
Advancing Gastrointestinal Health: Curcumin’s Efficacy and Nanopreparations

Abstract
:1. Introduction
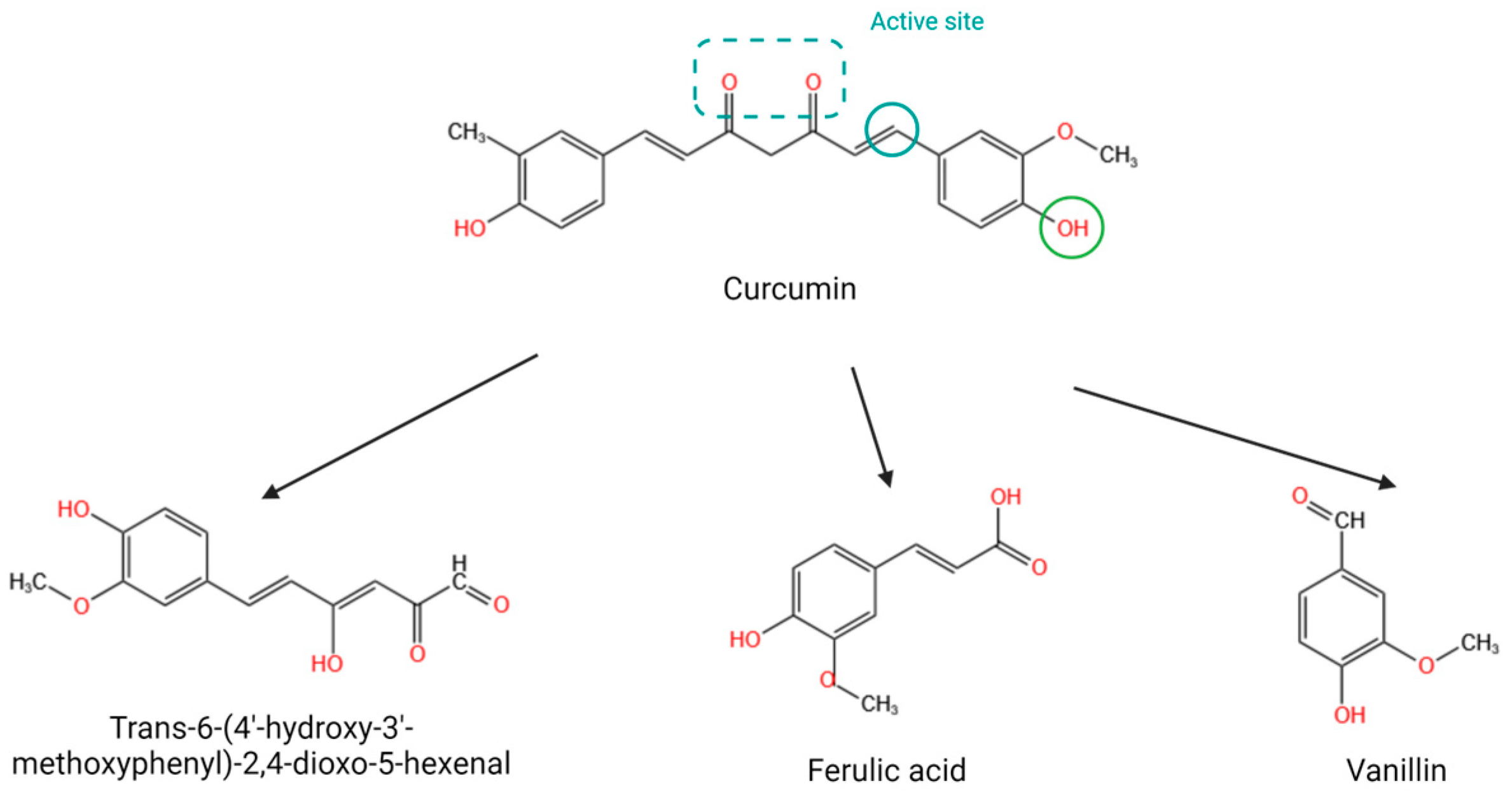
2. Structural Characteristics of Curcumin
3. Bioactivity of Curcumin
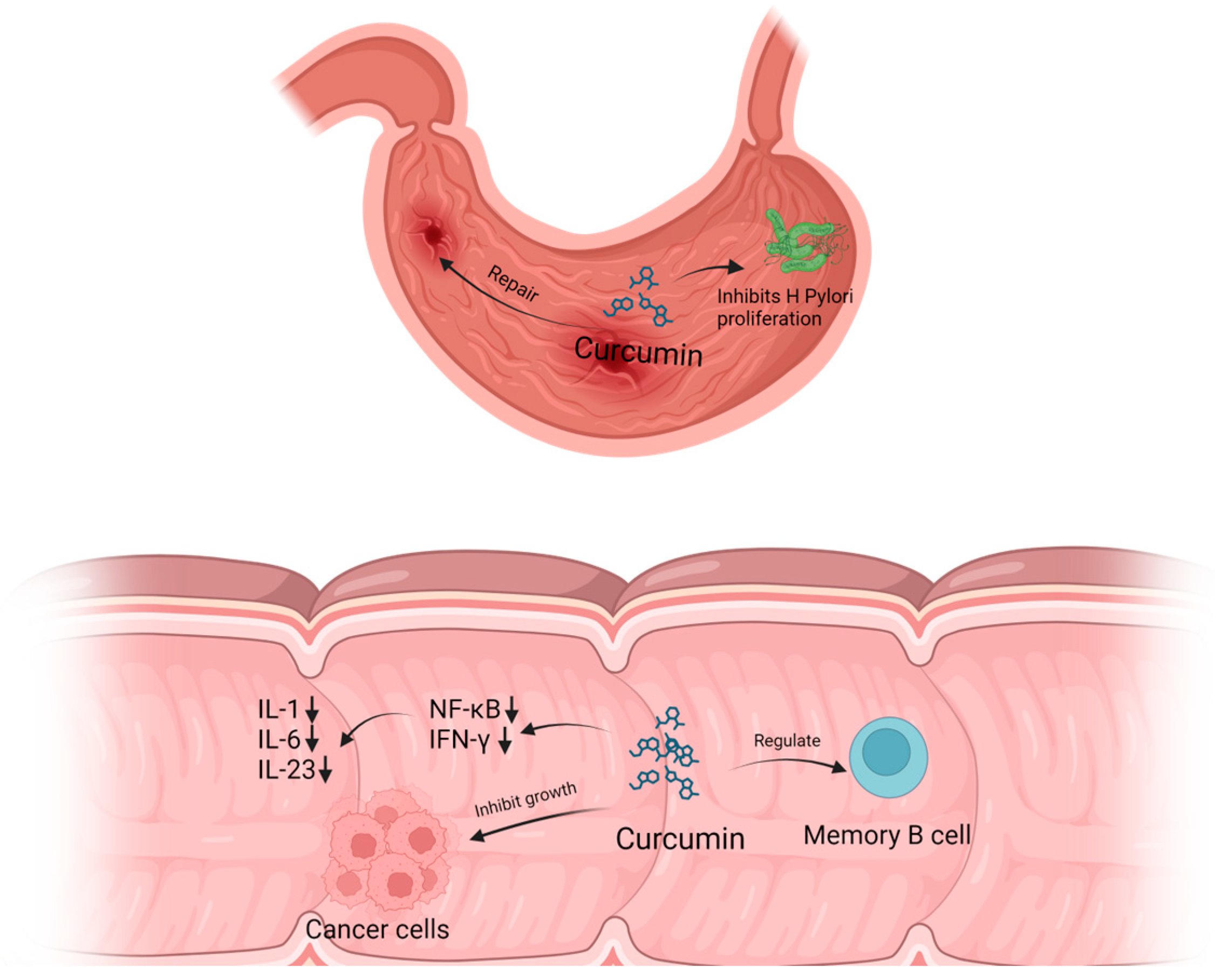
3.1. Antibacterial
3.2. Regulating Gut Microbes
3.3. Anti-Inflammation and Antitumor
3.4. Antioxidant
4. Curcumin Prevents and Treats Gastrointestinal Disease
4.1. Inflammatory Bowel Disease
4.2. Gastrointestinal Disease Caused by Helicobacter pylori
4.3. Colon Cancer
5. CCM Nanopreparation in Gastrointestinal Disease
5.1. Nanoparticle
5.2. Liposome
5.3. Noisome
5.4. Micelle
5.5. Nanoemulsion
5.6. Organic and Inorganic Hybrid Nanopreparation
6. The Properties of Nanopreparations Affect the Release of Curcumin
7. Conclusions and Prospect
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yin, Y.; Liang, H.; Wei, N.; Zheng, Z. Prevalence of chronic atrophic gastritis worldwide from 2010 to 2020: An updated systematic review and meta-analysis. Ann. Palliat. Med. 2022, 11, 3697–3703. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Jun, J.S.; Seo, J.H.; Youn, H.S.; Rhee, K.H. Changing prevalence of Helicobacter pylori infection in children and adolescents. Clin. Exp. Pediatr. 2021, 64, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.; Sousa, J.; Pais, A.; Vitorino, C. Nanomedicine: Principles, Properties, and Regulatory Issues. Front. Chem. 2018, 6, 360. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Ao, M.; Dong, B.; Jiang, Y.; Yu, L.; Chen, Z.; Hu, C.; Xu, R. Anti-Inflammatory Effects of Curcumin in the Inflammatory Diseases: Status, Limitations and Countermeasures. Drug Des. Dev. Ther. 2021, 15, 4503–4525. [Google Scholar] [CrossRef] [PubMed]
- Rinkunaite, I.; Simoliunas, E.; Alksne, M.; Dapkute, D.; Bukelskiene, V. Anti-inflammatory effect of different curcumin preparations on adjuvant-induced arthritis in rats. BMC Complement. Med. Ther. 2021, 21, 39. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Huang, C.; Huang, H.; Zhao, Y.; Khan, M.R.U.; Zhao, H.; Huang, L. Antibacterial Mechanism of Curcumin: A Review. Chem. Biodivers. 2020, 17, e2000171. [Google Scholar] [CrossRef] [PubMed]
- de Waure, C.; Bertola, C.; Baccarini, G.; Chiavarini, M.; Mancuso, C. Exploring the Contribution of Curcumin to Cancer Therapy: A Systematic Review of Randomized Controlled Trials. Pharmaceutics 2023, 15, 1275. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.P.; Sudheer, A.R. Antioxidant and anti-inflammatory properties of curcumin. Adv. Exp. Med. Biol. 2007, 595, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, A.; Young, K.N.; Moniruzzaman, M.; Beyene, A.M.; Do, K.; Kalaiselvi, S.; Min, T. Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook. Pharmaceutics 2021, 13, 484. [Google Scholar] [CrossRef]
- Talakesh, T.; Tabatabaee, N.; Atoof, F.; Aliasgharzadeh, A.; Sarvizade, M.; Farhood, B.; Najafi, M. Effect of Nano-Curcumin on Radiotherapy-Induced Skin Reaction in Breast Cancer Patients: A Randomized, Triple-Blind, Placebo-Controlled Trial. Curr. Radiopharm. 2022, 15, 332–340. [Google Scholar] [CrossRef]
- Zhang, L.; Cheng, L.; Chen, Z.; Fang, Y.; Li, C.; Chen, M.; He, P.; Wu, H.; Wu, J.; Chen, J. Chemical modification of curcumin increases its potency against hypopharyngeal carcinoma. J. Drug Target. 2023, 31, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Dhivya, R.; Ranjani, J.; Rajendhran, J.; Mayandi, J.; Annaraj, J. Enhancing the anti-gastric cancer activity of curcumin with biocompatible and pH sensitive PMMA-AA/ZnO nanoparticles. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 82, 182–189. [Google Scholar] [CrossRef]
- Hales, D.; Muntean, D.M.; Neag, M.A.; Kiss, B.; Stefan, M.G.; Tefas, L.R.; Tomuta, I.; Sesarman, A.; Ratiu, I.A.; Porfire, A. Curcumin-Loaded Microspheres Are Effective in Preventing Oxidative Stress and Intestinal Inflammatory Abnormalities in Experimental Ulcerative Colitis in Rats. Molecules 2022, 27, 5680. [Google Scholar] [CrossRef]
