
Dietary Lutein and Cognitive Function in Adults: A Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Methods
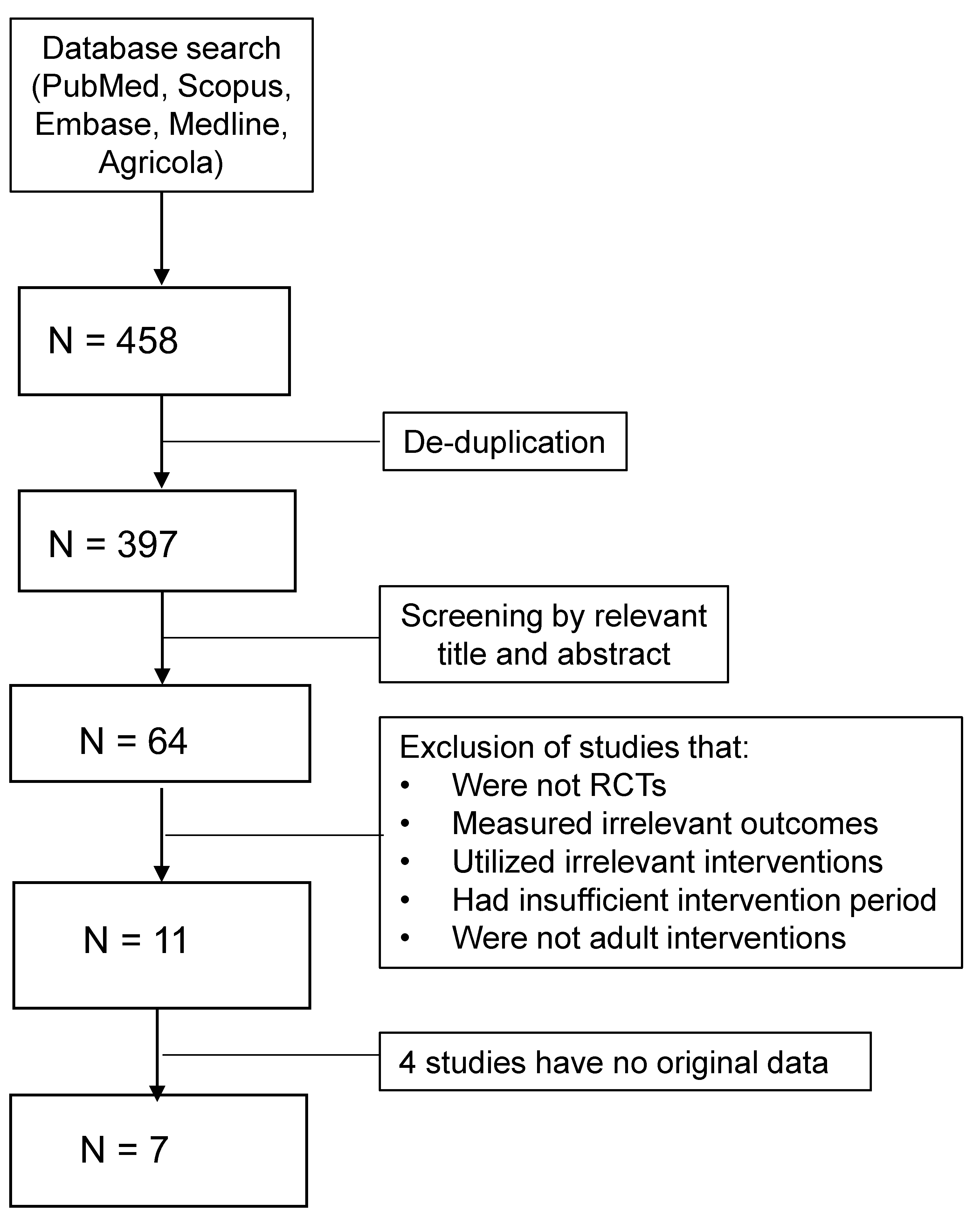
2.1. Literature Search and Selection of Studies
2.2. Data Extraction and Statistical Analysis
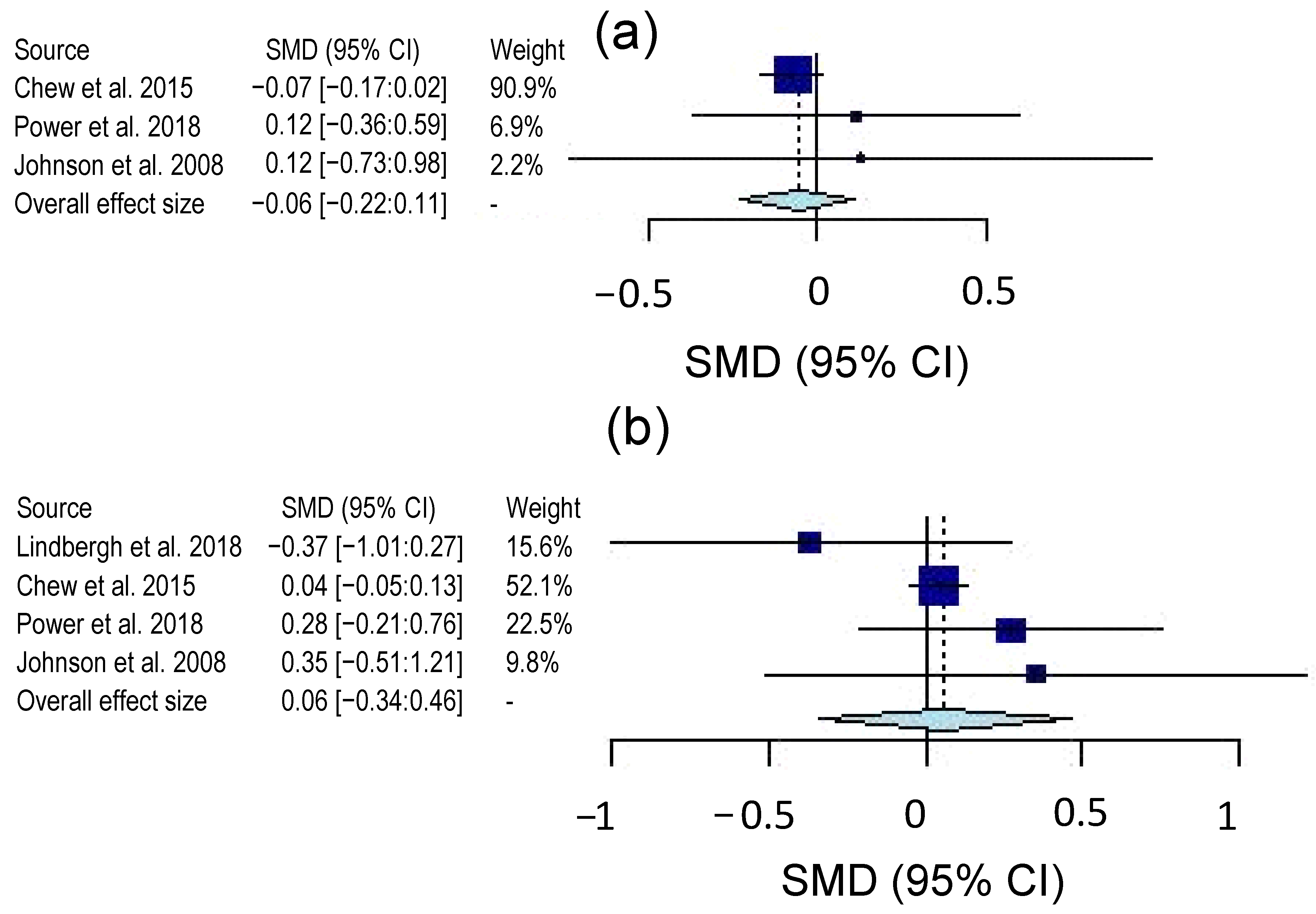
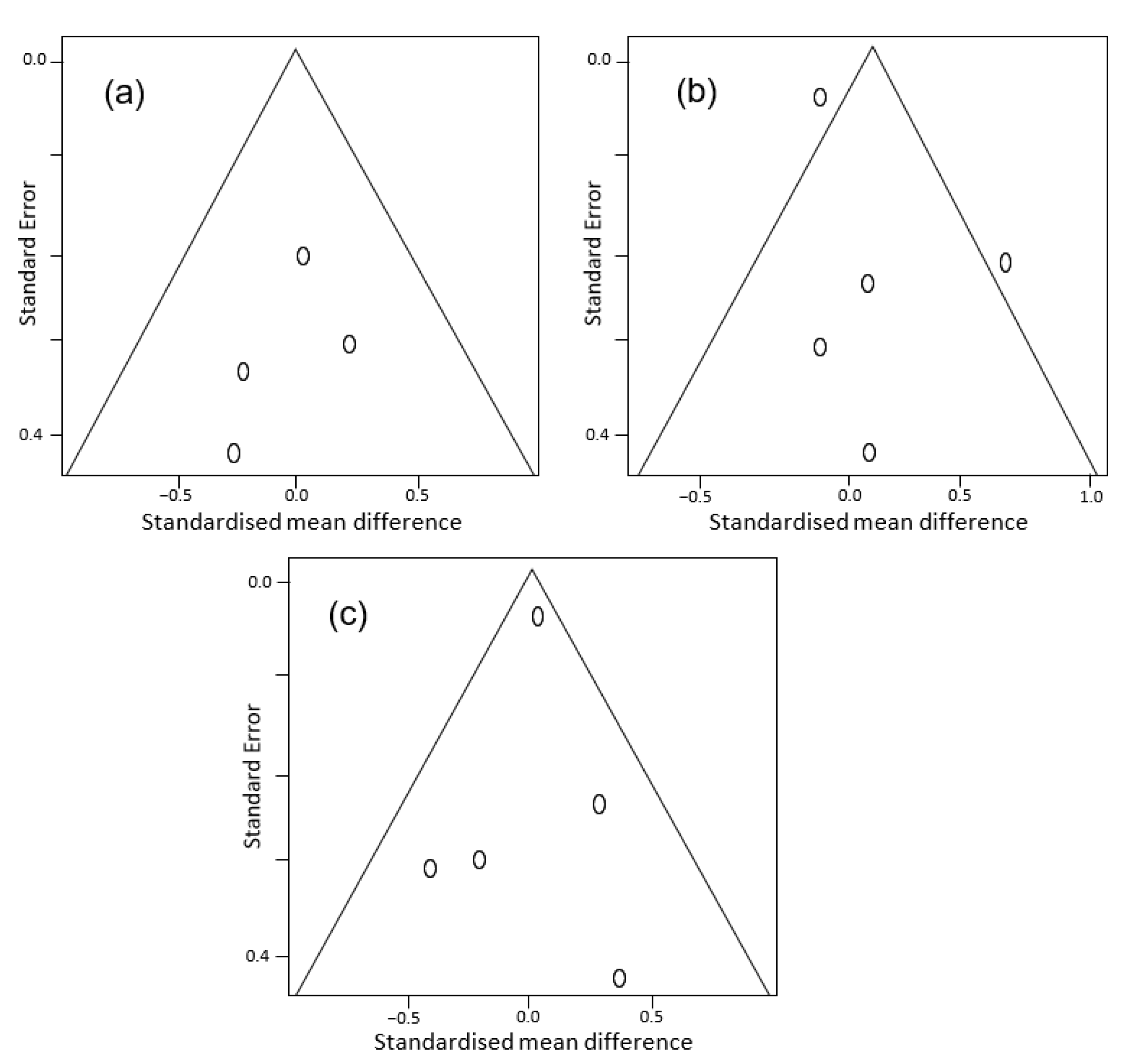
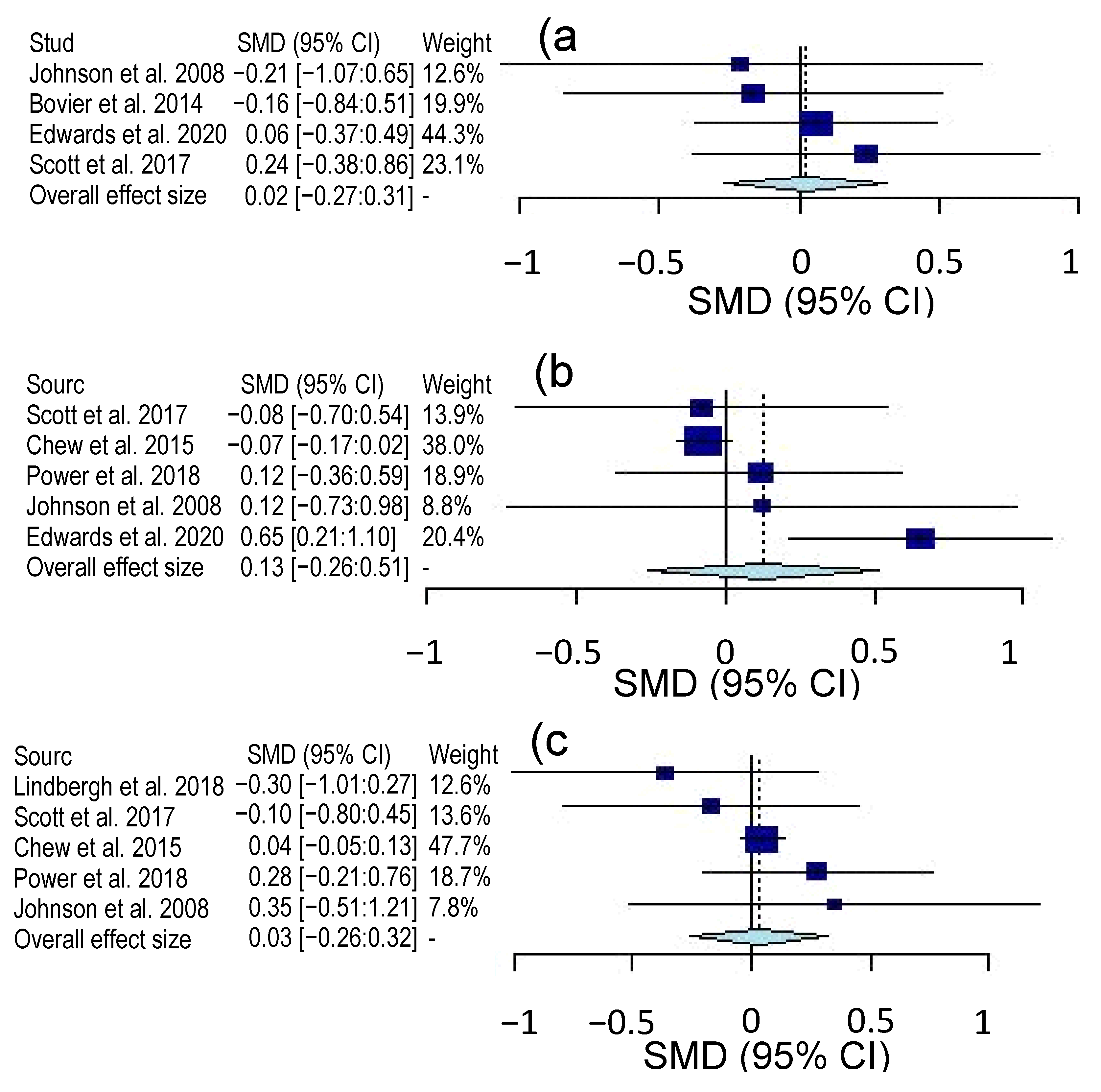
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdel-Aal, E.-S.M.; Akhtar, H.; Zaheer, K.; Ali, R. Dietary Sources of Lutein and Zeaxanthin Carotenoids and Their Role in Eye Health. Nutrients 2013, 5, 1169–1185. [Google Scholar] [CrossRef] [Green Version]
- Chung, H.-Y.; Rasmussen, H.M.; Johnson, E.J. Lutein Bioavailability Is Higher from Lutein-Enriched Eggs than from Supplements and Spinach in Men. J. Nutr. 2004, 134, 1887–1893. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.C. A Comprehensive Review of Eggs, Choline, and Lutein on Cognition Across the Life-span. J. Am. Coll. Nutr. 2018, 37, 269–285. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, B.; Natoli, S.; Liew, G.; Flood, V. Lutein and Zeaxanthin—Food Sources, Bioavailability and Dietary Variety in Age-Related Macular Degeneration Protection. Nutrients 2017, 9, 120. [Google Scholar] [CrossRef] [PubMed]
- Renzi, L.M.; Johnson, E.J. Lutein and Age-Related Ocular Disorders in the Older Adult. J. Nutr. Elder. 2007, 26, 139–157. [Google Scholar] [CrossRef] [PubMed]
- Stringham, J.M.; Johnson, E.J.; Hammond, B.R. Lutein across the Lifespan: From Childhood Cognitive Performance to the Aging Eye and Brain. Curr. Dev. Nutr. 2019, 3, nzz066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishwanathan, R.; Schalch, W.; Johnson, E.J. Macular Pigment Carotenoids in the Retina and Occipital Cortex are Related in Humans. Nutr. Neurosci. 2015, 19, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Tanito, M.; Obana, A.; Gohto, Y.; Okazaki, S.; Gellermann, W.; Ohira, A. Macular Pigment Density Changes in Japanese Individuals Supplemented with Lutein or Zeaxanthin: Quantification via Resonance Raman Spectrophotometry and Autofluorescence Imaging. Jpn. J. Ophthalmol. 2012, 56, 488–496. [Google Scholar] [CrossRef]
