
Pleiotropic Activity of Metformin and Its Sulfonamide Derivatives on Vascular and Platelet Haemostasis

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Cell Viability Studies
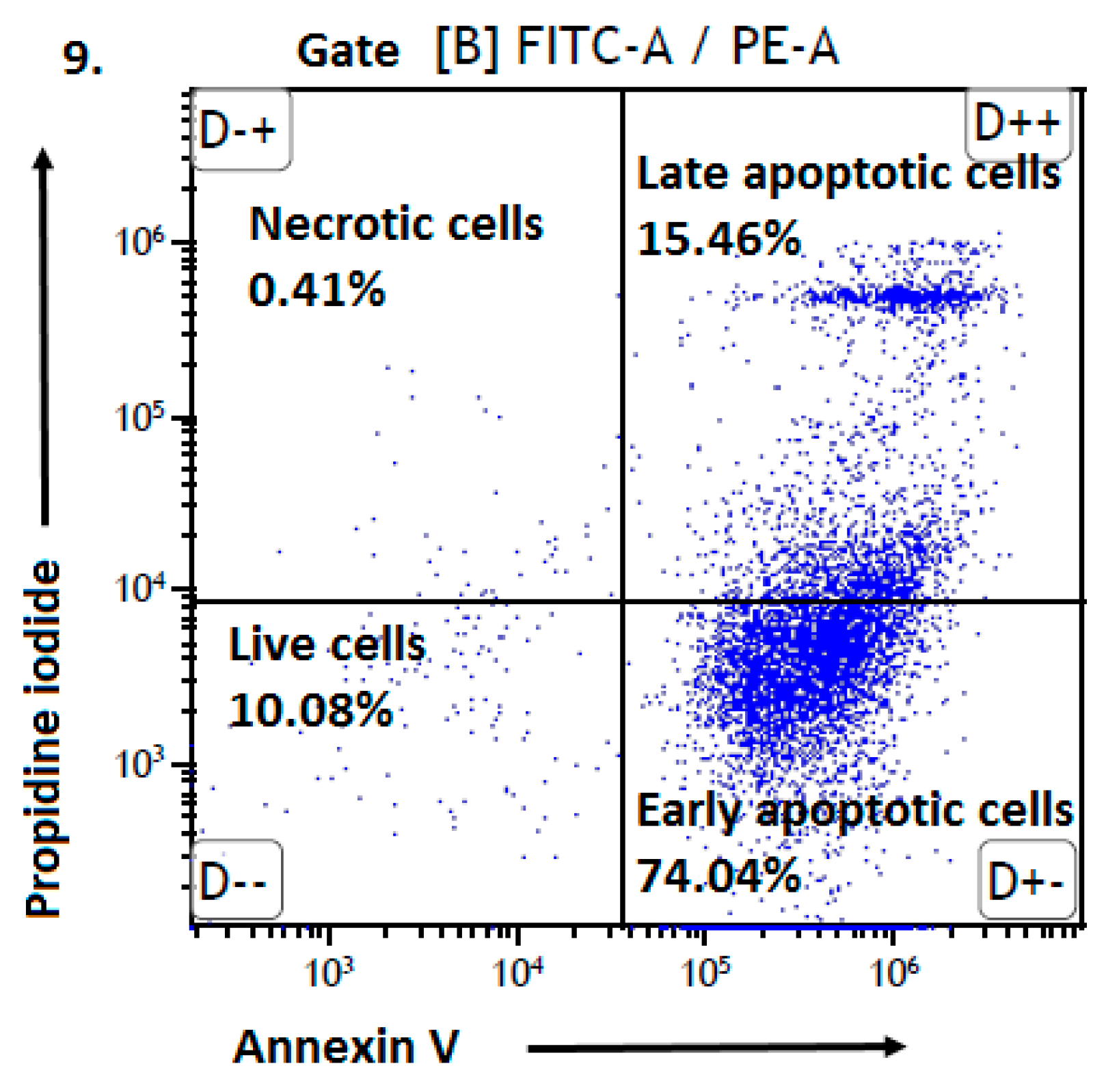
2.2. Apoptosis
2.3. Migration Test
2.4. Effects on ICAM-1 Expression
2.5. Platelet Aggregation
2.6. Platelet Adhesion
3. Materials and Methods
3.1. Materials
3.2. HUVEC and AoSMC Cells Subculturing
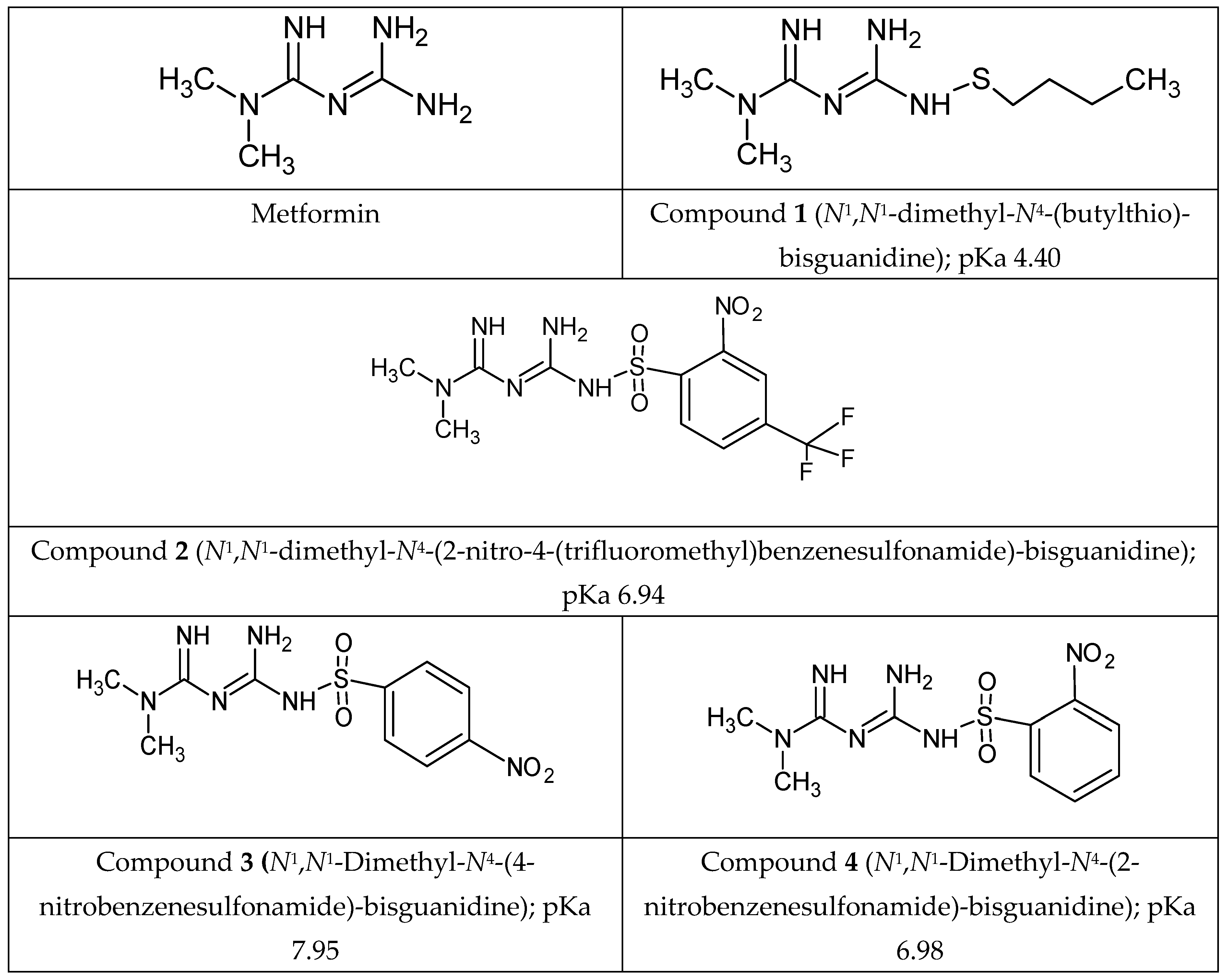
3.3. Tested Compounds
3.4. Cell Viability Studies
3.5. AoSMCs Apoptosis
3.6. Migration Test
3.7. ICAM Expression on AoSMCs Surface
3.8. Platelet Rich Plasma (PRP) for the Measurements of Platelets Aggregation and Adhesion
3.9. Platelet Aggregation Assay
3.10. Platelet Adhesion Assay
3.11. Statistical Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Markowicz-Piasecka, M.; Huttunen, K.M.; Mateusiak, L.; Mikiciuk-Olasik, E.; Sikora, J. Is Metformin a Perfect Drug? Updates in Pharmacokinetics and Pharmacodynamics. Curr. Pharm. Des. 2017, 23, 2532–2550. [Google Scholar] [CrossRef] [PubMed]
- Lipinski, B.; Pretorius, E. Novel pathway of iron-induced blood coagulation: Implications for diabetes mellitus and its complications. Pol. Arch. Intern. Med. 2012, 122, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Soma, P.; Swanepoel, A.C.; Noel, J.; Mqoco, T.; Pretorius, E. Flow cytometric analysis of platelets type 2 diabetes mellitus reveals ‘ angry ’ platelets. Cardiovasc. Diabetol. 2016, 15, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabit, C.E.; Chung, W.B.; Hamburg, N.M.; Vita, J.A. Endothelial dysfunction in diabetes mellitus: Molecular mechanisms and clinical implications. Rev. Endocr. Metab. Disord. 2010, 11, 61–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grzybowska, M.; Bober, J.; Olszewska, M. Metformin—Mechanisms of action and use for the treatment of type 2 diabetes mellitus. Postep. Hig. Med. Dosw. 2011, 65, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, K.; Naeem, M.; Ali, N. European Journal of Internal Medicine Metformin: The hidden chronicles of a magic drug. Eur. J. Intern. Med. 2013, 24, 20–26. [Google Scholar] [CrossRef]
