
Plant Essential Oils as Healthy Functional Ingredients of Nutraceuticals and Diet Supplements: A Review




Abstract
:1. Introduction
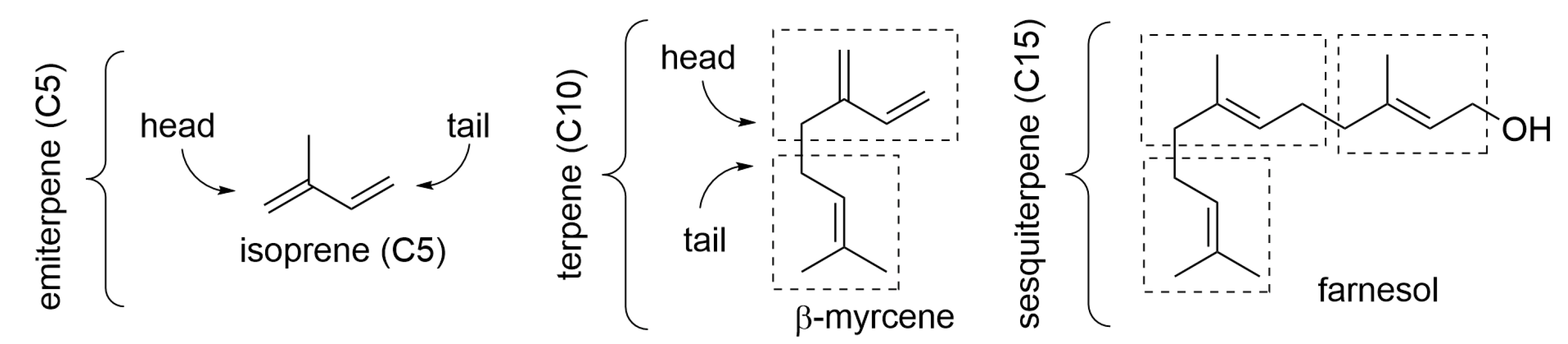
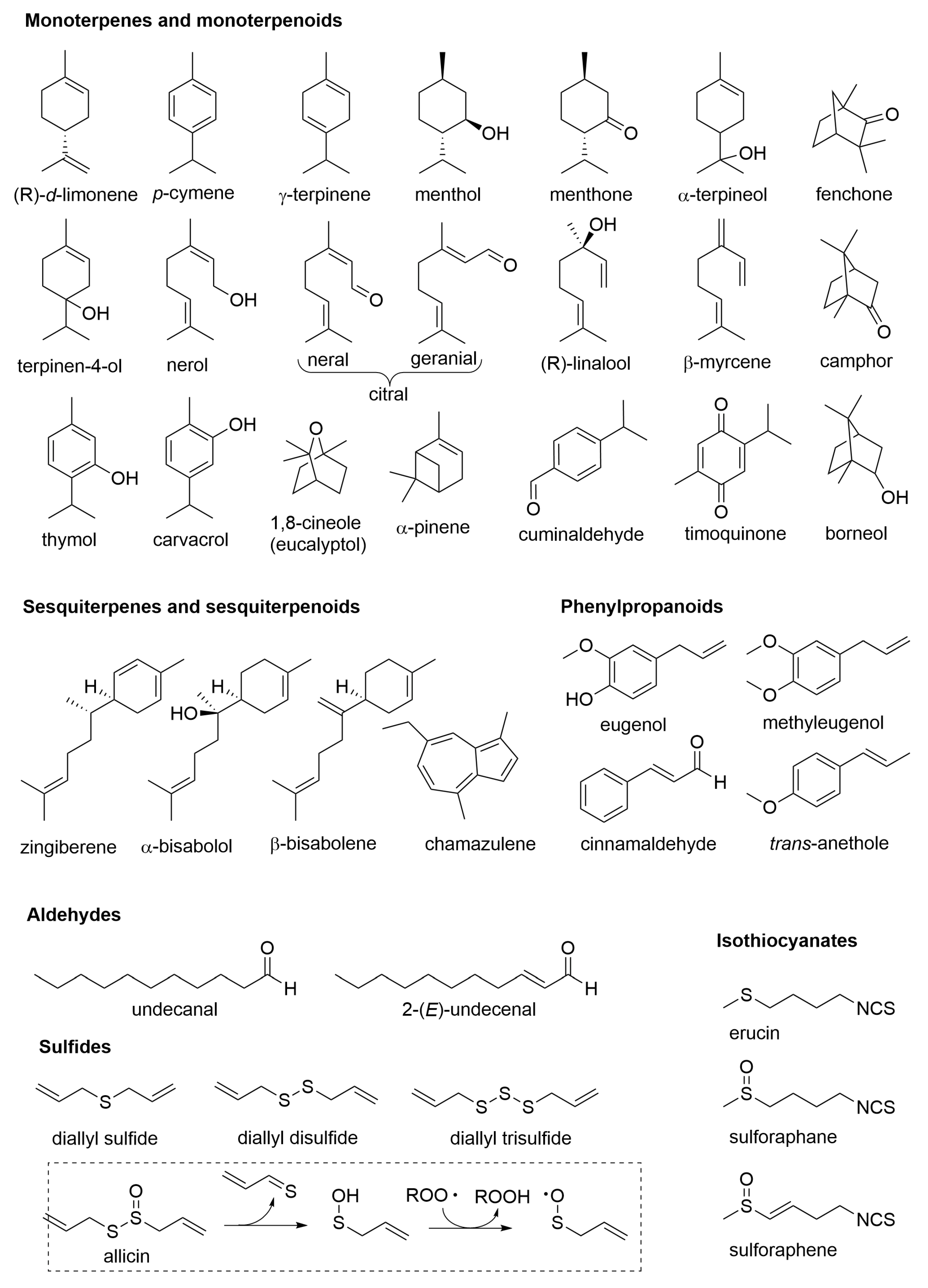
2. Composition of Essential Oils
3. Nutraceuticals, Diet Supplements, and Functional Food
4. Essential Oils Helpful in the Irritable Bowel Syndrome (IBS)
5. Essential Oils Helpful in Inflammatory Bowel Disease (IBD) and in the Prevention of Colorectal Cancer (CRC)
6. Essential Oils in Probiotic Food and Supplements for Regulation of Gut Microflora
7. Essential Oils for Gastric Protection and to Alleviate Peptic Ulcer
8. Essential Oils Useful in the Management of Metabolic Disorders
8.1. Essential Oils in Diabetes and Hyperglycemia
8.2. Essential Oils in Dyslipidemia, Metabolic Syndrome, and Obesity
9. Essential Oils to Protect Liver Function and Stimulate Digestion
10. Essential Oils for Diuresis and Protection of the Urinary Tract
11. Essential Oils to Reduce Inflammation and Pain
12. Essential Oils with Immunomodulatory and Anti-Influenza Activity
13. Essential Oils for Neuroprotection and Modulation of Mood and Cognitive Function
14. Conclusive Remarks and Perspective
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Marongiu, B.; Porceddu, S.; Piras, A.; Falconieri, D. Traditional and modern methods for the preparation of essential oils. In Essential Oils and Natural Food Additives: Composition, Applications, Antioxidant and Antimicrobial Properties; Valgimigli, L., Ed.; Nova Science Publishing: New York, NY, USA, 2012; pp. 25–46. ISBN 978-1-62100-241-3. [Google Scholar]
- Zhang, J.; Zhang, M.; Ju, R.; Chen, K.; Bhandari, B.; Wang, H. Advances in efficient extraction of essential oils from spices and its application in food industry: A critical review. Crit. Rev. Food Sci. Nutr. 2022, 2092834. [Google Scholar] [CrossRef] [PubMed]
- Mancianti, F.; Ebani, V.V. Biological Activity of Essential Oils. Molecules 2020, 25, 678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhifi, W.; Bellili, S.; Jazi, S.; Bahloul, N.; Mnif, W. Essential Oils’ Chemical Characterization and Investigation of Some Biological Activities: A Critical Review. Medicines 2016, 3, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, L. Essential oils: An overview on origins, chemistry, properties and uses. In Essential Oils and Natural Food Additives: Composition, Applications, Antioxidant and Antimicrobial Properties; Valgimigli, L., Ed.; Nova Science Publishing: New York, NY, USA, 2012; pp. 1–24. ISBN 978-1-62100-241-3. [Google Scholar]
- Valnet, J. The Practice of Aromatherapy. A Classic Compendium of Plant Medicines and Their Healing Properties; Tisserand, R.B., Ed.; Healing Arts Press: Rochester, NY, USA, 1982; ISBN 0-89281-398-9. [Google Scholar]
- Price, S.; Price, L. Aromatherapy for Health Professionals, 4th ed.; Elsevier: London, UK, 2012; ISBN 978-0-7020-3564-7. [Google Scholar]
- Farrar, A.J.; Farrar, F.C. Clinical Aromatherapy. Nurs. Clin. N. Am. 2020, 55, 489–504. [Google Scholar] [CrossRef] [PubMed]
- Ali, B.; Al-Wabel, N.A.; Shams, S.; Ahamad, A.; Khan, S.A.; Anwar, F. Essential oils used in aromatherapy: A systemic review. Asian Pac. J. Trop. Biomed. 2015, 5, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Baptista-Silva, S.; Borges, S.; Ramos, O.L.; Pintado, M.; Sarmento, B. The progress of essential oils as potential therapeutic agents: A review. J. Essent. Oil Res. 2020, 32, 279–295. [Google Scholar] [CrossRef]
- Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=182. (accessed on 22 December 2022).
