
Polymeric Gels and Their Application in the Treatment of Psoriasis Vulgaris: A Review



Abstract

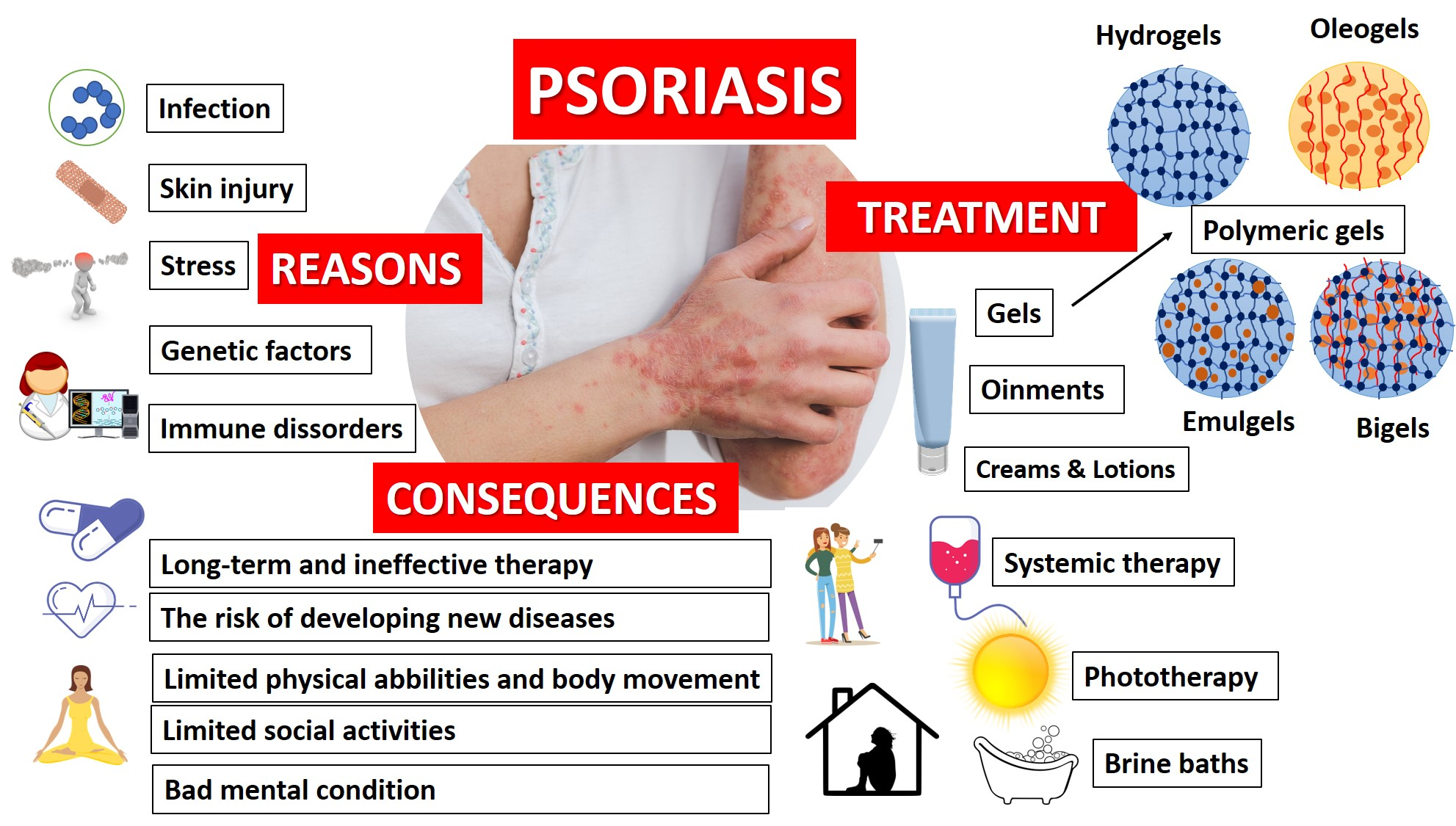
1. Introduction
1.1. Course and Symptoms of Psoriasis
1.2. Psoriasis Treatment
1.2.1. External Treatment—Topical Therapy
1.2.2. Systemic Psoriasis Treatment
1.2.3. Quality of Life of People with Psoriasis
- Belong to a group of non-Newton shear-thinning fluids; these fluids show greater viscosity when rubbed into a lesion area. Due to increased viscosity, their distribution is limited, so the formulation does not spill over the entire surface of the skin. This makes it possible to create a protective layer on the skin;
- Show thixotropy; the medicinal preparation becomes more liquid with the increased time of the applied forces, but when left undisturbed, it regains its viscosity;
- Have suitable soft consistency, skin adhesiveness, and lower firmness, good spreadability, as these properties mean easy and convenient application, in particular when taking the preparation from the packaging;
- Enhance transport of the medicinal substance deeper into the skin;
2. Polymeric Gels and Their Properties
2.1. Polymeric Gels and Their Groups
2.2. Properties of Polymeric Gels
Properties of Polymeric Gels Influencing Topical Drug Delivery
2.3. Hydrogels
2.3.1. Characteristics and Classification of Hydrogels
2.3.2. Basic Methods of Synthesis
2.3.3. Mechanism
2.3.4. Hydrogels in Psoriasis Treatment
2.4. Oleogels
2.4.1. Oil Structuring and Types of Oleogelators
2.4.2. Production Methods of Oleogels
2.4.3. Mechanism
2.4.4. Utilization of Oleogel Systems in Psoriasis Treatment
2.5. Emulgels
2.5.1. Emulgel Characteristics
2.5.2. Methods of Obtaining
2.5.3. Mechanism
2.5.4. Emulgels in Psoriasis Treatment
2.6. Bigels
2.6.1. Types of Bigels and Their Advantages over Other Polymeric Gels
2.6.2. Bigel Production Methods
2.6.3. Mechanism
2.6.4. Use of Bigels in Psoriasis Treatment
3. Conclusions and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Zagórska-Dziok, M.; Sobczak, M. Hydrogel-Based Active Substance Release Systems for Cosmetology and Dermatology Application: A Review. Pharmaceutics 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Reich, K. Łuszczyca jako układowa choroba zapalna: Implikacje dla postępowania. Dermatol. Dypl. 2012, 3, 4–15. [Google Scholar]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef]
- Reich, A.; Wójcik-Maciejewicz, A.; Slominski, A.T. Stress and the skin. G. Ital. Dermatol. Venereol. 2010, 145, 213–219. [Google Scholar]
- Szepietowski, J.; Adamski, Z.; Chodorowska, G.; Gliński, W.; Kaszuba, A.; Placek, W.; Rudnicka, L.; Reich, A. Diagnostics and treatment of psoriasis vulgaris: Guidelines of the Polish Dermatological Society. Part I: Mild psoriasis, psoriasis in children. Przegl. Dermatol. 2012, 99, 83–96. [Google Scholar]
- Partyka, A.; Czopek, A.; Stanisz-Wallis, K.; Zagórska, A. The use of biopharmaceuticals in the treatment od psoriasis. Postepy. Hig. Med. Dosw. 2018, 72, 642–658. [Google Scholar] [CrossRef]
- Krueger, J.G.; Bowock, A. Psoriasis pathophysiology: Current concepts of pathogenesis. Ann. Rheum. Dis. 2005, 64 (Suppl. 2), ii30–ii36. [Google Scholar] [CrossRef]
- O’Leary, C.J.; Creamer, D.; Higgins, E.; Weinman, J. Perceived stress, stress attributions and psychological distress in psoriasis. J. Psychosom. Res. 2004, 57, 465–471. [Google Scholar] [CrossRef]
- Hendriks, A.G.; van der Velden, H.M.; Wolberink, E.A.; Seyger, M.M.; Schalwijk, J.; Zeeuwen, P.L.; de Jond, E.M.; Pasch, M.C.; van Erp, P.E.; van de Kerkhof, P.C. The effect of adalimumab on key drivers in the pathogenesis of psoriasis. Br. J. Dermatol. 2014, 170, 571–580. [Google Scholar] [CrossRef]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 21, 263–271. [Google Scholar] [CrossRef]
- Jabłońska, S.; Chorzelski, T. Choroby Skóry, 5th ed.; Wydawnictwo Lekarskie PZWL: Warszawa, Poland, 2010. [Google Scholar]
- Lowes, M.A.; Bowock, A.M.; Krueger, J.G. Pathogenesis and therapy od psoriasis. Nature 2007, 445, 866–873. [Google Scholar] [CrossRef]
- Menter, A.; Griffiths, C.E. Current and future management of psoriasis. Lancet 2007, 21, 272–284. [Google Scholar] [CrossRef]
- Romańska-Gocka, K. Farmakoterapia łuszczycy. Farm. Pol. 2009, 65, 647–654. [Google Scholar]
- Dattola, A.; Silvestri, M.; Bennardo, L.; Del Duca, E.; Longo, C.; Bianchi, L.; Nisticò, S. Update of calcineurin inhibitors to treat inverse psoriasis: A systematic review. Dermatol. Ther. 2018, 31, e12728. [Google Scholar] [CrossRef]
- Kim, W.B.; Jerome, D.; Yeung, J. Diagnosis and management of psoriasis. Can. Fam. Phys. 2017, 63, 278–285. [Google Scholar]
- Kaszuba, A.; Uczniak, S.; Kaszuba, A. Dermatologia Geriatryczna Tom 1, 1st ed.; Wydawnictwo Czelej: Warszawa, Poland, 2016; p. 171. [Google Scholar]
- Jacobi, A.; Mayer, A.; Augustin, M. Keratolytics and Emollients and their role in the Therapy of Psoriasis: A systematic Review. Dermatol. Ther. 2015, 5, 1–18. [Google Scholar] [CrossRef]
- Bos, J.D.; Spuls, P.I. Topical treatments in psoriasis: Today and tomorrow. Clin. Dermatol. 2008, 26, 432–437. [Google Scholar] [CrossRef]
- Krzaczyński, J.; Strzałka-Mrozik, B. Farmakologiczne i niefarmakologiczne metody terapii łuszczycy ze szczególnym uwzględnieniem leków biologicznych. Farm. Pol. 2020, 76, 333–343. [Google Scholar] [CrossRef]
- Fluhr, J.; Cavallotti, C.; Berardesca, E. Emollients, moisturizers and keratolytic agents in psoriasis. Clin. Dermatol. 2008, 26, 380–386. [Google Scholar] [CrossRef]
- Dattola, A.; Silvestri, M.; Bennardo, L.; Rizzuto, F.; Dastoli, S.; Patruno, C.; Bianchi, L.; Nisticò, S. A novel vehicle for the treatment of psoriasis. Dermatol. Ther. 2020, 33, e13185. [Google Scholar] [CrossRef] [PubMed]
- Mattozzi, C.; Paolino, G.; Richetta, A.G.; Calvieri, S. Psoriasis, vitamin D and the importance of the cutaneous barrier’s integrity: An update. J. Dermatol. 2016, 43, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Visconti, B.; Paolino, G.; Carotti, S.; Pendolino, A.L.; Morini, S.; Richetta, A.G.; Calvieri, S. Immunohistochemical expression of VDR is associated with reduced integrity of tight junction complex in psoriatic skin. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2038–2042. [Google Scholar] [CrossRef]
- Loden, M. Role of Topical Emollients and Moisturizers in the Treatment of dry skin barrier disorders. Am. J. Clin. Dermatol. 2003, 4, 771–788. [Google Scholar] [CrossRef]
- Herman, A.; Herman, A.P. Topically Used Herbal Products for the Treatment of Psoriasis—Mechanism of Action, Drug Delivery, Clinical Studies. Planta Med. 2016, 82, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Jarret, A.; Spearmann, R.I.G. Psoriasis. In Histochemistry of the Skin, 1st ed.; Taverner, D., Trounce, J., Eds.; University Press: London, UK, 1964. [Google Scholar]
- Dhanabal, S.P.; Dwarampudi, L.P.; Muruganantham, N.; Vadivelan, R. Evaluation of the antipsoriatic activity of Aloe vera leaf extract using a mouse tail model of psoriasis. Phytother. Res. 2012, 26, 617–619. [Google Scholar] [CrossRef]
- Dwarampudi, L.P.; Palaniswamy, D.; Nithyanantham, M.; Raghu, P.S. Antipsoriatic activity and cytotoxicity of ethanolic extract of Nigella sativa seeds. Pharmacogn. Mag. 2012, 8, 268–272. [Google Scholar] [CrossRef]
- Lin, Z.X.; Jiao, B.W.; Che, C.T.; Zuo, Z.; Mok, C.F.; Zhao, M.; Ho, W.K.; Tse, W.P.; Lam, K.Y.; Fan, R.Q.; et al. Ethyl acetate fraction of the root of Rubia cordifolia L. inhibits keratinocyte proliferation in vitro and promotes keratinocyte differentiation in vivo: Potential application for psoriasis treatment. Phytother. Res. 2010, 24, 1056–1064. [Google Scholar] [CrossRef]