- Banji, D.; Banji, O.J.; Dasaroju, S.; Annamalai, A.R. Piperine and curcumin exhibit synergism in attenuating D-galactose induced senescence in rats. Eur. J. Pharmacol. 2013, 703, 91–99. [Google Scholar] [CrossRef]
- Racz, L.Z.; Racz, C.P.; Pop, L.C.; Tomoaia, G.; Mocanu, A.; Barbu, I.; Sarkozi, M.; Roman, I.; Avram, A.; Tomoaia-Cotisel, M.; et al. Strategies for Improving Bioavailability, Bioactivity, and Physical-Chemical Behavior of Curcumin. Molecules 2022, 27, 6854. [Google Scholar] [CrossRef]
- Shehata, A.A.; Yalcin, S.; Latorre, J.D.; Basiouni, S.; Attia, Y.A.; Abd El-Wahab, A.; Visscher, C.; El-Seedi, H.R.; Huber, C.; Hafez, H.M.; et al. Probiotics, Prebiotics, and Phytogenic Substances for Optimizing Gut Health in Poultry. Microorganisms 2022, 10, 395. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, A.; De, R.; Mukhopadhyay, A.K. Curcumin as a potential therapeutic candidate for Helicobacter pylori associated diseases. World J. Gastroenterol. 2016, 22, 2736–2748. [Google Scholar] [CrossRef]
- Kotha, R.R.; Luthria, D.L. Curcumin: Biological, Pharmaceutical, Nutraceutical, and Analytical Aspects. Molecules 2019, 24, 2930. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.E.; Frye, J.B.; Gorti, B.; Timmermann, B.N.; Funk, J.L. Bioactivity of turmeric-derived curcuminoids and related metabolites in breast cancer. Curr. Pharm. Des. 2013, 19, 6218–6225. [Google Scholar] [CrossRef]
- Dai, C.; Lin, J.; Li, H.; Shen, Z.; Wang, Y.; Velkov, T.; Shen, J. The Natural Product Curcumin as an Antibacterial Agent: Current Achievements and Problems. Antioxidants 2022, 11, 459. [Google Scholar] [CrossRef]
- Yasbolaghi Sharahi, J.; Aliakbar Ahovan, Z.; Taghizadeh Maleki, D.; Riahi Rad, Z.; Riahi Rad, Z.; Goudarzi, M.; Shariati, A.; Bostanghadiri, N.; Abbasi, E.; Hashemi, A. In vitro antibacterial activity of curcumin-meropenem combination against extensively drug-resistant (XDR) bacteria isolated from burn wound infections. Avicenna J. Phytomed. 2020, 10, 3–10. [Google Scholar] [PubMed]
- Darmani, H.; Smadi, E.A.M.; Bataineh, S.M.B. Blue light emitting diodes enhance the antivirulence effects of Curcumin against Helicobacter pylori. J. Med. Microbiol. 2020, 69, 617–624. [Google Scholar] [CrossRef] [PubMed]
- De, R.; Kundu, P.; Swarnakar, S.; Ramamurthy, T.; Chowdhury, A.; Nair, G.B.; Mukhopadhyay, A.K. Antimicrobial activity of curcumin against Helicobacter pylori isolates from India and during infections in mice. Antimicrob. Agents Chemother. 2009, 53, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- McFadden, R.M.; Larmonier, C.B.; Shehab, K.W.; Midura-Kiela, M.; Ramalingam, R.; Harrison, C.A.; Besselsen, D.G.; Chase, J.H.; Caporaso, J.G.; Jobin, C.; et al. The Role of Curcumin in Modulating Colonic Microbiota during Colitis and Colon Cancer Prevention. Inflamm. Bowel Dis. 2015, 21, 2483–2494. [Google Scholar] [CrossRef] [PubMed]
- Dudek-Wicher, R.K.; Junka, A.; Bartoszewicz, M. The influence of antibiotics and dietary components on gut microbiota. Prz. Gastroenterol. 2018, 13, 85–92. [Google Scholar] [CrossRef]
- Shanmugam, M.K.; Rane, G.; Kanchi, M.M.; Arfuso, F.; Chinnathambi, A.; Zayed, M.E.; Alharbi, S.A.; Tan, B.K.; Kumar, A.P.; Sethi, G. The multifaceted role of curcumin in cancer prevention and treatment. Molecules 2015, 20, 2728–2769. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Li, X.; Tu, S.; Tan, W.; Chen, L. Curcumin protect Schwann cells from inflammation response and apoptosis induced by high glucose through the NF-κB pathway. Tissue Cell 2022, 77, 101873. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, P.; Hong, H.; Wang, L.; Zhou, Y.; Lang, Y. JNK pathway mediates curcumin-induced apoptosis and autophagy in osteosarcoma MG63 cells. Exp. Ther. Med. 2017, 14, 593–599. [Google Scholar] [CrossRef]