- Guo, Y.; Baschieri, A.; Amorati, R.; Valgimigli, L. Synergic antioxidant activity of γ-terpinene with phenols and polyphenols enabled by hydroperoxyl radicals. Food Chem. 2021, 345, 128468. [Google Scholar] [CrossRef]
- Singh, S.; Chaurasia, P.K.; Bharati, S.L. Functional roles of essential oils as an effective alternative of synthetic food preservatives: A review. J. Food Process. Preserv. 2022, 46, e16804. [Google Scholar] [CrossRef]
- Falleh, H.; Ben Jemaa, M.; Saada, M.; Ksouri, R. Essential oils: A promising eco-friendly food preservative. Food Chem. 2020, 330, 127268. [Google Scholar] [CrossRef]
- Masyita, A.; Sari, R.M.; Astuti, A.D.; Yasir, B.; Rumata, N.R.; Emran, T.B.; Nainu, F.; Simal-Gandara, J. Terpenes and terpenoids as main bioactive compounds of essential oils, their roles in human health and potential application as natural food preservatives. Food Chem. X 2022, 13, 100217. [Google Scholar] [CrossRef]
- Maurya, A.; Prasad, J.; Das, S.; Dwivedy, A.K. Essential Oils and Their Application in Food Safety. Front. Sustain. Food Syst. 2021, 5, 653420. [Google Scholar] [CrossRef]
- Amiri, A.; Mottaghipisheh, J.; Jamshidi-Kia, F.; Saeidi, K.; Vitalini, S.; Iriti, M. Antimicrobial Potencies of Major Functional Foods’ Essential Oils in Liquid and Vapor Phases: A Short Review. Appl. Sci. 2020, 10, 8103. [Google Scholar] [CrossRef]
- Granata, G.; Stracquadanio, S.; Leonardi, M.; Napoli, E.; Malandrino, G.; Cafiso, V.; Stefani, S.; Geraci, C. Oregano and Thyme Essential Oils Encapsulated in Chitosan Nanoparticles as Effective Antimicrobial Agents against Foodborne Pathogens. Molecules 2021, 26, 4055. [Google Scholar] [CrossRef]
- Amorati, R.; Foti, M.C.; Valgimigli, L. Antioxidant Activity of Essential Oils. J. Agric. Food Chem. 2013, 61, 10835–10847. [Google Scholar] [CrossRef]
- Guo, Y.; Pizzol, R.; Gabbanini, S.; Baschieri, A.; Amorati, R.; Valgimigli, L. Absolute Antioxidant Activity of Five Phenol-Rich Essential Oils. Molecules 2021, 26, 5237. [Google Scholar] [CrossRef]
- Baschieri, A.; Ajvazi, M.D.; Tonfack, J.L.F.; Valgimigli, L.; Amorati, R. Explaining the antioxidant activity of some common non-phenolic components of essential oils. Food Chem. 2017, 232, 656–663. [Google Scholar] [CrossRef]
- Stevanović, Z.D.; Bošnjak-Neumüller, J.; Pajić-Lijaković, I.; Raj, J.; Vasiljević, M. Essential Oils as Feed Additives—Future Perspectives. Molecules 2018, 23, 1717. [Google Scholar] [CrossRef] [Green Version]
- Christaki, E.; Giannenas, I.; Bonos, E.; Florou-Paneri, P. Innovative uses of aromatic plants as natural supplements in nutrition. In Feed Additives. Aromatic Plants and Herbs in Animal Nutrition and Health; Florou-Paneri, P., Efterpi Christaki, E., Giannenas, I., Eds.; Elsevier Academic Press: London, UK, 2020; pp. 19–34. [Google Scholar] [CrossRef]
- Barillari, J.; Canistro, D.; Paolini, M.; Ferroni, F.; Pedulli, G.F.; Iori, R.; Valgimigli, L. Direct Antioxidant Activity of Purified Glucoerucin, the Dietary Secondary Metabolite Contained in Rocket (Eruca sativa Mill.) Seeds and Sprouts. J. Agric. Food Chem. 2005, 53, 2475–2482. [Google Scholar] [CrossRef]
- Barillari, J.; Iori, R.; Papi, A.; Orlandi, M.; Bartolini, G.; Gabbanini, S.; Pedulli, G.F.; Valgimigli, L. Kaiware Daikon (Raphanus sativus L.) Extract: A Naturally Multipotent Chemopreventive Agent. J. Agric. Food Chem. 2008, 56, 7823–7830. [Google Scholar] [CrossRef]
- Papi, A.; Orlandi, M.; Bartolini, G.; Barillari, J.; Iori, R.; Paolini, M.; Ferroni, F.; Fumo, M.G.; Pedulli, G.F.; Valgimigli, L. Cytotoxic and Antioxidant Activity of 4-Methylthio-3-butenyl Isothiocyanate from Raphanus sativus L. (Kaiware Daikon) Sprouts. J. Agric. Food Chem. 2008, 56, 875–883. [Google Scholar] [CrossRef]
- Valgimigli, L.; Iori, R. Antioxidant and pro-oxidant capacities of ITCs. Environ. Mol. Mutagen. 2009, 50, 222–237. [Google Scholar] [CrossRef]
- Lucchi, E.; Matera, R. Essential oils as active ingredients in functional food and nutraceutical formulations. In Essential Oils and Natural Food Additives: Composition, Applications, Antioxidant and Antimicrobial Properties; Valgimigli, L., Ed.; Nova Science Publishing: New York, NY, USA, 2012; pp. 1–24. ISBN 978-1-62100-241-3. [Google Scholar]
- del Castillo, M.D.; Iriondo-DeHond, A.; Martirosyan, D.M. Are Functional Foods Essential for Sustainable Health? Nutr. Food Sci. 2018, 2, 1015. [Google Scholar]
- Available online: https://www.efsa.europa.eu/en/topics/topic/food-supplements (accessed on 21 December 2022).
- Díaz, L.D.; Fernández-Ruiz, V.; Cámara, M. An international regulatory review of food health-related claims in functional food products labeling. J. Funct. Foods 2020, 68, 103896. [Google Scholar] [CrossRef]
- Rahimi, R. Herbal medicines for the management of irritable bowel syndrome: A comprehensive review. World J. Gastroenterol. 2012, 18, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, A. Therapeutic Uses of Peppermint—A Review. J. Pharm. Sci. Res. 2015, 7, 474. [Google Scholar]
- Hawthorn, M.; Ferrante, J.; Luchowski, E.; Rutledge, A.; Wei, X.Y.; Triggle, D.J. The actions of peppermint oil and menthol on calcium channel dependent processes in intestinal, neuronal and cardiac preparations. Aliment. Pharmacol. Ther. 1988, 2, 101–118. [Google Scholar] [CrossRef]
- Ford, A.C.; Talley, N.J.; Spiegel, B.M.R.; E Foxx-Orenstein, A.; Schiller, L.; Quigley, E.M.M.; Moayyedi, P. Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: Systematic review and meta-analysis. BMJ 2008, 337, a2313. [Google Scholar] [CrossRef] [Green Version]
- Merat, S.; Khalili, S.; Mostajabi, P.; Ghorbani, A.; Ansari, R.; Malekzadeh, R. The Effect of Enteric-Coated, Delayed-Release Peppermint Oil on Irritable Bowel Syndrome. Dig. Dis. Sci. 2010, 55, 1385–1390. [Google Scholar] [CrossRef]
- Ingrosso, M.R.; Ianiro, G.; Nee, J.; Lembo, A.J.; Moayyedi, P.; Black, C.J.; Ford, A.C. Systematic review and meta-analysis: Efficacy of peppermint oil in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2022, 56, 932–941. [Google Scholar] [CrossRef]
- Mosaffa-Jahromi, M.; Lankarani, K.B.; Pasalar, M.; Afsharypuor, S.; Tamaddon, A.-M. Efficacy and safety of enteric coated capsules of anise oil to treat irritable bowel syndrome. J. Ethnopharmacol. 2016, 194, 937–946. [Google Scholar] [CrossRef]
- Tanveer, M.; Wagner, C.; Haq, M.I.U.; Ribeiro, N.C.; Rathinasabapathy, T.; Butt, M.S.; Shehzad, A.; Komarnytsky, S. Spicing up gastrointestinal health with dietary essential oils. Phytochem. Rev. 2020, 19, 243–263. [Google Scholar] [CrossRef]
- Amorati, R.; Lynett, P.T.; Valgimigli, L.; Pratt, D.A. The Reaction of Sulfenic Acids with Peroxyl Radicals: Insights into the Radical-Trapping Antioxidant Activity of Plant-Derived Thiosulfinates. Chem. A Eur. J. 2012, 18, 6370–6379. [Google Scholar] [CrossRef]
- McGrath, A.J.; Garrett, G.E.; Valgimigli, L.; Pratt, D.A. The Redox Chemistry of Sulfenic Acids. J. Am. Chem. Soc. 2010, 132, 16759–16761. [Google Scholar] [CrossRef]
- Zielinski, Z.; Presseau, N.; Amorati, R.; Valgimigli, L.; Pratt, D.A. Redox Chemistry of Selenenic Acids and the Insight It Brings on Transition State Geometry in the Reactions of Peroxyl Radicals. J. Am. Chem. Soc. 2014, 136, 1570–1578. [Google Scholar] [CrossRef]
- Gabbai-Armelin, P.R.; Sales, L.S.; Ferrisse, T.M.; De Oliveira, A.B.; De Oliveira, J.R.; Giro, E.M.A.; Brighenti, F.L. A systematic review and meta-analysis of the effect of thymol as an anti-inflammatory and wound healing agent. Phytother. Res. 2022, 36, 3415–3443. [Google Scholar] [CrossRef]