- Vijayalakshmi, A.; Ravichandiran, V.; Velraj, M.; Nirmala, S.; Jayakumari, S. Screening of flavonoid “quercetin” from the rhizome of Smilax china Linn. for anti-psoriatic activity. Asian Pac. J. Trop. Biomed. 2012, 2, 269–275. [Google Scholar] [CrossRef]
- Shrivastav, S.; Sindhu, R.; Kumar, S.; Kumar, P. Anti-psoriatic and phyto chemical evaluation of Thespesia populnea bark extracts. Int. J. Pharm. Pharm. Sci. 2009, 1, 176–185. [Google Scholar]
- Dhanabal, S.P.; Raj, B.A.; Muruganantham, N.; Praveen, T.K.; Raghu, P.S. Screening of Wrightia tinctoria leaves for anti psoriatic activity. Hygeia J. Drug Med. 2012, 4, 73–78. [Google Scholar]
- Wu, J.; Li, H.; Li, M. Effects of baicalin cream in two mouse models: 2,4-dinitrofluorobenzene-induced contact hypersensitivity and mouse tailtest for psoriasis. Int. J. Clin. Exp. Med. 2015, 8, 2128–2213. [Google Scholar] [PubMed]
- Oyedeji, F.O.; Bankole-Ojo, O.S. Quantitative evaluation of the antipsoriatic activity of sausage tree (Kigelia africana). Afr. J. Pure Appl. Chem. 2012, 6, 214–218. [Google Scholar] [CrossRef]
- Menter, A.; Korman, N.J.; Elmets, C.A.; Feldman, S.R.; Gelfand, J.M.; Gordon, K.B.; Gottlieb, A.; Koo, J.Y.; Lebwohl, M.; Lim, H.W.; et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 5. Guidelines of care for the treatment of psoriasis with phototherapy and photochemotherapy. JAAD 2010, 62, 114–135. [Google Scholar] [CrossRef]
- Friedman, S.J. Management of Psoriasis Vulgaris With a Hydrocolloid Occlusive Dressing. Arch. Dermatol. 1987, 123, 1046–1052. [Google Scholar] [CrossRef]
- Griffiths, C.E.; Tranfaglia, M.G.; Kang, S. Prolonged occlusion in the treatment of psoriasis: A clinical and immunohistologic study. J. Am. Acad. Dermatol. 1995, 32, 618–622. [Google Scholar] [CrossRef]
- Lotti, T. Occlusive treatment in psoriasis: How does it work? J. Am. Acad. Dermatol. 1996, 35, 283–284. [Google Scholar] [CrossRef]
- Hwang, S.M.; Ahn, S.K.; Menon, G.K.; Choi, E.H.; Lee, S.H. Basis of occlusive therapy in psoriasis: Correcting defects in permeability barrier and calcium gradient. Int. J. Dermatol. 2001, 40, 223–231. [Google Scholar] [CrossRef]
- Koo, B.; Hong, J.; Colaco, S. Hydrogel Patch: A New Occlusive Device for the Treatment of Psoriasis—Patient Feedback from a Bilaterally Controlled Study. Psoriasis Forum 2007, 13, 27–30. [Google Scholar] [CrossRef]
- Revicki, D.; Wililian, M.K.; Saurat, J.H.; Papp, K.A.; Ortonne, J.P.; Sexton, C.; Cameza, A. Impact of adalimumab treatment on health-related quality of life and other patient-reported outcomes: Results from 16-week randomized controlled trial in patients with moderate to severe plaque psoriasis. Br. J. Dermatol. 2008, 158, 549–557. [Google Scholar] [CrossRef]
- Lehmann, J.C.; Listopad, J.J.; Rentzsch, C.U.; Igney, F.H.; von Bonin, A.; Hennekes, H.H.; Asadullah, K.; Docke, W.D. Dimethylfumarate induces immunosuprresion via glutathione depletion and subsequent induction of heme oxygenase 1. J. Investig. Dermatol. 2007, 127, 835–845. [Google Scholar] [CrossRef]
- Iannone, L.F.; Bennardo, L.; Palleria, C.; Roberti, R.; de Sarro, C.; Naturale, M.D.; Dastoli, S.; Donato, L.; Manti, A.; Valenti, G.; et al. Safety profile of biologic drugs for psoriasis in clinical practice: An Italian prospective pharmacovigilance study. PLoS ONE 2020, 15, e0241575. [Google Scholar] [CrossRef]
- Passante, M.; Dastoli, S.; Nisticò, S.P.; Bennardo, L.; Patruno, C. Effectiveness of brodalumab in acrodermatitis continua of Hallopeau: A case report. Dermatol. Ther. 2020, 33, e13170. [Google Scholar] [CrossRef]
- Hawkes, J.E.; Yan, B.Y.; Chan, T.C.; Krueger, J.G. Discovery of the IL-23/IL-17 Signaling Pathway and the Treatment of Psoriasis. J. Immunol. 2018, 201, 1605–1613. [Google Scholar] [CrossRef]
- Gisondi, P.; Del Giglio, M.; Girolomoni, G. Treatment Approaches to Moderate to Severe Psoriasis. Int. J. Mol. Sci. 2017, 18, 2427. [Google Scholar] [CrossRef]
- Gniadecki, R.; Bang, B.; Bryld, L.E.; Iversen, L.; Lasthein, S.; Skov, L. Comparison of long-term drug survival and safety of biologic angents in patients with psoriasis vulgaris. Br. J. Dermatol. 2015, 172, 244–252. [Google Scholar] [CrossRef]
- Rehman, K.; Zulfakar, M.H. Recent advences in gel technologies for topical and transdermal drug delivery. Drug Dev. Ind. Pharm. 2014, 40, 433–440. [Google Scholar] [CrossRef]
- Lotti, T.; Hercogova, J.; Prignano, F. The concept of psoriatic disease: Can cutaneous psoriasis any longer be separated by the systemic comorbidities? Dermatol. Ther. 2010, 23, 119–122. [Google Scholar] [CrossRef]
- Oliverida, M.d.F.; Rocha, B.d.O.; Duarte, G.V. Psoriasis: Classical and emerging comorbidites. An. Bras. Dermatol. 2015, 90, 9–20. [Google Scholar] [CrossRef]
- Henseler, T.; Christophers, E. Diease concomitance in psoriasis. JAAD 1995, 32, 982–986. [Google Scholar] [CrossRef]
- Christophers, E. Comorbidities in psoriasis. Clin. Dermatol. 2007, 25, 529–534. [Google Scholar] [CrossRef]
- Sarkar, R.; Chugh, S.; Bansal, S. General measures and quality of life issues in psoriasis. Indian Dermatol. Online J. 2016, 7, 481–488. [Google Scholar] [CrossRef]
- Bienias, W.; Uczniak, S.; Pastuszka, M.; Kaszuba, A. Łuszczyca—Psychologiczne, społeczne i ekonomiczne aspekty schorzenia. Post. Dermatol. Alergol. 2011, 3, 138–143. [Google Scholar]
- Grozdev, I.; Kast, D.; Cao, L.; Carlson, D.; Pujari, P.; Schmotzer, B.; Babineau, D.; Kern, D.; McCormick, T.; Cooper, K.D.; et al. Physical and Mental Impact of Psoriasis Severity as Measured by the Compact Short Form-12 Health Survey (SF-12) Quality of Life Tool. J. Investig. Dermatol. 2012, 132, 1111–1116. [Google Scholar] [CrossRef]
- Sathyanarayana Rao, T.S.; Basavaraj, K.H.; Das, K. Psychosomatic paradigms in psoriasis: Psoriasis, stress and mental health. Indian J. Psychiatry 2013, 55, 313–315. [Google Scholar] [CrossRef]
- Hongbo, Y.; Thomas, C.L.; Harrison, M.A.; Salek, M.S.; Finaly, A.Y. Translating the science of quality of life into practice: What do dermatology life quality index scores mean? J. Investig. Dermatol 2005, 125, 659–664. [Google Scholar] [CrossRef]
- Teixeria, A.; Vasconcelos, V.; Teixeira, M.; Almeida, V.; Azevedo, R.; Torres, T.; Sousa Lobo, J.M.; Costa, P.C.; Almeida, I.E. Mechanical Properties of Topical Anti-Psoriatic Medicines: Implications for Patient Satisfaction with Treatment. AAPS Pharm. Sci. Tech. 2019, 20, 1–10. [Google Scholar] [CrossRef]
- Kulawik-Pióro, A.; Ptaszek, A.; Kruk, J. Effective tool for assessment of the quality of barrier creams—Relationships between rheological, textural and sensory properties. Regul. Toxicol. Pharmacol. 2019, 103, 113–123. [Google Scholar] [CrossRef]
- Thorneloe, R.J.; Bundy, C.; Griffiths, C.E.M.; Ashcroft, D.M.; Cordingley, L. Adherence to medication in patients with psoriasis: A systematic review. Br. J. Dermatol. 2013, 168, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Iversen, L.; Dauden, E.; Segaert, S.; Freeman, K.; Magina, S.; Rigopoulos, D.; Thaci, D. Reformulations of weel-known active ingredients in the topical treatment of psoriasis vulgaris can improve clinical outcomes for patients. J. Eur. Acad. Dermatol. Venerol. 2017, 31, 1271–1284. [Google Scholar] [CrossRef] [PubMed]