- Johnson, E.J. Role of Lutein and Zeaxanthin in Visual and Cognitive Function Throughout the Lifespan. Nutr. Rev. 2014, 72, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.; Coen, R.F.; Akuffo, K.O.; Beatty, S.; Dennison, J.; Moran, R.; Stack, J.; Howard, A.N.; Mulcahy, R.; Nolan, J.M. Cognitive Function and its Relationship with Macular Pigment Optical Density and Serum Concentrations of its Constituent Carotenoids. J. Alzheimer’s Dis. 2015, 48, 261–277. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.-P.; Sun, L.; Yu, H.-S.; Liang, L.-P.; Li, W.; Ding, H.; Song, X.-B.; Zhang, L.-J. The Pharmacological Effects of Lutein and Zeaxanthin on Visual Disorders and Cognition Diseases. Molecules 2017, 22, 610. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; SanGiovanni, J.P.; Danis, R.; Ferris, F.L., III; Elman, M.; Antoszyk, A.; Ruby, A.; Orth, D.; Bressler, S.; et al. Lutein + Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration: The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA 2013, 309, 2005–2015. [Google Scholar] [CrossRef]
- Johnson, E.J. A Possible Role for Lutein and Zeaxanthin in Cognitive Function in the Elderly. Am. J. Clin. Nutr. 2012, 96, 1161S–1165S. [Google Scholar] [CrossRef] [Green Version]
- Harvey, P.D. Domains of Cognition and their Assessment. Dialogues. Clin. Neurosci. 2019, 21, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying Neurocognitive Disorders: The DSM-5 Approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Shinto, L.; Connor, W.E.; Quinn, J.F. Nutritional Biomarkers in Alzheimers Disease: The Association between Carotenoids, n-3 Fatty Acids, and Dementia Severity. J. Alzheimer’s Dis. 2008, 13, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Kesse-Guyot, E.; Andreeva, V.A.; Ducros, V.; Jeandel, C.; Julia, C.; Hercberg, S.; Galan, P. Carotenoid-rich Dietary Patterns During Midlife and Subsequent Cognitive Function. Br. J. Nutr. 2014, 111, 915–923. [Google Scholar] [CrossRef]
- Stringham, N.T.; Holmes, P.V.; Stringham, J.M. Effects of Macular Xanthophyll Supplementation on Brain-derived Neurotrophic Factor, Pro-inflammatory Cytokines, and Cognitive Performance. Physiol. Behav. 2019, 211, 112650. [Google Scholar] [CrossRef]