- Kang, Z.P.; Wang, M.X.; Wu, T.T.; Liu, D.Y.; Wang, H.Y.; Long, J.; Zhao, H.M.; Zhong, Y.B. Curcumin Alleviated Dextran Sulfate Sodium-Induced Colitis by Regulating M1/M2 Macrophage Polarization and TLRs Signaling Pathway. Evid. Based Complement. Altern. Med. 2021, 2021, 3334994. [Google Scholar] [CrossRef]
- Xiao, Q.P.; Zhong, Y.B.; Kang, Z.P.; Huang, J.Q.; Fang, W.Y.; Wei, S.Y.; Long, J.; Li, S.S.; Zhao, H.M.; Liu, D.Y. Curcumin regulates the homeostasis of Th17/Treg and improves the composition of gut microbiota in type 2 diabetic mice with colitis. Phytother. Res. 2022, 36, 1708–1723. [Google Scholar] [CrossRef]
- Wei, S.Y.; Wu, T.T.; Huang, J.Q.; Kang, Z.P.; Wang, M.X.; Zhong, Y.B.; Ge, W.; Zhou, B.G.; Zhao, H.M.; Wang, H.Y.; et al. Curcumin alleviates experimental colitis via a potential mechanism involving memory B cells and Bcl-6-Syk-BLNK signaling. World J. Gastroenterol. 2022, 28, 5865–5880. [Google Scholar] [CrossRef] [PubMed]
- Lim, T.G.; Lee, S.Y.; Huang, Z.; Lim, D.Y.; Chen, H.; Jung, S.K.; Bode, A.M.; Lee, K.W.; Dong, Z. Curcumin suppresses proliferation of colon cancer cells by targeting CDK2. Cancer Prev. Res. 2014, 7, 466–474. [Google Scholar] [CrossRef]
- Lin, X.; Bai, D.; Wei, Z.; Zhang, Y.; Huang, Y.; Deng, H.; Huang, X. Curcumin attenuates oxidative stress in RAW264.7 cells by increasing the activity of antioxidant enzymes and activating the Nrf2-Keap1 pathway. PLoS ONE 2019, 14, e0216711. [Google Scholar] [CrossRef] [PubMed]
- Demir, E.A.; Tutuk, O.; Dogan-Gocmen, H.; Ozyilmaz, D.S.; Karagul, M.I.; Kara, M.; Temiz, M.; Tumer, C. CREB1 and PPAR-alpha/gamma Pathways in Hepatic Ischemia/Reperfusion: Route for Curcumin to Hepatoprotection. Iran. J. Pharm. Res. 2022, 21, e133779. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kwon, J.; Bae, E.K. A pathophysiologic approach for subacute encephalopathy with seizures in alcoholics (SESA) syndrome. J. Clin. Neurosci. 2014, 21, 1649–1652. [Google Scholar] [CrossRef]
- Van Limbergen, J.; Radford-Smith, G.; Satsangi, J. Advances in IBD genetics. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 372–385. [Google Scholar] [CrossRef]
- Midura-Kiela, M.T.; Radhakrishnan, V.M.; Larmonier, C.B.; Laubitz, D.; Ghishan, F.K.; Kiela, P.R. Curcumin inhibits interferon-gamma signaling in colonic epithelial cells. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G85–G96. [Google Scholar] [CrossRef]
- Salh, B.; Assi, K.; Templeman, V.; Parhar, K.; Owen, D.; Gomez-Munoz, A.; Jacobson, K. Curcumin attenuates DNB-induced murine colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, G235–G243. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Barquero, L.; Villegas, I.; Sanchez-Calvo, J.M.; Talero, E.; Sanchez-Fidalgo, S.; Motilva, V.; Alarcon de la Lastra, C. Curcumin, a Curcuma longa constituent, acts on MAPK p38 pathway modulating COX-2 and iNOS expression in chronic experimental colitis. Int. Immunopharmacol. 2007, 7, 333–342. [Google Scholar] [CrossRef]
- Pituch-Zdanowska, A.; Dembinski, L.; Banaszkiewicz, A. Old but Fancy: Curcumin in Ulcerative Colitis—Current Overview. Nutrients 2022, 14, 5249. [Google Scholar] [CrossRef]
- Zeng, L.; Yang, T.; Yang, K.; Yu, G.; Li, J.; Xiang, W.; Chen, H. Curcumin and Curcuma longa Extract in the Treatment of 10 Types of Autoimmune Diseases: A Systematic Review and Meta-Analysis of 31 Randomized Controlled Trials. Front. Immunol. 2022, 13, 896476. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Iida, T.; Takeuchi, K.; Watanabe, F.; Maruyama, Y.; Andoh, A.; Tsujikawa, T.; Fujiyama, Y.; Mitsuyama, K.; Sata, M.; et al. Curcumin maintenance therapy for ulcerative colitis: Randomized, multicenter, double-blind, placebo-controlled trial. Clin. Gastroenterol. Hepatol. 2006, 4, 1502–1506. [Google Scholar] [CrossRef]