- Limón, D.; Talló Domínguez, K.; Garduńo-Ramírez, M.L.; Andrade, B.; Calpena, A.C.; Pérez-García, L. Nanostructured supramolecular hydrogels: Towards the topical treatment of Psoriasis and other skin diseases. Colloids Surf. B Biointerfaces 2019, 181, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.K.; Das, B. Introduction to polymeric gels. In Polymeric Gels Characterization, Properties and Biomedical Applications, 1st ed.; Pal, K., Banerjee, I., Eds.; Woodhead Publishing, Elsevier Ltd.: Cambridge, UK, 2018; pp. 3–27. [Google Scholar]
- Shapiro, Y.E. Structure and dynamics of hydrogels and organogels: An NMR spectroskopy approach. Prog. Polym. Sci. 2011, 36, 1184–1253. [Google Scholar] [CrossRef]
- Shakeel, A.; Farooq, U.; Gabriele, D.; Marangonie, A.G.; Lupi, F.R. Bigels and multi-component organogels: An overview from rheological perspective. Food Hydrocoll. 2021, 111, 106190. [Google Scholar] [CrossRef]
- Ueda, C.T.; Shah, V.P.; Deredzinski, K.; Ewing, G.; Flynn, G.; Maibach, H.; Marcues, M.; Rytting, H.; Shaw, S.; Thakker, K.; et al. Topical and transdermal drug products. Pharmacop. Forum 2009, 35, 750–764. [Google Scholar] [CrossRef]
- Shakeel, A.; Farooq, U.; Iqbal, T.; Yasin, S.; Lupi, F.R.; Gabriele, D. Key characteristics and modelling of bigels systems: A review. Mater. Sci. Eng. C 2019, 97, 932–953. [Google Scholar] [CrossRef]
- Patil, P.B.; Datir, S.K.; Saudagar, R.B. A Review on Topical Gels as Drug Delivery System. JDDT 2019, 9, 989–994. [Google Scholar] [CrossRef]
- Bohidar, H.B.; Dubin, P.; Osada, Y. Polymer Gels, Fundamentals and Applications, 1st ed.; American Chemical Society: Washington, DC, USA, 2003. [Google Scholar]
- Redkar, M.R.; Patil, S.V.; Rukari, T.G. Emulgel: A modern tool for topical drug delivery. World J. Pharm. Res. 2019, 8, 586–597. [Google Scholar] [CrossRef]
- Marangoni, A.G. Oleogoels: An introduction. In Edible Oleogels, 2nd ed.; Marangoni, A.G., Garti, N., Eds.; AOCS Press: Urbana, IL, USA, 2018; pp. 1–29. [Google Scholar]
- Li, J.; Mooney, D.J. Designing hydrogels for controlled drug delivery. Nat. Rev. Mater. 2016, 1, 16071. [Google Scholar] [CrossRef]
- Shakeel, A.; Lupi, F.R.; Gabriele, D.; Baldiono, N.; De Cindio, B. Bigels: A unique class of materials for drug delivery applications. Soft Mater. 2018, 17, 77–93. [Google Scholar] [CrossRef]
- Sharadha, M.; Gowda, D.V.; Vishal Gupta, N.; Akhila, A.R. An overview on topical drug delivery system—Updated review. Int. J. Res. Pharm. Sci. 2020, 11, 368–385. [Google Scholar] [CrossRef]
- Kajiwara, K. Structure of gels. In Gels Handbook the Fundamentals, 1st ed.; Osada, Y., Kajiwara, K., Fushimi, T., Irasa, O., Hirokawa, Y., Matsunaga, T., Shimomura, T., Wang, L., Ishida, H., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2001; Volume 4, pp. 122–171. [Google Scholar]
- Sharma, B.; Singh, L.R. Pharmaceutical gels for topical drug delivery: An overview. Int. J. Pharm. Pharm. Sci. 2018, 2, 19–24. [Google Scholar]
- Jagur-Grodzinski, J. Polymeric gels and hydrogels for biomedical and pharmaceutical applications. Polym. Adv. Technol. 2010, 21, 27–47. [Google Scholar] [CrossRef]
- Chang, R.K.; Raw, A.; Lionberger, R.; Yu, L. Generic development of topical dermatologic products: Formulation development, process developmnet and testing topical dermatologic products. AAPS J. 2013, 15, 41–52. [Google Scholar] [CrossRef]
- Lu, Z.; Fassihi, R. Influence of Colloidal Silicon Dioxide on Gel Strength, Robustness, and Adhesive Properties of Diclofenac Gel Formulation for Topical Application. AAPS Pharm. Sci. Tech. 2015, 16, 636–644. [Google Scholar] [CrossRef]
- Zhai, H.; Maibach, H.I. Effects of skin occlusion on percutaneous absorption: An overview. Skin Pharmacol. Physiol. 2001, 14, 1–10. [Google Scholar] [CrossRef]
- Patel, A.R. Alternative Routes to Oil Structuring, 1st ed.; Springer: New York, NY, USA, 2015; pp. 1–120. [Google Scholar]
- Peppas, N.A.; Bures, P.; Leobandung, W.; Ichikawa, H. Hydrogels in pharmaceutical formulations. Eur. J. Pharm. Biopharm. 2000, 50, 27–46. [Google Scholar] [CrossRef]
- Chen, X.; Peng, L.-H.; Shan, Y.-H.; Li, N.; Wei, W.; Yu, L.; Li, Q.-M.; Liang, W.-Q.; Gao, J.-Q. Astragaloside IV-loaded nanoparticle-enriched hydrogel induces wound healing and anti-scar activity throuhg topical delivery. Int. J. Pharm. 2013, 447, 171–181. [Google Scholar] [CrossRef]
- Gong, C.; Wu, Q.; Wang, Y.; Zhang, D.; Luo, F.; Zhao, X.; Wei, Y.; Qian, Z. A biodegradable hydrogel system contaning curcumin encapsulated in micelles for cutaneous wound healing. Biomaterial 2013, 34, 6377–6387. [Google Scholar] [CrossRef]
- Choi, S.; Beak, E.; Davaa, E.; Nho, Y.-C.; Lim, Y.-M.; Park, J.-S.; Gwon, H.-J.; Huh, K.M.; Park, J.-S. Topical treatment of the buccal mucosa and wounded skin in rats with triamcinolone acetonide-loaded hydrogel prepared using an electron beam. Int. J. Pharm. 2013, 447, 102–108. [Google Scholar] [CrossRef]
- Du, X.; Zhoou, J.; Shi, J.; Xu, B. Supramolecular hydrogelators and hydrogles from soft matter to molecular biomaterials. Chem. Rev. 2015, 115, 13165–13307. [Google Scholar] [CrossRef]
- Gellardo, V.; Munoz, M.; Ruiz, M.A. Formulations of hydrogels and lipogels with witamin E. J. Cosmet. Dermatol. 2005, 4, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Mitura, S.; Sionkowska, A.; Jaiswal, A. Biopolymers for hydrogels in cosmetics: Review. J. Mater. Sci. Mater. Med. 2020, 31, 50–64. [Google Scholar] [CrossRef] [PubMed]
- Peppas, N.A.; Merrill, E.W. Crosslinked poly(vinyl alcohol) hydrogels as swollen elastic networks. J. Appl. Sci. 1977, 21, 1763–1770. [Google Scholar] [CrossRef]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2002, 17, 3–12. [Google Scholar] [CrossRef]
- Vintiloiu, A.; Leroux, J.C. Organogels and their use in drug delivery—A review. J. Control. Release 2008, 125, 179–192. [Google Scholar] [CrossRef]
- Sushil, R.; Santosh, S.B.; Vaibah, U.; Mishra, V.; Gahane, A.; Kain, S.K. Lecithin organogel: A unique micellar system for the delivery of bioactive agents in the treatment of skin aging. Acta Pharm. Sin. B 2012, 2, 8–15. [Google Scholar] [CrossRef]
- Rajiv, K.; Om, P.K. Lecithin organogel as a potential phospholipid structured system for topical drug delivery: A reveiw. AAPS Pharma. Sci. Tech. 2005, 6, 298–310. [Google Scholar] [CrossRef]
- Shaikh, I.M.; Jadhav, K.R.; Gide, P.S.; Kadam, V.J.; Pisal, S.S. Topical delivery of aceclofenac from lecithin organogels: Preformulation study. Curr. Drug Deliv. 2006, 3, 417–427. [Google Scholar] [CrossRef]
- Willimann, H.; Walde, P.; Luisi, L.; Gazzaniga, A.; Stroppolo, F. Lecithin organogels as matrix for transdermal transport drugs. J. Pharm. Sci. 1992, 81, 871–874. [Google Scholar] [CrossRef]
- Shoo, S.; Kumar, N.; Bhattacharya, C.; Safiri, S.S.; Jain, K.; Pal, K.; Ray, S.S.; Nayak, B. Organogels: Properties and application in drug delivery. Des. Monomers. Polym. 2011, 14, 95–108. [Google Scholar] [CrossRef]
- Davidovich-Pinhas, M. Oleogles: A promising tool for delivery of hydrophobic bioactive molecules. Ther. Deliv. 2016, 7, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Davidovich-Pinhas, M. Chapter 8: Oleogels. In Polymeric Gels Characterization, Properties and Biomedical Applications, 1st ed.; Pal, K., Banerjee, I., Eds.; Woodhead Publishing, Elsevier Ltd.: Cambridge, UK, 2018; pp. 231–249. [Google Scholar]
- Sowa-Kasprzak, K.; Żwawiak, J.; Zaprutko, L. Organożele jako nowoczesne nośniki leków. Polimery 2018, 63, 169–177. [Google Scholar] [CrossRef]
