
Information-Theoretic Analysis of Cardio-Respiratory Interactions in Heart Failure Patients: Effects of Arrhythmias and Cardiac Resynchronization Therapy

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Experimental Protocol
2.2. Information-Theoretic Measures and Data Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Heart Rate and Respiratory Rate
4.2. Granger Causality and Transfer Entropy
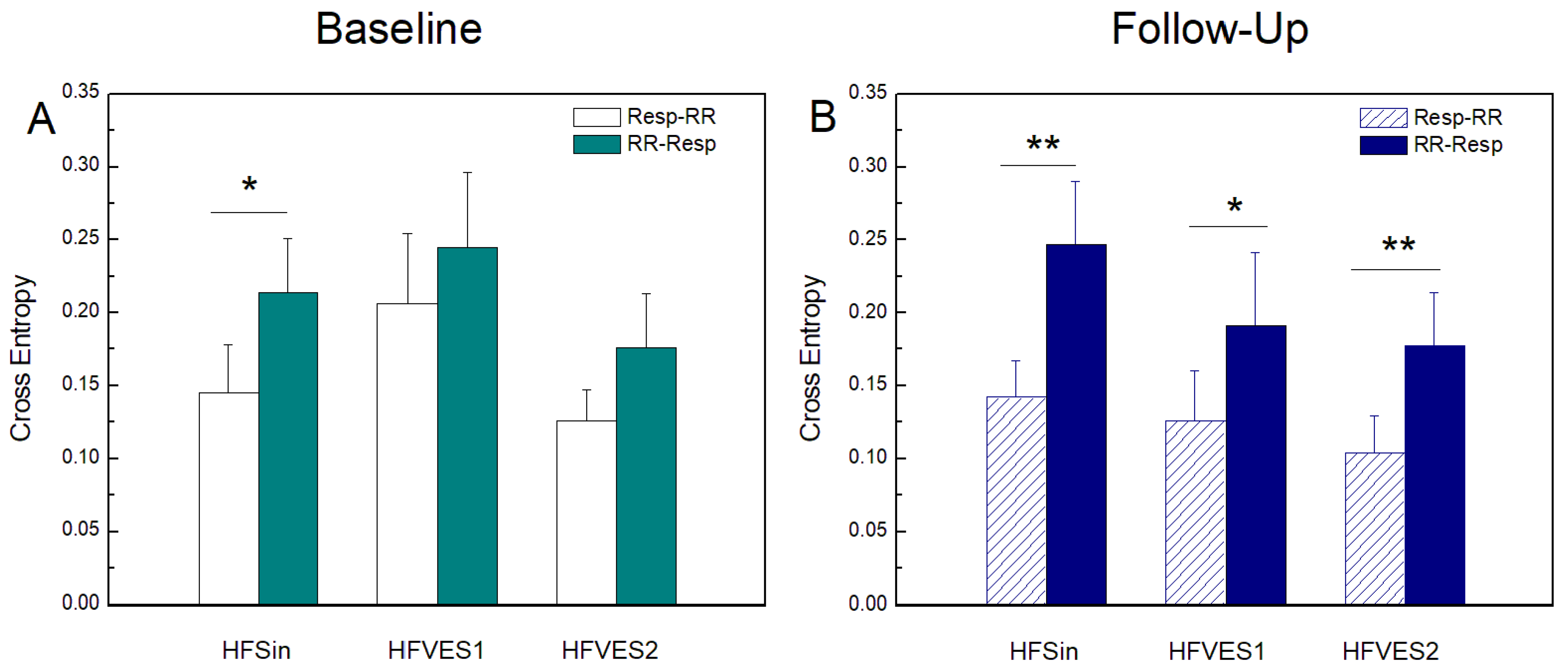
4.3. Cross Entropy
4.4. Cardiac Resynchronization Therapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Porta, A.; Guzzetti, S.; Montano, N.; Pagani, M.; Somers, V.; Malliani, A.; Baselli, G.; Cerutti, S. Information domain analysis of cardiovascular variability signals: Evaluation of regularity, synchronisation and co-ordination. Med. Biol. Eng. Comput. 2000, 38, 180–188. [Google Scholar] [CrossRef] [PubMed]
- de Abreu, R.M.; Cairo, B.; Porta, A. On the significance of estimating cardiorespiratory coupling strength in sports medicine. Front. Netw. Physiol. 2023, 2, 1114733. [Google Scholar] [CrossRef]
- Kapidžić, A.; Platiša, M.M.; Bojić, T.; Kalauzi, A. Nonlinear properties of cardiac rhythm and respiratory signal under paced breathing in young and middle-aged healthy subjects. Med. Eng. Phys. 2014, 36, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Borovkova, E.I.; Prokhorov, M.D.; Kiselev, A.R.; Hramkov, A.N.; Mironov, S.A.; Agaltsov, M.V.; Ponomarenko, V.I.; Karavaev, A.S.; Drapkina, O.M.; Penzel, T. Directional couplings between the respiration and parasympathetic control of the heart rate during sleep and wakefulness in healthy subjects at different ages. Front. Netw. Physiol. 2022, 2, 942700. [Google Scholar] [CrossRef] [PubMed]
- Sorelli, M.; Hutson, T.N.; Iasemidis, L.; Bocchi, L. Linear and Nonlinear Directed Connectivity Analysis of the Cardio-Respiratory System in Type 1 Diabetes. Front. Netw. Physiol. 2022, 2, 840829. [Google Scholar] [CrossRef]
- Radovanović, N.N.; Pavlović, S.U.; Milasinovic, G.; Kircanski, B.; Platiša, M. Bidirectional Cardio-Respiratory Interactions in Heart Failure. Front. Physiol. 2018, 9, 165. [Google Scholar] [CrossRef] [Green Version]
- Elstad, M.; O’callaghan, E.L.; Smith, A.J.; Ben-Tal, A.; Ramchandra, R. Cardiorespiratory interactions in humans and animals: Rhythms for life. Am. J. Physiol. Circ. Physiol. 2018, 315, H6–H17. [Google Scholar] [CrossRef] [Green Version]
- Platiša, M.M.; Radovanović, N.N.; Kalauzi, A.; Milašinović, G.; Pavlović, S.U. Multiscale Entropy Analysis: Application to Cardio-Respiratory Coupling. Entropy 2020, 22, 1042. [Google Scholar] [CrossRef]
- Lazic, I.; Pernice, R.; Loncar-Turukalo, T.; Mijatovic, G.; Faes, L. Assessment of Cardiorespiratory Interactions during Apneic Events in Sleep via Fuzzy Kernel Measures of Information Dynamics. Entropy 2021, 23, 698. [Google Scholar] [CrossRef]