- Ma, T.C.; Carrier, R.L.; Buescher, J.L.; Oatis, B.; Funk, J.A.; Nash, A.J. Metformin therapy in a transgenicmousemodel ofHuntington’s disease. Neurosci. Lett. 2007, 411, 98–103. [Google Scholar] [CrossRef]
- Adak, T.; Samadi, A.; Ünal, A.Z.; Sabuncuoğlu, S. A reappraisal on metformin, Regul. Toxicol. Pharmacol. 2018, 92, 324–332. [Google Scholar]
- Evans, J.M.M.; Donnelly, L.A.; Emslie-Smith, A.M.; Alessi, D.R.; Morris, A.D. Metformin and reduced risk of cancer in diabetic patients. BMJ 2005, 330, 1304–1305. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C.J. Metformin: Historical overview. Diabetologia 2017, 60, 1566–1576. [Google Scholar] [CrossRef] [Green Version]
- UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998, 352, 854–865. [Google Scholar] [CrossRef]
- Fernandez-Esteban, I.; Mataix, A.; Segura, M.A.; I Figuls, M.R.; Moher, D. Metformin monotherapy for type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2005, 20, CD002966. [Google Scholar]
- Mannucci, E.; Lamanna, C.; Monami, M.; Marchionni, N. Effect of metformin on cardiovascular events and mortality: A meta-analysis of randomized clinical trials. Diabetes Obes. Metab. 2011, 13, 221–228. [Google Scholar]
- Holmes, C.; Powell, L.; Clarke, N.S.; Jessen, M.E.; Pelts, M. Influence of metformin and insulin on myocardial substrate oxidation under conditions encoutnered during cardiac surgery. Surgery. 2018, 163, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Nesti, L.; Natali, A. Metformin effects on the heart and the cardiovascular system: A review of experimental and clinical data. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 657–669. [Google Scholar] [CrossRef]
- Grant, P. Beneficial effects of metformin on haemostasis and vascular function in man. Diabetes Metab. 2003, 29, 6S44–6S52. [Google Scholar] [CrossRef]
- Petersen, J.S.; DiBona, G.F. Acute Sympathoinhibitory Actions of Metformin in Spontaneously Hypertensive Rats. Hypertension 1996, 27, 619–625. [Google Scholar] [CrossRef]
- Yang, Q.; Yuan, H.; Chen, M.; Qu, J.; Wang, H.; Yu, B.; Chen, J.; Sun, S.; Tang, X.; Ren, W. Metformin ameliorates the progression of atherosclerosis via suppressing macrophage infiltration and inflammatory responses in rabbits. Life Sci. 2018, 198, 56–64. [Google Scholar] [CrossRef]