- Mohamed, M.I. Optimization of chlorphensin emulgel formulation. AAPS J. 2004, 6, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Khullar, R.; Kumar, D.; Seth, N.; Saini, S. Formulation and evalutaion of mefanemic acid emulgel for topical delivery. Saudi Pharm. J. 2012, 20, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Stanos, S.P. Topical agents for the managment of musculoskeletal pain. J. Pain Symptom Magn. 2007, 33, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Dhawas, V.; Dhabarde, D.; Patil, S. Emulgel: A comprehensive review for novel topical drug delivery system. Int. J. Recent Sci. Res. 2020, 11, 38134–38138. [Google Scholar] [CrossRef]
- Burki, I.K.; Khan, M.K.; Khan, B.A.; Uzair, B.; Braga, V.A.; Jamil, Q.A. Formulation Development, Characterization, and Evaluation of a Novel Dexibuprofen-Capsaicin Skin Emulgel with Improved In Vivo Anti-inflammatory and Analgesic Effects. AAPS Pharm. Sci. Tech. 2020, 21, 211. [Google Scholar] [CrossRef]
- Raut, S.; Uplanchiwar, V.; Bhadoria, S.; Gahane, A.; Jain, S.K.; Patil, S. Comparative evaluation of zidovudine loaded hydrogels and emulgels. Res. J. Pharm. Technol. 2012, 5, 41–45. [Google Scholar]
- Badilli, U.; Amasya, G.; Özkan, S.; Tarimci, N. Simultaneous determination of clobetasol propionate and calcipotriol in a novel fixed dose emulgel formulation by LC-UV. Chromatographia 2012, 76, 1–8. [Google Scholar] [CrossRef]
- Badilli, U.; Amasya, G.; Şen, T.; Tarimci, N. Topical emulgel formulation containing inclusion complex of calcipotriol with cyclodextrin. J. Incl. Phenom. Macrocycl. Chem. 2014, 78, 249–255. [Google Scholar] [CrossRef]
- Moniruzzaman, M.; Tamura, M.; Tahara, Y.; Kamiya, N.; Goto, M. Ionic liquid-in-oil microemulsion as a potential carrier of sparingly soluble drug: Characterization and cytotoxicity evaluation. Int. J. Pharm. 2010, 400, 243–250. [Google Scholar] [CrossRef]
- Dixit, A.S.; Charyulu, N.; Nayari, H. Design and evaluation of novel emulgel containing acyclovir for herpes simplex keratitis. Lat. Am. J. Pharm. 2011, 30, 844–852. [Google Scholar]
- Ajazuddin, A.A.; Khichariya, A.; Gupta, S.; Patel, R.J.; Giri, T.K.; Tripathi, D.K. Recent expansions in an emergent novel drug delivery technology: Emulgel. J. Control. Release 2013, 171, 122–132. [Google Scholar] [CrossRef]
- Baibhav, J.; Gurpreet, S.; Rana, A.C.; Saini, S.; Vikas, S. Emulgel: A comprehensive review on the recent advances in topical drug delivery. Int. Res. J. Pharm. 2011, 2, 66–70. [Google Scholar]
- Rhee, G.J.; Woo, J.S.; Hwang, S.J.; Lee, Y.W.; Lee, C.H. Topical ole-hydrogel preparation of ketoprofen with enanced skin permeability. Drug Dev. Ind. Pharm. 1999, 25, 717–726. [Google Scholar] [CrossRef]
- Almedia, I.F.; Fernandes, A.R.; Fernandes, L.; Pena Ferreira, M.R.; Costa, P.C.; Bahia, M.G. Moisturizing effect of oleogel/hydrogel mixtures. Pharm. Dev. Technol. 2008, 13, 487–494. [Google Scholar] [CrossRef]
- Singh, V.K.; Qureshi, D.; Nayak, S.K.; Pal, K. Chapter 10: Bigels. In Polymeric Gels Characterization, Properties and Biomedical Applications, 1st ed.; Pal, K., Banerjee, I., Eds.; Woodhead Publishing, Elsevier Ltd.: Cambridge, UK, 2018; pp. 265–282. [Google Scholar]
- Lupi, F.R.; Shakeel, A.; Greco, V.; Rossi, C.O.; Baldino, N.; Gabriele, D. A rheological and microstructural characterisation of bigels for cosmetic and pharmaceutical uses. Mater. Sci. Eng. C. 2016, 69, 358–365. [Google Scholar] [CrossRef]
- Andonova, V.Y.; Peneva, P.T.; Apostolova, E.G.; Dimcheva, T.D.; Peychev, Z.L.; Kassarova, M.I. Carbopol hydrogel/sorbitan monostearate-almond oil based organogel biphasic formulations: Preparation and characterization of the bigels. Trop. J. Pharm. Res. 2017, 16, 1455–1463. [Google Scholar] [CrossRef]
- Ullah, F.; Othman, M.B.H.; Javed, F.; Ahmad, Z.; Akil, H.M. Classification, processing and application of hydrogels: A review. Mater. Sci. Eng. C 2015, 57, 414–433. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Narain, R.; Zeng, H. Chapter 10—Hydrogels. In Polymer Science and Nanotechnology Fundamentals and Applications, 1st ed.; Narin, R., Ed.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 203–244. [Google Scholar]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2012, 64, 18–23. [Google Scholar] [CrossRef]
- Otto, W.; Drahoslav., L. Hydrophilic gels in biologic use. Nature 1960, 185, 117–118. [Google Scholar] [CrossRef]
- Wrzecionek, M.; Szymaniak, M.; Gadomska-Gajadhur, A. Materiały hydrożelowe i ich zastosowanie w medycynie. In Wybrane Rozwiązania Technologiczne W Medycynie, 1st ed.; Pilarz, Ł.B., Ed.; Wydawnictwo Naukowe TYGIEL sp. z o.o.: Lublin, Poland, 2018. [Google Scholar]
- Narayanaswamy, R.; Torchilin, V.P. Hydrogels and Their Applications in Targeted Drug Delivery. Molecules 2019, 24, 603. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.C.I.M.; Ahmad, N.; Halib, N.; Ahmad, I. Synthesis and characterizaton of thermo- and pH-responsive bacterial cellulose/acrylic acid hydrogels for drug delivery. Carbohydr. Polym. 2012, 88, 465–473. [Google Scholar] [CrossRef]
- Bhattarai, N.; Gunn, J.; Zhang, M. Chitosan-based hydrogels for controlled, localllized drug delivery. Adv. Deliv. Rev. 2010, 62, 83–99. [Google Scholar] [CrossRef]
- Quattrone, A.; Czajka, A.; Sibilla, S. Thermosensitive Hydrogel Mask Significantly Improves Skin Moisture and Skin Tone: Bilateral Clinical Trial. Cosmetic 2017, 4, 17. [Google Scholar] [CrossRef]
- Paulsen, E.; Korsholm, L.; Brandrup, F. A double-blind, placebo-controlled study of a commercial Aloe vera gel in the treatment of slight to moderate psoriasis vulgaris. JEADV 2005, 19, 326–331. [Google Scholar] [CrossRef]
- Tripathi, P.; Kumar, A.; Kumar Jain, P.; Patel, J.R. Carbomer gel bearing methotrexate loaded lipid nanocontainers shows improved topical delivery intended for effective management of psoriasis. Int. J. Biol. Macromol. 2018, 120, 1322–1334. [Google Scholar] [CrossRef]
- Kaur, N.; Sharma, K.; Bedi, N. Topical Nanostructured Lipid Carrier Based Hydrogel of Mometasone Furoate for the Treatment of Psoriasis. Pharm. Nanotechnol. 2018, 6, 133–143. [Google Scholar] [CrossRef]
- Wadher, K.; Dabre, S.; Gaidhane, A.; Trivedi, S.; Umekar, M. Evaluation of antipsoriatic activity of gel containing Pongamia pinnata extract on Imiquimod-induced psoriasis. Clin. Phytosci. 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Patil, S.C.; Gadade, D.D.; Rathi, P.B. Design, Development and Evaluation of Herbal Gel for Treatment of Psoriasis. JIPBS 2015, 2, 72–87. [Google Scholar]
- Sondhi, S.; Singh, N.; Goyal, K.; Jindal, S. Development of Topical Herbal Gel of Berberine Hydrochloride for the Treatment of Psoriasis. Res. J. Pharma. Dos. Forms Tech. 2021, 13, 12–18. [Google Scholar] [CrossRef]
- Hughes, N.E.; Marangoni, A.G.; Wright, A.J.; Rogers, M.A.; Rush, J.W.E. Potential food applications of edible oil organogels. Trends Food Sci. Tech. 2009, 20, 470–480. [Google Scholar] [CrossRef]
- Schaink, H.M.; van Melssen, K.F.; Morgado-Alves, S.; Kalnin, D.; van der Linden, E. Crystal network for edible oil organogels: Possibilitities and limitations of the fatty acid and fatty alcohol systems. Food Res. Int. 2007, 40, 1185–1193. [Google Scholar] [CrossRef]
- Lupi, F.R.; Garbiele, D.; Facciolo, D.; Baldiono, N.; Seta, L.; de Cindio, B. Effect of organogelator and fat source on rheological properties of olive oil-based organogels. Food Res. Int. 2012, 46, 177–184. [Google Scholar] [CrossRef]
- Dassanayake, L.S.K.; Kodali, D.R.; Ueno, S. Formation of oleogels based on edible lipid materials. Curr. Opin. Colloid Interface Sci. 2011, 16, 432–439. [Google Scholar] [CrossRef]
- Patel, A.R. A colloidal gel perspective for understanding oleogelation. Curr. Opin. Food Sci. 2017, 15, 1–7. [Google Scholar] [CrossRef]