- Subramaniyam, S.; Yang, S.; Diallo, B.N.; Fanshu, X.; Lei, L.; Li, C.; Bishop, O.T.; Bhattacharyya, S. Oral Phyto-thymol ameliorates the stress induced IBS symptoms. Sci. Rep. 2020, 10, 13900. [Google Scholar] [CrossRef]
- Toschi, A.; Tugnoli, B.; Rossi, B.; Piva, A.; Grilli, E. Thymol modulates the endocannabinoid system and gut chemosensing of weaning pigs. BMC Vet. Res. 2020, 16, 289. [Google Scholar] [CrossRef]
- Mahboubi, M. Therapeutic Potential of Zataria multiflora Boiss in Treatment of Irritable Bowel Syndrome (IBS). J. Diet. Suppl. 2019, 16, 119–128. [Google Scholar] [CrossRef]
- Jamalizadeh, H.; Ahmadi, B.; Shariffar, F.; Ansari, M.; Setayesh, M.; Shahesmaeili, A.; Tajadini, H. Clinical evaluation of the effect of Zataria multiflora Boiss and Trachyspermum copticum (L.) on the patients with irritable bowel syndrome. Explore 2022, 18, 342–346. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Portincasa, P.; Maes, N.; Albert, A. Efficacy of bio-optimized extracts of turmeric and essential fennel oil on the quality of life in patients with irritable bowel syndrome. Ann. Gastroenterol. 2018, 31, 685–691. [Google Scholar] [CrossRef]
- Di Vito, M.; Bellardi, M.G.; Sanguinetti, M.; Mondello, F.; Girolamo, A.; Barbanti, L.; Garzoli, S.; Sabatino, M.; Ragno, R.; Vitali, A.; et al. Potent In Vitro Activity of Citrus aurantium Essential Oil and Vitis vinifera Hydrolate Against Gut Yeast Isolates from Irritable Bowel Syndrome Patients—The Right Mix for Potential Therapeutic Use. Nutrients 2020, 12, 1329. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Aguliar, R.M.; Wantia, N.; Clavel, T.; Vehreschild, M.J.; Buch, T.; Bajbouj, M.; Haller, D.; Busch, D.; Schmid, R.M.; Stein-Thoeringer, C.K. An Open-Labeled Study on Fecal Microbiota Transfer in Irritable Bowel Syndrome Patients Reveals Improvement in Abdominal Pain Associated with the Relative Abundance of Akkermansia Muciniphila. Digestion 2018, 100, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Gönczi, L.; Lakatos, P.L.; Burisch, J. The Burden of Inflammatory Bowel Disease in Europe in 2020. J. Crohn’s Colitis 2021, 15, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Spisni, E.; Petrocelli, G.; Imbesi, V.; Spigarelli, R.; Azzinnari, D.; Sarti, M.D.; Campieri, M.; Valerii, M.C. Antioxidant, Anti-Inflammatory, and Microbial-Modulating Activities of Essential Oils: Implications in Colonic Pathophysiology. Int. J. Mol. Sci. 2020, 21, 4152. [Google Scholar] [CrossRef]
- Direito, R.; Rocha, J.; Lima, A.; Gonçalves, M.M.; Duarte, M.P.; Mateus, V.; Sousa, C.; Fernandes, A.; Pinto, R.; Ferreira, R.B.; et al. Reduction of Inflammation and Colon Injury by a Spearmint Phenolic Extract in Experimental Bowel Disease in Mice. Medicines 2019, 6, 65. [Google Scholar] [CrossRef] [Green Version]
- Almanea, A.; El-Aziz, G.S.A.; Ahmed, M.M.M. The Potential Gastrointestinal Health Benefits of Thymus Vulgaris Essential Oil: A Review. Biomed. Pharmacol. J. 2019, 12, 1793–1799. [Google Scholar] [CrossRef]
- De Cássia da Silveira e Sá, R.; Andrade, L.N.; de Sousa, D.P. A Review on Anti-Inflammatory Activity of Monoterpenes. Molecules 2013, 18, 1227–1254. [Google Scholar] [CrossRef]
- Oliyaei, N.; Tanideh, N.; Nasirifar, S.Z. Application of Essential Oils in the Treatment of Inflammatry Bowel Disease. In Essential Oils: Advances in Extractions and Biological Applications; Santana de Oliveira, M., de Aguilar Andrade, H., Eds.; IntechOpen: London, UK, 2022; pp. 139–152. ISBN 978-1-80355-754-0. [Google Scholar]
- Sahib, N.G.; Anwar, F.; Gilani, A.-H.; Hamid, A.A.; Saari, N.; Alkharfy, K.M. Coriander (Coriandrum sativum L.): A Potential Source of High-Value Components for Functional Foods and Nutraceuticals—A Review. Phytother. Res. 2013, 27, 1439–1456. [Google Scholar] [CrossRef] [Green Version]
- Laribi, B.; Kouki, K.; M’Hamdi, M.; Bettaieb, T. Coriander (Coriandrum sativum L.) and its bioactive constituents. Fitoterapia 2015, 103, 9–26. [Google Scholar] [CrossRef]
- Heidari, B.; Sajjadi, S.E.; Minaiyan, M. Effect of Coriandrum sativum hydroalcoholic extract and its essential oil on acetic acid- induced acute colitis in rats. Avicenna J. Phytomedicine 2016, 6, 205–214. [Google Scholar] [CrossRef]
- Musumeci, L.; Maugeri, A.; Cirmi, S.; Lombardo, G.E.; Russo, C.; Gangemi, S.; Calapai, G.; Navarra, M. Citrus fruits and their flavonoids in inflammatory bowel disease: An overview. Nat. Prod. Res. 2020, 34, 122–136. [Google Scholar] [CrossRef]
- Gonzalez-Ramírez, A.E.; Gonzalez-Trujano, M.E.; Hernandez-Leon, A.; Valle-Dorado, M.G.; Carballo-Villalobos, A.; Oroz-co-Suarez, S.; Alvarado-Vasquez, N.; e Lopez-Munoz, F.J. Limonene from Agastache mexicana essential oil produces antinociceptive effects, gastrointestinal protection and improves experimental ulcerative colitis. J. Ethnopharmacol. 2021, 280, 114462. [Google Scholar] [CrossRef]
- Estrada-Reyes, R.; Aguirre Hern´andez, E.; García-Arg´aez, A.; Soto Hern´andez, M.; Linares, E.; Bye, R.; Heinze, G.; Mar-tínez-V´azquez, M. Comparative chemical composition of Agastache mexicana subsp. mexicana and A. mexicana subsp. xolocotziana. Biochem. Syst. Ecol. 2004, 32, 685–694. [Google Scholar] [CrossRef]
- Baker, J.; Brown, K.; Rajendiran, E.; Yip, A.; DeCoffe, D.; Dai, C.; Molcan, E.; Chittick, S.A.; Ghosh, S.; Mahmoud, S.; et al. Medicinal lavender modulates the enteric microbiota to protect against Citrobacter rodentium-induced colitis. Am. J. Physiol. Liver Physiol. 2012, 303, G825–G836. [Google Scholar] [CrossRef]
- Wang, Y.; Zou, J.; Jia, Y.; Zhang, X.; Wang, C.; Shi, Y.; Guo, D.; Wu, Z.; Wang, F. The Mechanism of Lavender Essential Oil in the Treatment of Acute Colitis Based on “Quantity-Effect” Weight Coefficient Network Pharmacology. Front. Pharmacol. 2021, 12, 644140. [Google Scholar] [CrossRef]
- Majnooni, M.B.; Mohammadi, S.; Bahrami, G.; Noori, E.M.; Farzaei, M.H. Chemical Composition, Total Phenolic Content, and Anti-Ulcerative Colitis Effects of Extract and Essential Oil of Cupressus arizonica Greene Fruits. Tradit. Integr. Med. 2022, 7, 310–318. [Google Scholar] [CrossRef]
- Kim, D.-S.; Lee, H.-J.; Jeon, Y.-D.; Han, Y.-H.; Kee, J.-Y.; Kim, H.-J.; Shin, H.-J.; Kang, J.; Lee, B.S.; Kim, S.-H.; et al. Alpha-Pinene Exhibits Anti-Inflammatory Activity Through the Suppression of MAPKs and the NF-κB Pathway in Mouse Peritoneal Macrophages. Am. J. Chin. Med. 2015, 43, 731–742. [Google Scholar] [CrossRef]
- Minaiyan, M.; Ghannadi, A.R.; Afsharipour, M.; Mahzouni, P. Effects of extract and essential oil of Rosmarinus officinalis L. on TNBS-induced colitis in rats. Res. Pharm. Sci. 2011, 6, 13–21. [Google Scholar]
- Khosropour, P.; Sajjadi, S.-E.; Talebi, A.; Minaiyan, M. Anti-inflammatory effect of Myrtus communis hydroalcoholic extract and essential oil on acetic acid-induced colitis in rats. J. Rep. Pharm. Sci. 2019, 8, 204. [Google Scholar] [CrossRef]
- Alshahrani, A.; Ali, A. Pre-Clinical Safety and Efficacy Evaluation of a Herbal Nanoemulsion-Based Formulation for Treating Inflammatory Bowel Disease. J. AOAC Int. 2022, 105, 1153–1161. [Google Scholar] [CrossRef]
- Petrocelli, G.; Farabegoli, F.; Valerii, M.; Giovannini, C.; Sardo, A.; Spisni, E. Molecules Present in Plant Essential Oils for Prevention and Treatment of Colorectal Cancer (CRC). Molecules 2021, 26, 885. [Google Scholar] [CrossRef] [PubMed]
- Nutrition Division, FAO/WHO. Probiotics in food. Health and nutritional properties and guidelines for evaluation. FAO Food Nutr. Pap. (FAO) 2006, 85, 1–56. Available online: https://www.fao.org/publications/card/en/c/7c102d95-2fd5-5b22-8faf-f0b2e68dfbb6/ (accessed on 1 December 2022).