- Nooyens, A.C.J.; Milder, I.E.J.; Gelder, B.M.V.; Bueno-De-Mesquita, H.B.; Boxtel, M.P.J.V.; Verschuren, W.M.M. Diet and Cognitive Decline at Middle Age: The Role of Antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [Green Version]
- Demmig-Adams, B.; López-Pozo, M.; Stewart, J.J.; Adams, W.W., III. Zeaxanthin and Lutein: Photoprotectors, Anti-Inflammatories, and Brain Food. Molecules 2020, 25, 3607. [Google Scholar] [CrossRef]
- Schmidt, R.; Hayn, M.; Reinhart, B.; Roob, G.; Schmidt, H.; Schumacher, M.; Watzinger, N.; Launer, L.J. Plasma Antioxidants and Cognitive Performance in Middle-Aged and Older Adults: Results of the Austrian Stroke Prevention Study. J. Am. Geriatr. Soc. 2015, 46, 1407–1410. [Google Scholar] [CrossRef]
- Vishwanathan, R.; Iannaccone, A.; Scott, T.M.; Kritchevsky, S.B.; Jennings, B.J.; Carboni, G.; Forma, G.; Satterfield, S.; Harris, T.; Johnson, K.C.; et al. Macular Pigment Optical Density is Related to Cognitive Function in Older People. Age. Ageing 2014, 43, 271–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajana, S.; Weber, D.; Helmer, C.; Merle, B.M.; Stuetz, W.; Dartigues, J.-F.; Rougier, M.-B.; Korobelnik, J.-F.; Grune, T.; Delcourt, C.; et al. Plasma Concentrations of Lutein and Zeaxanthin, Macular Pigment Optical Density, and their Associations with Cognitive Performances Among Older Adults. Investig. Opthalmol. Vis. Sci. 2018, 59, 1828–1835. [Google Scholar] [CrossRef] [Green Version]
- Oliver, W.; Renzi-Hammond, L.M.; Thorne, S.A.; Clementz, B.; Miller, L.S.; Hammond, B.R., Jr. Neural Activation During Visual Attention Differs in Individuals with High versus Low Macular Pigment Density. Mol. Nutr. Food. Res. 2019, 63, 1801052. [Google Scholar] [CrossRef] [PubMed]
- Feeney, J.; Finucane, C.; Savva, G.M.; Cronin, H.; Beatty, S.; Nolan, J.M.; Kenny, R.A. Low Macular Pigment Optical Density is Associated with Lower Cognitive Performance in a Large, Population-based Sample of Older Adults. Neurobiol. Aging 2013, 34, 2449–2456. [Google Scholar] [CrossRef]
- Renzi, L.M.; Dengler, M.J.; Puente, A.; Miller, L.S.; Hammond, B.R. Relationships Between Macular Pigment Optical Density and Cognitive Function in Unimpaired and Mildly Cognitively Impaired Older Adults. Neurobiol. Aging 2014, 35, 1695–1699. [Google Scholar] [CrossRef]