- Terech, P.; Weiss, R.G. Low molecular mass gelators of organic liquids and properties of their gels. Chem. Rev. 1997, 97, 3133–3159. [Google Scholar] [CrossRef]
- Van Esch, J.H.; Feringa, B.L. New functional materials based on self assembling organogels: From serendipity towards design. Angew. Chem. 2000, 39, 2263–2266. [Google Scholar] [CrossRef]
- Balasubramaian, R.; Sughir, A.A.; Damodar, G. Oleogel a promising base. Asian J. Pharm. 2012, 6, 1–9. [Google Scholar] [CrossRef]
- Almeida, I.F.; Bahia, M.F. Evaluation of the physical stability of two oleogels. Int. J. Pharm. 2006, 327, 73–77. [Google Scholar] [CrossRef]
- Da Pieve, S.; Calligaris, S.; Panozzo, A.; Arrighetti, G.; Nicoli, M.C. Effect of monoglyceride organogel structure on cod liver oil stability. Food Res. Int. 2011, 44, 2978–2983. [Google Scholar] [CrossRef]
- Rocha, J.C.B.; Lopes, J.D.; Masceranhas, M.C.N.; Arellano, D.B.; Guerreiro, L.M.R.; Cunha, R.L. Thermal and rheological properties of ogranogels formed by sugarcane of candelila wax in soybean oil. Food Res. Int. 2013, 50, 318–323. [Google Scholar] [CrossRef]
- Toro-Vazquez, J.F.; Morales-Rueda, J.A.; Dibildox-Alvadoro, E.; Charó-Alonso, M.; Alonzo-Macias, M.; González-Chávez, M.M. Thermal and textural properties of organogels developed by candelilla wax in safflower oil. J. Am. Oil Chem. Soc. 2007, 84, 989–1000. [Google Scholar] [CrossRef]
- Patel, A.R.; Mankoc, B.; Bin Sintang, M.D.; Lesaffer, A.; Dewettinck, K. Fumed silica-based organogels and aqueous-organic bigels. RSC Adv. 2015, 5, 9703–9708. [Google Scholar] [CrossRef]
- Nikiforids, C.V.; Gilbertt, E.P. Self-assamblies of lecithin and alfa-tocopherol as gelators of lipid materials. RSC Adv. 2014, 4, 2466–2473. [Google Scholar] [CrossRef]
- Bodennec, M.; Guo, Q.; Rousseau, D. Molecular and microstructural characterization of lecithin-based oleogels made with vegetable oils. RSC Adv. 2016, 6, 47373–47381. [Google Scholar] [CrossRef]
- Blach, C.; Gravelle, A.J.; Peyronel, F.; Weiss, J.; Barbut, S.; Marangoni, A.G. Revisitig the crystalization behaviour of stearyl alcohol: Stearic acid (SO:SA) mixtutres in edible oils. RSC Adv. 2016, 6, 81151–81163. [Google Scholar] [CrossRef]
- Gandolfo, F.G.; Bot, A.; Flöter, E. Structuring of edible oils by long chain FA, fatty alcohols and their mixtures. J. Am. Oil Chem. Soc. 2004, 81, 1–6. [Google Scholar] [CrossRef]
- Uvanesh, K.; Sagiri, S.S.; Senthilguru, K.; Pramanik, K.; Banerjee, I.; Anis, A.; Al-Zahrani, S.M.; Pal, K. Effect of Span 60 on microstructure crystalization kinetics and mechanical properties of stearic acid oleogels: A in-depth analysis. J. Food Sci. 2016, 81, E380–E387. [Google Scholar] [CrossRef]
- Bin Sintang, M.D.; Danthine, S.; Brown, A.; van de Walle, D.; Patel, A.R.; Tavernier, I.; Rimaux, T.; Dewettinck, K. Phytosterols-induced visoelasticty of oleogels prepared by using monoglyceriders. Food Res. Int. 2017, 100, 832–840. [Google Scholar] [CrossRef]
- Bot, A.; Agterof, W.G.M. Structuring of edible oils by mixtures of γ-oryzanol with β-sitosterol or related phytosterols. J. Am. Oil Chem. Soc. 2006, 83, 513–521. [Google Scholar] [CrossRef]
- Rogers, M.A. Ceramide oleogels. In Edible Oleogles Structure and Health Implications, 2nd ed.; Marangoni, A.G., Garti, N., Eds.; AOCS Press: Urbana, IL, USA, 2018; pp. 235–248. [Google Scholar]
- Sanchez, R.; Franco, J.M.; Delgado, M.A.; Valencia, C.; Gallegos, C. Rheology of oleogels based on sorbitan and glyceryl monosteatates and vegetavle oil for lubricating applications. Grasas Aceit. 2011, 62, 328–336. [Google Scholar] [CrossRef]
- Patel, A.R.; Cludts, N.; Sintang, M.D.; Lesaffer, A.; Dewettinck, K. Edible oleogels based on water soluble food polymers: Preparation, charakterization and potential applications. Food Funct. 2014, 5, 2833–2841. [Google Scholar] [CrossRef] [PubMed]
- De Vries, A.; Wesseling, A.; vad der Linden, E.; Scholten, E. Protein oleogels from heat set whey protein agregates. J. Colloid Interface Sci. 2017, 15, 75–83. [Google Scholar] [CrossRef]
- Suzuki, M.; Setoguchi, C.; Shirai, H.; Hanabusa, K. Organogelation by Polymer Organogelators with a L-Lysine Derivative: Formation of a Three-Dimensional Network Consisting of Supramolecular and Conventional Polymers. Chem. Eur. J. 2007, 13, 8193–8200. [Google Scholar] [CrossRef]
- Okuro, P.K.; Martins, A.J.; Vicente, A.; Cunha, R.L. Perspective, on oleogelator mixtures, structure design, and behaviour, towards or by the crosslinking/self-assembly of polymers in any other solvents. Curr. Opin. Food Sci. 2020, 35, 1–9. [Google Scholar] [CrossRef]
- Suzuki, M.; Hanbusa, K. Polymer organogeltaors that make supramolecular organogels through physical cross-linking and self-assembly. Chem. Soc. Rev. 2010, 39, 455–463. [Google Scholar] [CrossRef]
- Sreedevi, T.; Ramaya Devi, D.; Vedha Hari, B.N. An emerging era in topical delivery: Organogels. Int. J. Drug Dev. Res. 2012, 4, 35–40. [Google Scholar]
- Kolahdooz, S.; Karimi, M.; Esmaili, N.; Zargaran, A.; Kordafshari, G.; Mozafari, N.; Ayati, M.H. Evaluation of the efficacy of a topical chamomile-pumpkin oleogel for the treatment of plaque psoriasis: An intra-patient, double-blind, randomized clinical trial. Biomed. Res. Ther. 2018, 5, 2811–2819. [Google Scholar] [CrossRef]
- Rehman, K.; Tan, C.M.; Zulfakar, M.H. Development and In-vitro Characterization of Fish Oil Oleogels Containing Benzoyl Peroxide and Salicylic Acid as Keratolytic Agents. Drug Res. 2014, 6, 159–165. [Google Scholar] [CrossRef]
- Lee, C.H.; Moturi, V.; Lee, Y. Thixotropic property in pharmaceutical formulations. J. Control. Release 2009, 136, 88–98. [Google Scholar] [CrossRef]
- Naga Sravan Kumar Varma, V.; Maheshwari, P.V.; Navya, M.; Reddy, S.C.; Shivakumar, H.G.; Gowda, D.V. Calcipotriol delivery into the skin as emulgel for effective permeation. Saudi Pharm. J. 2014, 22, 591–599. [Google Scholar] [CrossRef]
- Sarafian, G.; Afshar, M.; Mansouri, P.; Asgarpanah, J.; Raoufinejad, K.; Rajabi, M. Topical Turmeric Microemulgel in the Management of Plaque Psoriasis: A Clinical Evaluation. Iran J. Pharm. Res. 2015, 14, 865–876. [Google Scholar]
- Pandey, S.S.; Maulvi, F.A.; Patel, P.S.; Shukla, M.R.; Shah, K.M.; Gupta, A.R.; Joshi, S.V.; Shah, D.O. Cyclosporine laden tailored microemulsion-gel depot for effective treatment of psoriasis: In vitro and in vivo studies. Colloid. Surf. B Biointerfaces. 2020, 186, 110681. [Google Scholar] [CrossRef]
- Miastkowska, M.; Kulawik-Pióro, A.; Szczurek, M. Nanoemulsion Gel Formulation Optimization for Burn Wounds: Analysis of Rheological and Sensory Properties. Processes 2020, 8, 1416. [Google Scholar] [CrossRef]
- Ahmad, J.; Gautam, A.; Komath, S.; Bano, M.; Garg, A.; Jain, K. Topical Nano-emulgel for Skin Disorders: Formulation Approach and Characterization. Recent Pat. Antiinfect. Drug Discov. 2019, 14, 36–48. [Google Scholar] [CrossRef]
- Algahtani, M.S.; Ahmad, M.Z.; Ahmad, J. Nanoemulgel for Improved Topical Delivery of Retinyl Palmitate: Formulation Design and Stability Evaluation. Nanomaterials 2020, 10, 848. [Google Scholar] [CrossRef]
- Pund, S.; Pawar, S.; Gangurde, S.; Divate, D. Transcutaneous delivery of leflunomide nanoemulgel: Mechanistic investigation into physicomechanical characteristics, in vitro anti-psoriatic and anti-melanoma activity. Int. J. Pharm. 2015, 487, 148–156. [Google Scholar] [CrossRef]
- Kamal Eldin Hussein, E.E. Topical Herbal Emulgel for Psoriasis Treatment. Available online: http://khartoumspace.uofk.edu/handle/123456789/26557 (accessed on 4 April 2021).