- Kalauzi, A.; Matić, Z.; Platiša, M.M.; Bojić, T. Two Operational Modes of Cardio-Respiratory Coupling Revealed by Pulse-Respiration Quotient. Bioengineering 2023, 10, 180. [Google Scholar] [CrossRef]
- Faes, L.; Porta, A.; Nollo, G. Information Decomposition in Bivariate Systems: Theory and Application to Cardiorespiratory Dynamics. Entropy 2015, 17, 277–303. [Google Scholar] [CrossRef]
- Xiong, W.; Faes, L.; Ivanov, P.C. Entropy measures, entropy estimators, and their performance in quantifying complex dynamics: Effects of artifacts, nonstationarity, and long-range correlations. Phys. Rev. E 2017, 95, 062114. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Porta, A.; Nollo, G.; Javorka, M. Information Decomposition in Multivariate Systems: Definitions, Implementation and Application to Cardiovascular Networks. Entropy 2016, 19, 5. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating causal relations by econometric models and cross-spectral methods. Econom. J. Econom. Soc. 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Barrett, A.B.; Barnett, L.; Seth, A.K. Multivariate Granger causality and generalized variance. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2010, 81 Pt 1, 041907. [Google Scholar] [CrossRef] [Green Version]
- Porta, A.; Faes, L. Wiener–Granger Causality in Network Physiology with Applications to Cardiovascular Control and Neuroscience. Proc. IEEE 2015, 104, 282–309. [Google Scholar] [CrossRef]
- Pernice, R.; Faes, L.; Feucht, M.; Benninger, F.; Mangione, S.; Schiecke, K. Pairwise and higher-order measures of brain-heart interactions in children with temporal lobe epilepsy. J. Neural Eng. 2022, 19, 045002. [Google Scholar] [CrossRef]
- Faes, L.; Nollo, G.; Porta, A. Information Decomposition: A Tool to Dissect Cardiovascular and Cardiorespiratory Complexity. In Complexity and Nonlinearity in Cardiovascular Signals; Springer: Cham, Switzerland, 2017; pp. 87–113. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Porta, A. Conditional Entropy-Based Evaluation of Information Dynamics in Physiological Systems. In Directed Information Measures in Neuroscience; Springer: Berlin/Heidelberg, Germany, 2014; pp. 61–86. [Google Scholar] [CrossRef]
- Porta, A.; Faes, L.; Nollo, G.; Bari, V.; Marchi, A.; De Maria, B.; Takahashi, A.C.M.; Catai, A.M. Conditional Self-Entropy and Conditional Joint Transfer Entropy in Heart Period Variability during Graded Postural Challenge. PLoS ONE 2015, 10, e0132851. [Google Scholar] [CrossRef] [Green Version]
- Radovanović, N.N.; Pavlović, S.U.; Milašinović, G.; Platiša, M.M. Effects of Cardiac Resynchronization Therapy on Cardio-Respiratory Coupling. Entropy 2021, 23, 1126. [Google Scholar] [CrossRef]
