
Identification of Candidate Biomarker and Drug Targets for Improving Endometrial Cancer Racial Disparities

 , , ,
, , , 
Abstract
:1. Introduction
2. Results
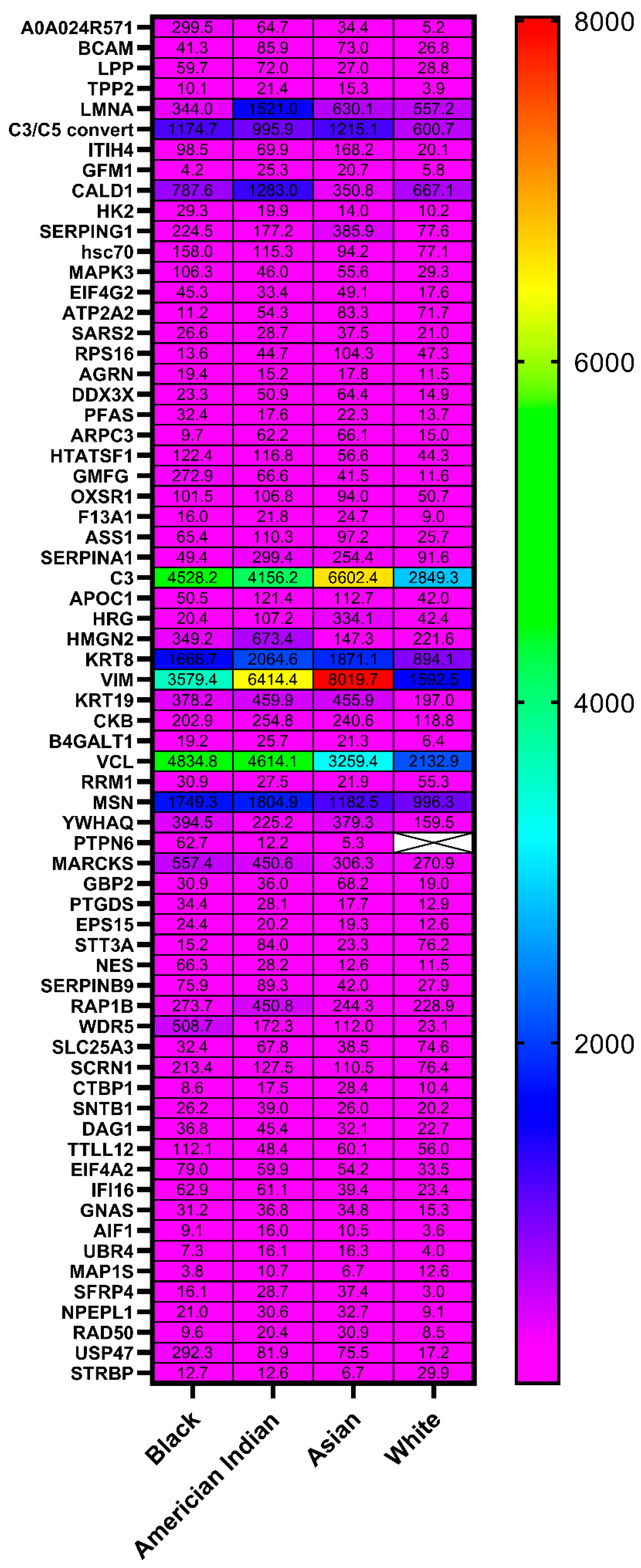
2.1. Proteomic Discovery
2.2. Bioinformatic Analysis
3. Discussion
4. Materials and Methods
4.1. Isolation of Proteins from Endometrial Cancer Specimens
4.2. Mass Spectrometry Analysis
4.3. Statistical Analysis
4.4. Bioinformatics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sud, S.; Holmes, J.; Eblan, M.; Chen, R.; Jones, E. Clinical characteristics associated with racial disparities in endometrial cancer outcomes: A surveillance, epidemiology and end results analysis. Gynecol. Oncol. 2018, 148, 349–356. [Google Scholar] [CrossRef]
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. J. Natl. Cancer Inst. 2017, 109, djx030. [Google Scholar] [CrossRef]
- Rodriguez, V.E.; LeBron, A.M.W.; Chang, J.; Bristow, R.E. Racial-Ethnic and Socioeconomic Disparities in Guideline-Adherent Treatment for Endometrial Cancer. Obstet. Gynecol. 2021, 138, 21–31. [Google Scholar] [CrossRef]
- Fucinari, J.; Elshaikh, M.A.; Ruterbusch, J.J.; Khalil, R.; Dyson, G.; Shultz, D.; Ali-Fehmi, R.; Cote, M.L. The impact of race, comorbid conditions and obesity on survival endpoints in women with high grade endometrial carcinoma. Gynecol. Oncol. 2021, 162, 134–141. [Google Scholar] [CrossRef]
- Javadian, P.; Washington, C.; Mukasa, S.; Benbrook, D.M. Histopathologic, Genetic and Molecular Characterization of Endometrial Cancer Racial Disparity. Cancers 2021, 13, 1900. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research, N.; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Bateman, N.W.; Dubil, E.A.; Wang, G.; Hood, B.L.; Oliver, J.M.; Litzi, T.A.; Gist, G.D.; Mitchell, D.A.; Blanton, B.; Phippen, N.T.; et al. Race-specific molecular alterations correlate with differential outcomes for black and white endometrioid endometrial cancer patients. Cancer 2017, 123, 4004–4012. [Google Scholar] [CrossRef] [Green Version]
- Dubil, E.A.; Tian, C.; Wang, G.; Tarney, C.M.; Bateman, N.W.; Levine, D.A.; Conrads, T.P.; Hamilton, C.A.; Maxwell, G.L.; Darcy, K.M. Racial disparities in molecular subtypes of endometrial cancer. Gynecol. Oncol. 2018, 149, 106–116. [Google Scholar] [CrossRef]