- Algahtani, M.S.; Ahmad, M.Z.; Ahmad, J. Nanoemulsion loaded polymeric hydrogel for topical delivery of curcumin in psoriasis. J. Drug Deliv. Sci. Technol. 2020, 59, 101847. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, A.; Sahni, J.K.; Ali, J.; Baboota, S. Nanoemulsion Based Hydrogel Containing Omega 3 Fatty Acids as a Surrogate of Betamethasone Dipropionate for Topical Delivery. Adv. Sci. Lett. 2012, 6, 221–231. [Google Scholar] [CrossRef]
- Ahmed, S.; Kumar, N. Omega 3—Fatty Acid (Epa and Dha) Rich Salmon Fish Oil Enhance Anti-Psoriatic activity of Glucocorticoid (Betamethasone Dipropionate) in Nano Form. Int. J. Drug Dev. Res. 2014, 6, 61–76. [Google Scholar]
- Marwaha, T.K. Formulation design and evaluation of herbal Anti psoriatic Emulgel. JPSI 2013, 2, 30–42. [Google Scholar] [CrossRef]
- Baboota, S.; Alam, S.; Sharma, S.; Sahni, J.K.; Kumar, A.; Ali, J. Nanocarrier-based hydrogel of betamethasone dipropionate and salicylic acid for treatment of psoriasis. Int. J. Pharm. Investig. 2011, 1, 139–147. [Google Scholar] [CrossRef]
- Cates, M.E.; Clegg, P.S. Bigels: A new class of soft materials. Soft Mater. 2008, 4, 2132–2138. [Google Scholar] [CrossRef]
- Hamed, R.; AbuRezeq, A.; Tarawneh, O. Development of hydrogels, oleogels and bigels for periodontitis. Drug Dev. Ind. Pharm. 2018, 44, 1488–1497. [Google Scholar] [CrossRef]
- Kodela, S.P.; Pandey, P.M.; Nayak, S.K.; Uvanesh, K.; Anis, A.; Pal, K. Novel agar-stearyl oleogel based bigels as structured delivery systems. Int. J. Polym. Mater. 2017, 66, 669–673. [Google Scholar] [CrossRef]
- Martins, A.J.; Silva, P.; Maciel, F.; Pastrana, L.M.; Cunha, R.L.; Cerqueira, M.A.; Vicente, A.A. Hybrid gels: Influence of oleogel/hydrogel ratio on rheological and textural properties. Food Res. Int. 2019, 116, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Behera, B.; Sagiri, S.S.; Singh, V.K.; Pal, K.; Anis, A. Mechanical properties and delivery of drug/probiotics from starch and non-starch based novel bigels: A comparative study. Starch 2014, 66, 865–879. [Google Scholar] [CrossRef]
- Singh, V.; Singh, V.K.; Banerjee, I.; Agarwal, T.; Pramanik, K.; Bhattacharya, M.K.; Pal, K. Guar Gum and Sesame Oil Based Novel Bigels for Controlled Drug Delivery. Colloid. Surf. B Biointerfaces 2014, 123, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Anis, A.; Banerjee, I.; Pramanik, K.; Bhattacharya, M.K.; Pal, K. Preparation and characterization of novel carbopol based bigels for topical delivery of metronidazole for the treatment of bacterial vaginosis. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 44, 151–158. [Google Scholar] [CrossRef]
- Behera, B.; Singh, V.K.; Senthilguru Kulanthaivel, M.K.; Paramanik, K.; Banerjee, I.; Pal, K. Physical and mechanical properties of sunflower oil and synthetic polymers based bigels for the delivery of nitroimidazole antibiotic—A thereapuetic aproach for controlled drug delivery. Eur. Polym. J. 2015, 64, 253–264. [Google Scholar] [CrossRef]
- Ibrachim, M.M.; Hafez, S.A.; Mahdy, M.M. Organogel, hydrogels bigels as transdermal delivery systems for diltiazem hydrochloride. Asian J. Pharm. Sci. 2013, 8, 48–57. [Google Scholar] [CrossRef]
- Sagiri, S.S.; Singh, V.K.; Kulanthaivel, S.; Banerjee, I.; Basak, P.; Battachrya, M.K.; Pal, K. Stearate organogel-gelatin hydrogel based bigels: Physicochemical, thermal, mechanical characterizations and in vitro drug delivery applications. J. Mech. Behav. Biomed. Mater. 2015, 43, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Satapathy, S.; Singh, V.K.; Sagiri, S.S.; Agarwal, T.; Banerjee, I.; Bhattacharya, M.K.; Kumar, N.; Pal, K. Development and characterization of gelatin-based hydrogels, emulsion hydrogels, and bigels: A comparative study. J. Appl. Polym. Sci. 2015, 132, 1–12. [Google Scholar] [CrossRef]
- Andonova, V.; Peneva, P.; Georgiev, G.S.; Toncheva, V.T.; Apostolova, E.; Peychev, Z.; Dimitrova, S.; Katsarova, M.; Petrova, N.; Kassarova, M. Ketoprofen-loaded polymer carriers in bigel formulation: An approach to enhancing drug photostability in topical application forms. Int. J. Nanomed. 2017, 12, 6221–6238. [Google Scholar] [CrossRef]
- Khelifi, I.; Saada, M.; Hayouni, E.A.; Tourette, A.; Bouajla, J.; Ksouri, R. Development and Characterization of Novel Bigel-Based 1,4-Naphthiquinones for Topical Application with Antioxidant Potential. Arab. J. Sci. Eng. 2020, 45, 53–61. [Google Scholar] [CrossRef]
- Salim, N.; Ahmad, N.; Musa, S.H.; Hashim, R.; Tadros, T.F.; Basri, M. Nanoemulsion as dopical delivery systems. RSC Adv. 2016, 6, 6234–6250. [Google Scholar] [CrossRef]

{kind=link}
| Gel Type | Specific Characteristics | Advantages | Disadvantages | Use | References |
|---|---|---|---|---|---|
| Hydrogels | – three-dimensional hydrophilic polymer networks that can absorb large quantities of liquids or biological fluids – the used gelling substances are hydrophilic in nature and contain groups such as hydroxyl groups, carboxyl groups, sulfonic acid groups, amide groups, imide groups – hydrophilic nature, high swelling ability, liquid capturing ability, softness, elasticity, flexibility | – cheap – biocompatible and non-toxic – biodegradable – versatile: many active substances can be introduced into their recipes, the release of therapeutic substances from hydrogel structures can be activated at any time by changes in temperature, local pH, physical stimuli, as well as by the presence of various types of enzymes – providing a starting point for other gel formulations, such as liposomal gels, emulgels, bigels – possibility of modifying and adapting the material to perform a specific function – sensitivity to external environment (temperature, pH, ionic strength) – good mucoadhesion – possibility of in vivo gelling by introducing first live cells into the hydrogel – well-tolerated by patients—low irritating potential – easily spreadable on the skin and water-washable – non-comedogenic – do not leave greasy film after application – cooling-effect – significant minimization of side effects | – poor mechanical strength – due to their hydrophilic nature, the transdermal delivery of the drug can be problematic—difficulty in introducing lipophilic substances into the recipe – polysaccharide-based hydrogels are easily contaminated by microbes – limited ability to improve barrier properties | – treatment of atopic dermatitis, eczema – anti-inflammatory products – care products: for hair, body, oral cavity – wound treatment, anti-scar activity – skin regeneration – dressing materials, dental materials, cell scaffolds, surgical adhesives and fillers, sensors, superabsorbents, medical implant components – due to the possibility of diffusion of the molecules of the active substance inside them, they are used as drug carriers for active substances with controlled release or as targeted release forms of the active substance and bioadhesive carriers of the drug | [2,50,65,67,84,85,86,87,88,89,90,91,92] |
| Organogels(also called oleogels) | – dispersion medium is an organic liquid (oil or non-polar liquid) entrapped within a thermoreversible three-dimensional gel network by using an organogelator – oleogelators: low-molecular weight components or oil soluble polymers | – easy to obtain – cheap – biocompatible – thermodynamically stable – due to an organogelator, they show an increased mechanical strength – creation of a crystalline network and entrapment of bulk oils despite low concentrations of organogelators <10% wt – suitable as a vehicle for transdermal drug delivery of lipophilic compounds – enhanced drug penetration through the stratum corneum because of their lipophilic nature – many of the organogel components perform an additional function of permeability promoters – thermoreversible – viscoelasticity – non-birefringence – optical clarity – more resistant to microbial infections than hydrogels and emulsions – the oils used in their production are safe for humans (many of them are used in the food industry) | – more favorable toward lipophilic drugs – stability problems at higher temperatures—increased stability requires the use of a specific group of gelators – oily texture—unpleasant sensation on the skin – difficult washing with water | – skin care products – emollients – compounding base – wound healing – drug carriers —transdermal systems, parenteral agents, bioadhesive agents, vaccine preparations, rectal products, preparations with analgesic, anti-inflammatory effect – in foods, oleogel is mainly aimed at structuring liquid oil with an emphasis to replace solid fats or to prevent oil migration (i.e., chocolate, sausages, cookies, cream filing) – another application of oil structuring includes the formation of green lubricants using oleogels as a thickener, paint, coating, and oil spillage treatments | [50,65,69,76,93,94,95,96,97,98,99,100,101] |
| Emulgel | – mainly emulsion-based gels—these are either an oil/water or water/oil type, which are gelled by incorporating a gelling agent | – simple to prepare and economical in terms of manufacturing because the steps involved in the preparation of the emulgel are simple, no special instruments are required – can be used as controlled release systems for medicines—they can supply both hydrophobic and lipophilic substances – thixotropic – can be easily spread and removed from the surface of the skin – non-staining – have an emollient effect – water soluble – bio-friendly – pleasant sensation on the skin—well-tolerated by patients – long shelf-life – materials used for its preparation are cheaper and easily available | – due to the necessary presence of a surfactant in their composition, they may have an irritating effect on the skin – air bubbles may be present after the obtaining process | – preparations with analgesic, anti-inflammatory effect – skin care—skin softening, moisturizing effect – used for treatment of various kinds of skin disorders, such as those caused by viral, bacterial, and fungal species (eczema, Herpes simplex, acne) – suitable for vaginal dryness, dehydration, and redness | [102,103,104,105,106,107,108,109,110,111,112,113] |
| Bigels | – solid-like formulations produced from a combination/mixture of oleogels and a hydrogel without the addition of surfactants – both unmixable phases are independently stabilized with independent gelators – types of bigels: oleogel dispersed in a hydrogel system, hydrogel dispersed in an oleogel system, bicontinuous bigel, complex bigel | – easy to obtain – no need to add an emulsifier to make the system physically stable—reducing skin irritation – improvement in the permeability of drugs through the skin – due to the presence of the aqueous and lipophilic phase, they can deliver lipophilic and hydrophilic substances deep into the skin – synergistic effect of hydrogels and oleogels compared to a single gel – increased hydration of stratum corneum – cooling-effect – good spreadability – water washability upon application to the skin – modification of the consistency and degree of release of the drug possible by changing the share of phases and/or type of the gelator | – the absence of an emulsifier promotes phase separation especially with longer storage times – lack of thermal reversibility—instability at high temperatures | – preparations with analgesic, anti-inflammatory effect – carrier for antibiotics, such as metronidazole, cicloproxolamine, diltiazem hydrochloride – moisturizing and care products | [50,67,69,75,114,115,116,117,118] |
