
Reduced Endocannabinoid Tone in Saliva of Chronic Orofacial Pain Patients

 ,
, 
Abstract
:1. Introduction
2. Methods
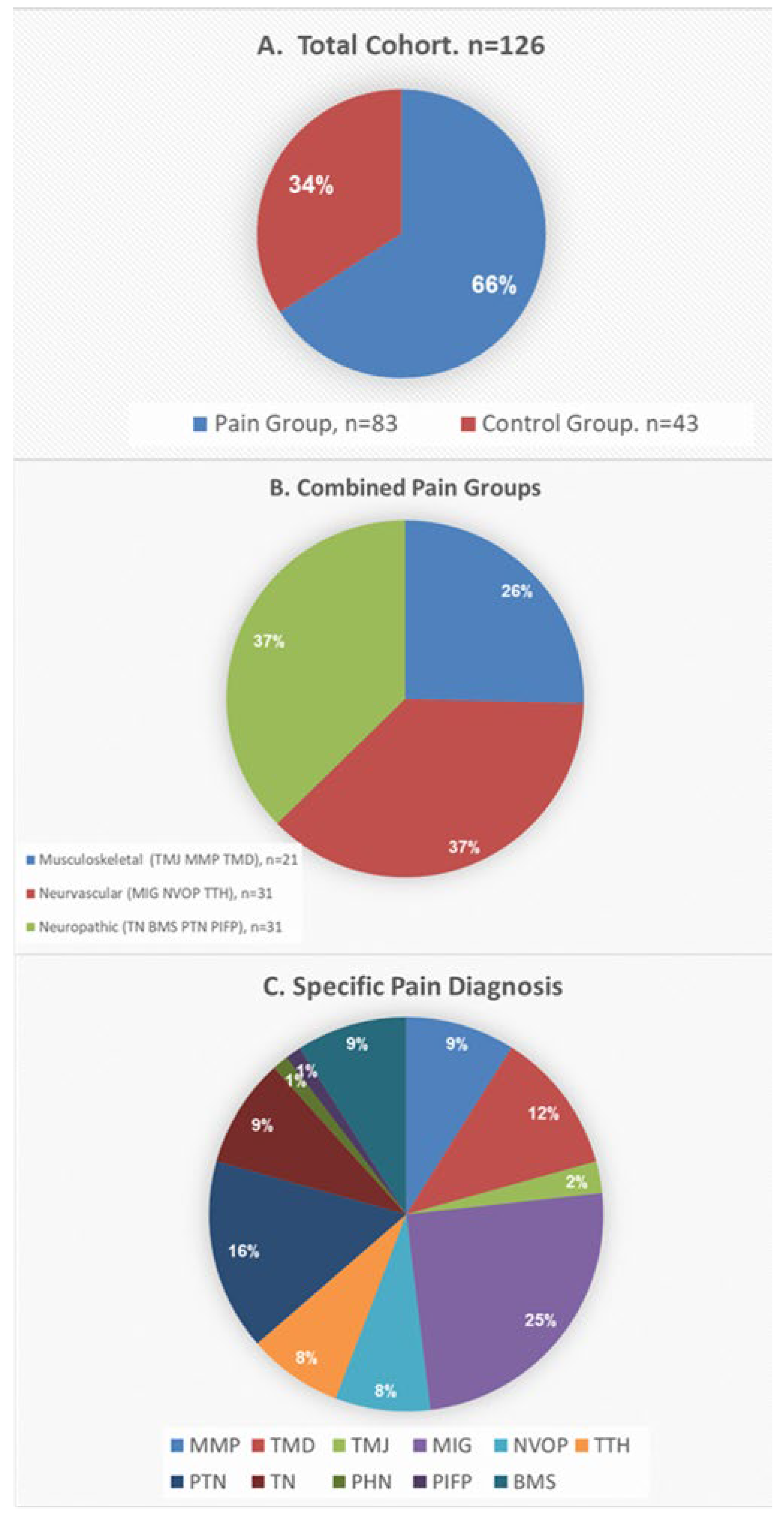
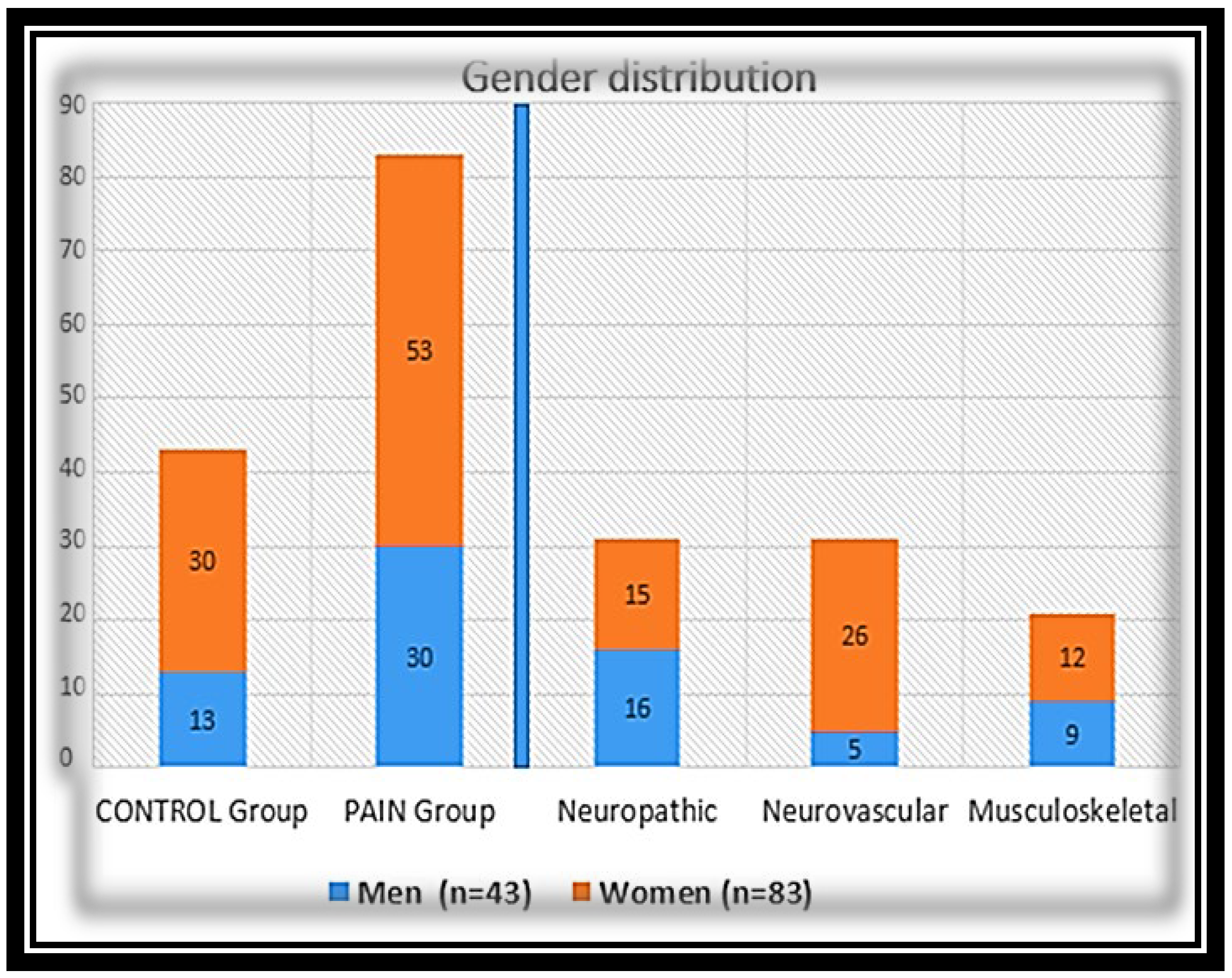
2.1. Participants
2.2. Orofacial Pain Diagnosis
2.3. Collection of Medical Records
2.4. Saliva Collection
2.5. Statistics: The Statistical Analysis Was Performed Using SPSS Version 25
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Abbreviations
| ECS | endocannabinoid system |
| eCBs | endocannabinoids and endocannabinoid-like compounds |
| AEA | Anandamide |
| 2-AG | 2-arachidonoylglycerol |
| PEA | N-palmitoylethanolamine |
| OEA | N-oleoylethanolamine |
| AA | Arachidonic acid |
| OFP | Orofacial Pain |
| VPS | Verbal Pain Score |
| IHS | International Headache Society |
| TMD | Ttemporomandibular Disorders (i.e., myofascial pain or joint) |
| DC/TMD | Diagnostic Criteria for Temporomandibular Disorders |
| Mig | Migraine |
| NVOP | Neurovascular Orofacial Pain (orofacial migraine) |
| TTH | Tension Type Headache |
| PTN | Post Traumatic Neuropathy |
| TN | Trigeminal Neuralgia |
| PHN | Post Herpetic Neuralgia |
| PIFP | Persistent Idiopathic Facial Pain |
| BMS | Burning Mouth Syndrome |
References
- Donvito, G.; Nass, S.R.; Wilkerson, J.L.; Curry, Z.A.; Schurman, L.D.; Kinsey, S.G.; Lichtman, A.H. The Endogenous Cannabinoid System: A Budding Source of Targets for Treating Inflammatory and Neuropathic Pain. Neuropsychopharmacoly 2018, 43, 52–79. [Google Scholar] [CrossRef] [Green Version]
- Felder, C.C.; Glass, M. Cannabinoid receptors and their endogenous agonists. Annu. Rev. Pharmacol. Toxicol. 1998, 38, 179–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossain, M.Z.; Ando, H.; Unno, S.; Kitagawa, J. Targeting Peripherally Restricted Cannabinoid Receptor 1, Cannabinoid Receptor 2, and Endocannabinoid-Degrading Enzymes for the Treatment of Neuropathic Pain Including Neuropathic Orofacial Pain. Int. J. Mol. Sci. 2020, 21, 41423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltramo, M. Cannabinoid type 2 receptor as a target for chronic—Pain. Mini Rev. Med. Chem. 2009, 9, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Sarchielli, P.; Pini, L.A.; Coppola, F.; Rossi, C.; Baldi, A.; Mancini, M.L.; Calabresi, P. Endocannabinoids in chronic migraine: CSF findings suggest a system failure. Neuropsychopharmacoly 2007, 32, 1384–1390. [Google Scholar] [CrossRef]
