2.1. Integration versus Differentiation
According to a study by Lawrence and Lorsch [
19], an organization is defined as “a system of interrelated behaviors of people who are performing a task that has been differentiated into several distinct subsystems, each subsystem performing a portion of the task, and the efforts of each being integrated to achieve the effective performance of the system”. As Lawrence and Lorsch [
19] argued, organizations must balance differentiation and integration to succeed. In their study, companies that managed to achieve high subsystem differentiation while maintaining high integration between subsystems seemed to be best equipped to adapt to environmental changes. Lawrence and Lorsch [
19] explained how as an organization becomes differentiated into subsystems, its environment becomes segmented in order to undertake whole tasks (with their uncertainty) in the related environment. Hence, the kind of integration needed to achieve effective performance depends on the characteristics of the tasks in the organization’s segments.
As an organization segments its environment, the accompanying uncertainty can disturb the organization in various ways. Hence, as Weick [
17] suggested, the organization needs multiple options to solve it. According to Weick’s [
17] model of organizing, situations like this are best resolved through collective interdependent communication and information processing activities that help reduce uncertainty and identify appropriate responses. One option to deal with uncertainty is to manage the distribution of authority within the organization. For instance, if a particular segment of the organization has a task environment that is not shared with other segments, and this segment also does not share resources with other segments, the kind of integration, such as central coordination of all decisions of this particular segment, would be costly and highly inefficient. Instead, the design solution is to transfer the decision points downward in the hierarchy to the organizational segment where the action takes place [
20].
Another way to deal with uncertainty is to manage a hospital (and the decentralized departments) as a closed-loop system [
5,
21] With the closed-loop system, hospitals maintain high integration between departments, although they, on the other hand, may have high department differentiation. This is because a closed-loop system is designed so that feedback is signaled to the input to achieve and maintain the desired output condition [
22]. To avoid blockages, decisions to match the supply demand of departments are based on feedback from each department and other interrelated departments. To enable decision-making in a closed-loop system, hospitals can create mechanisms that permit coordinated action across many interdependent departments [
5].
2.2. Information Processing Organizations in Hospitals
To enable decision-making in a closed-loop system, certain coordination mechanisms are required. Galbraith [
1] argued that having rules, providing programs, and setting goals are more straightforward approaches for an organization’s coordination mechanisms. Staff members working on different subtasks are taught about possible situations and events that could occur while performing each subtask [
1]. However, such a coordination mechanism may be a good solution for small companies, but it is only feasible in some organizations. In the case of an unforeseen event, management becomes a challenge, though this is solvable by hierarchy [
1]. We refer to this as “management by exception”, as Galbraith [
1] explained. In the case of an increasing number of unforeseen events, a hierarchy can reach its maximum capacity for processing information, resulting in an overload.
Galbraith [
1] then explained four integration design strategies for information processing organizations, in addition to the rules, programs, goals, and hierarchy mentioned above. The choice of a specific strategy depends on its relative cost and the uncertainty the organization faces. Hence, organizations may differ in their structure, though they can be equally effective.
