Abstract
Background: Accruing evidence suggests that Xanthine Oxidase inhibitors (XOis) may bring direct renal benefits, besides those related to their hypo-uricemic effect. We hence aimed at performing a systematic review of randomized controlled trials (RCTs) to verify if treatment with XOis may improve renal outcomes in individuals with chronic kidney disease (CKD). Methods: Ovid-MEDLINE, PubMed and CENTRAL databases were searched for RCTs comparing any XOi to standard therapy or placebo. The primary endpoint of interest was progression to End-Stage Kidney Disease (ESKD); secondary endpoints were changes in serum creatinine, glomerular filtration rate (eGFR), proteinuria and albuminuria. Results: XOis treatment significantly reduced the risk of ESKD compared to the control (3 studies, 204 pts; RR = 0.42; 95% CI, 0.22, 0.80) and also improved eGFR in data pooled from RCTs with long follow-up times (>3 mo.) (4 studies, 357 pts; mean difference (MD) 6.82 mL/min/1.73 m2; 95% CI, 3.50, 10.15) and high methodological quality (blind design) (3 studies, 400 pts; MD 2.61 mL/min/1.73 m2; 95% CI, 0.23, 4.99). Conversely, no definite effects were apparently noticed on serum creatinine, proteinuria and albuminuria. Conclusions: XOis may represent a promising tool for retarding disease progression in CKD patients. Future trials are awaited to confirm the generalizability of these findings to the whole CKD population.
1. Introduction
The search for alternative strategies to prevent chronic kidney disease (CKD) progression is still an open challenge. In daily practice, currently recommended approaches focusing on lifestyle and dietary modifications, as well as on blood pressure and proteinuria management by renin-angiotensin-aldosterone system (RAAS) antagonists, often fail to produce stable benefits in the long term, particularly in high risk populations [1]. As a result, the rate of individuals with CKD who progress to end-stage kidney disease (ESKD) requiring chronic dialysis remains dramatically high.
A large body of mechanistic and clinical evidence nowadays point at uric acid as a potential therapeutic target for slowing down CKD progression [2]. Gouty patients and even individuals with asymptomatic hyperuricemia have a sustained risk of developing future renal damage; similarly, in patients with overt CKD, steadily elevated uric acid levels may contribute to worsening renal function [3].
In view of their good efficacy and long-term proven safety, xanthine oxidase inhibitors (XOis) currently represent the first-choice treatment of hyperuricemia associated with various diseases, including CKD [4]. In the latter, XOi administration may also ameliorate renal damage, not only by reducing circulating uric acid levels (indirect benefit), but also through various mechanisms at the kidney level (direct benefits), including the reduction of inflammation and oxidative stress and the prevention of glomerular hypertension, afferent arteriolar thickening and ischemic renal histologic changes [5,6,7,8].
Notwithstanding such strong biological premises and a wealth of positive experimental and uncontrolled clinical studies, previously published meta-analyses of randomized controlled trials (RCTs) focusing on Allopurinol showed no effects or only slight improvements in renal function in individuals with overt CKD receiving this therapy [9,10,11].
In the last few years, however, new randomized controlled trials (RCTs) came out, providing novel evidence of renal benefits of XOis. Of note, the majority of these new studies employed Febuxostat and Topiroxostat, two “second-generation” XOis that are considered to be endowed with a more powerful reno-protective potential than Allopurinol [12].
This recently accrued new body of evidence calls for the necessity of a new, comprehensive systematic review and meta-analysis in order to clarify whether XOis could indeed be useful for improving renal outcomes in the CKD population.
2. Results
2.1. Search Results
Figure 1 shows the flow diagram of the study selection process. Two thousand nine hundred and eighty potentially relevant references were initially found. Three additional citations were added by a personal search. By screening titles and abstracts, a total of 2921 citations were excluded for various reasons (search overlap, study population or intervention not pertinent, review articles or other topics). Amongst the 60 studies selected for full text examination, 42 studies were excluded because: (1) non-randomized controlled trials (n = 11); (2) review articles (n = 1); (3) dealing with the wrong population (n = 3) or intervention/comparator (n = 12); (4) not providing data on the outcomes of interest (n = 15).