- Greco, R.; Gasperi, V.; Maccarrone, M.; Tassorelli, C. The endocannabinoid system and migraine. Exp. Neurol. 2010, 224, 85–91. [Google Scholar] [CrossRef]
- Fine, P.G.; Rosenfeld, M.J. The endocannabinoid system, cannabinoids, and pain. Rambam Maimonides Med. J. 2013, 4, e0022. [Google Scholar] [CrossRef]
- Burston, J.J.; Woodhams, S.G. Endocannabinoid system and pain: An introduction. Proc. Nutr. Soc. 2014, 73, 106–117. [Google Scholar] [CrossRef]
- Manzanares, J.; Julian, M.; Carrascosa, A. Role of the cannabinoid system in pain control and therapeutic implications for the management of acute and chronic pain episodes. Curr. Neuropharmacol. 2006, 4, 239–257. [Google Scholar] [CrossRef] [Green Version]
- Vuckovic, S.; Srebro, D.; Vujovic, K.S.; Vucetic, C.; Prostran, M. Cannabinoids and Pain: New Insights from Old Molecules. Front. Pharmacol. 2018, 9, 1259. [Google Scholar] [CrossRef] [Green Version]
- Pacher, P.; Batkai, S.; Kunos, G. The endocannabinoid system as an emerging target of pharmacotherapy. Pharmacol. Rev. 2006, 58, 389–462. [Google Scholar] [CrossRef] [Green Version]
- Sagar, D.R.; Gaw, A.G.; Okine, B.N.; Woodhams, S.G.; Wong, A.; Kendall, D.A.; Chapman, V. Dynamic regulation of the endocannabinoid system: Implications for analgesia. Mol. Pain 2009, 5, 59. [Google Scholar] [CrossRef] [Green Version]
- McPartland, J.M.; Guy, G.W.; Di Marzo, V. Care and feeding of the endocannabinoid system: A systematic review of potential clinical interventions that upregulate the endocannabinoid system. PLoS ONE 2014, 9, e89566. [Google Scholar] [CrossRef]
- Aran, A.; Eylon, M.; Harel, M.; Polianski, L.; Nemirovski, A.; Tepper, S.; Schnapp, A.; Cassuto, H.; Wattad, N.; Tam, J. Lower circulating endocannabinoid levels in children with autism spectrum disorder. Mol. Autism 2019, 10, 2. [Google Scholar] [CrossRef]
- Russo, E.B. Clinical endocannabinoid deficiency (CECD): Can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions? Neuro. Endocrinol. Lett. 2004, 25, 31–39. [Google Scholar]
- Greabu, M.; Battino, M.; Mohora, M.; Totan, A.; Didilescu, A.; Spinu, T.; Totan, C.; Miricescu, D.; Radulescu, R. Saliva—A diagnostic window to the body, both in health and in disease. J. Med. Life 2009, 2, 124–132. [Google Scholar]
- Loo, J.A.; Yan, W.; Ramachandran, P.; Wong, D.T. Comparative human salivary and plasma proteomes. J. Dent. Res. 2010, 89, 1016–1023. [Google Scholar] [CrossRef] [Green Version]