- Zmora, N.; Zilberman-Schapira, G.; Suez, J.; Mor, U.; Dori-Bachash, M.; Bashiardes, S.; Kotler, E.; Zur, M.; Regev-Lehavi, D.; Brik, R.B.-Z.; et al. Personalized Gut Mucosal Colonization Resistance to Empiric Probiotics Is Associated with Unique Host and Microbiome Features. Cell 2018, 174, 1388–1405.e21. [Google Scholar] [CrossRef] [PubMed]
- Probiotics. Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/Probiotics-HealthProfessional/ (accessed on 1 December 2022).
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deep, S.; Karmakar, S.; Khare, R.S.; Ojha, S.; Kundu, K.; Kundu, S. Development of Probiotic Candidate in Combination with Essential Oils from Medicinal Plant and Their Effect on Enteric Pathogens: A Review. Gastroenterol. Res. Pract. 2012, 2012, 457150. [Google Scholar] [CrossRef]
- Unusan, N. Essential oils and microbiota: Implications for diet and weight control. Trends Food Sci. Technol. 2020, 104, 60–71. [Google Scholar] [CrossRef]
- Ishtiaq, A.; Manyi, H.; Yan, L.; Jianyou, Z.; Yuting, D.; Fei, L. Fortification of yogurt with bioactive functional foods and ingredients and associated challenges—A review. Trends Food Sci. Technol. 2022, 129, 558–580. [Google Scholar] [CrossRef]
- Rehman, A.; Qunyi, T.; Rizwan Sharif, H.; Korma, S.A.; Karim, A.; Faisal Manzoor, M.; Mehmood, A.; Waheed Iqbal, M.; Raza, H.; Ali, A.; et al. Biopolymer based nanoemulsion delivery system: An effective approach to boost the antioxidant potential of essential oil in food products. Carbohydr. Polym. Technol. Appl. 2021, 2, 100082. [Google Scholar] [CrossRef]
- Sani, I.K.; Khaledabad, M.A.; Pirsa, S.; Kia, E.M. Physico-chemical, organoleptic, antioxidative and release characteristics of flavoured yoghurt enriched with microencapsulated Melissa officinalis essential oil. Int. J. Dairy Technol. 2020, 73, 542–551. [Google Scholar] [CrossRef]
- Keshavarzi, M.; Sharifan, A.; Ardakani, S.A.Y. Effect of the ethanolic extract and essential oil of Ferulago angulata (Schlecht.) Boiss. on protein, physicochemical, sensory, and microbial characteristics of probiotic yogurt during storage time. Food Sci. Nutr. 2021, 9, 197–208. [Google Scholar] [CrossRef]
- Azizkhani, M.; Parsaeimehr, M. Probiotics survival, antioxidant activity and sensory properties of yogurt flavored with herbal essential oils. Int. Food Res. J. 2018, 25, 921–927. [Google Scholar]
- Hamed, A.M.; Awad, A.A.; Abdel-Mobdy, A.E.; Alzahrani, A.; Salamatullah, A.M. Buffalo Yogurt Fortified with Eucalyptus (Eucalyptus camaldulensis) and Myrrh (Commiphora Myrrha) Essential Oils: New Insights into the Functional Properties and Extended Shelf Life. Molecules 2021, 26, 6853. [Google Scholar] [CrossRef]
- Jaiswal, S.; Kundu, K.; Karmakar, S.; Kundu, S. Bacterial strains from local curd, ice-cream and natural milk cultures as po-tential probiotic candidate: Isolation, characterization and in vitro analysis. Int. J. Probiotics Prebiotics 2009, 4, 187–194. [Google Scholar]
- Oliveira, F.D.A.; Andrade, L.N.; De Sousa, B.V.; de Sousa, D. Anti-Ulcer Activity of Essential Oil Constituents. Molecules 2014, 19, 5717–5747. [Google Scholar] [CrossRef] [Green Version]
- Alomair, M.K.; Alabduladheem, L.S.; Almajed, M.A.; Alobaid, A.A.; Alkhalifah, E.A.R.; Younis, N.S.; Mohamed, M.E. Achillea millefolium Essential Oil Mitigates Peptic Ulcer in Rats through Nrf2/HO-1 Pathway. Molecules 2022, 27, 7908. [Google Scholar] [CrossRef]
- Pramanik, K.C.; Biswas, R.; Bandyopadhyay, D.; Mishra, M.; Ghosh, C.; Chatterjee, T.K. Evaluation of anti-ulcer properties of the leaf extract of Juniperus communis L. in animals. J. Nat. Remedies 2007, 7, 207–213. [Google Scholar]
- Raina, R.; Verma, P.K.; Peshin, R.; Kour, H. Potential of Juniperus communis L as a nutraceutical in human and veterinary medicine. Heliyon 2019, 5, e02376. [Google Scholar] [CrossRef] [Green Version]
- Chama, Z.; Titsaoui, D.; Benabbou, A.; Hakem, R.; Djellouli, B. Effect of Thymus vulgaris oil on the growth of Helicobacter pylori. South Asian J. Exp. Biol. 2020, 10, 374–382. [Google Scholar] [CrossRef]
- Guesmi, F.; Ali, M.B.; Barkaoui, T.; Tahri, W.; Mejri, M.; Ben-Attia, M.; Bellamine, H.; Landoulsi, A. Effects of Thymus hirtus sp. algeriensis Boiss. Et Reut. (Lamiaceae) essential oil on healing gastric ulcers according to sex. Lipids Health Dis. 2014, 13, 138. Available online: http://www.lipidworld.com/content/13/1/138 (accessed on 3 January 2023). [CrossRef] [Green Version]
- Güvenir, M.; Hanoglu, A.; Hanoglu, D.; Suer, K.; Baser, H.C.; Yavuz, D.O.; Sanlıdag, T. Antimicrobial Activity of the Essential oil of Thymus capitatus against Helicobacter pylori. Acta Pol. Pharm. Drug Res. 2020, 77, 155–160. [Google Scholar] [CrossRef]
- Moraes, T.M.; Kushima, H.; Moleiro, F.C.; Santos, R.C.; Rocha, L.R.M.; Marques, M.O.; Vilegas, W.; Hiruma-Lima, C.A. Effects of limonene and essential oil from Citrus aurantium on gastric mucosa: Role of prostaglandins and gastric mucus secretion. Chem. Interact. 2009, 180, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Memariani, Z.; Sharifzadeh, M.; Bozorgi, M.; Hajimahmoodi, M.; Farzaei, M.H.; Gholami, M.; Siavoshi, F.; Saniee, P. Protective effect of essential oil of Pistacia atlantica Desf. on peptic ulcer: Role of α-pinene. J. Tradit. Chin. Med. 2017, 37, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Polo, C.M.; Moraes, T.M.; Pellizzon, C.H.; Marques, M.O.; Rocha, L.R.M.; Hiruma-Lima, C.A. Gastric Ulcers in Middle-Aged Rats: The Healing Effect of Essential Oil from Citrus aurantium L. (Rutaceae). Evid. Based Complement. Altern. Med. 2012, 2012, 509451. [Google Scholar] [CrossRef] [Green Version]
- Bonamin, F.; Moraes, T.M.; dos Santos, R.C.; Kushima, H.; de Faria, F.; Silva, M.A.; Junior, I.V.; Nogueira, L.; Bauab, T.M.; Souza Brito, A.R.; et al. The effect of a minor constituent of essential oil from Citrus aurantium: The role of β-myrcene in preventing peptic ulcer disease. Chem. Biol. Interact. 2014, 212, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ben Mansour, R.; Beji, R.S.; Wasli, H.; Zekri, S.; Ksouri, R.; Megdiche-Ksouri, W.; Cardoso, S.M. Gastroprotective Effect of Microencapsulated Myrtus communis Essential Oil against Ethanol/HCl-Induced Acute Gastric Lesions. Molecules 2022, 27, 1566. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani, A.; Esmaeilizadeh, M. Pharmacological properties of Salvia officinalis and its components. J. Tradit. Complement. Med. 2017, 7, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Fiorentin, T.R.; Bianchi De Mello, M.; Aquino, A.M.K.; Rigo, B.A.; Loss, C.G.; Schwanz, M.; Hofmann Junior, A.E.; Dias Macedo, S.M. Antiulcerogenic potential of Salvia officinalis L. extract in rats. J. Appl. Pharm. Sci. 2013, 3, 32–35. [Google Scholar] [CrossRef] [Green Version]
- Atea, D.I.; Hassan, B.F. Effect of Salvia officinalis and Thyme vulgaris oil on hematological parmeters, of induced gastric ulcer in mature female rats. Basrah J. Vet. Res. 2020, 19, 109–120. [Google Scholar] [CrossRef]
- Salehi, B.; Selamoglu, Z.; Sevindik, M.; Fahmy, N.M.; Al-Sayed, E.; El-Shazly, M.; Csupor-Löffler, B.; Csupor, D.; Yazdi, S.E.; Sharifi-Rad, J.; et al. Achillea spp.: A comprehensive review on its ethnobotany, phytochemistry, phytopharmacology and industrial applications. Cell. Moecularl Biol. 2020, 66, 78–103. [Google Scholar] [CrossRef]
- Mohamed, M.E.; Elsayed, S.A.; Madkor, H.R.; Eldien, H.M.S.; Mohafez, O.M. Yarrow oil ameliorates ulcerative colitis in mice model via regulating the NF-κB and PPAR-γ pathways. Intest. Res. 2021, 19, 194–205. [Google Scholar] [CrossRef]