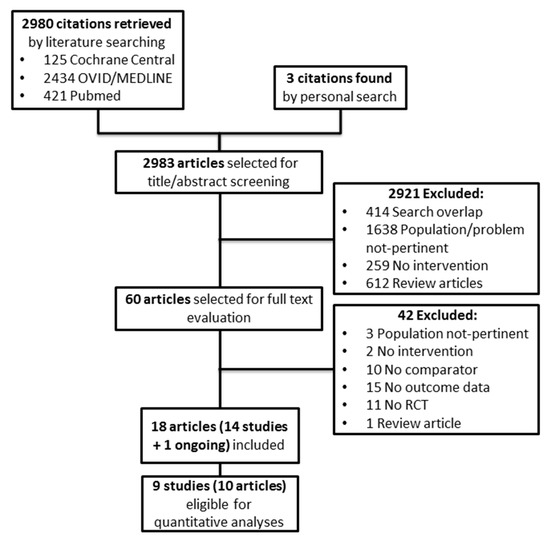
Figure 1.
Study selection flow. RCT: randomized controlled trial.
A total of 18 articles referring to 14 studies (1096 participants) and one ongoing trial were finally included in the review.
Nine randomized trials (695 participants) provided suitable numerical data on the outcomes of interest and were included in cumulative meta-analyses. The main characteristics of the studies reviewed are described in Table 1.

Table 1.
Summary of main characteristics and findings of the RCTs reviewed.
2.2. Study Characteristics
All the studies reviewed [13,14,15,16,17,18,19,20,22,23,24,25,26,27] had a parallel design. Three studies were multicenter [17,18,27]. The number of participants ranged from 40 [14,16] to 179 [18]. All trials reviewed [13,14,15,16,17,18,19,20,22,23,24,25,26,27] enrolled hyperuricemic (uric acid ≥ 6 mg/dL) CKD patients. Baseline uric acid levels ranged from ~6.2 [14] to 10.5 mg/dL [27]. Study participants had early renal failure (NKF KDOQI stage 2) in two RCTs [16,18] and mild-to-moderate (stage 3–4) CKD in nine [13,15,17,19,20,22,23,24,25]. One study [27] enrolled individuals with moderate-to-severe (stage 4–5) CKD. The prevalence of diabetes was available in eight studies [13,14,17,22,24,25,26,27], ranging from 21.5% [17] to 100% [14,26]. The mean age of patients ranged from ~40 [16] to 72.2 years [15]. Male gender ranged from 45% [14] to 100% [18]. Study follow-up varied from 4 weeks [18] to 84 months [20].
The type of XOi employed was Allopurinol in nine studies [13,14,15,16,18,19,20,22,23], Febuxostat in six [18,23,24,25,26,27] and Topiroxostat in one [17]. Drug intervention was compared to a placebo [14,15,17,18,24,26,27] or standard therapy [13,16,19,20,22,23,25]. Two RCTs [18,23] tested the effect of both Allopurinol and Febuxostat vs. the control. The daily dose of Allopurinol administered ranged from 100 [14,20] to 300 mg/day [15,16,18,22,23]. The dose of Febuxostat varied from 30 mg/twice a day [27] to 120 mg/day [18]. Saag et al. [27] tested Febuxostat at two different dose regimens (30 mg/twice a day, 40–80 mg/day). In the study conducted by Hosoya et al. [17], patients received Topiroxostat at a daily dose of 160 mg/day. End-of treatment uric acid levels ranged from 3.9 [26] to 6.6 mg/dL [20].
2.3. Risk of Bias
Risk of bias of randomized controlled trials is summarized in Table 2. Information on the random sequence generation and allocation concealment was reported in seven [13,16,20,22,24,25,26] and four studies [16,24,25,27], respectively. Seven RCTs [14,15,17,18,24,26,27] were double blind, six studies were open label [13,16,19,22,23,25] and only one [20] had a single-blind design. Only four [20,24,25,26] specifically provided information on blinding of the outcome assessors. Attrition bias was low in nine studies [13,16,17,18,20,24,25,26,27] and unclear in four [14,19,22,23]; in the RCT reported by Kao et al. [15], the overall drop-out rate was 25%. Reporting bias was low in all studies [13,14,15,16,17,18,19,20,22,23,24,25,26,27]. Risk of funding bias was potentially high in two studies [17,27] while two other studies specifically declared any sponsor involvement [24,26]. No other potential source of bias was apparently present in the remaining studies [13,14,15,16,18,19,20,22,23,25].
Table 2.
Risk of bias in randomized controlled trials.
2.4. Outcome Data
Data on the combined endpoint of progression to ESKD (serum creatinine doubling, eGFR decrease ≥50% or need for dialysis therapy) was available in only three RCTs [13,16,20]. Five studies provided data on serum creatinine change from baseline values [13,14,18,25,27]; information on change in creatinine clearance/eGFR was reported by 12 studies [15,16,17,18,19,20,22,23,24,25,26,27]. End of treatment proteinuria and albuminuria was analyzed in six [13,14,15,16,22,25] and four RCTs [17,23,25,26], respectively.
