2: ganglion blockade, TENS (no data available), psychotherapy. Case 3: electrical stimulation (no data available), psychotherapy, physical therapy, electrotherapy (no data available). Case 4: immobilization, laser therapy (no data available), local injections, FANS, physical therapy. Case 5: physiotherapy. Case 6: acetaminophen and psychotherapy. | Case 1: able to walk at discharge after 2 weeks. Case 2: persistence of symptoms after two years, with less severity and frequency. Case 3: good results of electrical stimulation initially. After 8 months patient had a conversion reaction treated with psychotherapy, physical therapy, and electrotherapy, with no benefits. Case 4: no improvement reported. Case 5: resolution of symptoms over time (not specified). Case 6: symptoms quickly improved (timing of follow-up not specified). |
| Raucci U. et al. 2016 | Scrambler therapy | Case series | n = 4 (3 patients had CRPS-I, one patient had CRPS-II) | A 45-min daily treatment was administered to each patient for 10 consecutive days. Intensity differed amongst patients (maximum intensity without additional pain). | Pain relief (measured by NRS) and improved quality of life for long periods (not specified). |
| Karabegovic A. et al. 2009 | Laser therapy, electrotherapy (TENS, stabile galvanization) | Case control study | n = 70 Experimental group (kinesiotherapy and ice massage plus laser therapy) n= 35 Control group (kinesiotherapy and ice massage plus TENS and stabile galvanization) n = 35 | Experimental group: Infrared laser: 830 nanometres. Dose: 3 Joule. Mean power: 50 milliwatts Control group: TENS, stabile galvanization: No data available Duration of treatments for both groups: 6 weeks. | Laser therapy shows significantly better results in reducing pain (measured by VAS score), swelling (range measured by the centimetres band), disability (DASH questionnaire), independence (Barthel index and FIM) and in increasing ROM compared to TENS. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretti, A.; Gimigliano, F.; Paoletta, M.; Liguori, S.; Toro, G.; Aulicino, M.; Conversano, S.; Iolascon, G. Efficacy and Effectiveness of Physical Agent Modalities in Complex Regional Pain Syndrome Type I: A Scoping Review. Appl. Sci. 2021, 11, 1857. https://doi.org/10.3390/app11041857
Moretti A, Gimigliano F, Paoletta M, Liguori S, Toro G, Aulicino M, Conversano S, Iolascon G. Efficacy and Effectiveness of Physical Agent Modalities in Complex Regional Pain Syndrome Type I: A Scoping Review. Applied Sciences. 2021; 11(4):1857. https://doi.org/10.3390/app11041857
Chicago/Turabian StyleMoretti, Antimo, Francesca Gimigliano, Marco Paoletta, Sara Liguori, Giuseppe Toro, Milena Aulicino, Stefano Conversano, and Giovanni Iolascon. 2021. "Efficacy and Effectiveness of Physical Agent Modalities in Complex Regional Pain Syndrome Type I: A Scoping Review" Applied Sciences 11, no. 4: 1857. https://doi.org/10.3390/app11041857
APA StyleMoretti, A., Gimigliano, F., Paoletta, M., Liguori, S., Toro, G., Aulicino, M., Conversano, S., & Iolascon, G. (2021). Efficacy and Effectiveness of Physical Agent Modalities in Complex Regional Pain Syndrome Type I: A Scoping Review. Applied Sciences, 11(4), 1857. https://doi.org/10.3390/app11041857