
First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. FDG/PET Imaging
2.3. Hypoxia PET Imaging
2.4. Qualitative and Quantitative Analysis
2.5. Parametric Imaging Method
2.6. Immunohistochemistry Analysis
2.7. Staining Assessment
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
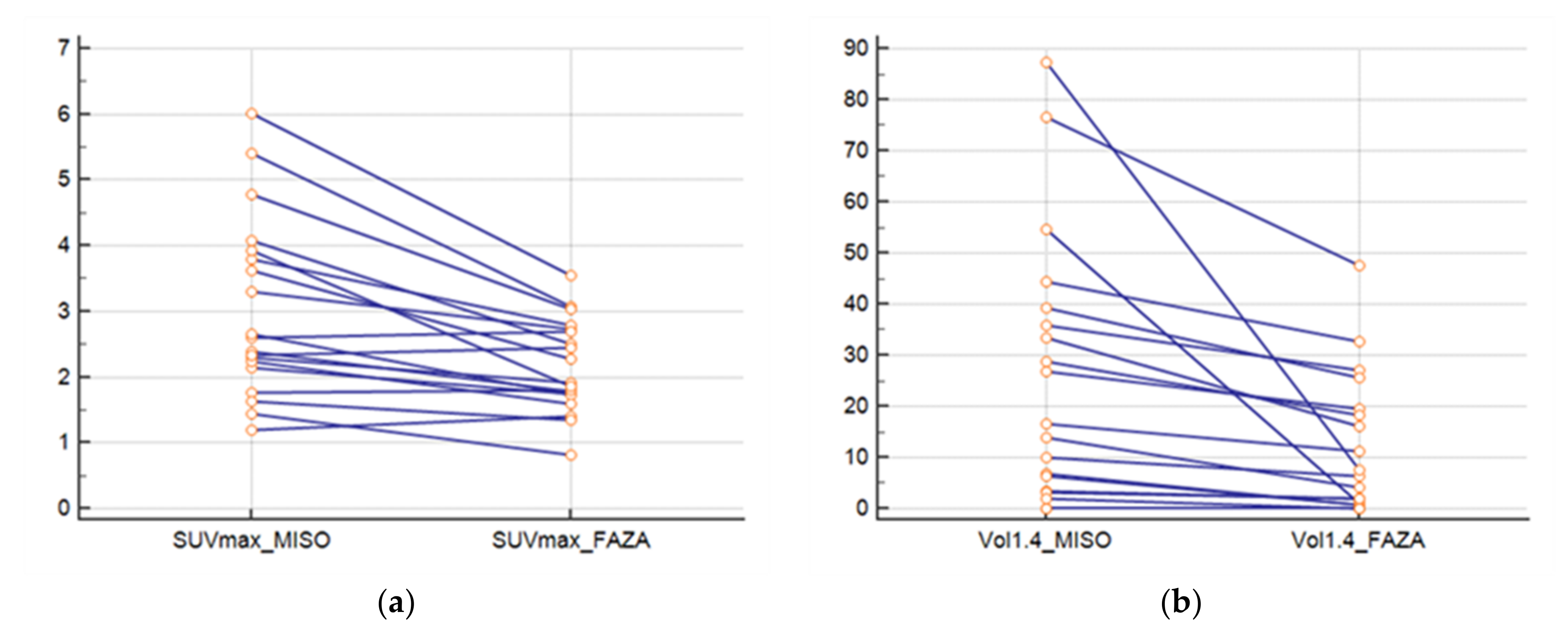
4.2. PET Results
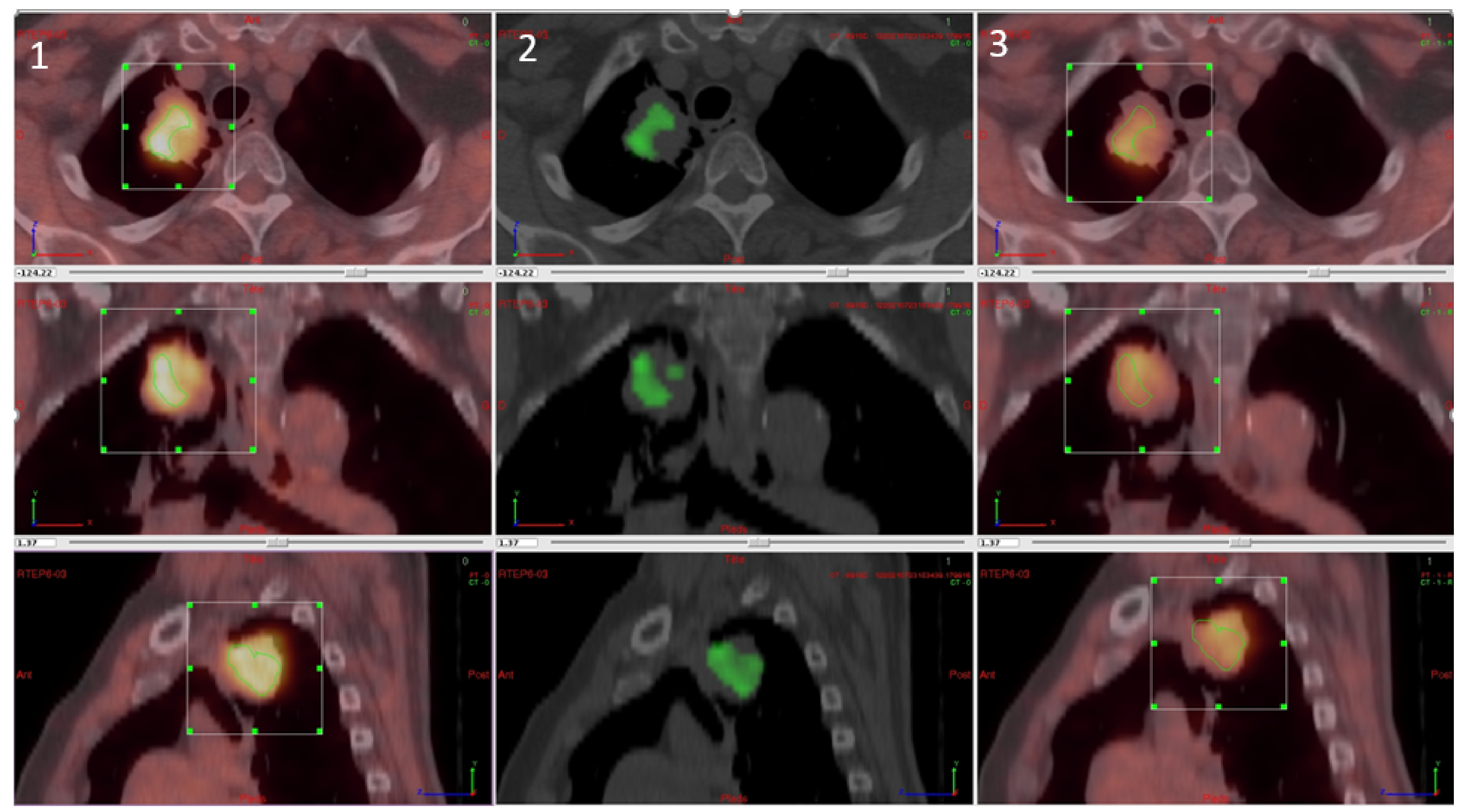
4.3. Overlap Fraction, Parametric Results, and Immunohistochemistry Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| DI | Dice index |
| FAZA | fluorine-18-fluoroazomycin-arabinoside |
| FMISO | fluorine-18-misonidazole |
| FDG | fluorodeoxyglucose |
| JI | Jaccard index |
| SUVmax | maximum standardised uptake value |
| NSCLC | non-small cell lung cancer |
| PET/CT | positron emission tomography/computed tomography |
| VOI | volume of interest |
References
- Cherk, M.H.; Foo, S.S.; Poon, A.M.; Knight, S.R.; Murone, C.; Papenfuss, A.T.; Sachinidis, J.I.; Saunder, T.H.; O’Keefe, G.J.; Scott, A.M. Lack of correlation of hypoxic cell fraction and angiogenesis with glucose metabolic rate in non-small cell lung cancer assessed by 18F-fluoromisonidazole and 18F-FDG PET. J. Nucl. Med. 2006, 47, 1921–1926. [Google Scholar]
- Lewis, J.S.; Welch, M.J. PET imaging of hypoxia. Q. J. Nucl. Med. 2001, 45, 183–188. [Google Scholar]
- Rischin, D.; Fisher, R.; Peters, L.; Corry, J.; Hicks, R. Hypoxia in Head and Neck Cancer: Studies with Hypoxic Positron Emission Tomography Imaging and Hypoxic Cytotoxins. Int. J. Radiat. Oncol. 2007, 69, S61–S63. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, J. Hypoxic Radiosensitization: Adored and Ignored. J. Clin. Oncol. 2007, 25, 4066–4074. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, L.S.; Buus, S.; Nordsmark, M.; Bentzen, L.; Munk, O.L.; Keiding, S.; Overgaard, J. Identifying hypoxia in human tumors: A correlation study between18F-FMISO PET and the Eppendorf oxygen-sensitive electrode. Acta Oncol. 2010, 49, 934–940. [Google Scholar] [CrossRef]
- Gagel, B.; Reinartz, P.; Dimartino, E.; Zimny, M.; Pinkawa, M.; Maneschi, P.; Stanzel, S.; Hamacher, K.; Coenen, H.H.; Westhofen, M.; et al. pO(2) Polarography versus positron emission tomography ([(18)F] fluoromisonidazole, [(18)F]-2-fluoro-2’-deoxyglucose). An appraisal of radiotherapeutically relevant hypoxia. Strahlenther Onkol. 2004, 180, 616–622. [Google Scholar] [CrossRef]