- Tadić, V.; Arsić, I.; Zvezdanović, J.; Zugić, A.; Cvetković, D.; Pavkov, S. The estimation of the traditionally used yarrow (Achillea millefolium L. Asteraceae) oil extracts with anti-inflamatory potential in topical application. J. Ethnopharmacol. 2017, 199, 138–148. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A.; Tripathi, P.; Pandey, R.; Srivatava, R.; Goswami, S. Alternative therapies useful in the management of diabetes: A systematic review. J. Pharm. Bioallied Sci. 2011, 3, 504–512. [Google Scholar] [CrossRef]
- Heghes, S.C.; Filip, L.; Vostinaru, O.; Mogosan, C.; Miere, D.; Iuga, C.A.; Moldovan, M. Essential Oil-Bearing Plants From Balkan Peninsula: Promising Sources for New Drug Candidates for the Prevention and Treatment of Diabetes Mellitus and Dyslipidemia. Front. Pharmacol. 2020, 11, 989. [Google Scholar] [CrossRef]
- Bower, A.; Marquez, S.; De Mejia, E.G. The Health Benefits of Selected Culinary Herbs and Spices Found in the Traditional Mediterranean Diet. Crit. Rev. Food Sci. Nutr. 2016, 56, 2728–2746. [Google Scholar] [CrossRef]
- Rauf, A.; Akram, M.; Anwar, H.; Daniyal, M.; Munir, N.; Bawazeer, S.; Bawazeer, S.; Rebezov, M.; Bouyahya, A.; Shariati, M.A.; et al. Therapeutic potential of herbal medicine for the management of hyperlipidemia: Latest updates. Environ. Sci. Pollut. Res. 2022, 29, 40281–40301. [Google Scholar] [CrossRef]
- De Blasio, A.; D’Anneo, A.; Lauricella, M.; Emanuele, S.; Giuliano, M.; Pratelli, G.; Calvaruso, G.; Carlisi, D. The Beneficial Effects of Essential Oils in Anti-Obesity Treatment. Int. J. Mol. Sci. 2021, 22, 11832. [Google Scholar] [CrossRef]
- Tan, X.; Chua, K.; Ram, M.R.; Kuppusamy, U. Monoterpenes: Novel insights into their biological effects and roles on glucose uptake and lipid metabolism in 3T3-L1 adipocytes. Food Chem. 2016, 196, 242–250. [Google Scholar] [CrossRef]
- Ibrahim, F.A.; Usman, L.A.; Akolade, J.O.; Idowu, O.A.; Abdulazeez, A.T.; Amuzat, A.O. Antidiabetic Potentials of Citrus aurantifolia Leaf Essential Oil. Drug Res. 2019, 69, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Selmi, S.; Rtibi, K.; Grami, D.; Sebai, H.; Marzouki, L. Rosemary (Rosmarinus officinalis) essential oil components exhibit anti-hyperglycemic, anti-hyperlipidemic and antioxidant effects in experimental diabetes. Pathophysiology 2017, 24, 297–303. [Google Scholar] [CrossRef]
- Giampieri, F.; Cianciosi, D.; Forbes-Hernández, T.Y. Myrtle (Myrtus communis L.) berries, seeds, leaves, and essential oils: New undiscovered sources of natural compounds with promising health benefits. Food Front. 2020, 1, 276–295. [Google Scholar] [CrossRef]
- Behradmanesh, S. Effect of Salvia officinalis on diabetic patients. J. Ren. Inj. Prev. 2013, 2, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Jafari, S.; Sattari, R.; Ghavamzadeh, S. Evaluation the effect of 50 and 100 mg doses of Cuminum cyminum essential oil on glycemic indices, insulin resistance and serum inflammatory factors on patients with diabetes type II: A double-blind randomized placebo-controlled clinical trial. J. Tradit. Complement. Med. 2017, 7, 332–338. [Google Scholar] [CrossRef]
- Jafari, T.; Mahmoodnia, L.; Tahmasebi, P.; Memarzadeh, M.R.; Sedehi, M.; Beigi, M.; Fallah, A.A. Effect of cumin (Cuminum cyminum) essential oil supplementation on metabolic profile and serum leptin in pre-diabetic subjects: A randomized double-blind placebo-controlled clinical trial. J. Funct. Foods 2018, 47, 416–422. [Google Scholar] [CrossRef]
- Keihan, S.G.; Gharib, M.H.; Momeni, A.; Hemati, Z.; Sedighin, R. A Comparison Between the Effect of Cuminum cyminum and Vitamin E on the Level of Leptin, Paraoxonase 1, HbA1c and Oxidized LDL in Diabetic Patients. Int. J. Mol. Cell Med. 2016, 5, 229–235. [Google Scholar] [CrossRef]
- Bamosa, A.O.; Kaatabi, H.; Lebdaa, F.M.; Al Elq, A.-M.; Al-Sultanb, A. Effect of Nigella sativa seeds on the glycemic control of patients with type 2 diabetes mellitus. Indian J. Physiol. Pharmacol. 2010, 54, 344–354. [Google Scholar]
- Kaatabi, H.; Bamosa, A.O.; Badar, A.; Al-Elq, A.; Abou-Hozaifa, B.; Lebda, F.; Al-Khadra, A.; Al-Almaie, S. Nigella sativa Improves Glycemic Control and Ameliorates Oxidative Stress in Patients with Type 2 Diabetes Mellitus: Placebo Controlled Participant Blinded Clinical Trial. PLoS ONE 2015, 10, e0113486. [Google Scholar] [CrossRef]
- Hosseini, M.S.; Mirkarimi, S.A.; Amini, M.; Mohtashami, R.; Kianbakht, S.; Fallah Huseini, H. Effects of Nigella sativa L. Seed Oil in Type II Diabetic Patients: A Randomized, Double-Blind, Placebo-Controlled Clinical. J. Med. Plants 2013, 12, 93–99. [Google Scholar]
- Rahmani, A.; Niknafs, B.; Naseri, M.; Nouri, M.; Tarighat-Esfanjani, A. Effect of Nigella Sativa Oil on Oxidative Stress, Inflammatory, and Glycemic Control Indices in Diabetic Hemodialysis Patients: A Randomized Double-Blind, Controlled Trial. Evid. Based Complement. Altern. Med. 2022, 2022, 2753294. [Google Scholar] [CrossRef]
- Hadi, A.; Mohammadi, H.; Hadi, Z.; Roshanravan, N.; Kafeshani, M. Cumin (Cuminum cyminum L.) is a safe approach for management of lipid parameters: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2018, 32, 2146–2154. [Google Scholar] [CrossRef]
- Mohtashami, A.; Mahaki, B.; Azadbakht, L.; Entezari, M.H. Effects of Bread with Nigella Sativa on Lipid Profiles, Apolipoproteins and Inflammatory Factor in Metabolic Syndrome Patients. Clin. Nutr. Res. 2016, 5, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Razmpoosh, E.; Safi, S.; Nadjarzadeh, A.; Fallahzadeh, H.; Abdollahi, N.; Mazaheri, M.; Nazari, M.; Salehi-Abargouei, A. The effect of Nigella sativa supplementation on cardiovascular risk factors in obese and overweight women: A crossover, double-blind, placebo-controlled randomized clinical trial. Eur. J. Nutr. 2021, 60, 1863–1874. [Google Scholar] [CrossRef]
- Namazi, N.; Larijani, B.; Ayati, M.H.; Abdollahi, M. The effects of Nigella sativa L. on obesity: A systematic review and meta-analysis. J. Ethnopharmacol. 2018, 219, 173–181. [Google Scholar] [CrossRef]
- Majd, F.S.; Talebi, S.S.; Abadi, A.N.A.; Poorolajal, J.; Dastan, D. Efficacy of a standardized herbal product from Pistacia atlantica subsp. Kurdica in type 2 diabetic patients with hyperlipidemia: A triple-blind randomized clinical trial. Complement. Ther. Clin. Pract. 2022, 48, 101613. [Google Scholar] [CrossRef]
- Asadi, A.; Shidfar, F.; Safari, M.; Malek, M.; Hosseini, A.F.; Rezazadeh, S.; Rajab, A.; Shidfar, S.; Hosseini, S. Safety and efficacy of Melissa officinalis (lemon balm) on ApoA-I, Apo B, lipid ratio and ICAM-1 in type 2 diabetes patients: A randomized, double-blinded clinical trial. Complement. Ther. Med. 2018, 40, 83–88. [Google Scholar] [CrossRef]
- Akbar, M.; Munir, A. Cholesterol Lowering Potential of Allium Sativum Essential Oil in Type 2 Diabetic Patients. Med. Forum 2020, 31, 7–11. [Google Scholar]
- D’Antuono, L.F.; Moretti, A.; Lovato, A.F.S. Seed yield, yield components, oil content and essential oil content and composition of Nigella sativa L. and Nigella damascena L. Ind. Crops Prod. 2002, 15, 59–69. [Google Scholar] [CrossRef]
- Petrisor, G.; Motelica, L.; Craciun, L.N.; Oprea, O.C.; Ficai, D.; Ficai, A. Melissa officinalis: Composition, Pharmacological Effects and Derived Release Systems—A Review. Int. J. Mol. Sci. 2022, 23, 3591. [Google Scholar] [CrossRef]
- Lai, Y.-S.; Chen, W.-C.; Ho, C.-T.; Lu, K.-H.; Lin, S.-H.; Tseng, H.-C.; Lin, S.-Y.; Sheen, L.-Y. Garlic Essential Oil Protects against Obesity-Triggered Nonalcoholic Fatty Liver Disease through Modulation of Lipid Metabolism and Oxidative Stress. J. Agric. Food Chem. 2014, 62, 5897–5906. [Google Scholar] [CrossRef]
- Valussi, M. Functional foods with digestion-enhancing properties. Int. J. Food Sci. Nutr. 2012, 63, 82–89. [Google Scholar] [CrossRef]
- Fahmy, M.A.; Diab, K.A.; Abdel-Samie, N.S.; Omara, E.A.; Hassan, Z.M. Carbon tetrachloride induced hepato/renal toxicity in experimental mice: Antioxidant potential of Egyptian Salvia officinalis L. essential oil. Environ. Sci. Pollut. Res. 2018, 25, 27858–27876. [Google Scholar] [CrossRef] [PubMed]
