
Local Interleukin-12 Treatment Enhances the Efficacy of Radiation Therapy by Overcoming Radiation-Induced Immune Suppression

 , and
, and
Abstract
:1. Introduction
2. Results
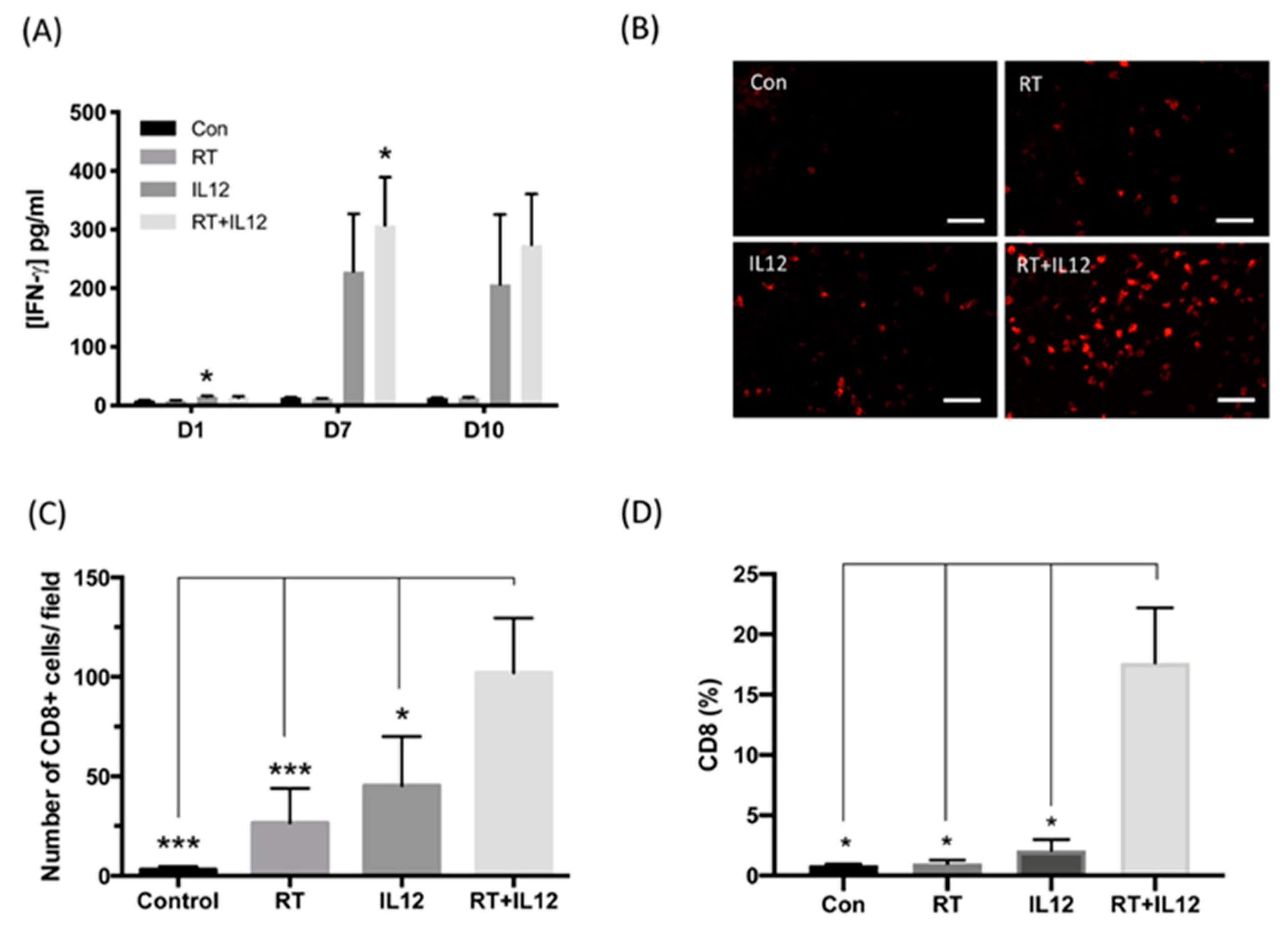
2.1. IL-12 Therapy Enhanced the Anti-Tumor Activity of RT
2.2. Combined RT and IL-12 Therapy Induced Systemic Anti-Tumor Activity
2.3. Combined Modality Therapy Promoted Vascular Maturation
2.4. Combined Modality Therapy Reduced the Occurrence of Side Effects Associated with IL-12 in Liver Injury
2.5. Radiation Therapy Did Not Enhance the Anti-Tumor Effect of IL-12 Immunotherapy on Distant Tumors
2.6. Treatment with IL-12 Resulted in the Dysfunction of Tumor-Infiltrating T Cells
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Cell Line Culture
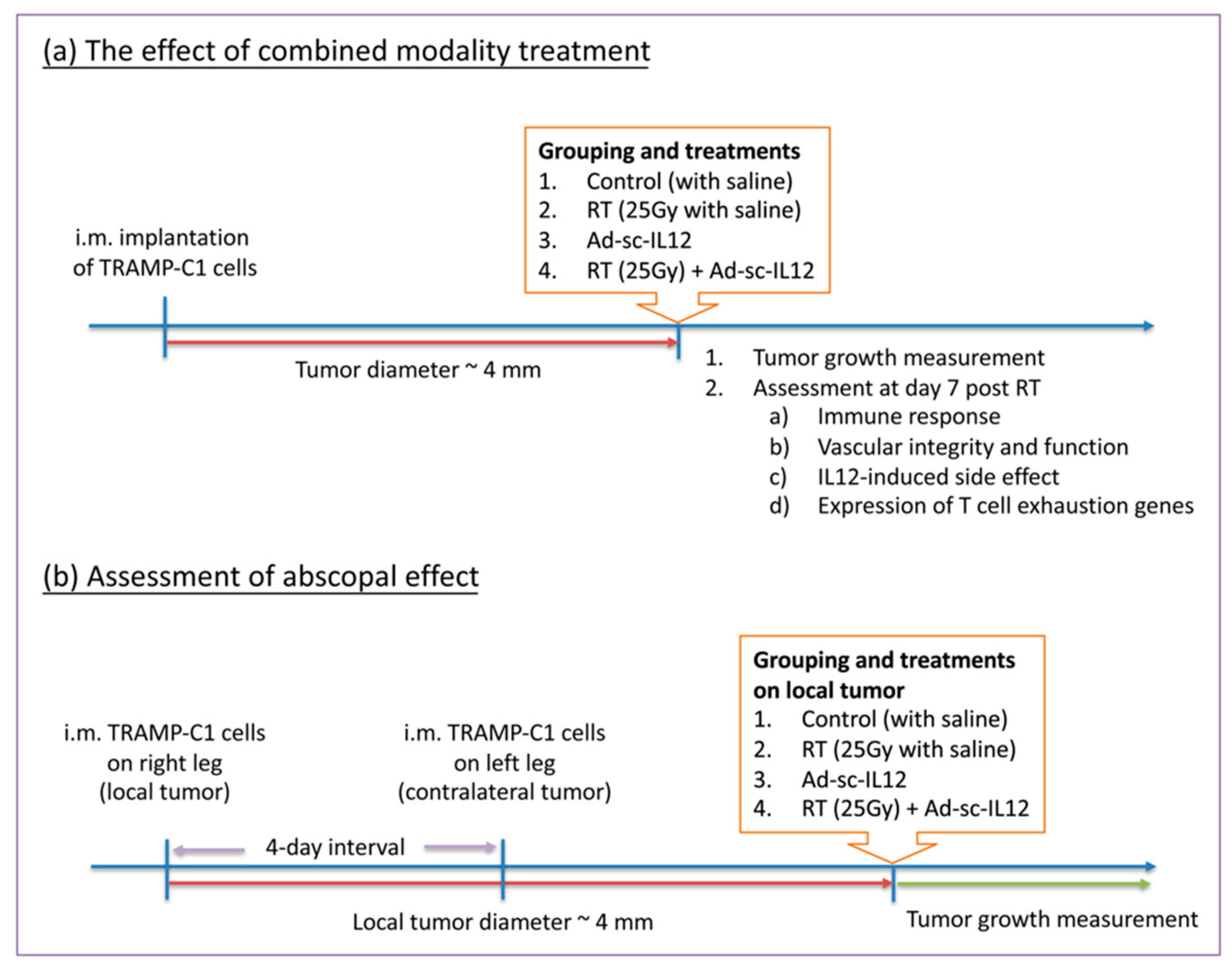
4.3. Tumor Inoculation and Treatment
4.4. Flow Cytometry
4.5. IL-12 and IFN-γ Measurement
4.6. Immunohistochemical Analysis
4.7. Liver Damage Analysis
4.8. RNA Isolation and Real-Time PCR
4.9. Statistics
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boettcher, A.N.; Usman, A.; Morgans, A.; VanderWeele, D.J.; Sosman, J.; Wu, J.D. Past, Current, and Future of Immunotherapies for Prostate Cancer. Front. Oncol. 2019, 9, 884. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Chargari, C.; Bauduceau, O.; Fayolle, M.; Ceccaldi, B.; Prat, F.; Le Moulec, S.; Vedrine, L. Pancreatic metastasis from prostate cancer. Case Rep. Med. 2010, 2010, 826273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gannot, G.; Richardson, A.M.; Rodriguez-Canales, J.; Pinto, P.A.; Merino, M.J.; Chuaqui, R.F.; Gillespie, J.W.; Emmert-Buck, M.R. Decrease in CD8+ lymphocyte number and altered cytokine profile in human prostate cancer. Am. J. Cancer Res. 2011, 1, 120–127. [Google Scholar] [PubMed]
- Patel, D.; McKay, R.; Parsons, J.K. Immunotherapy for Localized Prostate Cancer: The Next Frontier? Urol. Clin. N. Am. 2020, 47, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Gevensleben, H.; Dietrich, D.; Golletz, C.; Steiner, S.; Jung, M.; Thiesler, T.; Majores, M.; Stein, J.; Uhl, B.; Muller, S.; et al. The Immune Checkpoint Regulator PD-L1 Is Highly Expressed in Aggressive Primary Prostate Cancer. Clin. Cancer Res. 2016, 22, 1969–1977. [Google Scholar] [CrossRef] [Green Version]