- Sanduleanu, S.; Van Der Wiel, A.M.A.; Lieverse, R.I.Y.; Marcus, D.; Ibrahim, A.; Primakov, S.; Wu, G.; Theys, J.; Yaromina, A.; Dubois, L.J.; et al. Hypoxia PET Imaging with [18F]-HX4—A Promising Next-Generation Tracer. Cancers 2020, 12, 1322. [Google Scholar] [CrossRef]
- Challapalli, A.; Carroll, L.; Aboagye, E.O. Molecular mechanisms of hypoxia in cancer. Clin. Transl. Imaging 2017, 5, 225–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschmann, S.M.; Paulsen, F.; Reimold, M.; Dittmann, H.; Welz, S.; Reischl, G.; Machulla, H.J.; Bares, R. Prognostic impact of hypoxia imaging with 18F-misonidazole PET in non-small cell lung cancer and head and neck cancer before radiotherapy. J. Nucl. Med. 2005, 46, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Fujii, H.; Hayashi, Y.; Kamiyama, I.; Ohtsuka, T.; Asamura, H. Prognostic significance of hypoxic PET using 18 F-FAZA and 62 Cu-ATSM in non-small-cell lung cancer. Lung Cancer 2015, 91, 56–66. [Google Scholar] [CrossRef]
- Bollineni, V.R.; Koole, M.; Pruim, J.; Brouwer, C.L.; Wiegman, E.M.; Groen, H.J.; Vlasman, R.; Halmos, G.B.; Oosting, S.F.; Langendijk, J.A.; et al. Dynamics of tumor hypoxia assessed by 18F-FAZA PET/CT in head and neck and lung cancer patients during chemoradiation: Possible implications for radiotherapy treatment planning strategies. Radiother. Oncol. 2014, 113, 198–203. [Google Scholar] [CrossRef]
- Vera, P.; Thureau, S.; Chaumet-Riffaud, P.; Modzelewski, R.; Bohn, P.; Vermandel, M.; Hapdey, S.; Pallardy, A.; Mahé, M.-A.; Lacombe, M.; et al. Phase II Study of a Radiotherapy Total Dose Increase in Hypoxic Lesions Identified by 18F-Misonidazole PET/CT in Patients with Non–Small Cell Lung Carcinoma (RTEP5 Study). J. Nucl. Med. 2017, 58, 1045–1053. [Google Scholar] [CrossRef] [Green Version]
- Di Perri, D.; Lee, J.A.; Bol, A.; Hanin, F.-X.; Janssens, G.; LaBar, D.; Robert, A.; Sterpin, E.; Geets, X. Evolution of [18F]fluorodeoxyglucose and [18F]fluoroazomycin arabinoside PET uptake distributions in lung tumours during radiation therapy. Acta Oncol. 2017, 56, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thureau, S.; Chaumet-Riffaud, P.; Modzelewski, R.; Fernandez, P.; Tessonnier, L.; Vervueren, L.; Cachin, F.; Berriolo-Riedinger, A.; Olivier, P.; Kolesnikov-Gauthier, H.; et al. Interobserver Agreement of Qualitative Analysis and Tumor Delineation of 18F-Fluoromisonidazole and 3’-Deoxy-3’-18F-Fluorothymidine PET Images in Lung Cancer. J. Nucl. Med. 2013, 54, 1543–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopci, E.; Grassi, I.; Chiti, A.; Nanni, C.; Cicoria, G.; Toschi, L.; Fonti, C.; Lodi, F.; Mattioli, S.; Fanti, S. PET radiopharmaceuticals for imaging of tumor hypoxia: A review of the evidence. Am. J. Nucl. Med. Mol. Imaging 2014, 4, 365–384. [Google Scholar] [PubMed]