2.5. Effects of Xanthine Oxidase Inhibitors on Progression to ESKD
In a pooled meta-analysis of three RCTs (204 individuals) [13,16,20], XOis reduced the risk of the combined endpoint of progression to ESKD with respect to the control (RR = 0.42; 95% CI, 0.22, 0.80; Figure 2), with no heterogeneity in the analysis (χ2 = 1.95, p = 0.38; I2 = 0%). The quality of the body of evidence for this outcome (GRADE) was high (Table 3).
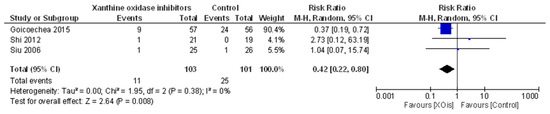
Figure 2.
Effects of XOis vs. control on progression to end-stage kidney disease (ESKD).
Table 3.
Summary of findings (GRADE).
2.6. Effects of Xanthine Oxidase Inhibitors on Secondary Outcomes
2.6.1. Serum Creatinine
Two studies [25,27] reported no concrete effects of Febuxostat on serum creatinine with respect to the control. These observations were in line with a pooled meta-analysis of three RCTs (4 intervention arms; 270 individuals) [13,14,18], showing no significant change in serum creatinine after treatment with XOis versus the control (MD −0.05 mg/dL; 95% CI, −0.12, 0.02; Figure 3). This analysis was affected by high heterogeneity (χ2 = 15.79, p = 0.001; I2 = 81%) that was significantly reduced (I2 = 58%) after excluding the only study with an open label design [13]. The quality of the body of evidence for this outcome (GRADE) was very low after being downgraded for high inconsistency and indirectness (applicability in study population/intervention/follow-up/study design) (Table 3).

Figure 3.
Effects of XOis vs. control on serum creatinine.
Visual inspection of the funnel plot and the Egger’s regression test (p = 0.13) indicate that the presence of publication bias was unlikely (Supplementary Figure S1a).
2.6.2. Renal Function
In one trial [23], eGFR significantly increased after Febuxostat administration, as compared to standard therapy. Conversely, four studies [15,17,26,27] did not report significant differences in eGFR after treatment with XOis or placebo.
This latter observation was in agreement with findings from a cumulative meta-analysis of seven RCTs (8 intervention arms; 641 individuals) [16,18,19,20,22,24,25], showing no apparent effect of XOi administration on renal function compared with the control (MD 2.33 mL/min/1.73 m2; 95% CI, −0.27, 4.92; Figure 4). Visual inspection of the funnel plot and the Egger’s regression test (p = 0.63) show absence of publication bias (Supplementary Figure S1b). The GRADE quality of this analysis was very low after downgrading for high inconsistency and indirectness (applicability in study population/intervention/follow-up/study design) (Table 3), and a mild level of heterogeneity was present (χ2 = 17.39, p = 0.02; I2 = 60%). Study stratification by CKD stage of participants, baseline and end-of-treatment uric acid levels, type of XOi administered or study design (blind vs open label) had no impact on such heterogeneity.
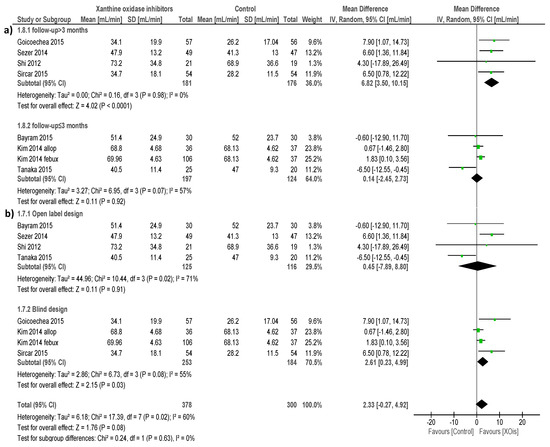
Figure 4.
Effects of XOis vs. the control on renal function.
Conversely, variable follow-up length across studies appeared to be the major determinant of heterogeneity, as this was fully nullified by sensitivity analyses including only studies with longer duration (>3 months) (χ2 = 0.16, p = 0.98; I2 = 0%). It was very interesting, that when focusing on such long-term studies, the impact of XOi treatment on eGFR also became significantly positive (4 studies, 357 individuals; MD 6.82 mL/min/1.73 m2; 95% CI, 3.50, 10.15; Figure 4a) compared with the control.