- Ahn, G.O.; Tseng, D.; Liao, C.H.; Dorie, M.J.; Czechowicz, A.; Brown, J.M. Inhibition of Mac-1 (CD11b/CD18) enhances tumor response to radiation by reducing myeloid cell recruitment. Proc. Natl. Acad. Sci. USA 2010, 107, 8363–8368. [Google Scholar] [CrossRef] [Green Version]
- Kozin, S.V.; Kamoun, W.S.; Huang, Y.; Dawson, M.R.; Jain, R.K.; Duda, D.G. Recruitment of myeloid but not endothelial precursor cells facilitates tumor regrowth after local irradiation. Cancer Res. 2010, 70, 5679–5685. [Google Scholar] [CrossRef] [Green Version]
- Meng, Y.; Beckett, M.A.; Liang, H.; Mauceri, H.J.; van Rooijen, N.; Cohen, K.S.; Weichselbaum, R.R. Blockade of tumor necrosis factor alpha signaling in tumor-associated macrophages as a radiosensitizing strategy. Cancer Res. 2010, 70, 1534–1543. [Google Scholar] [CrossRef] [Green Version]
- Trinchieri, G.; Rengaraju, M.; D’Andrea, A.; Valiante, N.M.; Kubin, M.; Aste, M.; Chehimi, J. Producer cells of interleukin 12. Parasitol. Today 1993, 9, 97. [Google Scholar] [CrossRef]
- Kobayashi, M.; Fitz, L.; Ryan, M.; Hewick, R.M.; Clark, S.C.; Chan, S.; Loudon, R.; Sherman, F.; Perussia, B.; Trinchieri, G. Identification and purification of natural killer cell stimulatory factor (NKSF), a cytokine with multiple biologic effects on human lymphocytes. J. Exp. Med. 1989, 170, 827–845. [Google Scholar] [CrossRef]
- Stern, A.S.; Podlaski, F.J.; Hulmes, J.D.; Pan, Y.C.; Quinn, P.M.; Wolitzky, A.G.; Familletti, P.C.; Stremlo, D.L.; Truitt, T.; Chizzonite, R.; et al. Purification to homogeneity and partial characterization of cytotoxic lymphocyte maturation factor from human B-lymphoblastoid cells. Proc. Natl. Acad. Sci. USA 1990, 87, 6808–6812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubler, U.; Chua, A.O.; Schoenhaut, D.S.; Dwyer, C.M.; McComas, W.; Motyka, R.; Nabavi, N.; Wolitzky, A.G.; Quinn, P.M.; Familletti, P.C.; et al. Coexpression of two distinct genes is required to generate secreted bioactive cytotoxic lymphocyte maturation factor. Proc. Natl. Acad. Sci. USA 1991, 88, 4143–4147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, S.F.; Temple, P.A.; Kobayashi, M.; Young, D.; Dicig, M.; Lowe, L.; Dzialo, R.; Fitz, L.; Ferenz, C.; Hewick, R.M.; et al. Cloning of cDNA for natural killer cell stimulatory factor, a heterodimeric cytokine with multiple biologic effects on T and natural killer cells. J. Immunol. 1991, 146, 3074–3081. [Google Scholar] [PubMed]