- Wei, Y.; Zhao, W.; Huang, Y.; Yu, Q.; Zhu, S.; Wang, S.; Zhao, S.; Hu, X.; Yu, J.; Yuan, S. A Comparative Study of Noninvasive Hypoxia Imaging with 18F-Fluoroerythronitroimidazole and 18F-Fluoromisonidazole PET/CT in Patients with Lung Cancer. PLoS ONE 2016, 11, e0157606. [Google Scholar] [CrossRef]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analy-sis. Mod. Pathol 1998, 11, 155–168. [Google Scholar] [PubMed]
- Bollineni, V.R.; Kerner, G.; Pruim, J.; Steenbakkers, R.J.; Wiegman, E.M.; Koole, M.J.; de Groot, E.H.; Willemsen, A.T.; Luurtsema, G.; Widder, J.; et al. PET Imaging of Tumor Hypoxia Using 18F-Fluoroazomycin Arabinoside in Stage III–IV Non–Small Cell Lung Cancer Patients. J. Nucl. Med. 2013, 54, 1175–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerner, G.S.M.A.; Bollineni, V.R.; Hiltermann, T.J.N.; Sijtsema, N.M.; Fischer, A.; Bongaerts, A.H.H.; Pruim, J.; Groen, H.J.M. An exploratory study of volumetric analysis for assessing tumor response with 18F-FAZA PET/CT in patients with advanced non-small-cell lung cancer (NSCLC). EJNMMI Res. 2016, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Saga, T.; Inubushi, M.; Koizumi, M.; Yoshikawa, K.; Zhang, M.; Tanimoto, K.; Horiike, A.; Yanagitani, N.; Ohyanagi, F.; Nishio, M. Prognostic value of 18 F-fluoroazomycin arabinoside PET / CT in patients with advanced non-small-cell lung cancer. Cancer Sci. 2015, 106, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Supiot, S.; Rousseau, C.; Dore, M.; Le-Rest, C.C.-; Kandel-Aznar, C.; Potiron, V.; Guerif, S.; Paris, F.; Ferrer, L.; Campion, L.; et al. Evaluation of tumor hypoxia prior to radiotherapy in intermediate-risk prostate cancer using 18F-fluoromisonidazole PET/CT: A pilot study. Oncotarget 2018, 9, 10005–10015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, J.; Kitagawa, Y.; Watanabe, S.; Asaka, T.; Ohga, N.; Hirata, K.; Okamoto, S.; Shiga, T.; Shindoh, M.; Kuge, Y.; et al. 18 F-Fluoromisonidazole positron emission tomography (FMISO-PET) may reflect hypoxia and cell proliferation activity in oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 261–270. [Google Scholar] [CrossRef]