- Zidverc-Trajkovic, J.; Stanimirovic, D.; Obrenovic, R.; Tajti, J.; Vecsei, L.; Gardi, J.; Nemeth, J.; Mijajlovic, M.; Sternic, N.; Jankovic, L. Calcitonin gene-related peptide levels in saliva of patients with burning mouth syndrome. J. Oral Pathol. Med. 2009, 38, 29–33. [Google Scholar] [CrossRef]
- Fischer, M.; Wille, G.; Klien, S.; Shanib, H.; Holle, D.; Gaul, C.; Broessner, G. Brain-derived neurotrophic factor in primary headaches. J. Headache Pain 2012, 13, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Gerdle, B.; Ghafouri, B.; Ernberg, M. Chronic musculoskeletal pain: Review of mechanisms and biochemical biomarkers as assessed by the microdialysis technique. J. Pain Res. 2014, 7, 313–326. [Google Scholar] [CrossRef] [Green Version]
- Mandel, A.L.; Ozdener, H.; Utermohlen, V. Identification of pro- and mature brain-derived neurotrophic factor in human saliva. Arch. Oral Biol. 2009, 54, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Krief, G.; Haviv, Y.; Deutsch, O.; Keshet, N.; Almoznino, G.; Zacks, B.; Palmon, A.; Aframian, D.J. Proteomic profiling of whole-saliva reveals correlation between Burning Mouth Syndrome and the neurotrophin signaling pathway. Sci. Rep. 2019, 9, 4794. [Google Scholar] [CrossRef] [Green Version]
- Segal, A.; Wong, D.T. Salivary diagnostics: Enhancing disease detection and making medicine better. Eur. J. Dent. Educ. Off. J. Assoc. Dent. Educ. Eur. 2008, 12, 22–29. [Google Scholar]
- Ney, L.J.; Matthews, A.; Hsu, C.K.; Zuj, D.V.; Nicholson, E.; Steward, T.; Nichols, D.; Graham, B.; Harrison, B.; Bruno, R.; et al. Cannabinoid polymorphisms interact with plasma endocannabinoid levels to predict fear extinction learning. Depress. Anxiety 2021, 38, 1087–1099. [Google Scholar] [CrossRef]
- Ney, L.; Stone, C.; Nichols, D.; Felmingham, K.; Bruno, R.; Matthews, A. Endocannabinoid reactivity to acute stress: Investigation of the relationship between salivary and plasma levels. Biol. Psychol. 2021, 159, 108022. [Google Scholar] [CrossRef]
- Matias, I.; Gatta-Cherifi, B.; Tabarin, A.; Clark, S.; Leste-Lasserre, T.; Marsicano, G.; Piazza, P.V.; Cota, D. Endocannabinoids measurement in human saliva as potential biomarker of obesity. PLoS ONE 2012, 7, e42399. [Google Scholar] [CrossRef] [Green Version]