Given the absence of inconsistency and the limited indirectness, the GRADE quality of this sub analysis increased to moderate. In subgroup analyses restricted to studies with a blind design, benefits of XOis over the control with respect to renal function remained significant (3 studies, 400 individuals; MD 2.61 mL/min/1.73 m2; 95% CI, 0.23, 4.99; Figure 4b), although the quality of this analysis was downgraded to low (presence of inconsistency and indirect applicability in study intervention).
2.6.3. Proteinuria
Tanaka et al. [25] reported a significant reduction in the urinary protein/creatinine ratio in individuals on Febuxostat therapy vs. standard therapy (−0.36 ± 0.66 vs. 0.07 ± 0.38 g/g; p = 0.018).
Conversely, in another trial [15], Allopurinol had no effects over the placebo on proteinuria excretion.
This latter observation was consistent with data from a meta-analysis of four RCTs (191 individuals) [13,14,16,22], showing no significant change in proteinuria levels in the active arm compared with the control (SMD −0.06; 95% CI, −0.39, 0.26; Figure 5). This analysis had a low level of heterogeneity (χ2 = 3.92, p = 0.27; I2 = 23%). Publication bias was very unlikely according to visual inspection of the funnel plot and results from Egger’s regression test (p = 0.30) (Supplementary Figure S1c). The quality of the body of evidence for this outcome (GRADE) was high (Table 3).

Figure 5.
Effects of XOis vs. the control treatment on proteinuria.
2.6.4. Albuminuria
Three single studies [17,23,25] reported a significant reduction of urinary albumin/creatinine levels in individuals taking XOis compared to the control. In these studies, data were reported in a format that was not suitable to be pooled in a cumulative meta-analysis. On the contrary, in another trial [26], no differences were found in this parameter after Febuxostat or placebo treatment.
3. Discussion
This systematic review has been performed with the purpose of clarifying whether XOi treatment may exert benefits on renal outcomes in CKD patients, besides their acknowledged utility and efficacy in reducing circulating uric acid levels.
Indeed, a wealth of mechanistic and experimental evidence previously indicated that this drug class may be endowed with some nephroprotective effects. This ranges from the improvement of oxidative stress by reducing reactive oxygen species generation at the kidney level [28] to the amelioration of endothelial dysfunction and inflammation [29].
As intra-renal oxidative stress exacerbates smooth muscle cell proliferation of the afferent arterioles and promotes renin-angiotensin system activation, XOis would also improve kidney micro-perfusion, thereby preventing glomerular hypertension and ischemic renal histologic changes [8,30]. Such a biological background would give the rationale for explaining a series of clinical benefits, including the improvement in proteinuria, hypertension and renal function, which have been reported by various observational and interventional studies [31].
Three other meta-analyses already approached this issue in the past, providing scant or indefinite conclusions and partial disagreement among findings reported [9,10,11].
We therefore felt it necessary to perform a new, updated systematic analysis of the available evidence, also in light of a series of new RCTs that have been finalized in the last few years on the same topic. Some of these trials provided novel evidence of the benefits of XOis and tested the effects of new-generation XOis (Febuxostat, Topiroxostat) that were not considered by some previous systematic reviews because they were not yet available at that time.
From a general point of view, the findings obtained in our review seem to support the hypothesis that XOis can improve disease course in individuals with non-advanced CKD.
In particular, in a pooled analysis of three studies including 204 participants, treatment with such drugs was associated with a significant reduction (RR = 0.42; 95% CI, 0.22, 0.80) in the risk of progression to a combined ESKD endpoint (encompassing the most widely used binary criteria to define ESKD occurrence), as compared with the control. Of note, although relying on a few studies, this analysis had null heterogeneity and the corresponding body of evidence (GRADE) was of high quality, according to a validated 5-item list of methodological assessment (absence of study limitations, inconsistency of effect, imprecision, indirectness and publication bias) [32]. This latter observation may indicate that further research is unlikely to change the confidence in the estimate of effect.
Renal benefits of XOis in CKD patients were somewhat confirmed when looking at “continuous” parameters of kidney function, although under particular conditions.
In fact, an overall cumulative analysis of seven trials enrolling a total of 641 individuals did not show evidence of any significant impact of XOis, compared to the control, on estimated glomerular filtration rate (eGFR). This apparent lack of effect was in line with data from four single RCTs (not suitable to be included in the same meta-analysis) [15,17,26,27] as well as with findings published in two previous systematic reviews [9,11].