- Singla, V.; Pratap Mouli, V.; Garg, S.K.; Rai, T.; Choudhury, B.N.; Verma, P.; Deb, R.; Tiwari, V.; Rohatgi, S.; Dhingra, R.; et al. Induction with NCB-02 (curcumin) enema for mild-to-moderate distal ulcerative colitis—A randomized, placebo-controlled, pilot study. J. Crohn’s Colitis 2014, 8, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.; Salomon, N.; Wu, J.C.; Kopylov, U.; Lahat, A.; Har-Noy, O.; Ching, J.Y.; Cheong, P.K.; Avidan, B.; Gamus, D.; et al. Curcumin in Combination with Mesalamine Induces Remission in Patients with Mild-to-Moderate Ulcerative Colitis in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1444–1449.e1441. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Bhatia, V.; Thareja, S.; Garg, S.; Mouli, V.P.; Bopanna, S.; Tiwari, V.; Makharia, G.; Ahuja, V. Low dose oral curcumin is not effective in induction of remission in mild to moderate ulcerative colitis: Results from a randomized double blind placebo controlled trial. World J. Gastrointest. Pharmacol. Ther. 2017, 8, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Masoodi, M.; Mahdiabadi, M.A.; Mokhtare, M.; Agah, S.; Kashani, A.H.F.; Rezadoost, A.M.; Sabzikarian, M.; Talebi, A.; Sahebkar, A. The efficacy of curcuminoids in improvement of ulcerative colitis symptoms and patients’ self-reported well-being: A randomized double-blind controlled trial. J. Cell. Biochem. 2018, 119, 9552–9559. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, N.; Mansoori, A.; Shayesteh, A.; Hashemi, S.J. The effect of curcumin supplementation on clinical outcomes and inflammatory markers in patients with ulcerative colitis. Phytother. Res. 2020, 34, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Pal, P.; Penmetsa, A.; Kathi, P.; Girish, G.; Goren, I.; Reddy, D.N. Novel Bioenhanced Curcumin with Mesalamine for Induction of Clinical and Endoscopic Remission in Mild-to-Moderate Ulcerative Colitis: A Randomized Double-Blind Placebo-controlled Pilot Study. J. Clin. Gastroenterol. 2021, 55, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Bommelaer, G.; Laharie, D.; Nancey, S.; Hebuterne, X.; Roblin, X.; Nachury, M.; Peyrin-Biroulet, L.; Fumery, M.; Richard, D.; Pereira, B.; et al. Oral Curcumin No More Effective Than Placebo in Preventing Recurrence of Crohn’s Disease after Surgery in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 1553–1560.e1551. [Google Scholar] [CrossRef]
- Sugimoto, K.; Ikeya, K.; Bamba, S.; Andoh, A.; Yamasaki, H.; Mitsuyama, K.; Nasuno, M.; Tanaka, H.; Matsuura, A.; Kato, M.; et al. Highly Bioavailable Curcumin Derivative Ameliorates Crohn’s Disease Symptoms: A Randomized, Double-Blind, Multicenter Study. J. Crohn’s Colitis 2020, 14, 1693–1701. [Google Scholar] [CrossRef]
- Khonche, A.; Biglarian, O.; Panahi, Y.; Valizadegan, G.; Soflaei, S.S.; Ghamarchehreh, M.E.; Majeed, M.; Sahebkar, A. Adjunctive Therapy with Curcumin for Peptic Ulcer: A Randomized Controlled Trial. Drug Res. 2016, 66, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Judaki, A.; Rahmani, A.; Feizi, J.; Asadollahi, K.; Hafezi Ahmadi, M.R. Curcumin in Combination with Triple Therapy Regimes Ameliorates Oxidative Stress and Histopathologic Changes in Chronic Gastritis-Associated Helicobacter pylori Infection. Arq. Gastroenterol. 2017, 54, 177–182. [Google Scholar] [CrossRef]
- Panahi, Y.; Saberi-Karimian, M.; Valizadeh, O.; Behnam, B.; Saadat, A.; Jamialahmadi, T.; Majeed, M.; Sahebkar, A. Effects of Curcuminoids on Systemic Inflammation and Quality of Life in Patients with Colorectal Cancer Undergoing Chemotherapy: A Randomized Controlled Trial. Adv. Exp. Med. Biol. 2021, 1328, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Macis, D.; Briata, I.M.; D’Ecclesiis, O.; Johansson, H.; Aristarco, V.; Buttiron Webber, T.; Oppezzi, M.; Gandini, S.; Bonanni, B.; DeCensi, A. Inflammatory and Metabolic Biomarker Assessment in a Randomized Presurgical Trial of Curcumin and Anthocyanin Supplements in Patients with Colorectal Adenomas. Nutrients 2023, 15, 3894. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Malfertheiner, P.; Yu, H.T.; Kuo, C.L.; Chang, Y.Y.; Meng, F.T.; Wu, Y.X.; Hsiao, J.L.; Chen, M.J.; Lin, K.P.; et al. Global prevalence of Helicobacter pylori infection and incidence of gastric cancer between 1980 and 2022. Gastroenterology 2024, 166, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Al Mutawa, O.A.; Izhari, M.A.; Alharbi, R.A.; Sindi, A.A.A.; Alqarni, A.M.; Alotaibi, F.E.; Gosady, A.R.A.; Dardari, D.M.M.; Almutairi, A.M.; Alshehri, M.; et al. Helicobacter pylori (H. pylori) Infection-Associated Anemia in the Asir Region, Saudi Arabia. Diagnostics 2023, 13, 2404. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e1317. [Google Scholar] [CrossRef]