| Origin | Examples |
|---|---|
| Natural | Alginic acid, pectin, hyaluronic acid, dextran sulfate, chondroitin sulfate, chitosan, polylysine, chitin, fibrin, collagen, gelatin, dextran, agar, pullulan |
| Synthetic | PEG-PLA-PEG, PEG-PLGA-PEG, PEG-PCL-PEG, PLA-PEG-PLA, PHB, PVA, PHEMA, polyphosphazene, N-vinylpyrrolidone |
| Combination of natural and synthetic hydrogelators | collagen-acrylate, alginate-acrylate, PEO-PPO-PEO |
| Solvent | Hydrogelator | Total Concentration of Hydrogelator | Additives | Drug | Key Rheological/Key Mechanical/Spreadability Properties | Key Findings of Effectiveness of Action | Ref. |
|---|---|---|---|---|---|---|---|
| Water | aloe vera leaf gel | 98% | xanthan gum, potassium sorbate, sodium benzoate, sodium sulfite, citric acid | aloe vera gel | no data available | – The score sum of erythema, infiltration, and desquamation decreased in 72.5% of the aloe vera-treated sites compared with 82.5% of the placebo-treated areas from week 0 to week 4, which was statistically significant in favor of the placebo treatment. | [128] |
| Water and/or ethanol | dicationic bis-imidazolium amphiphiles | 5 mg/mL | − | tacrolimus, methotrexate sodium salt, gemcitabine hydrochloride, triamcinolone acetonide, and betamethasone 17-valerate | – Amplitude sweep tests show that the phase angle for all samples across the Linear Viscoelastic Region (LVR) was relatively low (17°–20°). As well, G’ values are higher than G” ones in all samples. The results for these two parameters indicate that the elastic (solid-like) component is prevalent over the viscous (fluid-like) one. – Frequency sweep tests were performed in these gels at a constant shear stress of τ = 0.5 Pa for being within the LVR, finding also that, independently of the frequency applied, G’ is higher than G”, which confirms the solid-like behavior of these gels. | – Ex vivo skin permeation tests show how these gels successfully promote the drug permeation and retention inside the skin for reaching their therapeutic target, while in vivo experiments demonstrate that they decrease the hyperplasia and reduce the macroscopic tissue damage typically observed in psoriatic skin, significantly more than the drugs in solution. – Gels can incorporate drugs not only dissolved at the interstitial space, but also 72% of either gemcitabine or methotrexate, and 38% of tacrolimus, are found within their fibers. This unique fiber-incorporation behavior acts as a packaging that protects the drug, and more importantly, it influences a Two-Phase Exponential drug release profile, in which the first phase corresponds to the drug dissolved in the interstitial space of the gel, and the second phase corresponds to the drug exiting from the fibers. | [64] |
| Water | carbomer | 0.5% w/w | SLN (Solid Lipid Nanoparticles) and NLC (Nanostructured Lipid Carriers) composed of glyceryl monostearate and/or oleic acid as lipid constituents | methotrexate (MTX) | The spread diameter was found to be 6.8 for both formulations, which indicated good spreadability of carrier loaded gels. | – The pH of SLN and NLC hydrogel was determined to be 6.8 and 6.7, respectively, suggesting good skin compatibility. – The primary skin irritation studies indicated that MTX-loaded SLN or NLC hydrogels resulted in no erythema. It can be concluded that NLC represents a promising particulate carrier having prolonged drug release, improved skin permeation. – Skin permeation study of MTX-loaded SLN and NLC hydrogels showed prolonged drug release up to 24 h. – The skin drug deposition study showed the greatest deposition of drug enriched NLC hydrogel (28.8%) when compared to plain drug enriched hydrogel (11.4%) and drug enriched SLN hydrogel (18.6%). | [129] |
| Water | carbopol 940 | 0.5–2% v/w | NLC | Mometasone Furoate | Carbopol 940 was used to convert NLC dispersion into NLC-based hydrogel to improve its viscosity for topical administration. | – In vivo studies showed complete clearance of parakeratosis by treatment with the prepared NLC formulation. – NLC-based gel as compared to marketed formulation following Higuchi release kinetics. The skin deposition of the MF-loaded, NLC-based hydrogel was found to be 2.5 times higher than the marketed formulation. | [130] |
| Water | carbopol 934 | no data available | methyl parabens, propylene glycol | Hydroalcoholic extract from Pongamia pinnata (PP) leaves | The viscosity of the gel was found to be 2100 cps to 1400 cps at 1 rpm to 20 rpm. The spreadability was found to be 9.6 ± 0.53 g/s. |
– The drug content was found to be uniform throughout the formulated gel with the range of 92.32% ± 0.43, and the average value allowed the process adopted to prepare the gel to be capable of giving reproducible results.
– The prepared topical gel formulation with a PP extract released a maximum of 59.11% ± 0.512% of the extract over a period of 6 h, which shows that the gel formulation can control the release of the drug for a longer period of time. – The imiquimod-induced psoriatic mouse model showed a prominent antipsoriatic activity of the extract as evident through index grading. – Treatment with EPP confirmed a marked recovery from psoriasis in the treated groups, as there was a considerable diminution in the thickness and scaling of the skin. This was also confirmed through reduced grading of the PASI scale of the treated groups. – For the topical treatment with EPP, the result of histopathology clearly shows that regeneration in the tissue integrity was observed with greater collagen content, angiogenesis, keratinization, fibroblast proliferation as compared to the control groups. | [131] |
| Water | carbopol 940 | 1–4% w/v | ethanol, propylene glycol, methyl paraben, propylparaben, EDTA disodium | methanolic extract of Ricinus Communis | – The viscosity of the gel formulations generally reflects its consistency. Decrease in viscosity of the gel formulations showed increased drug release. - The viscosity of the studied formulations was 1210–1511 cps – Spreadability reached 30.66–54.3 mm | – The in vitro diffusion study carried out in a diffusion cell for 24 h and showed F9 formulation with maximum drug release (96.11%) as compared to other gel formulations. Samples F2, F3, and F9 showed a maximum release as compared to F1, F4, F5, F6, F7, and F8. This may be attributed to the percentage of carbopol 940 present in their composition. Carbopol contributes to the drug release of the gel formulation, and a decrease in the percentage of carbopol 940 causes an increase in the percentage of drug release. The optimal percentage of Carbopol 940 is 1%. – There are no in vivo studies concerning the effectiveness of the applied extract in psoriasis treatment | [132] |
| Water | carbopol 934 | 0.5–2% | glycerine, propyl glycol, methanol, Transcutol P, triethanolamine, methyl paraben, propyl paraben, | Berberine hydrochloride obtained from Tinospora cordifolia plant | – The concentration of carbopol influenced the consistency of the studied gel: low concentration—formulation becomes similar to a thick liquid only, not as a semi-solid substance. 2% concentration gives better gel properties, but at higher concentration, the gel becomes thick and non-homogenous with poor spreadability. – Viscosity range for preparations 2590–4494 cps – Spreadability 14.06–28.09 g.cm/s | – Berberine hydrochloride from the obtained hydrogel formulations may be released for 8 h. – The mechanism of drug release was found to be non-Fickian. – It was concluded from the results that the permeation of berberine hydrochloride hydrogel was enhanced by Transcutol P in two concentrations (0.1% and 0.2%). – There are no in vivo studies concerning the effectiveness of the obtained hydrogel in psoriasis treatment. | [133] |
| Solvent | Organogelator | Total Concentration of Gelators % Mass | Drug Employed | Additives | Key Rheological/Key Mechanical Properties | Key Findings of Effectiveness of Action | Ref. |
|---|---|---|---|---|---|---|---|
| Liquid paraffin | hydrogenated castor oil | no data available | Calcipotriol Betamethasone | Polyoxypropylene 15 stearyl ether, alpha tocopherol, BHT | – oleogel presented less pronounced shear thinning behavior with power law index (n) lower than 1 – oleogels showed no thixotropy – oleogel exhibited the lowest values of adhesiveness and firmness out of tested physicochemical forms | – the formulations with lower consistency, lower firmness and adhesiveness, such as creams and gels, were associated with higher patient satisfaction – textural analysis (adhesiveness, firmness), in particular spreadability and rheological characteristics, could be used in the prediction of patients’ satisfaction with topical treatment | [60] |
| Medicinal oleogel: M. chamomilla oil, C. pepo seed oil placebo: liquid paraffin, M. chamomilla oil, C. pepo seed oil, | colloidal silica | 5% | − | − | – the study (clinical study of 40 patients with mild to moderate plaque psoriasis) was limited only to the assessment of the effectiveness of the preparation against placebo | – the average values of the decrease of the PASI for the oleogel were significantly lower than in the placebo group. In accordance with PGA results, 35% of the patients using oleogel had a significant improvement of the skin condition against 0% of the placebo group – also the patients’ satisfaction with the therapy in the case of the medicinal oleogel was significantly higher than in the case of the placebo group – 37 people took part in the study, no one reported side effects | [162] |
| Fish oil | beeswax or sorbitan monostearate | Span 60 17.5–20 beeswax 7.5–15 | benzoyl peroxide (BP) salicylic acid (SA) | butylated hydroxyanisole (BHA) limonene | – no study of the rheological and mechanical properties of the obtained oleogels | – fish oil significantly increases the topical delivery of BP across the skin; such results were not achieved by the salicylic acid – beeswax is a better gelator for this system than sorbitan monostearate, optimum concentration in the formulation is 10% – in order to increase the SA penetration from the oleogel, its composition needs to be changed – all of the BP-fish oil oleogels and SA-fish oil oleogels showed significant difference in drug flux and cumulative release as compared with a commercial BP hydrogel and commercial hydrogel, respectively | [163] |
| Emulsion Type/Composition | Gelling Agent/Hydrogelator | Total Concentration of the Gelling Agent | Drug | Key Rheological/Key Mechanical/Spreadability Properties | Key Findings of Effectiveness of Action | Ref. |
|---|---|---|---|---|---|---|
| Emulsion/propylene glycol, Tween 60, methyl paraben, cetyl alcohol, stearyl alcohol, Span 60, liquid, and soft paraffins Cremophor EL | Carbopol 934 P | no data available | Calcipotriol | no data available | – The aim of this study was to develop a new topical drug delivery system of calcipotriol in order to improve the solubility and dissolution characteristics of the drug and reduce the undesirable side effects. – The drug release was significantly increased with the emulgel formulations compared to the commercial cream product. | [109] |