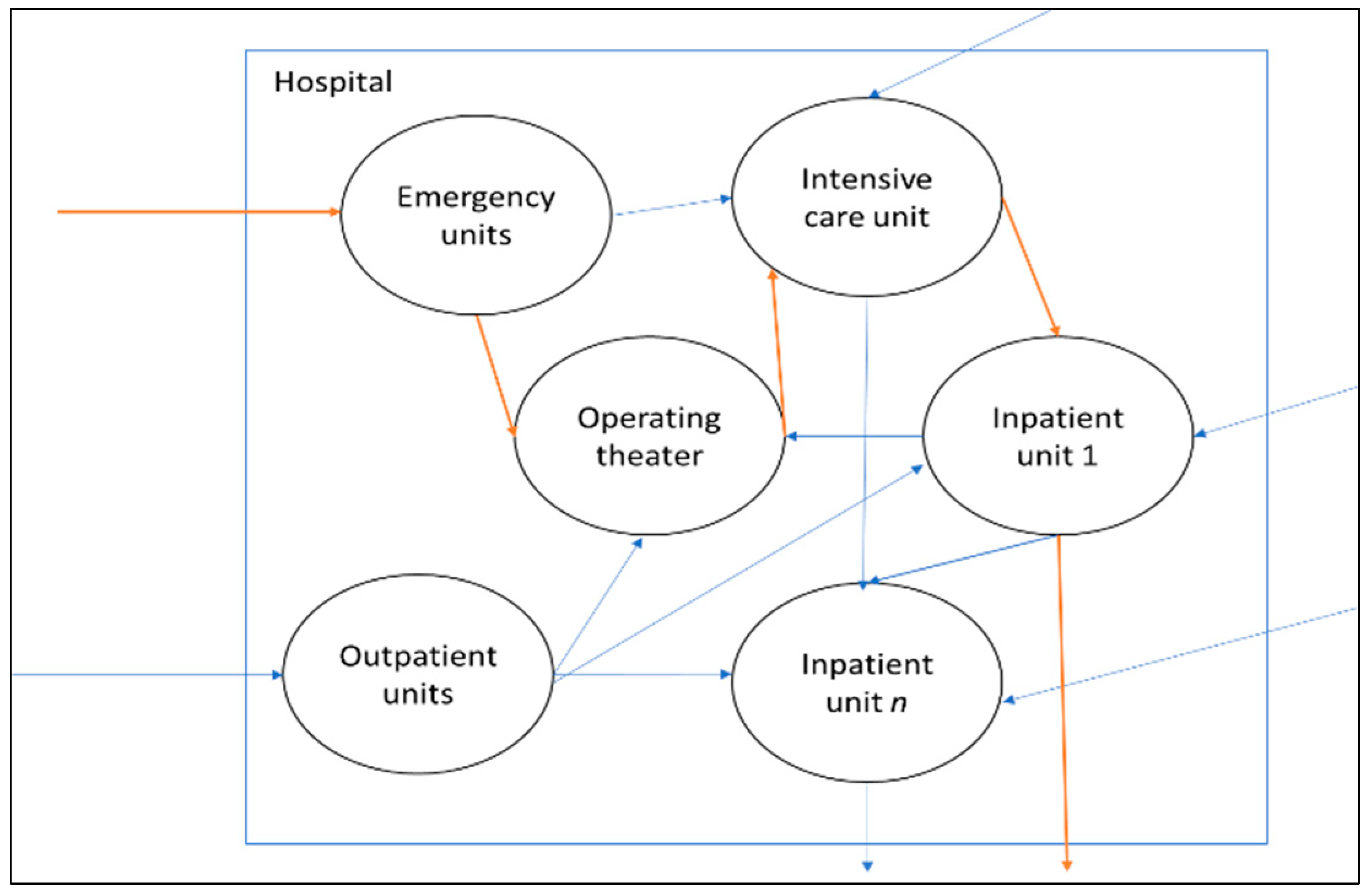
To illustrate Galbraith’s [
1] design strategy in a hospital system, we converted the example in
Figure 1 into a mini-hospital with only four departments, as shown in
Figure 2. The example departments are the emergency department (ED), where patients arrive, an intensive care unit (ICU), and two surgical/medical wards (IWs). The decision authority regarding patient movements is coordinated in a decentralized manner, which means the involved departments coordinate patients separately from the other departments. Here, the departments need the patients’ positional information to know their actual position in the system [
6]. The positional information can be acquired through the organization’s information system. As stated earlier, although positional information is essential, hospitals still need to check the detailed status of patients (e.g., obtaining better or remaining ill) to see whether they are ready to leave the hospital (i.e., recovered). The acquisition of such fine-grained information can contribute to delays in decision-making.
Furthermore, due to the division of labor in a hospital, nurses are allocated to departments in a decentralized manner by a local planner in each department. Here, the local planner needs task allocation information, often in fine granularity, to determine which types of nurses to deploy to which department beds for a specific shift.
Uncertainty about the rate of patient arrivals, the length of stay, or the care pathways in a hospital necessitates hospitals to acquire and process information to make planning adjustments. The first two designs of Galbraith’s [
1], the slack resources and the creation of self-contained tasks, aim to minimize the need for information processing. The other two designs increase the capability to process information for decision-making. These four strategies are related to the central point of Lawrence and Lorsch [
19], where the choice of an integration strategy depends on the characteristics of the tasks (uncertainty) in the organization’s segments.