- Bekaert, L.; Valable, S.; Lechapt-Zalcman, E.; Ponte, K.; Collet, S.; Constans, J.-M.; Levallet, G.; Bordji, K.; Petit, E.; Branger, P.; et al. [18F]-FMISO PET study of hypoxia in gliomas before surgery: Correlation with molecular markers of hypoxia and angiogenesis. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- Zschaeck, S.; Löck, S.; Hofheinz, F.; Zips, D.; Mortensen, L.S.; Zöphel, K.; Troost, E.G.; Boeke, S.; Saksø, M.; Mönnich, D.; et al. Individual patient data meta-analysis of FMISO and FAZA hypoxia PET scans from head and neck cancer patients undergoing definitive radio-chemotherapy. Radiother. Oncol. 2020, 149, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Rischin, D.; Hicks, R.; Fisher, R.; Binns, D.; Corry, J.; Porceddu, S.; Peters, L.J. Prognostic Significance of [18F]-Misonidazole Positron Emission Tomography–Detected Tumor Hypoxia in Patients With Advanced Head and Neck Cancer Randomly Assigned to Chemoradiation With or Without Tirapazamine: A Substudy of Trans-Tasman Radiation Oncology Group Study 98.02. J. Clin. Oncol. 2006, 24, 2098–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorwarth, D.; Eschmann, S.-M.; Holzner, F.; Paulsen, F.; Alber, M. Combined uptake of [18F]FDG and [18F]FMISO correlates with radiation therapy outcome in head-and-neck cancer patients. Radiother. Oncol. 2006, 80, 151–156. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, L.B.; Bollineni, V.R.; Wachters, J.E.; Schuuring, E.; Van Hemel, B.M.; Van Der Wal, J.E.; Slagter-Menkema, L.; De Bock, G.H.; Steenbakkers, R.J.; Langendijk, J.A.; et al. Assessment of hypoxic subvolumes in laryngeal cancer with 18F-fluoroazomycinarabinoside (18F-FAZA)-PET/CT scanning and immunohistochemistry. Radiother. Oncol. 2015, 117, 106–112. [Google Scholar] [CrossRef]
- Garcia-Parra, R.; Wood, D.; Shah, R.B.; Siddiqui, J.; Hussain, H.; Park, H.; Desmond, T.; Meyer, C.; Piert, M. Investigation on tumor hypoxia in resectable primary prostate cancer as demonstrated by 18F-FAZA PET/CT utilizing multimodality fusion techniques. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1816–1823. [Google Scholar] [CrossRef] [Green Version]
- Norikane, T.; Yamamoto, Y.; Maeda, Y.; Kudomi, N.; Matsunaga, T.; Haba, R.; Iwasaki, A.; Hoshikawa, H.; Nishiyama, Y. Correlation of 18F-fluoromisonidazole PET findings with HIF-1α and p53 expressions in head and neck cancer. Nucl. Med. Commun. 2014, 35, 30–35. [Google Scholar] [CrossRef]