- Rašković, A.; Milanović, I.; Pavlović, N.; Ćebović, T.; Vukmirović, S.; Mikov, M. Antioxidant activity of rosemary (Rosmarinus officinalis L.) essential oil and its hepatoprotective potential. BMC Complement. Altern. Med. 2014, 14, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual-Mathey, L.; Briones-Concha, J.; Jiménez, M.; Beristain, C.; Pascual-Pineda, L. Elaboration of essential oil nanoemulsions of Rosemary (Rosmarinus officinalis L.) and its effect on liver injury prevention. Food Bioprod. Process. 2022, 134, 46–55. [Google Scholar] [CrossRef]
- Goyal, M.; Gupta, V.K.; Singh, N. Carum Carvi—An Updated Review. Indian J. Pharm. Biol. Res. 2018, 6, 14–24. [Google Scholar] [CrossRef]
- Saddiqi, H.A.; Iqbal, Z. Usage and Significance of Fennel (Foeniculum vulgare Mill.) Seeds in Eastern Medicine. In Nuts and Seeds in Health and Disease Prevention; Preedy, V.R., Watson, R.R., Patel, V.B., Eds.; Elsevier: London, UK, 2011; pp. 461–467. [Google Scholar] [CrossRef]
- Darwish, R.S.; Hammoda, H.M.; Ghareeb, D.A.; Abdelhamid, A.S.; El Naggar, E.M.B.; Harraz, F.M.; Shawky, E. Efficacy-directed discrimination of the essential oils of three Juniperus species based on their in-vitro antimicrobial and anti-inflammatory activities. J. Ethnopharmacol. 2020, 259, 112971. [Google Scholar] [CrossRef]
- Cavaleiro, C.; Pinto, E.; Goncalves, M.; Salgueiro, L. Antifungal activity of Juniperus essential oils against dermatophyte, Aspergillus and Candida strains. J. Appl. Microbiol. 2006, 100, 1333–1338. [Google Scholar] [CrossRef]
- Sandner, G.; Heckmann, M.; Weghuber, J. Immunomodulatory Activities of Selected Essential Oils. Biomolecules 2020, 10, 1139. [Google Scholar] [CrossRef]
- Zuo, X.; Gu, Y.; Wang, C.; Zhang, J.; Zhang, J.; Wang, G.; Wang, F. A Systematic Review of the Anti-Inflammatory and Immunomodulatory Properties of 16 Essential Oils of Herbs. Evid. Based Complement. Altern. Med. 2020, 2020, 2020–8878927. [Google Scholar] [CrossRef]
- Guimarães, A.G.; Quintans, J.S.S.; Quintans-Júnior, L.J. Monoterpenes with Analgesic Activity—A Systematic Review. Phytother. Res. 2013, 27, 1–15. [Google Scholar] [CrossRef]
- de Cássia Da Silveira e Sá, R.; Andrade, L.N.; De Sousa, D.P. Sesquiterpenes from Essential Oils and Anti-Inflammatory Activity. Nat. Prod. Commun. 2015, 10, 1767–1774. [Google Scholar] [CrossRef] [Green Version]
- Matos, M.S.; Anastácio, J.D.; Nunes dos Santos, C. Sesquiterpene Lactones: Promising Natural Compounds to Fight Inflammation. Pharmaceutics 2021, 13, 991. [Google Scholar] [CrossRef]
- Lee, M.S.; Lee, H.W.; Khalil, M.; Lim, H.S. Aromatherapy for Managing Pain in Primary Dysmenorrhea: A Systematic Review of Randomized Placebo-Controlled Trials. J. Clin. Med. 2018, 7, 434. [Google Scholar] [CrossRef] [Green Version]
- Sá, R.D.C.D.S.E.; Andrade, L.N.; Oliveira, R.D.R.B.D.; De Sousa, D.P. A Review on Anti-Inflammatory Activity of Phenylpropanoids Found in Essential Oils. Molecules 2014, 19, 1459–1480. [Google Scholar] [CrossRef] [Green Version]
- Mahboubi, M. Clary sage essential oil and its biological activities. Orient. Pharm. Exp. Med. 2020, 20, 517–528. [Google Scholar] [CrossRef]
- Jeenapongsa, R.; Yoovathaworn, K.; Sriwatanakul, K.M.; Pongprayoon, U.; Sriwatanakul, K. Anti-inflammatory activity of (E)-1-(3,4-dimethoxyphenyl) butadiene from Zingiber cassumunar Roxb. J. Ethnopharmacol. 2003, 87, 143–148. [Google Scholar] [CrossRef]
- Kani, K.M.; Mirzania, Z.; Mirhaghjoo, F.; Mousavi, R.; Akbarzadeh, S.; Jafari, M. The Effect of Aromatherapy (with Lavender) on Dysmenorrhea: A Systematic Review and Meta-Analysis. Int. J. Pediatr. 2019, 7, 9657–9666. Available online: https://ijp.mums.ac.ir/article_12729.html (accessed on 13 January 2023).
- Peterfalvi, A.; Miko, E.; Nagy, T.; Reger, B.; Simon, D.; Miseta, A.; Czéh, B.; Szereday, L. Much More Than a Pleasant Scent: A Review on Essential Oils Supporting the Immune System. Molecules 2019, 24, 4530. [Google Scholar] [CrossRef] [Green Version]
- Oriola, A.O.; Oyedeji, A.O. Essential Oils and Their Compounds as Potential Anti-Influenza Agents. Molecules 2022, 27, 7797. [Google Scholar] [CrossRef]
- Kodikara, B.K.; Undugoda, L.J.S.; Karunaratne, H.S.; Kandisa, R.V. Antibacterial and Antiviral Properties of Coriandrum Sativum and Zingiber Officinale against Human Respiratory Tract Related Bacterial and Viral Infections: A Review with a Focus on the Case of SARS-CoV. Adv. Technol. 2022, 2, 361–381. [Google Scholar] [CrossRef]
- Sardari, S.; Mobaiend, A.; Ghassemifard, L.; Kamali, K.; Khavasi, N. Therapeutic Effect of Thyme (Thymus vulgaris) Essential Oil on Patients with COVID19: A Randomized Clinical Trial. J. Adv. Med Biomed. Res. 2021, 29, 83–91. [Google Scholar] [CrossRef]
- Agatonovic-Kustrin, S.; Kustrin, E.; Morton, D.W. Essential oils and functional herbs for healthy aging. Neural Regen. Res. 2019, 14, 441–445. [Google Scholar] [CrossRef] [PubMed]
- De Simone, A.; Bartolini, M.; Baschieri, A.; Apperley, K.Y.; Chen, H.H.; Guardigni, M.; Montanari, S.; Kobrlova, T.; Soukup, O.; Valgimigli, L.; et al. Hydroxy-substituted trans-cinnamoyl derivatives as multifunctional tools in the context of Alzheimer’s disease. Eur. J. Med. Chem. 2017, 139, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Sinyor, B.; Mineo, J.; Ochner, C. Alzheimer’s Disease, Inflammation, and the Role of Antioxidants. J. Alzheimer’s Dis. Rep. 2020, 4, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Tarozzi, A.; Bartolini, M.; Piazzi, L.; Valgimigli, L.; Amorati, R.; Bolondi, C.; Djemil, A.; Mancini, F.; Andrisano, V.; Rampa, A. From the dual function lead AP2238 to AP2469, a multi-target-directed ligand for the treatment of Alzheimer’s disease. Pharmacol. Res. Perspect. 2014, 2, e00023. [Google Scholar] [CrossRef] [PubMed]
- Farag, M.A.; Ezzat, S.M.; Salama, M.M.; Tadros, M.G.; Serya, R.A. Anti-acetylcholinesterase activity of essential oils and their major constituents from four Ocimum species. Z. Für Nat. C 2016, 71, 393–402. [Google Scholar] [CrossRef]
- Aazza, S.; Lyoussi, B.; Miguel, M.G. Antioxidant and Antiacetylcholinesterase Activities of Some Commercial Essential Oils and Their Major Compounds. Molecules 2011, 16, 7672–7690. [Google Scholar] [CrossRef] [Green Version]
- Min, S.L.S.; Liew, S.Y.; Chear, N.J.Y.; Goh, B.H.; Tan, W.-N.; Khaw, K.Y. Plant Terpenoids as the Promising Source of Cholinesterase Inhibitors for Anti-AD Therapy. Biology 2022, 11, 307. [Google Scholar] [CrossRef]
- Postu, P.A.; Gorgan, D.L.; Cioanca, O.; Russ, M.; Mikkat, S.; Glocker, M.O.; Hritcu, L. Memory-Enhancing Effects of Origanum majorana Essential Oil in an Alzheimer’s Amyloid beta1-42 Rat Model: A Molecular and Behavioral Study. Antioxidants 2020, 9, 919. [Google Scholar] [CrossRef]
- Hasanein, P.; Sharifi, M.; Emamjomeh, A. Recent Studies on the Neuropharmacological Effects of Salvia officinalis L.: A Promising Candidate for Alzheimer’s Disease. Med. Chem. 2017, 7, 348–352. [Google Scholar] [CrossRef]
- Moss, L.; Rouse, M.; Wesnes, K.; Moss, M. Differential effects of the aromas of Salvia species on memory and mood. Hum. Psychopharmacol. Clin. Exp. 2010, 25, 388–396. [Google Scholar] [CrossRef]
- Akhondzadeh, S.; Noroozian, M.; Mohammadi, M.; Ohadinia, S.; Jamshidi, A.H.; Khani, M. Salvia officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: A double blind, randomized and placebo-controlled trial. J. Clin. Pharm. Ther. 2003, 28, 53–59. [Google Scholar] [CrossRef]
- Scuteri, D.; Rombolà, L.; Morrone, L.A.; Bagetta, G.; Sakurada, S.; Sakurada, T.; Tonin, P.; Corasaniti, M.T. Neuropharmacology of the Neuropsychiatric Symptoms of Dementia and Role of Pain: Essential Oil of Bergamot as a Novel Therapeutic Approach. Int. J. Mol. Sci. 2019, 20, 3327. [Google Scholar] [CrossRef] [Green Version]