- Ray, A.K.; Luis, P.B.; Mishra, S.K.; Barry, D.P.; Asim, M.; Pandey, A.; Chaturvedi, M.; Gupta, J.; Gupta, S.; Mahant, S.; et al. Curcumin Oxidation Is Required for Inhibition of Helicobacter pylori Growth, Translocation and Phosphorylation of CAG A. Front. Cell. Infect. Microbiol. 2021, 11, 765842. [Google Scholar] [CrossRef]
- Mosieniak, G.; Adamowicz, M.; Alster, O.; Jaskowiak, H.; Szczepankiewicz, A.A.; Wilczynski, G.M.; Ciechomska, I.A.; Sikora, E. Curcumin induces permanent growth arrest of human colon cancer cells: Link between senescence and autophagy. Mech. Ageing Dev. 2012, 133, 444–455. [Google Scholar] [CrossRef]
- Pricci, M.; Girardi, B.; Giorgio, F.; Losurdo, G.; Ierardi, E.; Di Leo, A. Curcumin and Colorectal Cancer: From Basic to Clinical Evidences. Int. J. Mol. Sci. 2020, 21, 2364. [Google Scholar] [CrossRef]
- Shafei, L.; Mohamed Ibrahim, M.I.; Billa, N. Is Curcumin at the Threshold of Therapeutic Effectiveness on Patients with Colon Cancer?—A Systematic Review. Front. Pharmacol. 2021, 12, 707231. [Google Scholar] [CrossRef] [PubMed]
- Kocaadam, B.; Sanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Vareed, S.K.; Kakarala, M.; Ruffin, M.T.; Crowell, J.A.; Normolle, D.P.; Djuric, Z.; Brenner, D.E. Pharmacokinetics of curcumin conjugate metabolites in healthy human subjects. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Birajdar, S.V.; Mazahir, F.; Yadav, A.K. Transferrin functionalized poloxamer-chitosan nanoparticles of metformin: Physicochemical characterization, in-vitro, and Ex-vivo studies. Drug Dev. Ind. Pharm. 2023, 49, 734–747. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Luo, R.; Qi, S.; Wang, Y.; Dai, L.; Nie, W.; Lin, M.; He, H.; Ye, N.; Fu, C.; et al. “Dual sensitive supramolecular curcumin nanoparticles” in “advanced yeast particles” mediate macrophage reprogramming, ROS scavenging and inflammation resolution for ulcerative colitis treatment. J. Nanobiotechnol. 2023, 21, 321. [Google Scholar] [CrossRef] [PubMed]
- Sesarman, A.; Tefas, L.; Sylvester, B.; Licarete, E.; Rauca, V.; Luput, L.; Patras, L.; Porav, S.; Banciu, M.; Porfire, A. Co-delivery of curcumin and doxorubicin in PEGylated liposomes favored the antineoplastic C26 murine colon carcinoma microenvironment. Drug Deliv. Transl. Res. 2019, 9, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Baiza-Duran, L.M.; Munoz-Villegas, P.; Sanchez-Rios, A.; Olvera-Montano, O. Efficacy and Safety of an Ophthalmic DMPC-Based Nanoemulsion in Patients with Dry Eye Disease: A Phase I/II Randomized Clinical Trial. J. Ophthalmol. 2023, 2023, 1431473. [Google Scholar] [CrossRef] [PubMed]
- Beloqui, A.; Coco, R.; Memvanga, P.B.; Ucakar, B.; des Rieux, A.; Preat, V. pH-sensitive nanoparticles for colonic delivery of curcumin in inflammatory bowel disease. Int. J. Pharm. 2014, 473, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Sufi, S.A.; Hoda, M.; Pajaniradje, S.; Mukherjee, V.; Coumar, S.M.; Rajagopalan, R. Enhanced drug retention, sustained release, and anti-cancer potential of curcumin and indole-curcumin analog-loaded polysorbate 80-stabilizied PLGA nanoparticles in colon cancer cell line SW480. Int. J. Pharm. 2020, 588, 119738. [Google Scholar] [CrossRef]
- Alam, J.; Dilnawaz, F.; Sahoo, S.K.; Singh, D.V.; Mukhopadhyay, A.K.; Hussain, T.; Pati, S. Curcumin Encapsulated into Biocompatible Co-Polymer PLGA Nanoparticle Enhanced Anti-Gastric Cancer and Anti-Helicobacter pylori Effect. Asian Pac. J. Cancer Prev. 2022, 23, 61–70. [Google Scholar] [CrossRef]