The results from this analysis, however, could be considered poorly reliable “such as they are”, given the presence of relevant heterogeneity (60%) and the very low GRADE quality of the body of evidence for high inconsistency and indirectness. When looking at potential sources of heterogeneity by exploratory subgroup analyses, we found that duration of treatment (study length) was the main factor responsible for this condition. Of note, such separate analysis also revealed the capacity of XOis to produce a clinically significant improvement in eGFR values (MD 6.82 mL/min/1.73 m2; 95% CI, 3.50, 10.15) if the observation is restricted to long-term studies only. This finding is not particularly surprising, bearing in mind that stable improvements in renal function by therapies directly targeting kidney function are usually related to hemodynamic adaptations and parenchymal/histological modifications that need more than few weeks to manifest. Accordingly, in a previous meta-analysis, similar although less remarkable benefits on eGFR (MD 3.2 mL/min/1.73 m2) were confined only to inception analyses considering trials longer than 3 months [10]. Of note, we also noticed a slightly positive effect of XOis on renal function in subgroup analyses restricted to blind trials (MD 2.61 mL/min/1.73 m2; 95% CI, 0.23, 4.99); this would support the need to minimize potential detection and performance bias of future trials by making use of a blind design in order to avoid a confounding effect on treatment efficacy.
In a pooled analysis of three studies (270 individuals), XOis had no definite effects on serum creatinine, an observation in line with findings from two other single trials [25,27] and with a previously published systematic review [11]. Although this observation might contradict the above-reported positive effects on eGFR, the true significance remains questionable given the partially unexplained heterogeneity and the very low quality of the body of evidence for high inconsistency and indirectness.
In a high quality, low-heterogeneity analysis pooling of data from four RCTs, no tangible benefits of XOis over the control were evidenced on proteinuria levels. This result confirms findings reported from previous meta-analyses [9,10,11] and from another single trial of Allopurinol [15]. Conversely, XOi treatment seemed to be effective in improving urinary albumin excretion in single data obtained from three RCTs [17,23,25]. Unfortunately, as the information from these trials was provided in a format not suitable to be pooled in cumulative analyses, the question as to whether these drugs may also improve early renal damage remains cannot be answered in a definite manner.
Our paper has a series of strengths and limitations that deserve mentioning. This review follows all current best methodological standards for systematic reviews including a pre-published protocol, a thorough literature search of multiple databases by focused, high sensitive search strategies and a systematic approach to study selection, data extraction, cumulative analyses and bias and outcome quality assessment. The key limitations of this review are represented by the few number of trials suitable to be included in cumulative analyses and the strength and quality of information available from single studies. Despite good homogeneity across studies in terms of population characteristics (e.g., CKD stage, baseline and end-of-treatment uric acid levels, co-morbidities, etc.), a substantial percentage of the included trials had a questionable (open label) design, were single-center, enrolled few participants and were of short to very-short duration. Only a few RCTs looked specifically at solid outcomes, such as the need for dialysis or kidney transplantation, while the remaining were mostly powered to catch differences in surrogate endpoints. No less important, information on the effects of XOis on early renal damage (albuminuria) was sparse or lacking.
The low number of studies finally included in the meta-analyses prevented the possibility of performing more complex investigations, such as additional subgroup or meta-regression analyses, as initially pre-planned, in order to identify all potential treatment-effect modifiers. Although we were able to explain major sources of heterogeneity for relevant outcome analyses and to identify duration of treatment and study quality as major determinants of response to treatment, the question as to whether the beneficial effects of XOis on renal function can be generalized to the whole CKD population remains to be answered.
In conclusion, there is cumulative evidence suggesting that, besides the hypo-uricemic effect, long-term treatment with Xanthine Oxidase inhibitors may bring reno-protective benefits in individuals with non-advanced chronic kidney disease. Future trials targeting solid rather than surrogate renal endpoints (e.g., ESKD) that are designed according to the highest methodological standards (double or triple-blind) are needed to support this observation further. The question as to whether administration of these agents may also positively impact early clinical damage remains to be solved by upcoming research.
4. Materials and Methods
This review follows Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [33] for reporting in systematic reviews and meta-analysis and was conducted according to a previously published protocol [34].
4.1. Data Source and Search Strategy
Ovid-MEDLINE, PubMed and CENTRAL databases were searched for articles without time or language restriction up to 28 June 2017 using focused, highly sensitive search strategies (Supplementary Table S1). References from relevant studies and reviews were screened for additional articles. The search was designed and performed by two Authors (Davide Bolignano, Anna Pisano).