- Jacobson, N.G.; Szabo, S.J.; Weber-Nordt, R.M.; Zhong, Z.; Schreiber, R.D.; Darnell, J.E., Jr.; Murphy, K.M. Interleukin 12 signaling in T helper type 1 (Th1) cells involves tyrosine phosphorylation of signal transducer and activator of transcription (Stat) 3 and Stat4. J. Exp. Med. 1995, 181, 1755–1762. [Google Scholar] [CrossRef] [PubMed]
- Zeh, H.J., 3rd; Hurd, S.; Storkus, W.J.; Lotze, M.T. Interleukin-12 promotes the proliferation and cytolytic maturation of immune effectors: Implications for the immunotherapy of cancer. J. Immunother. Emphas. Tumor Immunol. 1993, 14, 155–161. [Google Scholar] [CrossRef]
- Nguyen, Q.H.; Roberts, R.L.; Ank, B.J.; Lin, S.J.; Lau, C.K.; Stiehm, E.R. Enhancement of antibody-dependent cellular cytotoxicity of neonatal cells by interleukin-2 (IL-2) and IL-12. Clin. Diagn. Lab. Immunol. 1998, 5, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.; Umezu, Y.; Saijo, Y.; Satoh, G.; Abe, Y.; Satoh, K.; Nukiwa, T. Exogenous recombinant human IL-12 augments MHC class I antigen expression on human cancer cells in vitro. Tohoku J. Exp. Med. 1998, 185, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Su, W.; Ito, T.; Oyama, T.; Kitagawa, T.; Yamori, T.; Fujiwara, H.; Matsuda, H. The direct effect of IL-12 on tumor cells: IL-12 acts directly on tumor cells to activate NF-kappaB and enhance IFN-gamma-mediated STAT1 phosphorylation. Biochem. Biophys. Res. Commun. 2001, 280, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Cheng, F.; Ma, T.T.; Xiong, H.Y.; Li, Z.W.; Xie, C.L.; Liu, C.Y.; Tu, Z.G. Interleukin-12 inhibits the hepatocellular carcinoma growth by inducing macrophage polarization to the M1-like phenotype through downregulation of Stat-3. Mol. Cell. Biochem. 2016, 415, 157–168. [Google Scholar] [CrossRef]
- Sgadari, C.; Angiolillo, A.L.; Tosato, G. Inhibition of angiogenesis by interleukin-12 is mediated by the interferon-inducible protein 10. Blood 1996, 87, 3877–3882. [Google Scholar] [CrossRef] [Green Version]
- Kanegane, C.; Sgadari, C.; Kanegane, H.; Teruya-Feldstein, J.; Yao, L.; Gupta, G.; Farber, J.M.; Liao, F.; Liu, L.; Tosato, G. Contribution of the CXC chemokines IP-10 and Mig to the antitumor effects of IL-12. J. Leukoc. Biol. 1998, 64, 384–392. [Google Scholar] [CrossRef]