- Chen, J.; Xue, F.; Du, W.; Yu, H.; Yang, Z.; Du, Q.; Chen, H. An Endogenous H(2)S-Activated Nanoplatform for Triple Synergistic Therapy of Colorectal Cancer. Nano Lett. 2022, 22, 6156–6165. [Google Scholar] [CrossRef] [PubMed]
- Firouzi Amandi, A.; Jokar, E.; Eslami, M.; Dadashpour, M.; Rezaie, M.; Yazdani, Y.; Nejati, B. Enhanced anti-cancer effect of artemisinin- and curcumin-loaded niosomal nanoparticles against human colon cancer cells. Med. Oncol. 2023, 40, 170. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zheng, F.; Guo, G.; Liu, X.; Fan, R.; Qian, Z.Y.; Huang, N.; Wei, Y.Q. Improving the anti-colon cancer activity of curcumin with biodegradable nano-micelles. J. Mater. Chem. B 2013, 1, 5778–5790. [Google Scholar] [CrossRef]
- Hu, Y.; He, Y.; Ji, J.; Zheng, S.; Cheng, Y. Tumor Targeted Curcumin Delivery by Folate-Modified MPEG-PCL Self-Assembly Micelles for Colorectal Cancer Therapy. Int. J. Nanomed. 2020, 15, 1239–1252. [Google Scholar] [CrossRef] [PubMed]
- Lei, F.; Zeng, F.; Yu, X.; Deng, Y.; Zhang, Z.; Xu, M.; Ding, N.; Tian, J.; Li, C. Oral hydrogel nanoemulsion co-delivery system treats inflammatory bowel disease via anti-inflammatory and promoting intestinal mucosa repair. J. Nanobiotechnol. 2023, 21, 275. [Google Scholar] [CrossRef] [PubMed]
- Mosallam, F.M.; Bendary, M.M.; Elshimy, R.; El-Batal, A.I. Curcumin clarithromycin nano-form a promising agent to fight Helicobacter pylori infections. World J. Microbiol. Biotechnol. 2023, 39, 324. [Google Scholar] [CrossRef] [PubMed]
- Dhivya, R.; Ranjani, J.; Bowen, P.K.; Rajendhran, J.; Mayandi, J.; Annaraj, J. Biocompatible curcumin loaded PMMA-PEG/ZnO nanocomposite induce apoptosis and cytotoxicity in human gastric cancer cells. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 80, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Jiang, F.; Xing, Z.; Fan, L.; Li, Y.; Wang, S.; Ling, J.; Ouyang, X.K. Efficient Delivery of Curcumin by Alginate Oligosaccharide Coated Aminated Mesoporous Silica Nanoparticles and In Vitro Anticancer Activity against Colon Cancer Cells. Pharmaceutics 2022, 14, 1166. [Google Scholar] [CrossRef] [PubMed]
- Harish, V.; Ansari, M.M.; Tewari, D.; Gaur, M.; Yadav, A.B.; Garcia-Betancourt, M.L.; Abdel-Haleem, F.M.; Bechelany, M.; Barhoum, A. Nanoparticle and Nanostructure Synthesis and Controlled Growth Methods. Nanomaterials 2022, 12, 3226. [Google Scholar] [CrossRef]
- Rezaeian, A.; Amini, S.M.; Najafabadi, M.R.H.; Farsangi, Z.J.; Samadian, H. Plasmonic hyperthermia or radiofrequency electric field hyperthermia of cancerous cells through green-synthesized curcumin-coated gold nanoparticles. Lasers Med. Sci. 2022, 37, 1333–1341. [Google Scholar] [CrossRef]
- Yao, H.; Wang, F.; Chong, H.; Wang, J.; Bai, Y.; Du, M.; Yuan, X.; Yang, X.; Wu, M.; Li, Y.; et al. A Curcumin-Modified Coordination Polymers with ROS Scavenging and Macrophage Phenotype Regulating Properties for Efficient Ulcerative Colitis Treatment. Adv. Sci. 2023, 10, e2300601. [Google Scholar] [CrossRef]
- Hu, Y.; Song, J.; Feng, A.; Li, J.; Li, M.; Shi, Y.; Sun, W.; Li, L. Recent Advances in Nanotechnology-Based Targeted Delivery Systems of Active Constituents in Natural Medicines for Cancer Treatment. Molecules 2023, 28, 7767. [Google Scholar] [CrossRef] [PubMed]
- Sesarman, A.; Tefas, L.; Sylvester, B.; Licarete, E.; Rauca, V.; Luput, L.; Patras, L.; Banciu, M.; Porfire, A. Anti-angiogenic and anti-inflammatory effects of long-circulating liposomes co-encapsulating curcumin and doxorubicin on C26 murine colon cancer cells. Pharmacol. Rep. 2018, 70, 331–339. [Google Scholar] [CrossRef]
- Wang, X.; Fu, L.; Cheng, W.; Chen, J.; Zhang, H.; Zhu, H.; Zhang, C.; Fu, C.; Hu, Y.; Zhang, J. Oral administration of Huanglian-Houpo herbal nanoemulsion loading multiple phytochemicals for ulcerative colitis therapy in mice. Drug Deliv. 2023, 30, 2204207. [Google Scholar] [CrossRef]