- Mapelli, P.; Bettinardi, V.; Fallanca, F.; Incerti, E.; Compierchio, A.; Rossetti, F.; Coliva, A.; Savi, A.; Doglioni, C.; Negri, G.; et al. 18F-FAZA PET/CT in the Preoperative Evaluation of NSCLC: Comparison with 18F-FDG and Immunohistochemistry. Curr. Radiopharm. 2018, 11, 50–57. [Google Scholar] [CrossRef]
- Kawai, N.; Lin, W.; Cao, W.-D.; Ogawa, D.; Miyake, K.; Haba, R.; Maeda, Y.; Yamamoto, Y.; Nishiyama, Y.; Tamiya, T. Correlation between 18F-fluoromisonidazole PET and expression of HIF-1α and VEGF in newly diagnosed and recurrent malignant gliomas. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1870–1878. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, H.; Harris, A.L. Advances in Hypoxia-Inducible Factor Biology. Cell Metab. 2018, 27, 281–298. [Google Scholar] [CrossRef] [PubMed]
- Linehan, W.M.; Rouault, T.A. Molecular pathways: Fumarate hydratase-deficient kidney cancer—Argeting the Warburg effect in cancer. Clin. Cancer Res. 2013, 19, 3345–3352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaluz, S.; Kaluzová, M.; Liao, S.-Y.; Lerman, M.; Stanbridge, E.J. Transcriptional control of the tumor- and hypoxia-marker carbonic anhydrase 9: A one transcription factor (HIF-1) show? Biochim. Biophys. Acta BBA Bioenergy 2009, 1795, 162–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holbrook, J.J.; Liljas, A.; Steindel, S.J.; Rossman, M.G. Lactate dehydrogenase. In The Enzymes, 3rd ed.; Boyer, P.D., Ed.; Academic Press: New York, NY, USA, 1975; Volume XI, pp. 191–292. [Google Scholar]
- Semenza, G.L.; Jiang, B.H.; Leung, S.W.; Passantino, R.; Concordet, J.P.; Maire, P.; Giallongo, A. Hypoxia response elements in the aldolase A, enolase 1, and lactate dehydrogenase A gene promoters contain essential binding sites for hypox-ia-inducible factor 1. J. Biol Chem. 1996, 271, 32529–32537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopci, E.; Toschi, L.; Grizzi, F.; Rahal, D.; Olivari, L.; Castino, G.F.; Marchetti, S.; Cortese, N.; Qehajaj, D.; Alloisio, M.; et al. Correlation of metabolic information on FDG-PET with tissue expression of immune markers in patients with non-small cell lung cancer (NSCLC) who are candidates for upfront surgery. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, N.; Kaira, K.; Bao, P.; Higuchi, T.; Arisaka, Y.; Erkhem-Ochir, B.; Sunaga, N.; Ohtaki, Y.; Yajima, T.; Kosaka, T.; et al. Correlation of tumor-related immunity with 18F-FDG-PET in pulmonary squamous-cell carcinoma. Lung Cancer 2018, 119, 71–77. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | Stade | Pathology | Delay | SUVmax | |||