- Cefalu, W.T.; Schneider, D.J.; Carlson, H.E.; Migdal, P.; Lim, L.G.; Izon, M.P.; Kapoor, A.; Bell-Farrow, A.; Terry, J.G.; Sobel, B.E. Effect of combination glipizide GITS/metformin on fibrinolytic and metabolic parameters in poorly controlled type 2 diabetic subjects. Diabetes Care 2002, 25, 2123–2128. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Mamputu, J.-C.; Wiernsperger, N.; Renier, G. Signaling pathways involved in human vascular smooth muscle cell proliferation and matrix metalloproteinase-2 expression induced by leptin: Inhibitory effect of metformin. Diabetes 2005, 54, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- Mamputu, J.; Wiernsperger, N.; Renier, G. Antiatherogenic properties of metformin: The experimental evidence. Diabetes Metab. 2003, 29, 6S71–6S76. [Google Scholar] [CrossRef]
- Esfahanian, N.; Shakiba, Y.; Nikbin, B.; Soraya, H.; Maleki-Dizaji, N.; Ghazi-Khansari, M.; Garjani, A. Effect of metformin on the proliferation, migration, and MMP-2 and -9 expression of human umbilical vein endothelial cells. Mol. Med. Rep. 2012, 5, 1068–1074. [Google Scholar] [CrossRef] [Green Version]
- Kapelouzou, A.; Kadoglou, N.P.; Tsanikidis, H. Effects of rosiglitazone and metformin treatment on apelin, visfatin, and ghrelin levels in patients with type 2 diabetes mellitus. Metabolism 2010, 59, 373–379. [Google Scholar]
- Arunachalam, G.; Samuel, S.M.; Marei, I.; Ding, H.; Triggle, C.R. Metformin modulates hyperglycaemia-induced endothelial senescence and apoptosis through SIRT1. Br. J. Pharmacol. 2014, 171, 523–535. [Google Scholar] [CrossRef]
- Majithiya, J.B.; Balaraman, R. Metformin reduces blood pressure and restores endothelial function in aorta of streptozotocin-induced diabetic rats. Life Sci. 2006, 78, 2615–2624. [Google Scholar] [CrossRef]
- De Jager, J.; Kooy, A.; Schalkwijk, C.; van der Kolk, J.; Lehert, P.; Bets, D.; Wulffelé, M.G.; Donker, A.J.; Stehouwer, C.D. Long-term effects of metformin on endothelial function in type 2 diabetes: A randomized controlled trial. J. Intern. Med. 2014, 275, 59–70. [Google Scholar] [CrossRef]
- Vitale, C.; Mercuro, G.; Cornoldi, A.; Fini, M.; Volterrani, M.; Rosano, G.M.C. Metformin improves endothelial function in patients with metabolic syndrome. J. Intern. Med. 2005, 258, 250–256. [Google Scholar] [CrossRef]