- Scuteri, D.; Sandrini, G.; Tamburin, S.; Corasaniti, M.T.; Nicotera, P.; Tonin, P.; Bagetta, G. Bergamot rehabilitation against agitation in dementia (BRAINAID): Study protocol for a randomized, double-blind, placebo-controlled trial to assess the efficacy of furocoumarin-free bergamot loaded in a nanotechnology-based delivery system of the essential oil in the treatment of agitation in elderly affected by severe dementia. Phytother. Res. 2021, 35, 5333–5338. [Google Scholar] [CrossRef]
- Tildesley, N.T.J.; Kennedy, D.O.; Perry, E.K.; Ballard, C.G.; Wesnes, K.A.; Scholey, A.B. Positive modulation of mood and cognitive performance following administration of acute doses of Salvia lavandulaefolia essential oil to healthy young volunteers. Physiol. Behav. 2005, 83, 699–709. [Google Scholar] [CrossRef]
- Igarashi, M.; Ikei, H.; Song, C.; Miyazaki, Y. Effects of olfactory stimulation with rose and orange oil on prefrontal cortex activity. Complement. Ther. Med. 2014, 22, 1027–1031. [Google Scholar] [CrossRef]
- Chaves Neto, G.; Braga, J.E.F.; Alves, M.F.; de Morais Pordeus, L.C.; Dos Santos, S.G.; Scotti, M.T.; Almeida, R.N.; Diniz, M.D.F.F.M. Anxiolytic Effect of Citrus aurantium L. in Crack Users. Evid. Based Complement. Altern. Med. 2017, 2017, 7217619. [Google Scholar] [CrossRef] [Green Version]
- Moradi, K.; Ashtarian, H.; Danzima, N.Y.; Saeedi, H.; Bijan, B.; Akbari, F.; Mohammadi, M.M. Essential Oil from Citrus aurantium Alleviates Anxiety of Patients Undergoing Coronary Angiography: A Single-Blind, Randomized Controlled Trial. Chin. J. Integr. Med. 2021, 27, 177–182. [Google Scholar] [CrossRef]
- Du, B.; Schwartz-Narbonne, H.; Tandoc, M.; Heffernan, E.M.; Mack, M.L.; Siegel, J.A. The impact of emissions from an essential oil diffuser on cognitive performance. Indoor Air 2022, 32, e12919. [Google Scholar] [CrossRef]
- Liu, S.-H.; Lin, T.-H.; Chang, K.-M. The Physical Effects of Aromatherapy in Alleviating Work-Related Stress on Elementary School Teachers in Taiwan. Evid. Based Complement. Altern. Med. 2013, 2013, 853809. [Google Scholar] [CrossRef]
- Zamanifar, S.; Bagheri-Saveh, M.I.; Nezakati, A.; Mohammadi, R.; Seidi, J. The Effect of Music Therapy and Aromatherapy with Chamomile-Lavender Essential Oil on the Anxiety of Clinical Nurses: A Randomized and Double-Blind Clinical Trial. J. Med. Life 2020, 13, 87–93. [Google Scholar] [CrossRef]
- Mahmoodi-Shan, G.R.; Yadegari, M.; Kamkar, M.Z.; Vakili, M.A. Effects of inhaling jasmine essential oil on anxiety and blood cortisol levels in candidates for laparotomy: A randomized clinical trial. J. Nurs. Midwifery Sci. 2021, 8, 128. [Google Scholar] [CrossRef]
- Rafieian-Kopaei, M.; Hasanpour-Dehkordi, A.; Lorigooini, Z.; Deris, F.; Solati, K.; Mahdiyeh, F. Comparing the effect of intranasal lidocaine 4% with peppermint essential oil drop 1.5% on migraine attacks: A double-blind clinical trial. Int. J. Prev. Med. 2019, 10, 121. [Google Scholar] [CrossRef] [PubMed]
- Mahdavikian, S.; Fallahi, M.; Khatony, A. Comparing the Effect of Aromatherapy with Peppermint and Lavender Essential Oils on Fatigue of Cardiac Patients: A Randomized Controlled Trial. Evid. Based Complement. Altern. Med. 2021, 2021, 9925945. [Google Scholar] [CrossRef] [PubMed]
- Jaradat, N.A.; Al Zabadi, H.; Rahhal, B.; Hussein, A.M.A.; Mahmoud, J.S.; Mansour, B.; Khasati, A.I.; Issa, A. The effect of inhalation of Citrus sinensis flowers and Mentha spicata leave essential oils on lung function and exercise performance: A quasi-experimental uncontrolled before-and-after study. J. Int. Soc. Sport. Nutr. 2016, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veiskaramian, A.; Gholami, M.; Yarahmadi, S.; Baharvand, P.A.; Birjandi, M. Effect of aromatherapy with Melissa essential oil on stress and hemodynamic parameters in acute coronary syndrome patients: A clinical trial in the emergency department. Complement. Ther. Clin. Pract. 2021, 44, 101436. [Google Scholar] [CrossRef]
- Toda, M.; Morimoto, K. Effect of lavender aroma on salivary endocrinological stress markers. Arch. Oral Biol. 2008, 53, 964–968. [Google Scholar] [CrossRef]
- Lari, Z.N.; Hajimonfarednejad, M.; Riasatian, M.; Abolhassanzadeh, Z.; Iraji, A.; Vojoud, M.; Heydari, M.; Shams, M. Efficacy of inhaled Lavandula angustifolia Mill. Essential oil on sleep quality, quality of life and metabolic control in patients with diabetes mellitus type II and insomnia. J. Ethnopharmacol. 2020, 251, 112560. [Google Scholar] [CrossRef]
- Cerezer, M.F.; Nedel, S.S.; Christmann, M.; Nunes, L.S.; Vieira, I.S.; Badke, M.R.; Branco, J.C. Lavender essential oil for spinal pain in obese women: A clinical trial. Columna 2021, 20, 192–196. [Google Scholar] [CrossRef]
- Jafarbegloo, E.; Tehran, H.A.; Bakouei, S. The impacts of inhalation aromatherapy with lavender essential oil on students’ test anxiety: A randomized placebo-controlled clinical trial. J. Med. Plants 2020, 19, 100–108. [Google Scholar] [CrossRef]
- Cho, M.-Y.; Min, E.S.; Hur, M.-H.; Lee, M.S. Effects of Aromatherapy on the Anxiety, Vital Signs, and Sleep Quality of Percutaneous Coronary Intervention Patients in Intensive Care Units. Evid. Based Complement. Altern. Med. 2013, 2013, 381381. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Shindo, S.; Kanbayashi, T.; Takeshima, M.; Imanishi, A.; Mishima, K. Examination of the influence of cedar fragrance on cognitive function and behavioral and psychological symptoms of dementia in Alzheimer type dementia. Neuropsychopharmacol. Rep. 2020, 40, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Yao, L. Anxiolytic Effect of Essential Oils and Their Constituents: A Review. J. Agric. Food Chem. 2019, 67, 13790–13808. [Google Scholar] [CrossRef] [PubMed]
- Meamarbashi, A.; Rajabi, A. The effects of peppermint on exercise performance. J. Int. Soc. Sport. Nutr. 2013, 10, 15. [Google Scholar] [CrossRef] [Green Version]
- Bao, G.; Zhang, Y.; Yang, X. Effect of lemon peel flavonoids on anti-fatigue and anti-oxidation capacities of exhaustive exercise mice. Appl. Biol. Chem. 2020, 63, 85. [Google Scholar] [CrossRef]
- Satyal, P.; Murray, B.L.; McFeeters, R.L.; Setzer, W.N. Essential Oil Characterization of Thymus vulgaris from Various Geographical Locations. Foods 2016, 5, 70. [Google Scholar] [CrossRef]
- Gurav, T.P.; Dholakia, B.B.; Giri, A.P. A glance at the chemodiversity of Ocimum species: Trends, implications, and strategies for the quality and yield improvement of essential oil. Phytochem. Rev. 2022, 21, 879–913. [Google Scholar] [CrossRef]
- Tadrent, W.; Kabouche, A.; Touzani, R.; Kabouche, Z. Chemotypes investigation of essential oils of Chamomile herbs: A short review. J. Mater. Environ. Sci. 2016, 7, 1229–1235. [Google Scholar]
- Craft, J.D.; Satyal, P.; Setzer, W.N. The Chemotaxonomy of Common Sage (Salvia officinalis) Based on the Volatile Constituents. Medicines 2017, 4, 47. [Google Scholar] [CrossRef] [Green Version]
- Kohlert, C.; van Rensen, I.; März, R.; Schindler, G.; Graefe, E.U.; Veit, M. Bioavailability and Pharmacokinetics of Natural Volatile Terpenes in Animals and Humans. Planta Med. 2000, 66, 495–505. [Google Scholar] [CrossRef] [Green Version]
- Delshadi, R.; Bahrami, A.; Tafti, A.G.; Barba, F.J.; Williams, L.L. Micro and nano-encapsulation of vegetable and essential oils to develop functional food products with improved nutritional profiles. Trends Food Sci. Technol. 2020, 104, 72–83. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Plant | Treatment | Study model | Effects | Ref. |
|---|---|---|---|---|
| Sage (Salvia officinalis) | (150 mg × 3)/day; 3 months | T2DM patients, DB | ↓↓2hpp; (NS)FBS; (NS)HbA1c; ↓↓TC | [112] |