- Leyva, F.; Nisam, S.; Auricchio, A. 20 Years of Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2014, 64, 1047–1058. [Google Scholar] [CrossRef] [Green Version]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Dhesi, S.; Lockwood, E.; Sandhu, R.K. Troubleshooting Cardiac Resynchronization Therapy in Nonresponders. Can. J. Cardiol. 2017, 33, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Chakir, K.; Daya, S.K.; Aiba, T.; Tunin, R.S.; Dimaano, V.L.; Abraham, T.P.; Jaques-Robinson, K.M.; Lai, E.W.; Pacak, K.; Zhu, W.Z.; et al. Mechanisms of enhanced beta-adrenergic reserve from cardiac resynchronization therapy. Circulation 2009, 119, 1231–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMazumder, D.; Kass, D.A.; O’rourke, B.; Tomaselli, G.F. Cardiac Resynchronization Therapy Restores Sympathovagal Balance in the Failing Heart by Differential Remodeling of Cholinergic Signaling. Circ. Res. 2015, 116, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Daubert, C.; Behar, N.; Martins, R.P.; Mabo, P.; Leclercq, C. Avoiding non-responders to cardiac resynchronization therapy: A prac-tical guide. Eur. Heart J. 2017, 38, 1463–1472. [Google Scholar]
- Faes, L.; Nollo, G.; Porta, A. Compensated Transfer Entropy as a Tool for Reliably Estimating Information Transfer in Physiological Time Series. Entropy 2013, 15, 198–219. [Google Scholar] [CrossRef] [Green Version]
- Pernice, R.; Lazic, I.; Bara, C.; Sparacino, L.; Mijatovic, G.; Loncar-Turukalo, T.; Faes, L. Assessment of Cardiorespiratory Interactions During Spontaneous and Controlled Breathing: Non-linear Model-free Analysis. In Proceedings of the 2022 12th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO), Štrbské Pleso, Slovakia, 9–12 October 2022; pp. 1–2. [Google Scholar] [CrossRef]
- Geweke, J. Measurement of linear dependence and feedback between multiple time series. J. Am. Stat. Asso-Ciation 1982, 77, 304–313. [Google Scholar] [CrossRef]
- Schiatti, L.; Nollo, G.; Rossato, G.; Faes, L. Extended Granger causality: A new tool to identify the structure of physiological networks. Physiol. Meas. 2015, 36, 827–843. [Google Scholar] [CrossRef]
- Kozachenko, L.F.; Leonenko, N.N. Sample Estimate of the Entropy of a Random Vector. Probl. Peredachi Inf. 1987, 23, 9–16. [Google Scholar]
- Kraskov, A.; Stögbauer, H.; Grassberger, P. Estimating mutual information. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2004, 69, 066138, Erratum in 2011, 83, 019903. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Erla, S.; Nollo, G. Measuring Connectivity in Linear Multivariate Processes: Definitions, Interpretation, and Practical Analysis. Comput. Math. Methods Med. 2012, 2012, 140513. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Kugiumtzis, D.; Nollo, G.; Jurysta, F.; Marinazzo, D. Estimating the decomposition of predictive information in multivariate systems. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2015, 91, 032904. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Alvarez, B.; García-Seara, J.; Martínez-Sande, J.L.; Rodríguez-Mañero, M.; López, X.A.F.; González-Melchor, L.; Bermejo, R.M.A.; Iglesias-Alvarez, D.; Sampedro, F.G.; Díaz-Louzao, C.; et al. Cardiac resynchronization therapy outcomes in patients under nonoptimal medical therapy. J. Arrhythmia 2018, 34, 548–555. [Google Scholar] [CrossRef]
- Hori, M.; Okamoto, H. Heart rate as a target of treatment of chronic heart failure. J. Cardiol. 2012, 60, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Urso, C.; Brucculeri, S.; Caimi, G. Acid–base and electrolyte abnormalities in heart failure: Pathophysiology and implications. Heart Fail. Rev. 2015, 20, 493–503. [Google Scholar] [CrossRef] [Green Version]
- Forleo, G.B.; Santini, L.; Campoli, M.; Malavasi, M.; Scaccia, A.; Menichelli, M.; Riva, U.; Lamberti, F.; Carreras, G.; Orazi, S.; et al. Long-term monitoring of respiratory rate in patients with heart failure: The Multiparametric Heart Failure Evaluation in Implantable Cardioverter-Defibrillator Patients (MULTITUDE-HF) study. J. Interv. Card. Electrophysiol. 2015, 43, 135–144. [Google Scholar] [CrossRef]
- Seith, A.K. A MATLAB toolbox for Granger causal connectivity analysis. J. Neurosci. Methods 2010, 186, 262–273. [Google Scholar] [CrossRef]
- Nemati, S.; Edwards, B.A.; Lee, J.; Pittman-Polletta, B.; Butler, J.P.; Malhotra, A. Respiration and heart rate complexity: Effects of age and gender assessed by band-limited transfer entropy. Respir. Physiol. Neurobiol. 2013, 189, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Iatsenko, D.; Bernjak, A.; Stankovski, T.; Shiogai, Y.; Owen-Lynch, P.J.; Clarkson, P.B.M.; McClintock, P.V.E.; Stefanovska, A. Evolution of cardiorespiratory interactions with age. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20110622. [Google Scholar] [CrossRef] [Green Version]
- O’mahony, D.; Bennett, C.; Green, A.; Sinclair, A. Reduced baroreflex sensitivity in elderly humans is not due to efferent autonomic dysfunction. Clin. Sci. 2000, 98, 103. [Google Scholar] [CrossRef]
- Gerritsen, J.; TenVoorde, B.J.; Dekker, J.M.; Kostense, P.J.; Bouter, L.M.; Heethaar, R.M. Baroreflex sensitivity in the elderly: Influence of age, breathing and spectral methods. Clin. Sci. 2000, 99, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Breston, L.; Leonardis, E.J.; Quinn, L.K.; Tolston, M.; Wiles, J.; Chiba, A.A. Convergent cross sorting for estimating dynamic coupling. Sci. Rep. 2021, 11, 20374. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, D.; Montalto, A.; Vlemincx, E.; Marinazzo, D.; Van Huffel, S.; Faes, L. Cardiorespiratory Information Dynamics during Mental Arithmetic and Sustained Attention. PLoS ONE 2015, 10, e0129112. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Baseline (×103) | Follow-Up (×103) | p (Baseline vs. F-Up) |