- Wang, D.; Uhrin, P.; Mocan, A.; Waltenberger, B.; Breuss, J.M.; Tewari, D.; Mihaly-Bison, J.; Huminiecki, Ł.; Starzyński, R.R.; Tzvetkov, N.T.; et al. Vascular smooth muscle cell proliferation as a therapeutic target. Part 1: Molecular targets and pathways. Biotechnol. Adv. 2018, 36, 1586–1607. [Google Scholar] [CrossRef]
- Hao, B.; Xiao, Y.; Song, F.; Long, X.; Huang, J. Metformin-induced activation of AMPK inhibits the proliferation and migration of human aortic smooth muscle cells through upregulation of p53 and IFI16. Int. J. Mol. Med. 2018, 41, 1365–1376. [Google Scholar] [CrossRef]
- Formoso, G.; De Filippis, E.A.; Michetti, N.; Di Fulvio, P.; Pandolfi, A.; Bucciarelli, T.; Ciabattoni, G.; Nicolucci, A.; Davì, G.; Consoli, A. Decreasedin vivo oxidative stress and decreased platelet activation following metformin treatment in newly diagnosed type 2 diabetic subjects. Diabetes/Metabolism Res. Rev. 2008, 24, 231–237. [Google Scholar] [CrossRef]
- Huttunen, K.M.; Leppänen, J.; Kemppainen, E.; Palonen, P.; Rautio, J.; Järvinen, T.; Vepsäläinen, J. Towards metformin prodrugs. Synthesis (Stuttg.) 2008, 22, 3619–3624. [Google Scholar] [CrossRef]
- Markowicz-Piasecka, M.; Sikora, J.; Mateusiak, Ł.; Mikiciuk-Olasik, E.; Huttunen, K.M. New prodrugs of metformin do not influence the overall haemostasis potential and integrity of the erythrocyte membrane. Eur. J. Pharmacol. 2017, 811, 208–221. [Google Scholar] [CrossRef] [Green Version]
- Markowicz-Piasecka, M.; Huttunen, K.M.; Mateusiak, Ł.; Mikiciuk-Olasik, E.; Sikora, J. Sulfenamide and sulfonamide derivatives of metformin can exert anticoagulant and profibrinolytic properties. Chem. Interactions 2018, 284, 126–136. [Google Scholar] [CrossRef]
- Markowicz-piasecka, M.; Huttunen, K.M.; Broncel, M.; Sikora, J. Sulfenamide and Sulfonamide Derivatives of Metformin—A New Option to Improve Endothelial Function and Plasma Haemostasis, Sci. Rep. 2019, 9, 1–19. [Google Scholar]
- Kevil, C.G.; Orr, A.W.; Langston, W.; Mickett, K.; Murphy-Ullrich, J.; Patel, R.P.; Kucik, D.F.; Bullard, D.C. Intercellular Adhesion Molecule-1 (ICAM-1) Regulates Endothelial Cell Motility through a Nitric Oxide-dependent Pathway. J. Boil. Chem. 2004, 279, 19230–19238. [Google Scholar] [CrossRef] [Green Version]