|---|---|---|---|---|---|---|---|---|---|
| FAZA/FMISO | PET/Surgery | FDG | FMISO | FAZA | |||||
| 1 | M | 78 | T2bN1 | SCC | 6 | 3 | 12.12 | 2.39 | 1.79 |
| 2 | M | 57 | T2aN0 | ADK | 1 | 1 | 5.34 | 2.15 | 1.74 |
| 3 | W | 64 | T2aN0 | ADK | 1 | 1 | 11.33 | 6.02 | 3.54 |
| 4 | M | 76 | T3N0 | SCC | 2 | 2 | 26.97 | 3.31 | 2.74 |
| 5 | W | 65 | T4N1 | SCC | 1 | 5 | 21.56 | 3.79 | 2.78 |
| 6 | M | 65 | T4N0 | SCC | 1 | 1 | 10.03 | 2.6 | 2.7 |
| 7 | M | 67 | T3N1 | SCC | 1 | 1 | 7.3 | 2.65 | 1.72 |
| 8 | M | 75 | T2aN0 | ADK | 6 | 3 | 8.72 | 2.3 | 1.91 |
| 9 | M | 59 | T2aN2 | SCC | 1 | 9 | 15.93 | 2.24 | 1.6 |
| 10 | M | 66 | T2bN0 | SCC | 1 | 6 | 15.21 | 4.08 | 2.5 |
| 11 | M | 69 | T2bN2 | ADK | 1 | 10 | 11.67 | 5.4 | 3.07 |
| 12 | W | 77 | T2bN2 | ADK | 1 | 2 | 9.92 | 2.46 | 2.29 |
| 13 | M | 75 | T1cN1 | SCC | 2 | 1 | 5.32 | 1.2 | 1.75 |
| 14 | M | 63 | T2aN0 | ADK | 1 | 1 | 15.45 | 1.77 | 1.81 |
| 15 | W | 51 | T3N2 | ADK | 3 | 3 | 7.96 | 1.64 | 1.34 |
| 16 | M | 65 | T1cN0 | ADK | 3 | 4 | 10.38 | 1.44 | 0.82 |
| 17 | M | 68 | T4N0 | SCC | 3 | 1 | 9.5 | 3.92 | 1.85 |
| 18 | M | 83 | T3N0 | SCC | 3 | 1 | 12.95 | 3.63 | 2.28 |
| 19 | M | 72 | T2aN0 | ADK | 3 | 2 | 15.60 | 4.78 | 3.03 |
| Mean | 68.2 | 2.1 | 3.1 | 12.4 | 3.0 | 2.2 | |||
| SE | 8.2 | 1.6 | 2.8 | 5.5 | 1.4 | 0.7 | |||
| Patient | GLUT1 | (SE) | LDH5 | (SE) | HIF1 | (SE) | CAIX | (SE) |
|---|---|---|---|---|---|---|---|---|
| 1 | 290.0 | (17.3) | 271.7 | (40.7) | 113.3 | (28.9) | 13.3 | (2.9) |
| 2 | 63.3 | (25.2) | 260.0 | (69.3) | 15.0 | (15.0) | 36.7 | (5.8) |
| 3 | 170.0 | (11.5) | 250.0 | (17.3) | 3.3 | (2.9) | 0.0 | (0.0) |
| 4 | 283.3 | (28.9) | 250.0 | (43.6) | 65.0 | (15.0) | 226.7 | (68.1) |
| 5 | 191.7 | (45.4) | 286.7 | (11.5) | 1.7 | (2.9) | 40.0 | (36.1) |
| 6 | 198.3 | (31.7) | 290. | (17.3) | 140.0 | (32.8) | 161.7 | (59.6) |
| 7 | 273.3 | (15.3) | 293.3 | (11.5) | 180.0 | (55.7) | 130.0 | (10.0) |
| 8 | 160.0 | (34.6) | 273.3 | (25.2) | 68.3 | (46.5) | 8.3 | (10.4) |
| 9 | 288.3 | (20.2) | 293.3 | (11.5) | 81.7 | (46.5) | 43.3 | (2.9) |
| 10 | 256.7 | (15.3) | 201.7 | (122.1) | 0.0 | (0.0) | 33.3 | (16.1) |
| 11 | 196.7 | (51.3) | 290.0 | (10.0) | 131.7 | (86.1) | 3.3 | (5.8) |