|---|---|---|---|
| HFSin (N = 14; 71% R) | 1.31 ± 0.18 | 1.22 ± 0.19 | 0.124 |
| HFVES1 (N = 11; 64% R) | 1.34 ± 0.29 | 1.25 ± 0.22 | 0.131 |
| HFVES2 (N = 14; 57% R) | 1.49 ± 0.18 | 1.30 ± 0.17 | 0.008 |
| p (Among groups) | 0.061 | 0.469 | |
| Responders (N = 25) | 1.43 ± 0.22 | 1.28 ± 0.18 | 0.007 |
| Non-Responders (N = 14) | 1.30 ± 0.22 | 1.22 ± 0.21 | 0.090 |
| p (Resp. vs. Non-Resp.) | 0.118 | 0.149 |
| HF Groups | CRT Groups | |||||
|---|---|---|---|---|---|---|
| Condition | HFSin | HFVES1 | HFVES2 | Responders | Non-Responders | |
| RR [s] | Baseline | 0.930 ± 0.032 ττ | 0.932 ± 0.054 | 0.813 ± 0.026 ** | 0.857 ± 0.027 * | 0.943 ± 0.040 |
| Follow-up | 1.010 ± 0.053 | 0.99± 0.40 | 0.934 ± 0.031 | 0.959 ± 0.036 | 1.007 ± 0.051 | |
| BB [s] | Baseline | 4.25 ± 0.38 | 3.82 ± 0.27 | 3.40 ± 0.13 | 4.01 ± 0.24 * | 3.49 ± 0.14 |
| Follow-up | 4.30 ± 0.39 | 3.96 ± 0.37 | 3.65 ± 0.21 | 4.32 ± 0.26 # | 3.35 ± 0.14 | |
| Baseline | Follow-Up | |||||
|---|---|---|---|---|---|---|
| HFSin vs. HFVES1 | HFSin vs. HFVES2 | HFVES1 vs. HFVES2 | HFSin vs. HFVES1 | HFSin vs. HFVES2 | HFVES1 vs. HFVES2 | |
| GC(Resp-RR) | 0.432 | 0.001 | 0.002 | 0.013 | 0.004 | 0.751 |
| GC(RR-Resp) | 0.297 | 0.001 | 0.001 | 0.212 | 0.012 | 0.527 |
| TE(Resp-RR) | 0.572 | 0.635 | 0.165 | 0.080 | 0.246 | 0.681 |
| TE(RR-Resp) | 0.181 | 0.137 | 0.005 | 1.000 | 0.946 | 0.918 |
| CE(Resp-RR) | 0.258 | 0.131 | 0.123 | 0.440 | 0.781 | 0.758 |
| CE(RR-Resp) | 0.643 | 0.274 | 0.258 | 0.411 | 0.980 | 0.957 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Platiša, M.M.; Radovanović, N.N.; Pernice, R.; Barà, C.; Pavlović, S.U.; Faes, L. Information-Theoretic Analysis of Cardio-Respiratory Interactions in Heart Failure Patients: Effects of Arrhythmias and Cardiac Resynchronization Therapy. Entropy 2023, 25, 1072. https://doi.org/10.3390/e25071072
Platiša MM, Radovanović NN, Pernice R, Barà C, Pavlović SU, Faes L. Information-Theoretic Analysis of Cardio-Respiratory Interactions in Heart Failure Patients: Effects of Arrhythmias and Cardiac Resynchronization Therapy. Entropy. 2023; 25(7):1072. https://doi.org/10.3390/e25071072
Chicago/Turabian StylePlatiša, Mirjana M., Nikola N. Radovanović, Riccardo Pernice, Chiara Barà, Siniša U. Pavlović, and Luca Faes. 2023. "Information-Theoretic Analysis of Cardio-Respiratory Interactions in Heart Failure Patients: Effects of Arrhythmias and Cardiac Resynchronization Therapy" Entropy 25, no. 7: 1072. https://doi.org/10.3390/e25071072