- Skowron, W.; Zemanek, K.; Wojdan, K.; Gorzelak, P.; Borowiec, M.; Broncel, M.; Chalubinski, M. The effect of interleukin-35 on the integrity, ICAM-1 expression and apoptosis of human aortic smooth muscle cells. Pharmacol. Rep. 2015, 67, 376–381. [Google Scholar] [CrossRef]
- Markowicz-Piasecka, M.; Huttunen, K.H.; Mikiciuk-Olasik, E.; Sikora, J. Biocompatible sulfenamide and sulfonamide derivatives of metformin can exert beneficial effects on plasma haemostasis. Chem. Interactions 2018, 280, 15–27. [Google Scholar] [CrossRef]
- Kajbaf, F.; De Broe, M.E.; Lalau, J.D. Therapeutic Concentrations of Metformin: A Systematic Review. Clin. Pharmacokinet. 2016, 55, 439–459. [Google Scholar] [CrossRef]
- He, L.; Wondisford, F.E. Essay Metformin Action: Concentrations Matter. Cell Metab. 2015, 21, 159–162. [Google Scholar] [CrossRef] [Green Version]
- Bakhashab, S.; Ahmed, F.; Schulten, H.-J.; Ahmed, F.W.; Glanville, M.; Al-Qahtani, M.H.; Weaver, J.U. Proangiogenic Effect of Metformin in Endothelial Cells Is via Upregulation of VEGFR1/2 and Their Signaling under Hyperglycemia-Hypoxia. Int. J. Mol. Sci. 2018, 19, 293. [Google Scholar] [CrossRef] [Green Version]
- Detaille, D.; Guigas, B.; Chauvin, C.; Batandier, C.; Fontaine, E.; Wiernsperger, N.; Leverve, X. Metformin prevents high-glucose-induced endothelial cell death through a mitochondrial permeability transition-dependent process. Diabetes 2005, 54, 2179–2187. [Google Scholar] [CrossRef] [Green Version]
- Gerthoffer, W.T. Mechanisms of Vascular Smooth Muscle Cell Migration. Circ. Res. 2007, 100, 607–621. [Google Scholar] [CrossRef] [Green Version]
- Louis, S.F.; Zahradka, P. Vascular smooth muscle cell motility: From migration to invasion. Exp. Clin. Cariol. 2010, 15, 75–85. [Google Scholar]
- Braun, M.; Pietsch, P.; Schrör, K.; Baumann, G.; Felix, S.B. Cellular adhesion molecules on vascular smooth muscle cells. Cardiovasc. Res. 1999, 41, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Tang, Q.; Zheng, G.; Wang, C.; Zhou, Y.; Wu, Y.; Xuan, J.; Tian, N.; Wang, X.; Wu, Y.; et al. Metformin ameliorates BSCB disruption by inhibiting neutrophil infiltration and MMP-9 expression but not direct TJ proteins expression regulation. J. Cell. Mol. Med. 2017, 21, 3322–3336. [Google Scholar] [CrossRef] [Green Version]