- Feeney, J.; O’Leary, N.; Moran, R.; O’Halloran, A.M.; Nolan, J.M.; Beatty, S.; Young, I.S.; Kenny, R.A. Plasma Lutein and Zeaxanthin are Associated with Better Cognitive Function Across Multiple Domains in a Large Population-Based Sample of Older Adults: Findings from The Irish Longitudinal Study on Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1431–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindbergh, C.A.; Mewborn, C.M.; Hammond, B.R.; Renzi-Hammond, L.M.; Curran-Celentano, J.M.; Miller, L.S. Relationship of Lutein and Zeaxanthin Levels to Neurocognitive Functioning: An fMRI Study of Older Adults. J. Int. Neuropsychol. Soc. 2017, 23, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Zuniga, K.E.; Bishop, N.J.; Turner, A.S. Dietary Lutein and Zeaxanthin are Associated with Working Memory in an Older Population. Public Health Nutr. 2021, 24, 1708–1715. [Google Scholar] [CrossRef]
- Cannavale, C.; Hassevoort, K.; Edwards, C.; Thompson, S.; Burd, N.; Holscher, H.; Erdman, J.; Cohen, N.; Khan, N. Serum Lutein is Related to Relational Memory Performance. Nutrients 2019, 11, 768. [Google Scholar] [CrossRef] [Green Version]
- Akbaraly, N.T.; Faure, H.; Gourlet, V.; Favier, A.; Berr, C. Plasma Carotenoid Levels and Cognitive Performance in an Elderly Population: Results of the EVA Study. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 308–316. [Google Scholar] [CrossRef] [Green Version]
- Hammond, B.R. Lutein and Cognition in Children. J. Nutr. Sci. 2014, 3, e53. [Google Scholar] [CrossRef] [Green Version]
- Christensen, K.; Gleason, C.E.; Mares, J.A. Dietary Carotenoids and Cognitive Function Among US Adults, NHANES 2011–2014. Nutr. Neurosci. 2020, 23, 554–562. [Google Scholar] [CrossRef]
- Yuan, C.; Fondell, E.; Ascherio, A.; Okereke, O.I.; Grodstein, F.; Hofman, A.; Willett, W.C. Long-Term Intake of Dietary Carotenoids is Positively Associated with Late-Life Subjective Cognitive Function in a Prospective Study in US Women. J. Nutr. 2020, 150, 1871–1879. [Google Scholar] [CrossRef]
- Khan, N.; Walk, A.; Edwards, C.; Jones, A.; Cannavale, C.; Thompson, S.; Reeser, G.; Holscher, H. Macular Xanthophylls are Related to Intellectual Ability among Adults with Overweight and Obesity. Nutrients 2018, 10, 396. [Google Scholar] [CrossRef] [Green Version]