- Brunda, M.J.; Luistro, L.; Warrier, R.R.; Wright, R.B.; Hubbard, B.R.; Murphy, M.; Wolf, S.F.; Gately, M.K. Antitumor and antimetastatic activity of interleukin 12 against murine tumors. J. Exp. Med. 1993, 178, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.P.; Trinchieri, G. Interleukin-12 in anti-tumor immunity and immunotherapy. Cytokine Growth Factor Rev. 2002, 13, 155–168. [Google Scholar] [CrossRef]
- Janát-Amsbury, M.M.; Yockman, J.W.; Lee, M.; Kern, S.; Furgeson, D.Y.; Bikram, M.; Kim, S.W. Combination of local, nonviral IL12 gene therapy and systemic paclitaxel treatment in a metastatic breast cancer model. Mol. Ther. 2004, 9, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Seong, J.; Oh, H.J.; Koom, W.S.; Choi, K.J.; Yun, C.O. A novel combination treatment of armed oncolytic adenovirus expressing IL-12 and GM-CSF with radiotherapy in murine hepatocarcinoma. J. Radiat. Res. 2011, 52, 646–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, F.; Jelas, I.; Oehme, M.; Huber, S.M.; Sonntag, K.; Welker, C.; Gillies, S.D.; Strittmatter, W.; Zips, D.; Handgretinger, R.; et al. Tumor-targeted IL-12 combined with local irradiation leads to systemic tumor control via abscopal effects in vivo. Oncoimmunology 2017, 6, e1323161. [Google Scholar] [CrossRef] [Green Version]
- Leonard, J.P.; Sherman, M.L.; Fisher, G.L.; Buchanan, L.J.; Larsen, G.; Atkins, M.B.; Sosman, J.A.; Dutcher, J.P.; Vogelzang, N.J.; Ryan, J.L. Effects of single-dose interleukin-12 exposure on interleukin-12-associated toxicity and interferon-gamma production. Blood 1997, 90, 2541–2548. [Google Scholar]
- Car, B.D.; Eng, V.M.; Lipman, J.M.; Anderson, T.D. The toxicology of interleukin-12: A review. Toxicol. Pathol. 1999, 27, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.S.; Chen, F.H.; Wang, C.C.; Huang, H.L.; Jung, S.M.; Wu, C.J.; Lee, C.C.; McBride, W.H.; Chiang, C.S.; Hong, J.H. Macrophages from irradiated tumors express higher levels of iNOS, arginase-I and COX-2, and promote tumor growth. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 499–507. [Google Scholar] [CrossRef]
- Chen, F.H.; Chiang, C.S.; Wang, C.C.; Tsai, C.S.; Jung, S.M.; Lee, C.C.; McBride, W.H.; Hong, J.H. Radiotherapy decreases vascular density and causes hypoxia with macrophage aggregation in TRAMP-C1 prostate tumors. Clin. Cancer Res. 2009, 15, 1721–1729. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.Y.; Chen, F.H.; Wang, C.C.; Yu, C.F.; Chiang, C.S.; Hong, J.H. Role of Myeloid-Derived Suppressor Cells in High-Dose-Irradiated TRAMP-C1 Tumors: A Therapeutic Target and an Index for Assessing Tumor Microenvironment. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1547–1558. [Google Scholar] [CrossRef]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Gately, M.K.; Gubler, U.; Brunda, M.J.; Nadeau, R.R.; Anderson, T.D.; Lipman, J.M.; Sarmiento, U. Interleukin-12: A cytokine with therapeutic potential in oncology and infectious diseases. Ther. Immunol. 1994, 1, 187–196. [Google Scholar] [PubMed]
- Sarmiento, U.M.; Riley, J.H.; Knaack, P.A.; Lipman, J.M.; Becker, J.M.; Gately, M.K.; Chizzonite, R.; Anderson, T.D. Biologic effects of recombinant human interleukin-12 in squirrel monkeys (Sciureus saimiri). Lab. Investig. 1994, 71, 862–873. [Google Scholar] [PubMed]
- Schilbach, K.; Alkhaled, M.; Welker, C.; Eckert, F.; Blank, G.; Ziegler, H.; Sterk, M.; Müller, F.; Sonntag, K.; Wieder, T.; et al. Cancer-targeted IL-12 controls human rhabdomyosarcoma by senescence induction and myogenic differentiation. Oncoimmunology 2015, 4, e1014760. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Li, X.; Wang, J.; Gao, D.; Li, Y.; Li, H.; Chu, Y.; Zhang, Z.; Liu, H.; Jiang, G.; et al. Re-designing Interleukin-12 to enhance its safety and potential as an anti-tumor immunotherapeutic agent. Nat. Commun. 2017, 8, 1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portielje, J.E.; Kruit, W.H.; Schuler, M.; Beck, J.; Lamers, C.H.; Stoter, G.; Huber, C.; de Boer-Dennert, M.; Rakhit, A.; Bolhuis, R.L.; et al. Phase I study of subcutaneously administered recombinant human interleukin 12 in patients with advanced renal cell cancer. Clin. Cancer Res. 1999, 5, 3983–3989. [Google Scholar]
- Wu, C.J.; Tsai, Y.T.; Lee, I.J.; Wu, P.Y.; Lu, L.S.; Tsao, W.S.; Huang, Y.J.; Chang, C.C.; Ka, S.M.; Tao, M.H. Combination of radiation and interleukin 12 eradicates large orthotopic hepatocellular carcinoma through immunomodulation of tumor microenvironment. Oncoimmunology 2018, 7, e1477459. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.Z.; Grote, D.M.; Ziesmer, S.C.; Niki, T.; Hirashima, M.; Novak, A.J.; Witzig, T.E.; Ansell, S.M. IL-12 upregulates TIM-3 expression and induces T cell exhaustion in patients with follicular B cell non-Hodgkin lymphoma. J. Clin. Investig. 