| Emulsion/ cocoyl caprylocaprate, polyoxyl 20 cetostearyl ether, liquid paraffin, propylene glycol, PEG 400, isopropyl alcohol, water | Carbopol 940 | 0.6–1.2% | Calcipotriol | The increase of the gelling agent concentration in the formulation causes the decrease of the formulation spreadability. | – Optimized formulation (carbopol concentration was 1%) had shown 86.42 ± 2.0% drug release at the end of an 8 h study. – The release rate through dialysis membrane and rat skin is higher when compared to a commercial calcipotriol ointment. | [165] |
| Microemulsion/ Tween 80, isopropyl alcohol, isopropyl myristate water | Carbopol 940 | 1% w/w | Cyclosporine | – The data indicate insufficient adhesiveness and high cohesiveness and gumminess of the prepared microemulsion-gel in comparison to marketed Volini gel. Thus, tailoring of Carbopol content is needed in future studies to achieve the required mechanical characteristics of the microemulsion gel. | The ex vivo diffusion study showed improved permeation (>24 h) with the microemulsion gel in comparison to cyclosporine suspension. | [167] |
| Nanoemulsion/ Capryol 90, Cremophor EL, Transcutol HP | Pluronic F127 | 1% | leflunomide | – Mechanical properties of the nanoemulgel measured as force–time relationship using mechanical texture characteristics were optimum for its convenient and easy application to the skin surface. – Complete mechanical characterization was carried out using Texture Analyzer and hardness, adhesiveness and springiness index were found to be 523 gms, 431 gms and 1.02, respectively. | The in vitro cytotoxicity of LFD nanoemulgel in human HaCaT, melanoma A375, and SK-MEL-2 cell lines showed significantly enhanced therapeutic response. In summary, LFD nanoemulgel for transcutaneous delivery will reduce the overall dose and drug consumption by effectively localizing at the applied target site and will ultimately minimize systemic side effects. | [171] |
| Emulsion | Carbopol 940 | 0.2–1.5 g | aqueous coffee extract, Myrrh alcoholic extract, Cymbopogon proximus (volatile oil), Nigella sativa seeds total oil, Olibanum alcoholic extract and theophylline | – All formulations have good spreadability and exhibit non-Newtonian behavior with pseudoplastic properties. | – Carbopol concentrations have direct influence on the viscosity and release of the active ingredients. —Optimized formulations were (E1) and (R3) that showed 77.60% and 97.16% mean cumulative % release respectively after 480 min. – No skin irritation was noticed. – Antipsoriatic activity study showed that (E1) emulgel decreased the number of nucleated cells, which shows significant increase in % orthokeratosis (p < 0.0001) in comparison with the control group, while (R3) showed lower effect compared to (E1). – The formulated (E1) emulgel (contains: 50% aqueous coffee extract, Myrrh alcoholic extract, Cymbopogon proximus (volatile oil), Nigella sativa seeds total oil, and Olibanum alcoholic extract) is a promising new herbal formula to treat psoriasis, also (R3) had antipsoriatic effect but lower than (E1). | [172] |
| Nanoemulsion Labrafac PGTM Tween 20 solutol-HS15 transcutol-HP and acconon-MC8-2–solubilizer for curcumin | Carbopol 934 | 0.25–1.0% w/w | curcumin | – Mean viscosity of formulations 123.85–130.53 cP – Placebo gel as well as CUR-NEG showed similar resistance and spreadability | – Despite the high solubility of curcumin in acconon-MC8-2, it showed physical incompatibility, while transcutol-HP was found to be compatible with the developed nanoemulsion. – The release of curcumin from the nanoemulsion follows Korsmeyer–Peppas kinetics with Fickian diffusion and exhibits a 4.87-fold increase in the permeation of curcumin from the developed nanoemulgel. – The nanoemulgel formulation exhibited quicker and early healing in psoriatic mice compared to curcumin and betamethasone-17-valerate gel. | [173] |
| Nanoemulsion/ fish oil Unitop 100 PEG 400, water | Carbopol 971 | betamethasone dipropionate (BD) | The obtained hydrogel-thickened nanoemulsion system (HTN) had a viscosity of 98.67 ± 0.06 PaS |
– The optimized formulation had a small average diameter (125 nm) with zeta potential of -39 mV, which indicated good long-term stability.
– In vivo anti-inflammatory activity indicated 87.64% and 48.76% inhibition of inflammation for drug-loaded and placebo formulations, respectively. | [174] | |
| Nanoemulsion/ Salmon fish oil Tween 80 Transcutol P water | ethyl cellulose, sodium alginate, Carbopol 934, Carbopol 971 HPMC | 1% |
Betamethasone Dipropionate (BD)
salicylic acid | – The obtained hydrogel-thickened nanoemulsion system (HTN) had a viscosity of 98.07 ± 0.07 mP. – As the concentration of the polymer increased, its viscosity increased simultaneously. A small quantity of the gel was pressed between the thumb and index finger and the consistency and homogeneity of the gel were observed. – Carbopol 971 in HTN resulted in high viscosity and oily droplets might be distributed in the gel network, which might contribute to the enhancement of the stability of droplets in the nanoemulsion. | – It was concluded that Carbopol 940, sodium alginate, and HPMC were not good gel-forming polymers for BD-loaded nanoemulsions. – Hydrogel containing 1% Carbopol 971 was found to have good viscosity, and the maximum amount of the drug was retained in the skin during the permeation study. – Overall, all the formulations have low irritation score; hence, they are safe for human use. – The optimized formulation had a small average diameter (129.89 nm) with zeta potential of 36.09 mV, which indicated good long-term stability. – In vivo anti-inflammatory activity indicated 85.22% and 33.31% inhibition of inflammation for drug-loaded and placebo formulations, respectively. – Anti-inflammatory activity of the placebo nanoemulsion reveals that salmon fish oil has an anti-inflammatory effect and in combination with BD may be useful for psoriasis treatment in the future. | [175] |
| Microemulsion/ Captex 355 Cremophor® RH Capmul MCM) | Sodium CMC, Methocel K4000M, HPMC CR, Carbopol 934, Carbopol 940 | no data available | Commiphora mukul (Gum guggul) Psoralea corylifolia (Babchi oil) | no data available | – In 24 h, there were no symptoms of allergies found on the rat skin (inflammation, redness, irritation). – For the M3 after 6 h, %EE was 79.72% and %DR was 94.34%. – In the control group that received carrageenan only, a rapid and continuous increase in paw volume was observed and the inflammation was sustained during the entire period of the 6 h study. In the groups that received test products, the percentage increase in paw volume was low when compared to the control group. This indicates that test and marked products possess good anti-inflammatory activity. – By comparing % of the inflammation inhibition, the market product and tested formulations reached 74.51% and 75.64%, respectively. | [176] |
| O/W microemulsion composed of oleic acid, sefsol, Tween 20, isopropyl alcohol, and distilled water | Carbopol 934 | 3% | betamethasone dipropionate and salicylic acid | The spreadability of the formulation was found to be 1.44 times greater than the marketed formulation (Betagel) | In vivo anti-inflammatory activity indicated 72.11% and 43.96% inhibition of inflammation in the case of the developed microemulsion gel and marketed gel, respectively. | [177] |
| Solvent | Gelator Agent | Total Conc. of Gelators (wt %) | Drug Employed | Additives | Organogel/ Hydrogel Ratio (wt/wt) | Key Rheological/ Mechanical Properties | Key Findings | Ref. | |
|---|---|---|---|---|---|---|---|---|---|
| Oil Phase | Water Phase | ||||||||
| Sweet almond oil or liquid paraffin | Span 60 Cholesterol Zinc stearate silicic acid | Carbopol 934 | 4.2–19.7 | − | triethanolamine | 2/98, 5/95, 7/93, 10/90, 12/88, 30/70, 50/50,70/30, 90/10 | – Textural profiles of the analyzed bigels are very similar to a hydrogel. – Oleogels presented higher firmness and adhesiveness than bigels and hydrogels. | – Type of the oleogel used in production determines the properties of the obtained bigel (the preparations differed in homogeneity as well as glossiness and smoothness). – Depending on the oleogel portion in the bigel, the moisturizing effect was observed after 2 to 4 h. – Bigels exhibit cooling effect, good spreadability, water washability (similar to hydrogel) with an enhanced emollience and moisturizing effect. | [115] |
| Almond oil | Span 60 | Carbopol 940 | 16 | − | propylene glycol, ethanol, triethanolamine | 20/80, 30/70, 40/60 | – Bigels belong to shear thinning fluids. – The increase of viscosity is observed together with the increase of Span 60 concentration in the recipe. – Bigel spreadability is affected by oleogel to hydrogel ratio. – Bigels were classified as semi-solid because the determined spread diameter was <50 mm. | – Bigels had pH suitable for skin application. No symptoms of skin toxicity (redness, edema), irritation, or inflammation were observed. The formulation can be considered as safe for dermal use. – Results of the FTIR analysis suggest lack of chemical interaction between the almond oil organogel and Carbopol hydrogel, as well as the existence of a physical mixture of the two phases. | [118] |
| Sweet almond oil | Span 65 | Alginate | 23.0 | 5,8-dihydroxy-1,4-naphthoquinone (M1) 2,3-dichloro-5,8-dihydroxy-1,4-naphthoquinone (M2) | − | 50/50 | – Non-Newtonian shear thinning fluids—the nature of the fluids is adequate for semi-solid formulations for topical application. | – Bigels with M1 and M2 substances have high quality, ensure skin protection against the damage caused by oxidative stress-mediated aging and UV radiation. – Active compounds have found a suitable environment with bigel matrix, so they preserved their antioxidant properties. – Bigels have pH suitable for skin application. – Bigel samples present a tridimensional network constituted by interconnected porosity and the pores were regular in size. The porous structure promotes their use for drug delivery. – They are well evaluated by the patients for the following properties: spreadability, lack of greasy sensation on the skin, absorption rate, give hydration sensation perceived as favorable, and a feeling of freshness. | [189] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulawik-Pióro, A.; Miastkowska, M. Polymeric Gels and Their Application in the Treatment of Psoriasis Vulgaris: A Review. Int. J. Mol. Sci. 2021, 22, 5124. https://doi.org/10.3390/ijms22105124
Kulawik-Pióro A, Miastkowska M. Polymeric Gels and Their Application in the Treatment of Psoriasis Vulgaris: A Review. International Journal of Molecular Sciences. 2021; 22(10):5124. https://doi.org/10.3390/ijms22105124
Chicago/Turabian StyleKulawik-Pióro, Agnieszka, and Małgorzata Miastkowska. 2021. "Polymeric Gels and Their Application in the Treatment of Psoriasis Vulgaris: A Review" International Journal of Molecular Sciences 22, no. 10: 5124. https://doi.org/10.3390/ijms22105124
APA StyleKulawik-Pióro, A., & Miastkowska, M. (2021). Polymeric Gels and Their Application in the Treatment of Psoriasis Vulgaris: A Review. International Journal of Molecular Sciences, 22(10), 5124. https://doi.org/10.3390/ijms22105124