- Papazafiropoulou, A.; Papanas, N.; Pappas, S.; Maltezos, E.; Mikhailidis, D.P. Effects of oral hypoglycemic agents on platelet function. J. Diabetes Its Complicat. 2015, 29, 846–851. [Google Scholar] [CrossRef]
- Aubertin, J.; Gin, H.; Freyburger, G.; Boisseau, M. Study of the effect of metformin on platelet aggregation in insulin-dependent diabetics. Diabetes Res. Clin. Pr. 1989, 6, 61–67. [Google Scholar]
- Ruggeri, Z.M.; Mendolicchio, G.L. Adhesion Mechanisms in Platelet Function. Circ. Res. 2007, 100, 1673–1685. [Google Scholar] [CrossRef]
- Huttunen, K.M.; Mannila, A.; Laine, K.; Kemppainen, E.; Leppanen, J.; Vepsalainen, J.; Jarvinen, T.; Rautio, J. The First Bioreversible Prodrug of Metformin with Improved Lipophilicity and Enhanced Intestinal Absorption. J. Med. Chem. 2009, 52, 4142–4148. [Google Scholar] [CrossRef]
- Huttunen, K.M.; Leppänen, J.; Laine, K.; Vepsalainen, J.; Rautio, J. Convenient microwave-assisted synthesis of lipophilic sulfenamide prodrugs of metformin. Eur. J. Pharm. Sci. 2013, 49, 624–628. [Google Scholar] [CrossRef]
- Rautio, J.; Vernerová, M.; Aufderhaar, I.; Huttunen, K.M. Glutathione-S-transferase selective release of metformin from its sulfonamide prodrug. Bioorganic Med. Chem. Lett. 2014, 24, 5034–5036. [Google Scholar] [CrossRef]
- Cierniewski, C.S.; Walkowiak, B.; Michalak, E.; Koziołkiewicz, W. Rapid photometric method for estimation of platelet count in blood plasma in platelet suspension. Thromb. Res. 1989, 56, 763–766. [Google Scholar]
- Sikora, J.; Markowicz-Piasecka, M.; Broncel, M.; Mikiciuk-Olasik, E. Extract of Aronia melanocarpa-modified hemostasis: In vitro studies. Eur. J. Nutr. 2014, 53, 1493–1502. [Google Scholar] [CrossRef] [Green Version]
Sample Availability: Samples of the compounds (metformin and compounds 1–4) are available from the authors. |











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | HUVEC Cells [µmol/mL] | AoSMC Cells [µmol/mL] |
|---|---|---|
| 1 | 3.781 ± 1.130 | 0.902 ± 0.015 |
| 2 | 1.044 ± 0.131 | 1.247 ± 0.062 |
| 3 | 2.407 ± 0.203 | NE# |