The creation of slack resources is about creating buffers to reduce the effect of uncertainty on organizational segments. Creating slack resources may be necessary to accommodate disruptions or peaks in demand [
23,
24]. The design choices for creating buffer resources comprise the what (e.g., lead time, utilization, etc.), the when and the where in the organization.
In the example given in
Figure 2, the hospital can create spare beds (i.e., a buffer) in the inpatient wards (IW1 and IW2). Creating a buffer in the inpatient wards reduces the need for information processing when more acute patients arrive from the ED and the ICU than anticipated. This is because a mismatch between the number of inpatient beds and the patient demand for inpatient beds would be less likely to occur. Although uncertainty always requires some buffering, the required number and size of buffers can be mitigated with capacity pooling [
23,
25,
26].
When inpatient wards are physically pooled, from the perspective of decision-makers, the complexity of patient allocation to wards is reduced as the number of states to be considered decreases. In this case, a portion of patient positional information processing belonging to the pooled wards is now delegated to the pooled wards. Reduced complexity from the system perspective can lead to minimized delays in decision-making.
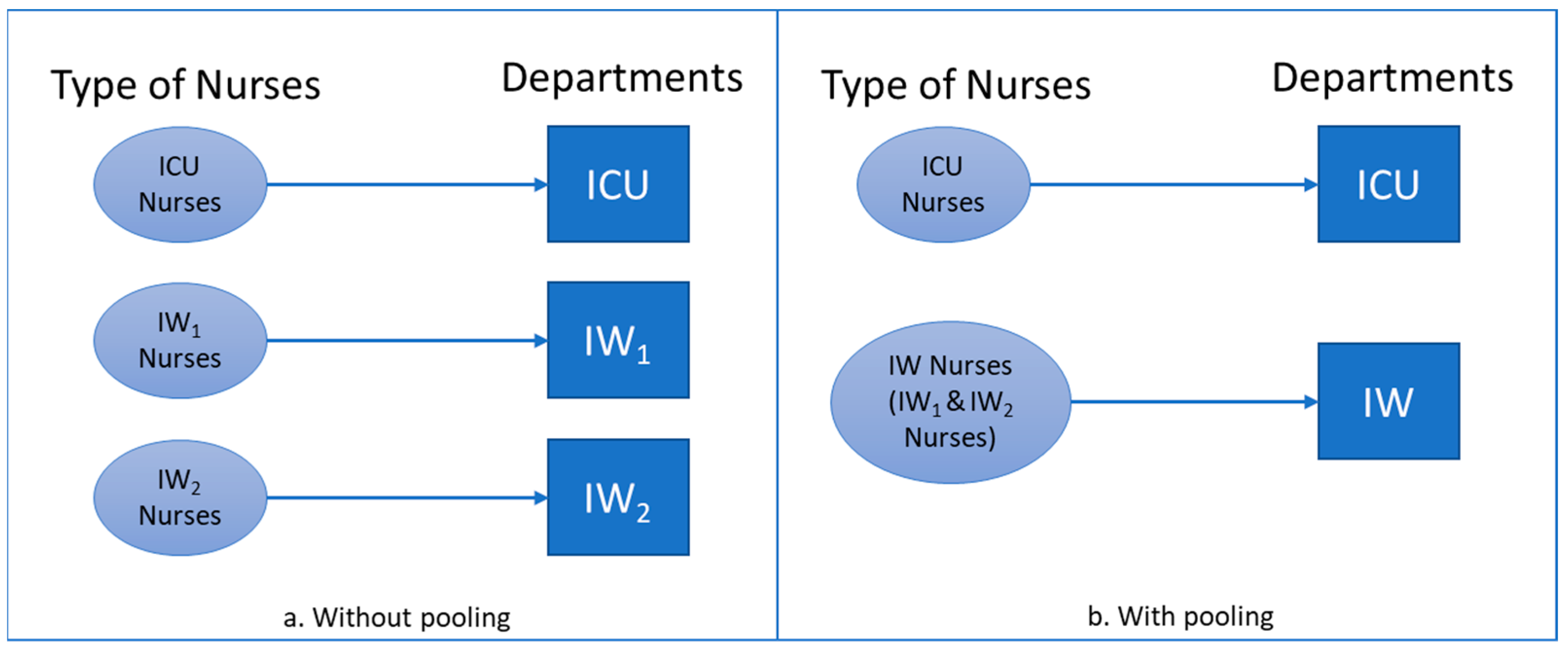
Furthermore, the nurses are now multi-skilled within the pooled wards and can be assigned to them, as can be seen in
Figure 3b. When the planner (i.e., the one who makes the decision to allocate nurses to beds in the pooled wards) is centralized along with the nurses, as the wards are physically pooled, the complexity of nurse allocation to wards from the hospital system perspective is also reduced, as the number of states to be considered (i.e., types of nurses and wards) decreases. The system then needs less information to complete the work.