- Tarragon, E.; Bindila, L.; Zimmer, P.; Lutz, B.; Meyer, J. Salivary endocannabinoids as mediators in the relationship between omega-6 and omega-3 fatty acid ratio intake from highly-processed foods and anthropometric markers of health in women. Int. J. Food Sci. Nutr. 2020, 71, 235–241. [Google Scholar] [CrossRef]
- Sharav, Y.B.R. Quintessence 2015. Orofacial Pain and Headache; Quintessence: Surrey, UK, 2015. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network * and Orofacial Pain Special Interest Groupdagger. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia Int. J. Headache 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Benoliel, R.; Sharav, Y.; Eliav, E. Neurovascular orofacial pain. J. Am. Dent. Assoc. 2010, 141, 1094–1096. [Google Scholar] [CrossRef] [Green Version]
- Haviv, Y.; Khan, J.; Zini, A.; Almoznino, G.; Sharav, Y.; Benoliel, R. Trigeminal neuralgia (part I): Revisiting the clinical phenotype. Cephalalgia Int. J. Headache 2016, 36, 730–746. [Google Scholar] [CrossRef] [PubMed]
- Haviv, Y.; Zadik, Y.; Sharav, Y.; Benoliel, R. Painful traumatic trigeminal neuropathy: An open study on the pharmacotherapeutic response to stepped treatment. J. Oral Facial Pain Headache 2014, 28, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Benoliel, R.; Gaul, C. Persistent idiopathic facial pain. Cephalalgia Int. J. Headache 2017, 37, 680–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benoliel, R.; Eliav, E.; Elishoov, H.; Sharav, Y. Diagnosis and treatment of persistent pain after trauma to the head and neck. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1994, 52, 1138–1147, discussion 1147–1138. [Google Scholar] [CrossRef]
- Haviv, Y.; Rettman, A.; Aframian, D.; Sharav, Y.; Benoliel, R. Myofascial pain: An open study on the pharmacotherapeutic response to stepped treatment with tricyclic antidepressants and gabapentin. J. Oral Facial Pain Headache 2015, 29, 144–151. [Google Scholar] [CrossRef]
- Haviv, Y.; Zini, A.; Etzioni, Y.; Klitinich, V.; Dobriyan, A.; Sharav, Y.; Benoliel, R.; Almoznino, G. The impact of chronic orofacial pain on daily life: The vulnerable patient and disruptive pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 58–66. [Google Scholar] [CrossRef]
- Aframian, D.J.; Helcer, M.; Livni, D.; Markitziu, A. Pilocarpine for the treatment of salivary glands’ impairment caused by radioiodine therapy for thyroid cancer. Oral Dis. 2006, 12, 297–300. [Google Scholar] [CrossRef]