| 12 | 131.7 | (27.5) | 196.7 | (45.1) | 71.7 | (43.1) | 8.3 | (7.6) |
| 13 | 290.0 | (10.0) | 300.0 | (0.0) | 66.67 | (55.1) | 106.7 | (28.9) |
| 14 | 100.0 | (173.2) | 266.7 | (57.7) | 5.0 | (8.7) | 73.3 | (66.6) |
| 15 | 263.3 | (47.3) | 293.3 | (11.5) | 145.0 | (48.2) | 26.7 | (20.8) |
| 16 | 263.3 | (15.3) | 283.3 | (20.8) | 196.7 | (73.7) | 5.0 | (5.0) |
| 17 | 296.7 | (5.8) | 317.5 | (32.5) | 96.7 | (25.2) | 2.5 | (2.5) |
| 18 | 298.3 | (2.9) | 298.3 | (2.9) | 1.7 | (2.9) | 145.0 | (18.0) |
| 19 | 106.7 | (57.7) | 293.3 | (11.5) | 53.3 | (28.4) | 3.3 | (2.9) |
| Mean | 216.9 | (33.5) | 263.6 | (29.6) | 79.6 | (32.5) | 56.2 | (19.5) |
| SE | 76.7 | 60.4 | 53.3 | 64.0 |
| F | CAIX | LDH5 | GLUT1 | HIF1 | ||||
|---|---|---|---|---|---|---|---|---|
| ρ | p-value | ρ | p-value | ρ | p-value | ρ | p-value | |
| SUVmax FMISO | −0.32 | 0.17 | −0.08 | 0.74 | −0.04 | 0.87 | −0.35 | 0.14 |
| SUVmax FAZA | −0.21 | 0.40 | −0.32 | 0.18 | −0.35 | 0.15 | −0.47 | 0.04 |
| Volume 1.4 FMISO | 0.06 | 0.79 | 0.07 | 0.77 | 0.19 | 0.43 | −0.03 | 0.89 |
| Volume 1.4 FAZA | 0.03 | 0.89 | −0.26 | 0.28 | −0.09 | 0.71 | −0.36 | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thureau, S.; Piton, N.; Gouel, P.; Modzelewski, R.; Dujon, A.; Baste, J.-M.; Melki, J.; Rinieri, P.; Peillon, C.; Rastelli, O.; et al. First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer. Cancers 2021, 13, 4101. https://doi.org/10.3390/cancers13164101
Thureau S, Piton N, Gouel P, Modzelewski R, Dujon A, Baste J-M, Melki J, Rinieri P, Peillon C, Rastelli O, et al. First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer. Cancers. 2021; 13(16):4101. https://doi.org/10.3390/cancers13164101
Chicago/Turabian StyleThureau, Sébastien, Nicolas Piton, Pierrick Gouel, Romain Modzelewski, Antoine Dujon, Jean-Marc Baste, Jean Melki, Philippe Rinieri, Christophe Peillon, Olivier Rastelli, and et al. 2021. "First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer" Cancers 13, no. 16: 4101. https://doi.org/10.3390/cancers13164101
APA StyleThureau, S., Piton, N., Gouel, P., Modzelewski, R., Dujon, A., Baste, J.-M., Melki, J., Rinieri, P., Peillon, C., Rastelli, O., Lequesne, J., Hapdey, S., Sabourin, J.-C., Bohn, P., & Vera, P. (2021). First Comparison between [18f]-FMISO and [18f]-Faza for Preoperative Pet Imaging of Hypoxia in Lung Cancer. Cancers, 13(16), 4101. https://doi.org/10.3390/cancers13164101