- Liu, J.; Li, L.; Zhang, B.; Xu, Z.P. MnO(2)-shelled Doxorubicin/Curcumin nanoformulation for enhanced colorectal cancer chemo-immunotherapy. J. Colloid Interface Sci. 2022, 617, 315–325. [Google Scholar] [CrossRef]
- Iacob, A.T.; Lupascu, F.G.; Apotrosoaei, M.; Vasincu, I.M.; Tauser, R.G.; Lupascu, D.; Giusca, S.E.; Caruntu, I.D.; Profire, L. Recent Biomedical Approaches for Chitosan Based Materials as Drug Delivery Nanocarriers. Pharmaceutics 2021, 13, 587. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Wang, F.; Sui, Y.; She, Z.; Zhai, W.; Wang, C.; Deng, Y. Effect of particle size on solubility, dissolution rate, and oral bioavailability: Evaluation using coenzyme Q(1)(0) as naked nanocrystals. Int. J. Nanomed. 2012, 7, 5733–5744. [Google Scholar] [CrossRef]
- Lombardo, S.M.; Gunday Tureli, N.; Koch, M.; Schneider, M.; Tureli, A.E. Reliable release testing for nanoparticles with the NanoDis System, an innovative sample and separate technique. Int. J. Pharm. 2021, 609, 121215. [Google Scholar] [CrossRef]
- Johnston, S.T.; Faria, M.; Crampin, E.J. An analytical approach for quantifying the influence of nanoparticle polydispersity on cellular delivered dose. J. R. Soc. Interface 2018, 15, 20180364. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Disease | Study | Sample Size | Intervention | Age (years) | Duration | |||
|---|---|---|---|---|---|---|---|---|
| Trial Group | Control Group | Trial Group | Control Group | Trial Group | Control Group | |||
| UC | Hanai et al. [9,41,42] 2006 | 43 | 39 | CCM 2000 mg/d + sulfasalazine 1000–3000 mg/d or mesalamine 1500 mg–3000 mg/d | Placebo + sulfasalazine 1000–3000 mg/d or mesalamine 1500 mg–3000 mg/d | 45.2 ± 15.8 | 39.7 ± 14.2 | 24 weeks |
| Singla et al. [9,41,43] 2014 | 14 | 16 | CCM enema + 5-Aminosalicylic acid | Placebo enema + 5-Aminosalicylic acid | 32.7 ± 8.9 | 35.5 ± 13.8 | 8 weeks | |
| Lang et al. [9,41,44] 2015 | 25 | 22 | CCM 3000 mg/d + mesalamine | Placebo + mesalamine | 40.4 ± 12.7 | 41.4 ± 13.9 | 4 weeks | |
| Kedia et al. [41,45] 2017 | 16 | 25 | CCM 450 mg/d + mesalamine 2400 mg/d | Placebo + mesalamine 2400 mg/d | 36 ± 12 | 34 ± 7 | 8 weeks | |
| Masoodi et al. [41,46] 2018 | 28 | 28 | CCM 240 mg/d + mesalamine 3 g/d | Placebo + mesalamine 3 g/d | 38.21 ± 16.37 | 36.04 ± 11.78 | 4 weeks | |
| Sadeghi et al. [9,41,47] 2020 | 31 | 32 | CCM 1500 mg/d | Placebo | 40.1 ± 13.2 | 40.6 ± 12.4 | 8 weeks | |
| Banerjee et al. [9,41,48] 2021 | 30 | 32 | CCM 100 mg/d + mesalamine | Placebo + mesalamine | 33.56 ± 10.1 | 34.66 ± 10.27 | 12 weeks | |
| Crohn | Bommelaer et al. [9,41,49] 2020 | 31 | 31 | CCM 3000 mg/d + 2–2.5 mg/kg/d azathioprine | Placebo + 2–2.5 mg/kg/d azathioprine | 36.3 ± 8.9 | 32.9 ± 13.4 | 24 weeks |
| Sugimoto et al. [9,41,50] 2020 | 17 | 9 | CCM 360 mg/d | Placebo | 36.3 ± 8.9 | 32.9 ± 13.4 | 12 weeks | |
| H. pylori infection | Khonche et al. [51] 2016 | 30 | 30 | CCM 500 mg/d + clarithromycin 500 mg/d + amoxicillin 1000 mg/d + pantoprazole 40 mg/d | Placebo + clarithromycin 500 mg/d + amoxicillin 1000 mg/d + pantoprazole 40 mg/d | 35.03 ± 9.29 | 35.10 ± 8.96 | 4 weeks |
| Judaki et al. [52] 2017 | 50 | 50 | CCM 2100 mg/d + omeprazole 40 mg/d + amoxicillin 2000 mg/d + and metronidazole 1600 mg/d | Placebo + omeprazole 40 mg/d + amoxicillin 2000 mg/d + and metronidazole 1600 mg/d | 53.65 ± 15.65 | 54.65 ± 16.54 | 4 weeks | |
| Colon cancer | Panahi et al. [53] 2021 | 36 | 36 | CCM (500 mg) + piperine (5 mg) capsule | Placebo capsule | 58.68 ± 12.24 | 63.94 ±10.40 | 8 weeks |
| Macis et al. [54] 2023 | 15 | 14 | CCM (Meriva) 1000 mg/d + anthocyanin (Mirtoselect) 1000 mg/d | Placebo + anthocyanin (Mirtoselect) 1000 mg/d | 70.8 ± 9.8 | 67.9 ± 10.8 | 4–6 weeks | |
| Category | Study | Carriers | Size (nm) | Zeta-Potential (mV) | Polydispersity Index | Encapsulation Efficiency (%) | Drug Loading (%) (mg CCM/100 mg Polymer) | Disease Models | Drug Combination | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|