- Mewborn, C.M.; Lindbergh, C.A.; Hammond, B.R.; Renzi-Hammond, L.M.; Miller, L.S. The Effects of Lutein and Zeaxanthin Supplementation on Brain Morphology in Older Adults: A Randomized, Controlled Trial. J. Aging Res. 2019, 2019, 3709402. [Google Scholar] [CrossRef] [PubMed]
- Bovier, E.R.; Renzi, L.M.; Hammond, B.R. A Double-Blind, Placebo-Controlled Study on the Effects of Lutein and Zeaxanthin on Neural Processing Speed and Efficiency. PLoS ONE 2014, 9, e108178. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.M.; Rasmussen, H.M.; Chen, O.; Johnson, E.J. Avocado Consumption Increases Macular Pigment Density in Older Adults: A Randomized, Controlled Trial. Nutrients 2017, 9, 919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, E.J.; Mcdonald, K.; Caldarella, S.M.; Chung, H.-Y.; Troen, A.M.; Snodderly, D.M. Cognitive findings of an Exploratory Trial of Docosahexaenoic Acid and Lutein Supplementation in Older Women. Nutr. Neurosci. 2008, 11, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.G.; Walk, A.M.; Thompson, S.V.; Reeser, G.E.; Erdman, J.W.; Burd, N.A.; Holscher, H.D.; Khan, N.A. Effects of 12-week Avocado Consumption on Cognitive Function among Adults with Overweight and Obesity. Int. J. Psychophysiol. 2020, 148, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Renzi-Hammond, L.; Bovier, E.; Fletcher, L.; Miller, L.; Mewborn, C.; Lindbergh, C.; Baxter, J.; Hammond, B. Effects of a Lutein and Zeaxanthin Intervention on Cognitive Function: A Randomized, Double-Masked, Placebo-Controlled Trial of Younger Healthy Adults. Nutrients 2017, 9, 1246. [Google Scholar] [CrossRef] [Green Version]
- Hammond, B.R.; Miller, L.S.; Bello, M.O.; Lindbergh, C.A.; Mewborn, C.; Renzi-Hammond, L.M. Effects of Lutein/Zeaxanthin Supplementation on the Cognitive Function of Community Dwelling Older Adults: A Randomized, Double-Masked, Placebo-Controlled Trial. Front. Aging Neurosci. 2017, 9, 254. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; Agrón, E.; Launer, L.J.; Grodstein, F.; Bernstein, P.S. Effect of Omega-3 Fatty Acids, Lutein/Zeaxanthin, or Other Nutrient Supplementation on Cognitive Function. JAMA 2015, 314, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Lindbergh, C.A.; Renzi-Hammond, L.M.; Hammond, B.R.; Terry, D.P.; Mewborn, C.M.; Puente, A.N.; Miller, L.S. Lutein and Zeaxanthin Influence Brain Function in Older Adults: A Randomized Controlled Trial. J. Int. Neuropsychol. Soc. 2018, 24, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Power, R.; Coen, R.; Beatty, S.; Mulcahy, R.; Moran, R.; Stack, J.; Howard, A.; Nolan, J. Supplemental Retinal Carotenoids Enhance Memory in Healthy Individuals with Low Levels of Macular Pigment in a Randomized, Double Blind, Placebo-Controlled Clinical Trial. J. Alzheimer’s Dis. 2018, 61, 947–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, J.M.; Loskutova, E.; Howard, A.; Mulcahy, R.; Moran, R.; Stack, J.; Bolger, M.; Coen, R.F.; Dennison, J.; Akuffo, K.O.; et al. The Impact of Supplemental Macular Carotenoids in Alzheimers Disease: A Randomized Clinical Trial. J. Alzheimer’s Dis. 2015, 44, 1157–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009; ISBN 978-0-470-05724-7. [Google Scholar]
- Makambi, K.H. The Effect of the Heterogeneity Variance Estimator on Some Tests of Treatment Efficacy. J. Biopharm. Stat. 2004, 14, 439–449. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.A.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman Method for Random Effects Meta-Analysis is Straightforward and Considerably Outperforms the Standard DerSimonian-Laird Method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Chapter 13: Assessing Risk of Bias due to Missing Results in a Synthesis. Available online: https://training.cochrane.org/handbook/current/chapter-13 (accessed on 19 March 2021).
- Nolan, J.M.; Mulcahy, R.; Power, R.; Moran, R.; Howard, A.N. Nutritional Intervention to Prevent Alzheimer’s Disease: Potential Benefits of Xanthophyll Carotenoids and Omega-3 Fatty Acids Combined. J. Alzheimer’s Dis. 2018, 64, 367–378. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population (Age, Location and Health Status) | Treatment (Daily Dose, mg) | Comparison Treatment | Health Outcomes | Intervention Length |
|---|---|---|---|---|---|
| Bovier et al. 2014 | 18–32, USA, Healthy | 20 Z & 26 Z + 8 L | Placebo | MPOD, CFF, motor reaction time | 4 months |