In a self-contained design, the functional grouping of resources is carried out based on the product category [
1]. This design minimizes the need for information processing because it reduces the amount of output diversity (and hence its uncertainty) that would occur with a single collection of resources.
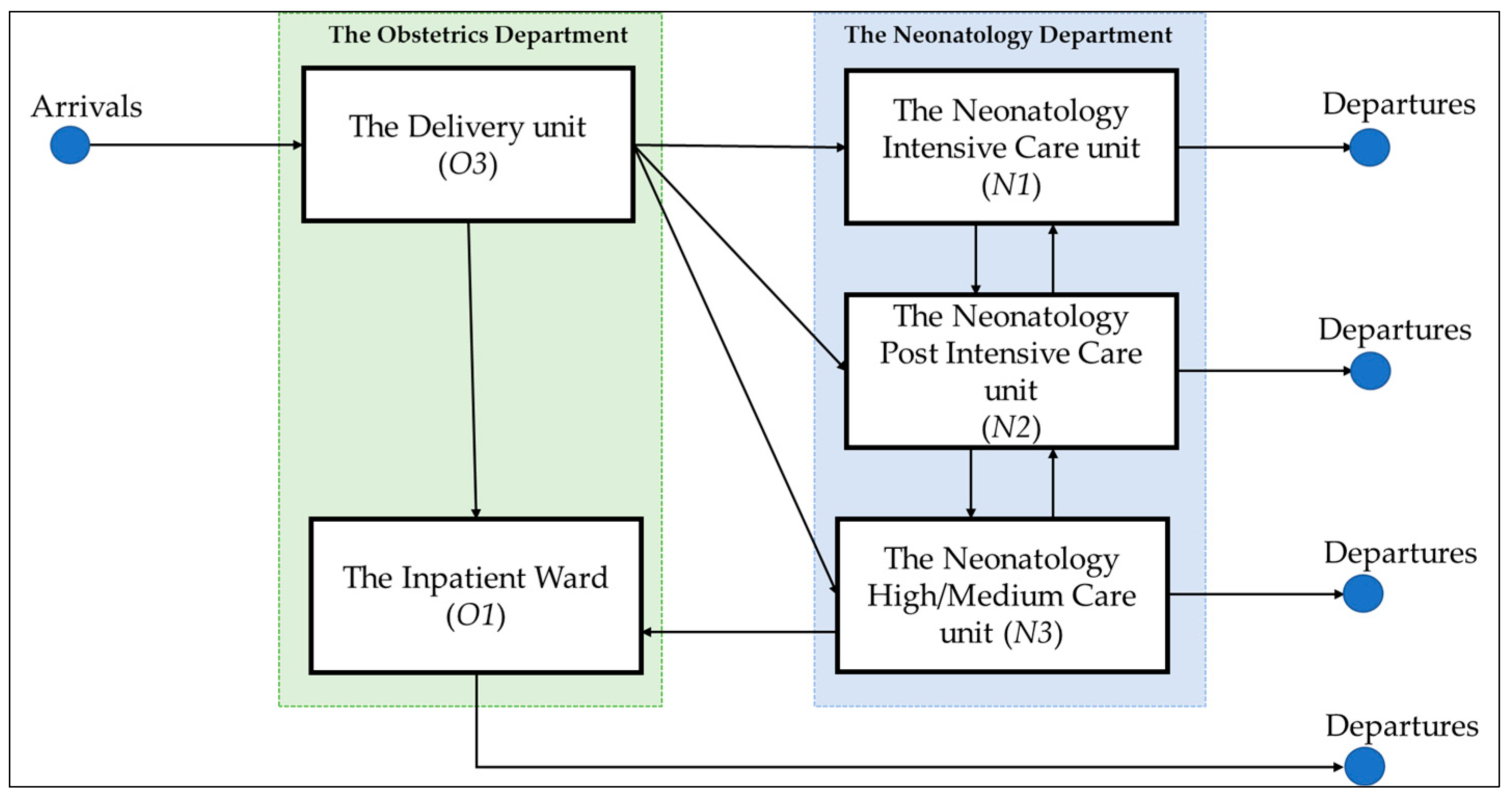
For the hospital example shown in
Figure 2, resource departments are grouped according to the nature of the illness (e.g., neurological or orthopedic inpatient wards) and the type of bed (e.g., intensive care or regular beds in inpatient wards). Once diagnosed in the ED, a patient can progress to the neurological ward, the orthopedic ward, or the intensive care unit. Supposing the hospital focuses its grouping only on the type of bed, the output diversity is reduced to only intensive care or regular beds in wards (i.e., there is no distinction between neurological and orthopedic inpatient wards). This design eventually reduces the division of labor (i.e., from three groups to two groups), and thus the needed information processing to allocate patients to wards. However, the coordinated effort in the regular wards increases as the number of choices (i.e., multi-skilled nurses) increases.
A coordinated effort for nurse allocation in the regular wards requires less information to complete the work when the number of states to be considered (i.e., types of nurses and wards) decreases.
Given the uncertainty (e.g., patient arrivals), exceptions such as mismatches between supply (e.g., of beds) and demand (e.g., for beds) require hospitals to adjust their plan accordingly. Galbraith [
1] explained “management by exception,” which occurs when the subordinate reports the mismatches to the manager when the supply–demand mismatch is outside of the subordinate’s scope. The subordinate waits for the manager’s instructions to solve the unforeseen mismatch. In the case of increasing mismatches, a hierarchy can reach its maximum capacity for processing information, resulting in an overload. Investing in a vertical information system is then needed to enable feedback from the operational level to cascade up to the tactical level, where there is a global overview of all affected subsystems, without overloading the hierarchical communication channels.
As discussed in Galbraith [