| 4 | 2.742 ± 0.119 | NE‡ |
| Compound [μmol/mL] | Single Cells in Gate B [%] 1 | Living Cells [D - -] [%] 2 | Necrotic Cells [D - +] [%] 2 | Early Apoptotic [D + -] [%] 2 | Late Apoptotic [D + +] [%] 2 | |
|---|---|---|---|---|---|---|
| Control_1 | B | 91.04 ± 0.81 | 91.20 ± 2.11 | 0.92 ± 0.25 | 4.78 ± 1.46 | 3.11 ± 0.87 |
| Met [0.3 μmol/mL] | B | 91.99 ± 0.03 | 91.81 ± 1.03 | 0.61 ± 0.11 | 4.02 ± 0.92 | 3.57 ± 0.23 |
| Met [1.5 μmol/mL] | B | 91.82 ± 0.43 | 92.13 ± 0.57 | 0.55 ± 0.09 | 3.77 ± 0.10 | 3.55 ± 0.42 |
| Comp. 1 [0.1 μmol/mL] | B | 92.70 ± 0.41 | 91.36 ± 2.59 | 0.60 ± 0.05 | 4.71 ± 1.95 | 3.33 ± 0.68 |
| Comp. 1 [0.9 μmol/mL] | B | 61.36 ± 1.15 | 12.33 ± 2.03 | 0.55 ± 0.15 | 71.36 ± 2.55 | 15.76 ± 0.61 |
| Control_2 | B | 92.45 ± 0.58 | 92.34 ± 2.02 | 0.90 ± 0.41 | 4.05 ± 0.91 | 2.71 ± 0.82 |
| Comp. 2 [0.3 μmol/mL] | B | 92.85 ± 0.67 | 89.26 ± 3.13 | 0.70 ± 0.20 | 4.82 ± 1.48 | 4.70 ± 1.63 |
| Comp. 2 [1.0 μmol/mL] | B | 92.19 ± 0.60 | 83.84 ± 0.47 | 0.90 ± 0.23 | 7.96 ± 0.43 | 7.30 ± 0.63 |
| Comp. 3 [0.3 μmol/mL] | B | 94.32 ± 0.43 | 90.83 ± 1.78 | 0.83 ± 0.15 | 4.98 ± 1.40 | 3.37 ± 0.63 |
| Comp. 3 [1.5 μmol/mL] | B | 94.20 ± 0.47 | 89.23 ± 2.55 | 0.99 ± 0.22 | 5.69 ± 1.92 | 4.08 ± 0.73 |
| Comp. 4 [0.3 μmol/mL] | B | 93.79 ± 0.52 | 88.84 ± 0.21 | 1.05 ± 0.22 | 5.11 ± 0.41 | 5.01 ± 0.13 |
| Comp. 4 [1.5 μmol/mL] | B | 93.08 ± 0.45 | 82.61 ± 0.97 | 1.58 ± 0.26 | 8.29 ± 0.35 | 7.52 ± 0.56 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markowicz-Piasecka, M.; Huttunen, K.M.; Sadkowska, A.; Sikora, J. Pleiotropic Activity of Metformin and Its Sulfonamide Derivatives on Vascular and Platelet Haemostasis. Molecules 2020, 25, 125. https://doi.org/10.3390/molecules25010125
Markowicz-Piasecka M, Huttunen KM, Sadkowska A, Sikora J. Pleiotropic Activity of Metformin and Its Sulfonamide Derivatives on Vascular and Platelet Haemostasis. Molecules. 2020; 25(1):125. https://doi.org/10.3390/molecules25010125
Chicago/Turabian StyleMarkowicz-Piasecka, Magdalena, Kristiina M. Huttunen, Adrianna Sadkowska, and Joanna Sikora. 2020. "Pleiotropic Activity of Metformin and Its Sulfonamide Derivatives on Vascular and Platelet Haemostasis" Molecules 25, no. 1: 125. https://doi.org/10.3390/molecules25010125