| Chew et al. 2015 | Mean 72.7, USA, With or at risk of AMD | 10 L + 2 Z | Placebo | TICS, MMSE | 5 years |
| Edwards et al. 2020 | 25–45, USA, BMI >= 27.5 | 1 avocado (0.5 L) | Isocaloric meal | MPOD, Flanker, Nogo, Oddball | 12 weeks |
| Johnson et al. 2008 | 60–80, USA, Healthy | 12 L & 12 L + 800 DHA | Placebo | Custom tests | 4 months |
| Lindbergh et al. 2017 | 64–86, USA, Healthy | 10 L + 2 Z | Placebo | MPOD, fMRI | 12 months |
| Power et al. 2018 | Mean 45.5, USA, Healthy with low MPOD | 10 L + 10 meso-Z + 2 Z | Placebo | MPOD, CANTAB | 12 months |
| Scott et al. 2017 | >50, USA, Healthy | 1 avocado (0.5 L) | Isocaloric meal | MPOD, CANTAB | 6 months |
| No of Studies | Certainty Assessment | Participants (n) | Certainty (Overall Quality) b | Heterogeneity (X2, I2) c | |||||
|---|---|---|---|---|---|---|---|---|---|
| Study Design | Risk of Bias a | Inconsistency a | Indirectness a | Imprecision a | Treatment | Control | |||
| Complex attention | |||||||||
| 4 | RCT | Not serious | Serious | Not serious | Not serious | 132 | 77 | Moderate | 1.06 (p = 0.79), 0% (0–57%) |
| Executive function | |||||||||
| 5 | RCT | Not serious | Serious | Not serious | Not serious | 1037 | 1031 | Moderate | 10.51 (p = 0.03), 62% (0–86%) |
| Memory | |||||||||
| 5 | RCT | Not serious | Serious | Not serious | Not serious | 1018 | 1007 | Moderate | 3.42 (p = 0.49), 0% (0–76%) |
| Study | Measurement | Outcome | Group (n) | Baseline (Mean ± SD) | Post-Intervention (Mean ± SD) | Significance Level |
|---|---|---|---|---|---|---|
| Bovier et al. 2014 | Reaction Time (ms) | Complex Attention a | Placebo (10) | 219.6 ± 14.2 | 220.1 ± 20.4 | NS |
| Treatment (54) | 229.9 ± 23.3 | 223.4 ± 21.6 | HS | |||
| Chew et al. 2015 | Word recall | Memory | Placebo (932) | NA | 2.4 ± 2.2 | NA |
| Treatment (921) | NA | 2.5 ± 2.4 | NA | |||
| Animal | Executive function | Placebo (933) | NA | 16.8 ± 5.4 | NA | |
| Treatment (922) | NA | 16.4 ± 5.4 | NA | |||
| Edwards et al. 2020 | Oddball (%) | Complex attention | Placebo (37) | 88.6 ± 11.19 | 92.8 ± 7.6 | NS |
| Treatment (47) | 91.6 ± 7.7 | 93.2 ± 6.0 | NS | |||
| Flanker (%) | Executive function | Placebo | 93.5 ± 4.7 | 92.5 ± 5.9 | NS | |