- Azar, S.; Sherf-Dagan, S.; Nemirovski, A.; Webb, M.; Raziel, A.; Keidar, A.; Goitein, D.; Sakran, N.; Shibolet, O.; Tam, J.; et al. Circulating Endocannabinoids Are Reduced Following Bariatric Surgery and Associated with Improved Metabolic Homeostasis in Humans. Obes. Surg. 2019, 29, 268–276. [Google Scholar] [CrossRef]
- Baraghithy, S.; Smoum, R.; Drori, A.; Hadar, R.; Gammal, A.; Hirsch, S.; Attar-Namdar, M.; Nemirovski, A.; Gabet, Y.; Langer, Y.; et al. Magel2 Modulates Bone Remodeling and Mass in Prader-Willi Syndrome by Affecting Oleoyl Serine Levels and Activity. J. Bone Miner. Res. 2019, 34, 93–105. [Google Scholar] [CrossRef] [Green Version]
- Knani, I.; Earley, B.J.; Udi, S.; Nemirovski, A.; Hadar, R.; Gammal, A.; Cinar, R.; Hirsch, H.J.; Pollak, Y.; Gross, I.; et al. Targeting the endocannabinoid/CB1 receptor system for treating obesity in Prader-Willi syndrome. Mol. Metab. 2016, 5, 1187–1199. [Google Scholar] [CrossRef]
- Tartakover Matalon, S.; Azar, S.; Meiri, D.; Hadar, R.; Nemirovski, A.; Abu Jabal, N.; Konikoff, F.M.; Drucker, L.; Tam, J.; Naftali, T. Endocannabinoid Levels in Ulcerative Colitis Patients Correlate With Clinical Parameters and Are Affected by Cannabis Consumption. Front. Endocrinol. 2021, 12, 685289. [Google Scholar] [CrossRef]
- Walker, J.M.; Hohmann, A.G. Cannabinoid mechanisms of pain suppression. Handb. Exp. Pharmacol. 2005, 168, 509–554. [Google Scholar]
- Woodhams, S.G.; Sagar, D.R.; Burston, J.J.; Chapman, V. The role of the endocannabinoid system in pain. Handb. Exp. Pharmacol. 2015, 227, 119–143. [Google Scholar]
- Agarwal, N.; Pacher, P.; Tegeder, I.; Amaya, F.; Constantin, C.E.; Brenner, G.J.; Rubino, T.; Michalski, C.W.; Marsicano, G.; Monory, K.; et al. Cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors in nociceptors. Nat. Neurosci. 2007, 10, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.D.; Aanonsen, L.; Hargreaves, K.M. Hypoactivity of the spinal cannabinoid system results in NMDA-dependent hyperalgesia. J. Soc. Neurosci. 1998, 18, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Hong, S.; Stone, V.; Smith, P.J. Expression of cannabinoid CB1 receptors in models of diabetic neuropathy. J. Pharmacol. Exp. Ther. 2007, 323, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Ramesh, D.; D’Agata, A.; Starkweather, A.R.; Young, E.E. Contribution of Endocannabinoid Gene Expression and Genotype on Low Back Pain Susceptibility and Chronicity. Clin. J. Pain 2018, 34, 8–14. [Google Scholar] [CrossRef]