| Nanoparticle | Beloqui et al. [68] 2014 | PLGA/Eudragit S100 | 116 ± 3 | −40.4 ± 0.6 | 0.261 ± 0.03 | 67 ± 8 | 7.4 ± 0.9 | Mouse colitis | NA | Compared with CCM, nano-CCM DSS-treated mice showed a significant reduction in both MPO activity and TNF-α secretion. |
| Sufi et al. [69] 2020 | PLGA/Tween-80 | 30–250 | - | - | ~74 | 7.4 ± 0.8 | SW480 cell | NA | Drug loaded nanopreparation offers stability in different pH; Nano-CCM IC50 = 7–9 μM, CCM IC50 = 15–17 μΜ. | |
| Alam et al. [70] 2022 | PLGA | 175 ± 2.1 | −16.4 ± 0.38 | 0.1 ± 0.004 | 80 ± 2.1 | - | H. pylori | NA | CCM MIC = 16 μg·mL−1; nano-CCM MIC = 8 μg·mL−1. | |
| Chen et al. [71] 2022 | P@HMPB 1 | ~173 | ~−14.7 | - | ~58.2 | - | Mouse colorectal cancer | 5-fluorouracil | 5-Fu/Cur 2-P@HMPB group was found to have the highest tumor inhibition efficiency. | |
| Han et al. [65] 2023 | β-CD/Man/YPs | 143.44 ± 2.05 | +16.6 ± 0.21 | - | 90.24 ± 1.49 | - | Mouse colitis | NA | After the treatment with Man-CUR 2 NPs, the level of TNF-α and IL-1β is significantly lower compared to the free CCM. | |
| Liposome | Sesarman et al. [66] 2019 | PEG-LEL | 170 | −50 | <0.1 | >90 | - | Mouse colon cancer | Doxorubicin | Compared to free CCM (~190 mm3) and DOX (~190 mm3), treatment with LCL-CURC-DOX significantly reduced tumor size (~50 mm3). |
| Noisome | Firouzi et al. [72] 2023 | Span 80/Tween 80/Cholesterol | 210.10 ± 13.04 | −50.47 ± 0.47 | 0.47 ± 0.08 | 93.36 ± 0.10 | - | SW480 | Artemisinin | Compared with free CCM and Art, treatment with Cur 2-Art NioNPs significantly inhibit the growth of SW480 cells. |
| Micelle | Gao et al. [73]. 2013 | MPEG-PLA | ~30 | - | - | - | 8.0 | Mouse colon cancer | NA | The therapeutic effect of Cur 2/MPEG-PLA was much greater than that of free CCM in vitro and in mice with colon cancer. |
| Hu et al. [74] 2020 | MPEG-PCL | 30.47 ± 0.65 | −3.55 | 0.17 | 98 | - | CT26 cells; Mouse colorectal cancer | FA | FA/Nano-Cur 2 and Nano-Cur 2 induced more cell apoptosis than Free CCM at the same concentration. In vivo, tumor size grew slowly in the treatment with FA/Nano-Cur 2. | |
| Nanoemulsion | Lei et al. [75] 2023 | hydrogel/SA 3 | 130.4 ± 2.4 | −21.6 ± 1.9 | <0.3 | 88.75 ± 1.82 | 2.36 ± 0.04 | Mouse IBD | Emodin | the levels of TNF-α and IL-6 were lower in CUR 2/EMO NE group than in CCM group. |
| Mosallam et al. [76] 2023 | coconut oil/Tween 80/Propylene glycol | 61.2 ± 2.15 | +0.57 ± 4.05 | 0.245 ± 0.01 | 98 ± 2 | - | Mouse infected with H. pylori | Clarithromycin (CLR) | Cur 2-CLR-NE MIC = 6.25–12.5 μg·mL−1; Free CCM MIC = 50 μg·mL−1. | |
| Organic and inorganic hybrid nanopreparation | Dhivya et al. [77] 2017 | PMMA-PEG/ZnO | 40–90 | - | - | - | ~92 | AGS cell | NA | PMMA-PEG/ZnO nanoparticles loaded with CCM showed better anti-gastric cancer cell activity. |
| Liu et al. [78] 2022 | MSN-NH2-AOS 4 | 150.8 ± 4.6 | −32.2 ± 0.6 | 0.190 ± 0.039 | 91.24 ± 1.23 | - | HCT-116 cell | NA | The pH-sensitive AOS 4 coating made the total release rate of Cur only 28.9 ± 1.6% under neutral conditions and 67.5 ± 1% under acidic conditions. the MSN-NH2-Cur 2-AOS 4 nanoparticles were more easily absorbed by colon cancer cells than free CCM, achieving a high tumor cell targeting efficiency. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, J.; Ma, Z.; Wang, Y. Advancing Gastrointestinal Health: Curcumin’s Efficacy and Nanopreparations. Molecules 2024, 29, 1659. https://doi.org/10.3390/molecules29071659
Ji J, Ma Z, Wang Y. Advancing Gastrointestinal Health: Curcumin’s Efficacy and Nanopreparations. Molecules. 2024; 29(7):1659. https://doi.org/10.3390/molecules29071659
Chicago/Turabian StyleJi, Jialin, Zhaojie Ma, and Yingshuai Wang. 2024. "Advancing Gastrointestinal Health: Curcumin’s Efficacy and Nanopreparations" Molecules 29, no. 7: 1659. https://doi.org/10.3390/molecules29071659
APA StyleJi, J., Ma, Z., & Wang, Y. (2024). Advancing Gastrointestinal Health: Curcumin’s Efficacy and Nanopreparations. Molecules, 29(7), 1659. https://doi.org/10.3390/molecules29071659