| Treatment | 93.4 ± 5.3 | 95.6 ± 3.5 | HS | |||
| Johnson et al. 2008 | Pattern recognition Speed (s) | Complex attention a | Placebo (10) | 6.8 ± 3.0 | 5.9 ± 2.3 | NS |
| Treatment (11) | 6.1 ± 2.3 | 6.4 ± 2.3 | NS | |||
| Verbal Fluency | Memory | Placebo | 12.9 ± 6.2 | 13.8 ± 3.5 | NS | |
| Treatment | 11.3 ± 5.1 | 15.5 ± 5.5 | S | |||
| Stroop Test (s) | Executive function a | Placebo | 25.0 ± 14.8 | 23.1 ± 22.0 | NS | |
| Treatment | 24.2 ± 10.9 | 21.0 ± 7.8 | NS | |||
| Lindbergh et al. 2018 | Word Recall | Memory | Placebo (14) b | 9.4 ± 0.8 | 8.2 ± 2.3 | S |
| Treatment (30) | 8.9 ± 1.5 | 8.8 ± 2.2 | NS | |||
| Power et al. 2018 | AST | Executive function | Placebo (31) | 841.4 ± 159.0 | 775.4 ± 217.6 | NS |
| Treatment (37) | 832.0 ± 191.9 | 751.6 ± 191.7 | NS | |||
| PAL (errors) | Memory a | Placebo (31) | 4.2 ± 3.8 | 4.5 ± 4.9 | NS | |
| Treatment (36) | 6.8 ± 7.1 | 3.2 ± 4.5 | NS | |||
| Scott et al. 2017 | CRT (ms) | Complex attention a | Placebo (20) | 356.0 ± 70.6 | 359.1 ± 75.5 | NS |
| Treatment (20) | 347.4 ± 55.4 | 342.8 ± 56.8 | NS | |||
| PAL (errors) | Memory a | Placebo | 27.3 ± 18.7 | 16.8 ± 14.9 | NS | |
| Treatment | 28.0 ± 17.8 | 19.5 ± 15.5 | NS | |||
| Stockings of Cambridge (# completed) | Executive function | Placebo | 8.0 ± 2.0 | 9.0 ± 2.7 | NS | |
| Treatment | 7.8 ± 2.3 | 8.8 ± 2.2 | HS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Abdel-Aal, E.-S.M. Dietary Lutein and Cognitive Function in Adults: A Meta-Analysis of Randomized Controlled Trials. Molecules 2021, 26, 5794. https://doi.org/10.3390/molecules26195794
Li J, Abdel-Aal E-SM. Dietary Lutein and Cognitive Function in Adults: A Meta-Analysis of Randomized Controlled Trials. Molecules. 2021; 26(19):5794. https://doi.org/10.3390/molecules26195794
Chicago/Turabian StyleLi, Jeffrey, and El-Sayed M. Abdel-Aal. 2021. "Dietary Lutein and Cognitive Function in Adults: A Meta-Analysis of Randomized Controlled Trials" Molecules 26, no. 19: 5794. https://doi.org/10.3390/molecules26195794
APA StyleLi, J., & Abdel-Aal, E.-S. M. (2021). Dietary Lutein and Cognitive Function in Adults: A Meta-Analysis of Randomized Controlled Trials. Molecules, 26(19), 5794. https://doi.org/10.3390/molecules26195794