- Stensson, N.; Gerdle, B.; Ernberg, M.; Mannerkorpi, K.; Kosek, E.; Ghafouri, B. Increased Anandamide and Decreased Pain and Depression after Exercise in Fibromyalgia. Med. Sci. Sports Exerc. 2020, 52, 1617–1628. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Petzke, F.; Tolle, T.R.; Hauser, W. Cannabis-Based Medicines and Medical Cannabis in the Treatment of Nociplastic Pain. Drugs 2021, 81, 2103–2116. [Google Scholar] [CrossRef]
- Baggelaar, M.P.; Maccarrone, M.; van der Stelt, M. 2-Arachidonoylglycerol: A signaling lipid with manifold actions in the brain. Prog. Lipid Res. 2018, 71, 1–17. [Google Scholar] [CrossRef]
- Suardiaz, M.; Estivill-Torrus, G.; Goicoechea, C.; Bilbao, A.; Rodriguez de Fonseca, F. Analgesic properties of oleoylethanolamide (OEA) in visceral and inflammatory pain. Pain 2007, 133, 99–110. [Google Scholar] [CrossRef]
- Wang, X.; Miyares, R.L.; Ahern, G.P. Oleoylethanolamide excites vagal sensory neurones, induces visceral pain and reduces short-term food intake in mice via capsaicin receptor TRPV1. J. Physiol. 2005, 564, 541–547. [Google Scholar] [CrossRef]
- De Fonseca, F.R.; Del Arco, I.; Bermudez-Silva, F.J.; Bilbao, A.; Cippitelli, A.; Navarro, M. The endocannabinoid system: Physiology and pharmacology. Alcohol Alcohol. 2005, 40, 2–14. [Google Scholar] [CrossRef]
- De Fonseca, F.R.; Navarro, M.; Gomez, R.; Escuredo, L.; Nava, F.; Fu, J.; Murillo-Rodriguez, E.; Giuffrida, A.; LoVerme, J.; Gaetani, S.; et al. An anorexic lipid mediator regulated by feeding. Nature 2001, 414, 209–212. [Google Scholar] [CrossRef] [Green Version]
- Pellkofer, H.L.; Havla, J.; Hauer, D.; Schelling, G.; Azad, S.C.; Kuempfel, T.; Magerl, W.; Huge, V. The major brain endocannabinoid 2-AG controls neuropathic pain and mechanical hyperalgesia in patients with neuromyelitis optica. PLoS ONE 2013, 8, e71500. [Google Scholar]
- Fanelli, F.; Mezzullo, M.; Belluomo, I.; Di Lallo, V.D.; Baccini, M.; Ibarra Gasparini, D.; Casadio, E.; Mastroroberto, M.; Vicennati, V.; Gambineri, A.; et al. Plasma 2-arachidonoylglycerol is a biomarker of age and menopause related insulin resistance and dyslipidemia in lean but not in obese men and women. Mol. Metab. 2017, 6, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Liktor-Busa, E.; Lipinski, A.A.; Couture, S.; Balasubramanian, S.; Aicher, S.A.; Langlais, P.R.; Vanderah, T.W.; Largent-Milnes, T.M. Sex differences in the expression of the endocannabinoid system within V1M cortex and PAG of Sprague Dawley rats. Biol. Sex Differ. 2021, 12, 60. [Google Scholar] [CrossRef] [PubMed]