1], the greater the frequency of re-planning, the greater the amount of resources required to process information to fulfill the adjustments. Galbraith [
1] suggested that the cost of information processing can be minimized if the language is formalized. Formalizing the decision-making language means that “more information is transmitted with the same number of the symbol”. Formalization can also be achieved through information aggregation, in which the granularity of information is reduced. This involves the concept of coarse graining. A fine-grained description is a detailed description of the system’s microscopic behavior, while a coarse-grained description is one where the fine detail has been smoothed over through aggregation.
Several methods of coarse graining can be used. Gong et al. [
6] discussed how a manufacturing system worked with aggregated information to plan and control its production using a CONWIP system. In CONWIP, the system authorizes the release of patients based on system status [
23,
27]. The system status here is information aggregated by workload.
For the hospital example shown in
Figure 2, feedback from the ICU and IWs is needed to know if patients can be admitted from the ED accordingly. When the information from all of the wards is aggregated only to report their workload (i.e., the number of occupied beds), instead of every detail on patient mismatches, the hospital can have a shorter planning horizon (i.e., greater feedback frequency) to acquire and process information from interdependent wards. Due to the aggregated information (i.e., workload as the number of occupied beds), this design eventually reduces the output diversity, hence the need for information processing to allocate patients to wards.
In a hospital, patients move through different departments to obtain their needed treatments, and in this way, departments are interdependent, as shown in
Figure 2. When an organization has several interdependent subsystems, uncertainty about supply and demand might make it difficult for decision-makers to communicate with all the roles with which they are interdependent. The design solution for this is to create a mechanism that permits coordinated action across large numbers of interdependent roles and subsystems [
1,
19], and to transfer the decision points downward in the hierarchy to the points where the action takes place in order to ensure flexibility with increasing uncertainty.