4.2. Study Selection and Data Extraction
We aimed at including any RCT or quasi-RCT (trials in which allocation to treatment was made by alternation, use of alternate medical records, date of birth or other expected methods) providing evidence on potential benefits on kidney function/damage of first and second generation XOis in patients with CKD.
Studies were considered regardless of dosage or duration of administration of XOis and without follow-up duration restrictions. The type of comparator was a placebo or standard treatment.
The presence of CKD was defined according to the National Kidney Foundation-Kidney Disease Outcomes Quality Initiative (NKF KDOQI) guidelines [35] by a reduced glomerular filtration rate (GFR) <90 mL/min/1.73 m2 or by the persistence of urinary abnormalities such as albuminuria, proteinuria or hematuria in subjects with GFR ≥90 mL/min/1.73 m2.
The primary endpoint of interest was progression to End-Stage Kidney disease (ESKD) defined as one of the following events: serum creatinine doubling, eGFR decrease ≥50%, need for dialysis therapy or kidney transplantation. Secondary outcomes were changes in serum creatinine, renal function (creatinine clearance/eGFR), proteinuria and albuminuria.
Studies were excluded for the following reasons: (1) they dealt with hyperuricemic/gouty individuals without manifested CKD or on chronic renal replacement therapy (e.g., hemodialysis or peritoneal dialysis); (2) the did not provide short- or long-term data on the outcomes of interest; (3) they reported on treatment with other drugs endowed with hypouricemic effects not belonging to the XOi class (e.g., Benzbromarone, Rasburicase, Losartan); (4) they were non-randomized controlled trials.
Titles and abstracts were screened independently by two authors (Valeria Cernaro, Guido Gembillo) who discarded studies that were not pertinent to the topic. Non-randomized studies, reviews, editorials, letters and studies performed on children (age < 18) were excluded from qualitative analyses but screened for potential additional references. Two Authors (Anna Pisano, Valeria Cernaro) independently assessed the retrieved abstracts and the full text of these studies to determine eligibility according to the inclusion/exclusion criteria.
A third reviewer (DB) solved possible discrepancies on study judgments. Data extraction and analysis were performed by two reviewers (Anna Pisano, Valeria Cernaro) and independently verified by another (Guido Gembillo).
4.3. Data Analysis
Cumulative meta-analyses were performed for outcomes in which data were provided in a suitable and consistent format and by more than two studies. In order to maximize the information provided to readers, data on outcomes reported by single studies or in a descriptive way were reported narratively. The effects of treatment on continuous variables were assessed as the mean difference (MD) or standardized mean difference (SMD), as appropriate. The relative risk (RR) was calculated for dichotomous outcomes. Data were pooled using the random-effects model. To ensure robustness of the model and susceptibility to outliers, pooled data were also analyzed with the fixed-effects model. Heterogeneity was assessed by the χ-squared test on N − 1 degrees of freedom, with an alpha of 0.05 considered for statistical significance and the Cochrane-I-squared statistic [36]. I2 values of 25%, 50% and 75% were considered to correspond to low, medium and high levels of heterogeneity, respectively. Sources of heterogeneity, for identifying possible effect modifiers on the pooled analyses, were explored by sensitivity analyses according to: population characteristics (e.g., severity of CKD), duration of follow-up, study design and quality, type of intervention employed and baseline/end of treatment uric acid levels.
Given the overall paucity of studies looking at similar outcomes, we could not perform meta-regression analyses, as originally planned in the review protocol.
Publication bias was investigated by Egger’s regression test and by visual inspection of funnel plots. Statistical analyses were performed by two Authors (AP, GD) using Review Manager (RevMan; Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and Stata/IC (Version 13.1, StataCorp LP, College Station, TX, USA).
4.4. Risk of Bias (Quality) Assessment
Likelihood of bias in the single RCTs was evaluated by using the checklist developed by the Cochrane Renal Group, which considers the presence of potential selection bias (random sequence generation and allocation concealment), performance bias (blinding of investigators and participants), detection bias (blinding of outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective reporting) and possible other sources of bias (e.g., funding bias).
4.5. Summary of Findings and Quality of the Evidence
A “Summary of findings” table summarizing pooled evidence for the main outcomes was constructed according to the GRADE method [32]. The five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) were taken into account to assess the quality of a body of evidence for the main pre-specified outcomes. All decisions to downgrade or upgrade the quality of studies were justified using footnotes, and comments were made, when appropriate, to help readers’ understanding of the review.
Supplementary Materials
Supplementary materials can be found at www.mdpi.com/1422-0067/18/11/2283/s1.