- Rovner, G.S.; Sunnerhagen, K.S.; Bjorkdahl, A.; Gerdle, B.; Borsbo, B.; Johansson, F.; Gillanders, D. Chronic pain and sex-differences; women accept and move, while men feel blue. PLoS ONE 2017, 12, e0175737. [Google Scholar] [CrossRef] [Green Version]
- Ney, L.J.; Felmingham, K.L.; Bruno, R.; Matthews, A.; Nichols, D.S. Simultaneous quantification of endocannabinoids, oleoylethanolamide and steroid hormones in human plasma and saliva. J. Chromatogr. B. Anal. Technol. Biomed. Life Sci. 2020, 1152, 122252. [Google Scholar] [CrossRef]
- Mennella, I.; Di Monaco, R.; Balazy, A.; Ferracane, R.; Miele, N.A.; Cavella, S.; Vitaglione, P.S. Alivary endocannabinoids and N-acylethanolamines upon mastication of a semisolid food: Implications in fat taste, appetite and food liking. Food Funct. 2018, 9, 476–484. [Google Scholar] [CrossRef]
- Staud, R. Abnormal endogenous pain modulation is a shared characteristic of many chronic pain conditions. Expert Rev. Neurother. 2012, 12, 577–585. [Google Scholar] [CrossRef]
- Khan, J.; Korczeniewska, O.; Benoliel, R.; Kalladka, M.; Eliav, E.; Nasri-Heir, C. Age and gender differences in mechanically induced intraoral temporal summation and conditioned pain modulation in healthy subjects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 134–141. [Google Scholar] [CrossRef]
- Yarnitsky, D. Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): Its relevance for acute and chronic pain states. Curr. Opin. Anaesthesiol. 2010, 23, 611–615. [Google Scholar] [CrossRef]
- Hillard, C.J. Circulating Endocannabinoids: From Whence Do They Come and where are They Going? Neuropsychopharmacoly 2018, 43, 155–172. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Endocannabinoids (eCBs) | fmol/mg (Mean ± SD) | Women (Mean ± SD) | Men (Mean ± SD) | p Value |
|---|---|---|---|---|
| AEA | 0.17 ± 0.3 | 0.15 ± 0.17 | 0.21 ± 0.69 | 0.28 |
| 2-AG | 41.3 ± 40.6 | 44.15 ± 45.32 | 37.71 ± 29.25 | 0.40 |
| OEA | 49.1 ± 59.8 | 37.93 ± 50.35 | 73.16 ± 70.33 | <0.001 |
| PEA | 11.5 ± 11.8 | 8.34 ± 7.96 | 17.73 ± 15.30 | <0.001 |
| AA | 7659.1 ± 1876.1 | 12112.25 ± 1154 | 3262.18 ± 2452 | <0.001 |
| * Group | AA (Mean ± SD) | PEA (Mean ± SD) | OEA (Mean ± SD) | 2-AG (Mean ± SD) | AEA (Mean ± SD) |