2012, 122, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.T.; Chen, D.W.; Dougherty, G.J.; McBride, W.H. Adenoviral interleukin-3 gene-radiation therapy for prostate cancer in mouse model. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 579–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philippou, Y.; Sjoberg, H.T.; Murphy, E.; Alyacoubi, S.; Jones, K.I.; Gordon-Weeks, A.N.; Phyu, S.; Parkes, E.E.; Gillies McKenna, W.; Lamb, A.D.; et al. Impacts of combining anti-PD-L1 immunotherapy and radiotherapy on the tumour immune microenvironment in a murine prostate cancer model. Br. J. Cancer 2020, 123, 1089–1100. [Google Scholar] [CrossRef] [PubMed]
- Dudzinski, S.O.; Cameron, B.D.; Wang, J.; Rathmell, J.C.; Giorgio, T.D.; Kirschner, A.N. Combination immunotherapy and radiotherapy causes an abscopal treatment response in a mouse model of castration resistant prostate cancer. J. Immunother. Cancer 2019, 7, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Name | Sequence |
|---|---|
| β-actin forward | ACCCTAAGGCCAACCGTGAA |
| β-actin reverse | ATGGCGTGAGGGAGAGCATAG |
| PD-L1 forward | GCTCCAAAGGACTTGTACGTG |
| PD-L1 reverse | TGATCTGAAGGGCAGCATTTC |
| PD-1 forward | TGATCTGAAGGGCAGCATTTC |
| PD-1 reverse | CATTTGCTCCCTCTGACACTG |
| TIM-3 forward | CCACGGAGAGAAATGGTTC |
| TIM-3 reverse | CATCAGCCCATGTGGAAAT |
| LAG-3 forward | CTGGGACTGCTTTGGGAAG |
| LAG-3 reverse | GGTTGATGTTGCCAGATAACCC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.-F.; Chang, C.-H.; Wang, C.-C.; Hong, J.-H.; Chiang, C.-S.; Chen, F.-H. Local Interleukin-12 Treatment Enhances the Efficacy of Radiation Therapy by Overcoming Radiation-Induced Immune Suppression. Int. J. Mol. Sci. 2021, 22, 10053. https://doi.org/10.3390/ijms221810053
Yu C-F, Chang C-H, Wang C-C, Hong J-H, Chiang C-S, Chen F-H. Local Interleukin-12 Treatment Enhances the Efficacy of Radiation Therapy by Overcoming Radiation-Induced Immune Suppression. International Journal of Molecular Sciences. 2021; 22(18):10053. https://doi.org/10.3390/ijms221810053
Chicago/Turabian StyleYu, Ching-Fang, Chun-Hsiang Chang, Chun-Chieh Wang, Ji-Hong Hong, Chi-Shiun Chiang, and Fang-Hsin Chen. 2021. "Local Interleukin-12 Treatment Enhances the Efficacy of Radiation Therapy by Overcoming Radiation-Induced Immune Suppression" International Journal of Molecular Sciences 22, no. 18: 10053. https://doi.org/10.3390/ijms221810053