Author Contributions
Research idea and study design: Davide Bolignano, Michele Buemi; Data acquisition: Anna Pisano, Valeria Cernaro, Guido Gembillo; Data analysis/interpretation: Davide Bolignano, Anna Pisano, Valeria Cernaro, Guido Gembillo; Statistical analysis: Anna Pisano, Graziella D’Arrigo; Manuscript writing: Davide Bolignano, Anna Pisano, Michele Buemi.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bolignano, D.; Pisano, A.; Coppolino, G. The Dark Side of Blocking RAS in Diabetic Patients with Incipient or Manifested Nephropathy. Exp. Clin. Endocrinol. Diabetes 2016, 124, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, T.; Ota, T.; Tamura, Y.; Chang, W.X.; Shibata, S.; Uchida, S. Time to target uric acid to retard CKD progression. Clin. Exp. Nephrol. 2017, 21, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Nakagawa, T.; Jalal, D.; Sanchez-Lozada, L.G.; Kang, D.H.; Ritz, E. Uric acid and chronic kidney disease: Which is chasing which? Nephrol. Dial. Transplant. 2013, 28, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Thurston, M.M.; Phillips, B.B.; Bourg, C.A. Safety and efficacy of allopurinol in chronic kidney disease. Ann. Pharmacother. 2013, 47, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Kabul, S.; Shepler, B. A review investigating the effect of allopurinol on the progression of kidney disease in hyperuricemic patients with chronic kidney disease. Clin. Ther. 2012, 34, 2293–2296. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Nakagawa, T.; Feng, L.; Watanabe, S.; Han, L.; Mazzali, M.; Truong, L.; Harris, R.; Johnson, R.J. A role for uric acid in the progression of renal disease. J. Am. Soc. Nephrol. 2002, 13, 2888–2897. [Google Scholar] [CrossRef] [PubMed]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001, 38, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lozada, L.G.; Tapia, E.; Soto, V.; Avila-Casado, C.; Franco, M.; Wessale, J.L.; Zhao, L.; Johnson, R.J. Effect of febuxostat on the progression of renal disease in 5/6 nephrectomy rats with and without hyperuricemia. Nephron Physiol. 2008, 108, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Bose, B.; Badve, S.V.; Hiremath, S.S.; Boudville, N.; Brown, F.G.; Cass, A.; de Zoysa, J.R.; Fassett, R.G.; Faull, R.; Harris, D.C.; et al. Effects of uric acid-lowering therapy on renal outcomes: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2014, 29, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Kanji, T.; Gandhi, M.; Clase, C.M.; Yang, R. Urate lowering therapy to improve renal outcomes in patients with chronic kidney disease: Systematic review and meta-analysis. BMC Nephrol. 2015, 16, 58. [Google Scholar] [CrossRef] [PubMed]
- Fleeman, N.; Pilkington, G.; Dundar, Y.; Dwan, K.; Boland, A.; Dickson, R.; Anijeet, H.; Kennedy, T.; Pyatt, J. Allopurinol for the treatment of chronic kidney disease: A systematic review. Health Technol. Assess. 2014, 18, 1–77. [Google Scholar] [CrossRef] [PubMed]
- Filiopoulos, V.; Hadjiyannakos, D.; Vlassopoulos, D. Febuxostat Renoprotection in CKD Patients With Asymptomatic Hyperuricemia. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2016, 67, 989–990. [Google Scholar] [CrossRef] [PubMed]
- Siu, Y.; Leung, K.; Tong, M.; Kwan, T. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level. Am. J. Kidney Dis. 2006, 47, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Momeni, A.; Shahidi, S.; Seirafian, S.; Taheri, S.; Kheiri, S. Effect of allopurinol in decreasing proteinuria in type 2 diabetic patients. Iran. J. Kidney Dis. 2010, 4, 128–132. [Google Scholar] [PubMed]
- Kao, M.; Ang, D.; Gandy, S.; Nadir, M.; Houston, J.; Lang, C.; Struthers, A. Allopurinol benefits left ventricular mass and endothelial dysfunction in chronic kidney disease. J. Am. Soc. Nephrol. 2011, 22, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Chen, W.; Jalal, D.; Li, Z.; Chen, W.; Mao, H.; Yang, Q.; Johnson, R.J.; Yu, X. Clinical outcome of hyperuricemia in IgA nephropathy: A retrospective cohort study and randomized controlled trial. Kidney Blood Press. Res. 2012, 35, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, T.; Ohno, I.; Nomura, S.; Hisatome, I.; Uchida, S.; Fujimori, S.; Yamamoto, T.; Hara, S. Effects of topiroxostat on the serum urate levels and urinary albumin excretion in hyperuricemic stage 3 chronic kidney disease patients with or without gout. Clin. Exp. Nephrol. 