| Control | 2327.1 ± 2539 | 12.9 ± 11.75 | 67.7 ± 77.09 | 54.71 ± 36.47 | 0.2 ± 0.18 |
| Pain | 1710.2 ± 1552 | 10.7 ± 11.93 | 41.2 ± 47.04 | 35.88 ± 41.29 | 0.17 ± 0.2 |
| p-value | 0.09 | 0.34 | 0.02 | 0.01 | 0.94 |
| Musculoskeletal | 2177.3 ± 1868 | 9.9 ± 9.30 | 40.4 ± 37.06 | 39.6 ± 40.91 | 0.1 ± 0.14 |
| Neurovascular | 1354.3 ± 1354 | 8.8 ± 10.21 | 35.6 ± 40.31 | 33.2 ± 41.45 | 0.0 ± 0.09 |
| Neuropathic | 1749.80 ± 143 | 13.2 ± 14.71 | 47.3 ± 58.63 | 35.9 ± 42.56 | 0.2 ± 0.45 |
| p-value | 0.17 | 0.36 | 0.11 | 0.09 | 0.07 |
| Group | eCBs | Pain (mean ± SD) | Control (mean ± SD) | p-Value |
|---|---|---|---|---|
| Neurovascular | AEA | 0.09 ± 0.09 | 0.17 ± 0.18 | 0.02 |
| OEA | 35.65 ± 40.31 | 67.7 ± 77.09 | 0.04 | |
| AA | 1354.3 ± 1386.94 | 2327.15 ± 2539.27 | 0.06 | |
| Neuropathic | 2-AG | 35.97 ± 42.56 | 54.71 ± 36.47 | 0.05 |
| Musculoskeletal | None | - | - | NS |
| Group | eCBs | Pain Level * | n | fmol/mg Protein (Mean ± SD) | p-Value |
|---|---|---|---|---|---|
| Neurovascular | OEA | Mild | 3 | 85.42 ± 97.27 | 0.097 |
| Moderate | 7 | 30.83 ± 24.87 | |||
| Severe | 19 | 31.65 ± 30.98 | |||
| PEA | Mild | 2 | 22.44 ± 27.85 | 0.062 | |
| Moderate | 7 | 7.97 ± 6.86 | |||
| Severe | 14 | 7.64 ± 5.86 | |||
| Neuropathic | PEA | Mild | 3 | 17.26 ± 9.96 | 0.067 |
| Moderate | 7 | 5.57 ± 4.44 | |||
| Severe | 14 | 9.02 ± 7.14 | |||
| AA | Mild | 2 | 4027.43 ± 596 | 0.028 | |
| Moderate | 7 | 1214.79 ± 1336 | |||
| Severe | 14 | 1514.9 ± 1202 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haviv, Y.; Georgiev, O.; Gaver-Bracha, T.; Hamad, S.; Nemirovski, A.; Hadar, R.; Sharav, Y.; Aframian, D.J.; Brotman, Y.; Tam, J. Reduced Endocannabinoid Tone in Saliva of Chronic Orofacial Pain Patients. Molecules 2022, 27, 4662. https://doi.org/10.3390/molecules27144662
Haviv Y, Georgiev O, Gaver-Bracha T, Hamad S, Nemirovski A, Hadar R, Sharav Y, Aframian DJ, Brotman Y, Tam J. Reduced Endocannabinoid Tone in Saliva of Chronic Orofacial Pain Patients. Molecules. 2022; 27(14):4662. https://doi.org/10.3390/molecules27144662
Chicago/Turabian StyleHaviv, Yaron, Olga Georgiev, Tal Gaver-Bracha, Sharleen Hamad, Alina Nemirovski, Rivka Hadar, Yair Sharav, Doron J. Aframian, Yariv Brotman, and Joseph Tam. 2022. "Reduced Endocannabinoid Tone in Saliva of Chronic Orofacial Pain Patients" Molecules 27, no. 14: 4662. https://doi.org/10.3390/molecules27144662