One way to do this is to create lateral relationships (i.e., horizontally, outside the hierarchical level) to develop collaborative decision-making processes that cut across lines of authority and to increase the decision-making power of lower levels in the hierarchy. There are various design options, as discussed in Galbraith [
1], from direct contact between managers who share a problem but have no formal decision power to a matrix with dual authority (e.g., technical and formal authority) in the organization. This aligns with Weick’s [
17] model of organizing, in which decisions to identify appropriate responses to supply and demand uncertainty are made through collective interdependent communication.
In the example shown in
Figure 2, the hospital can adopt the “integrating” role discussed in Galbraith [
1]. At the operational level, an integrating role is created to acquire aggregated information (i.e., coarse-grained, as explained earlier) about the number of occupied beds in the ICU and the IWs. When a supply–demand mismatch occurs in a department, the role will have enough decision power to prioritize where patients should be admitted into wards. Having decision power at lower levels of the hierarchy reduces management’s effort and time, hence minimizing the effort needed for information processing to allocate patients to wards.
2.3. Entropy and Information Processing Structure
A given system design follows a specific structure in which information is gathered and processed. An information entropy model can be used to measure the amount of information [
7]. Entropy is defined as a measure of randomness or disorder in a system [
6,
9]. One may ask why we should focus on entropy. It is because information entropy values can be assigned to specific structures so that we can compare them in order to gain insights into the factors that lead to effective decision-making. To calculate the information entropy (
H), we can follow Shannon’s information entropy formula [
8]. If the average uncertainty associated with an outcome is represented by discrete random variable
X, Shannon’s information entropy of a discrete random variable of
X, with
n outcomes (
x1,
x2, …,
xn), is as follows:
Zhang and Xiao [
7] defined the amount of information needed to describe the expected states of a system as structural entropy. As stated earlier, when a hospital system is characterized as having several workstations (i.e., departments) connected in a network, uncertainty about patients’ required positions in the system can cause delays in the decision-making process. We refer to this as positional uncertainty [
6]. Furthermore, when departments have multi-skilled nurses, there is uncertainty about where to allocate nurses to the needed departments in the system, and this can also lead to delays in decision-making. We refer to this as task allocation uncertainty. Positional and task allocation uncertainty can both be measured with information entropy.
Given a specific system structure, we need the information of
, that is, the probability of a patient
progressing to department
. For every
,
Having
, the positional entropy of a patient in department
can be calculated as follows:
The positional entropy of all patients in the system is the following:
where
is the positional entropy of the system,
is the probability of patient
progressing to department
,
is the number of patients, and
is the number of possible states (i.e., departments) for patient
.
To measure task allocation entropy, we followed Shuiabi et al. [
28] in conceptualizing entropy as a measure of flexibility. Shuiabi et al. [
28] applied entropy to measure the relative demand for products, which is the ratio of time spent on processing a product to the total processing time for all products. When workstations can handle more products (i.e., they are flexible), the entropy associated with the process also increases. We applied the same concept to using multi-skilled nurses who can care for various patient groups:
, that is, the probability of a patient
being cared for by nurse type
j. For every
,
The relative demand
P of patient
i being cared for by nurse type
j is as follows:
The task allocation entropy of nurse type
j is the following:
The task allocation entropy of all nurses in the system is the following:
where
is the task allocation entropy of the system,
is the number of patient groups,
is the number of patient groups that nurse type
j handles, and
is the hours caring for patient
i by nurse type
j.
As stated above, probabilities are needed to calculate entropy, which depends on the available information in the system. When such information is unknown, assumptions are made to estimate probability. Instead of using an estimation, we can consider the extremum of information entropy [
6].
The extremum of information entropy is used to discover the probability distribution, leading to the highest value for this uncertainty, thereby assuring that no information is carelessly assumed. That is, for the positional entropy example, we acknowledge that it is impossible to say that a patient is more likely to be in department . When assuming the extremum of information entropy, the patient has an equal probability of being in any department within the system.
As stated earlier, information entropy values can be assigned to specific structures of information processing in order to compare them so that insights into the factors that lead to effective decision-making can be gained. In this respect, assigning the information entropy is the work that has to be performed to obtain information about situations. The multiplicity perspective can be used to evaluate the number of ways different outcomes can occur [
29]. In this regard, the more independent options a department has, the more uncertainty it has in explaining a situation; hence, the higher the entropy will be.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}