2014, 18, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.A.; Seo, Y.I.; Song, Y.W. Four-week effects of allopurinol and febuxostat treatments on blood pressure and serum creatinine level in gouty men. J. Korean Med. Sci. 2014, 29, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Sezer, S.; Karakan, S.; Atesagaoglu, B.; Acar, F.N. Allopurinol reduces cardiovascular risks and improves renal function in pre-dialysis chronic kidney disease patients with hyperuricemia. Saudi J. Kidney Dis. Transplant. 2014, 25, 316–320. [Google Scholar]
- Goicoechea, M.; Garcia de Vinuesa, S.; Verdalles, U.; Verde, E.; Macias, N.; Santos, A.; Perez de Jose, A.; Cedeno, S.; Linares, T.; Luno, J. Allopurinol and progression of CKD and cardiovascular events: Long-Term follow-up of a randomized clinical trial. Am. J. Kidney Dis. 2015, 65, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Goicoechea, M.; de Vinuesa, S.G.; Verdalles, U.; Ruiz-Caro, C.; Ampuero, J.; Rincon, A.; Arroyo, D.; Luno, J. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin. J. Am. Soc. Nephrol. 2010, 5, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Bayram, D.; Tuqrul, S.M.; Inal, S.; Altunta, A.; Kidir, V.; Orhan, H. The effects of allopurinol on metabolic acidosis and endothelial functions in chronic kidney disease patients. Clin. Exp. Nephrol. 2015, 19, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, D.; Ivanova, M. Febuxostat improves GFR and BP in non-diabetic adults with CKD 2–3: 4 years follow-up. Nephrol. Dial. Transplant. 2015, 30, iii486–iii487. [Google Scholar]
- Sircar, D.; Chatterjee, S.; Waikhom, R.; Golay, V.; Raychaudhury, A.; Chatterjee, S.; Pandey, R. Efficacy of Febuxostat for Slowing the GFR Decline in Patients With CKD and Asymptomatic Hyperuricemia: A 6-Month, Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Kidney Dis. 2015, 66, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Nakayama, M.; Kanno, M.; Kimura, H.; Watanabe, K.; Tani, Y.; Hayashi, Y.; Asahi, K.; Terawaki, H.; Watanabe, T. Renoprotective effects of febuxostat in hyperuricemic patients with chronic kidney disease: A parallel-group, randomized, controlled trial. Clin. Exp. Nephrol. 2015, 19, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Beddhu, S.; Filipowicz, R.; Wang, B.; Wei, G.; Chen, X.; Roy, A.C.; DuVall, S.L.; Farrukh, H.; Habib, A.N.; Bjordahl, T.; et al. A Randomized Controlled Trial of the Effects of Febuxostat Therapy on Adipokines and Markers of Kidney Fibrosis in Asymptomatic Hyperuricemic Patients With Diabetic Nephropathy. Can. J. Kidney Health Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.; Whelton, A.; Becker, M.A.; MacDonald, P.; Hunt, B.; Gunawardhana, L. Impact of Febuxostat on Renal Function in Gout Patients With Moderate-to-Severe Renal Impairment. Arthritis Rheumatol. 2016, 68, 2035–2043. [Google Scholar] [CrossRef] [PubMed]
- Jalal, D.I.; Chonchol, M.; Chen, W.; Targher, G. Uric acid as a target of therapy in CKD. Am. J. Kidney Dis. 2013, 61, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Yelken, B.; Caliskan, Y.; Gorgulu, N.; Altun, I.; Yilmaz, A.; Yazici, H.; Oflaz, H.; Yildiz, A. Reduction of uric acid levels with allopurinol treatment improves endothelial function in patients with chronic kidney disease. Clin. Nephrol. 2012, 77, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lozada, L.G.; Tapia, E.; Santamaria, J.; Avila-Casado, C.; Soto, V.; Nepomuceno, T.; Rodriguez-Iturbe, B.; Johnson, R.J.; Herrera-Acosta, J. Mild hyperuricemia induces vasoconstriction and maintains glomerular hypertension in normal and remnant kidney rats. Kidney Int. 2005, 67, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Santos, A.B.; Neogi, T. Management of Gout and Hyperuricemia in CKD. Am. J. Kidney Dis. 2017. [Google Scholar] [CrossRef] [PubMed]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Pisano, A.; D’Arrigo, G. Xanthine oxidase inhibitors for improving renal damage in CKD patients. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42017067881 (accessed on 31 May 2017).
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]





© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).