| Green cumin (Cuminum cyminum) | 50 mg or 100 mg/day; 2 months | T2DM patients, DB | ↓↓FBG; ↓↓HbA1c; ↓↓insulin; ↓TNF-α; ↓hsCRP; ↑↑adiponectin; ↓HOMA-IR | [113] |
| Green cumin (Cuminum cyminum) | 75 mg/day; 10 weeks | Prediabetic patients, DB | ↓↓HOMA-IR; (NS)FBS; (NS)HbA1c; ↓LDL; ↑HDL; ↓↓leptin ↓WC; ↓BMI; ↓BW | [114] |
| Green cumin (Cuminum cyminum) | 25 mg/day; 3 months | T2DM patients, DB vs. Vit. E | ↓↓FBG; ↓HbA1c; ↓oxLDL; ↓ApoA1; ↑↑paraoxonase 1; ↓↓leptin; ↓↓TG | [115] |
| Black cumin (Nigella sativa) | 2 g seed powder/day; 3 months | T2DM patients, DB | ↓2hpp; ↓↓FBG; ↓HbA1c; ↓↓HOMA2-IR; ↑↑β-cell | [116] |
| Black cumin (Nigella sativa) | 2 g deed powder/day; 1 year | T2DM patients, DB | ↓2hpp; ↓FBG; ↓HbA1c; ↓HOMA2-IR; ↑↑β-cell; ↑↑CAT; ↑SOD; ↑↑GSH; ↓↓TBARS | [117] |
| Black cumin (Nigella sativa) | 2.5 mL oil/day; 3 months | T2DM patients, DB | ↓2hpp; ↓FBG; ↓HbA1c; ↓BMI; | [118] |
| Black cumin (Nigella sativa) | 2 g oil/day; 12 weeks | T2DM dialysis patients, DB | ↓FBG; ↓HbA1c; ↑↑insulin; ↓hsCRP; ↑SOD; ↑TAC; ↓TBARS | [119] |
| Plant | Treatment | Study Model | Effects | Ref. |
|---|---|---|---|---|
| Green cumin (Cuminum cyminum) | 3 g seeds powder/day; 3 months | Overweight and obese, SB | ↓TC; ↓↓TG; ↓LDL-C; ↑HDL-C | [120] |
| Green cumin (Cuminum cyminum) | 100 mg EO/day; 2 months | T2DM patients, DB | ↓TC; ↓LDL-C; ↑HDL-C | [120] |
| Green cumin (Cuminum cyminum) | 50 mg EO/day; 2 months | T2DM patients, DB | ↓TC; ↓LDL-C | [120] |
| Black cumin (Nigella sativa) | 100 g bread with seeds/day; 2 months | Metabolic synd. patients, DB | No significant change in lipid profile | [121] |
| Black cumin (Nigella sativa) | 2 g oil/day; 2 months | Overweight and obese women, DB | ↓TC/HDL-C; ↓TG; ↓LDL-C; ↑HDL-C; ↓GOT; ↓SBP; (NS)DBP | [122] |
| Black cumin (Nigella sativa) | 100 mg extract to 3g oil/day | Meta-analysis of 11 clinical trials | ↓BMI; ↓BW; ↓WC | [123] |
| Wild pistachio (Pistacia atlantica) | 500 mg/day fruit powder; 2 months | T2DM patients, triple-blind | ↓2hpp; ↓TG; ↓TC; ↓↓LDL-C; (NS) FBG, HbA1c; (NS) TG, HDL-C, ALT, AST, Cr | [124] |
| Lemon balm (Melissa officinalis) | 1.4 g extract/day; 8 weeks | T2DM patients, DB | ↑Apo A-I; ↓TC/HDL-C; ↓LDL-C/HDL-C | [125] |
| Garlic (Allium sativum) | 13.5 mg EO/day; 3 and 6 months | T2DM patients with TC > 200 mg/dL | ↓FBG; ↓HbA1c; ↓↓TC | [126] |
| Essential Oil | Treatment | Study model | Effects | Ref. |
|---|---|---|---|---|
| Sage, 2 types (S. officinalis and S. lavandulaefolia) | 5 drops of EO in 5 mL water/inhalation | DB on 45 healthy adult volunteer per EO or placebo/135 total | ↑mood; ↑cognitive performance; ↑memory | [161] |
| Sage (S. lavandulaefolia) | 25 μL or 50 μL EO/oral administration | Placebo-controlled, DB crossover on 24 volunteer students | ↑mood ↑cognitive performance; ↓ catabolism of ACh | [165] |
| Rose (R. damascena) or orange (C. sinensis) | Exposure for 90 s to air impregnated with rose or orange | oxy-Hb using near-infrared TRS on 20 female university students | ↓ oxy-Hb in the right prefrontal cortex; ↑subjective reports of relaxed feeling | [166] |
| Bitter orange (C. aurantium) | 0.1 ml EO in 1.9 ml of distilled water by inhalation | Randomized on healthy subjects exposed to an anxiogenic task: crack users in abstinence | ↓DBP; ↓HR; ↓ autonomic excitability; acute anxiolytic effects | [167] |
| Sweet orange (C. aurantium) | Inhalation for 15–20 min 1 h before intervention | SB randomized/80 patients undergoing coronary angiography | ↓mean score of STAI; ↓SBP; ↓DBP; ↓respiratory and pulse rate | [168] |
| Lemon (Citrus limon) | Repeated inhalation: 4–6 sessions of 1 h/4 days | 59 healthy students, DB, computer-based objective cognitive tests | ↓reaction time; ↓memory sensibility; faster responses at the cost of accuracy | [169] |
| Bergamot (Citrus bergamia) | 80 mg of EO trans-epidermally/4 weeks | Randomized, DB, 134 patients aged ≥ 65 y with severe dementia | Target: ↓agitation in severely demented elderly. The trial in ongoing. | [164] |
| Bergamot (Citrus bergamia) | Inhalation of 2%EO/twice a day | Placebo, single-blind test on 29 elementary school teachers | ↓LF; ↓LF%;↓LF/HF | [170] |
| Chamomile + lavender (mixed) | Inhalation of mixed aroma diluted 5% | Randomized, DB on 120 nurses conducted between 2018 and 2019 | ↓anxiety; ↓depression; ↓stress (DASS scale) | [171] |
| Jasmine flower (Jasminum spp.) | Inhalation of EO/60 min before | Patients undergoing laparotomy; SB parallel, randomized | ↓cortisol; ↓mean score anxiety | [172] |
| Peppermint (Mentha piperita) | Nasal drop application of EO 1.5% vs. lidocaine 4% | Randomized, DB, controlled crossover on 120 patients with migraine | ↓headache frequency; ↓headache intensity; (similar to lidocaine) | [173] |
| Peppermint (Mentha piperita) | Inhalation of 3 drops of EO/7 nights | Randomized controlled on 105 cardiac patients | ↓average fatigue, (not different from lavender) | [174] |
| Lavender (L. angustifolia) | Inhalation 3 drops of EO/7 nights | Randomized controlled on 105 cardiac patients | ↓average fatigue, (not different from peppermint) | [174] |
| Spearmint (Mentha spicata) | Physical edu. students inhalation | Quasi-experimental, uncontrolled, before and after | ↑forced expiration vol.; ↑lung status; ↑spirometry; ↓running time | [175] |
| Sweet orange (Citrus sinensis) | Physical edu. students inhalation | Quasi-experimental, uncontrolled, before and after | ↑forced expiration vol.; ↑lung status; ↓running time | [175] |
| Lemon balm (M. officinalis) | Inhalation 2 drops of EO diluted in oil | DB controlled, 72 patients suffering from ACS | ↓mean score of stress; ↓HR; ↓MAP | [176] |
| Lavender (Lavandula spp.) | Exposure to airborne organic EO | 30 healthy students performing serial arithmetic task | ↓salivary CgA no significant change in level of Cortisol | [177] |
| Lavender (L. angustifolia) | Inhalation for 5 min at bedtime/8 weeks | 52 patients with T2DM and insomnia, randomized crossover | ↑sleep quality and quantity, ↑quality of life; ↑mood. No significant effect on metabolic status | [178] |
| Lavender (L. angustifolia) | EO 1 drop on the pillow, twice a week for one month | 49 obese women randomized, data collected in two moments on VAS for pain | ↓total spinal pain; ↓cervical region pain; ↓lumbar region pain | [179] |
| Lavender (Lavandula spp.) | 10 drops of EO in 1 L of water, for 15 min by humidifier | Single-blind randomized, 33 nursing students/anxiety (TAI) | No positive effects on students | [180] |
| Lavender, Roman chamomile, and neroli 6:2:0.5 ratio | Inhalation of 2 drops of EO blend, 10 times | 56 patients in ICU nonequivalent control group, quasi-experimental, before and after | ↓anxiety; ↑sleep quality; No significant difference on BP | [181] |
| Akita cedar (C. japonica) | Inhalation/8 weeks | 36 AD patients, randomized | ↑NPI score; ↑J-ZBI; (NS) ADAS-cog score | [182] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matera, R.; Lucchi, E.; Valgimigli, L. Plant Essential Oils as Healthy Functional Ingredients of Nutraceuticals and Diet Supplements: A Review. Molecules 2023, 28, 901. https://doi.org/10.3390/molecules28020901
Matera R, Lucchi E, Valgimigli L. Plant Essential Oils as Healthy Functional Ingredients of Nutraceuticals and Diet Supplements: A Review. Molecules. 2023; 28(2):901. https://doi.org/10.3390/molecules28020901
Chicago/Turabian StyleMatera, Riccardo, Elena Lucchi, and Luca Valgimigli. 2023. "Plant Essential Oils as Healthy Functional Ingredients of Nutraceuticals and Diet Supplements: A Review" Molecules 28, no. 2: 901. https://doi.org/10.3390/molecules28020901
APA StyleMatera, R., Lucchi, E., & Valgimigli, L. (2023). Plant Essential Oils as Healthy Functional Ingredients of Nutraceuticals and Diet Supplements: A Review. Molecules, 28(2), 901. https://doi.org/10.3390/molecules28020901