- Ferguson, S.E.; Olshen, A.B.; Levine, D.A.; Viale, A.; Barakat, R.R.; Boyd, J. Molecular profiling of endometrial cancers from African–American and Caucasian women. Gynecol. Oncol. 2006, 101, 209–213. [Google Scholar] [CrossRef]
- Maxwell, G.L.; Allard, J.; Gadisetti, C.V.R.; Litzi, T.; Casablanca, Y.; Chandran, U.; Darcy, K.M.; Levine, D.A.; Berchuck, A.; Hamilton, C.A.; et al. Transcript expression in endometrial cancers from Black and White patients. Gynecol. Oncol. 2013, 130, 169–173. [Google Scholar] [CrossRef]
- Available online: http://ualcan.path.uab.edu (accessed on 29 June 2022).
- Rabinovich, S.; Adler, L.; Yizhak, K.; Sarver, A.; Silberman, A.; Agron, S.; Stettner, N.; Sun, Q.; Brandis, A.; Helbling, D.; et al. Diversion of aspartate in ASS1-deficient tumours fosters de novo pyrimidine synthesis. Nature 2015, 527, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Bendell, J.C.; Strauss, J.F.; Fakih, M.; McRee, A.J.; Hendifar, A.E.; Rosen, L.S.; Cercek, A.; Rowinsky, E.K.; Szarek, M.; Gonsalves, F.; et al. Phase I monotherapy dose escalation of RGX-202, a first-in-class oral inhibitor of the SLC6a8/CKB pathway, in patients with advanced gastrointestinal (GI) solid tumors. J. Clin. Oncol. 2020, 38, 3504. [Google Scholar] [CrossRef]
- Kurth, I.; Yamaguchi, N.; Andreu-Agullo, C.; Tian, H.S.; Sridhar, S.; Takeda, S.; Gonsalves, F.C.; Loo, J.M.; Barlas, A.; Manova-Todorova, K.; et al. Therapeutic targeting of SLC6A8 creatine transporter suppresses colon cancer progression and modulates human creatine levels. Sci. Adv. 2021, 7, eabi7511. [Google Scholar] [CrossRef]
- Study of eFT226 in Subjects With Selected Advanced Solid Tumor Malignancies (Zotatifin). Available online: https://www.clinicaltrials.gov/ct2/show/NCT04092673 (accessed on 29 June 2022).
- Available online: https://clinicaltrials.gov/ct2/show/NCT04898634?term=HK2&draw=2&rank=7 (accessed on 29 June 2022).
- Sullivan, R.J.; Infante, J.R.; Janku, F.; Wong, D.J.L.; Sosman, J.A.; Keedy, V.; Patel, M.R.; Shapiro, G.I.; Mier, J.W.; Tolcher, A.W.; et al. First-in-Class ERK1/2 Inhibitor Ulixertinib (BVD-523) in Patients with MAPK Mutant Advanced Solid Tumors: Results of a Phase I Dose-Escalation and Expansion Study. Cancer Discov. 2018, 8, 184–195. [Google Scholar] [CrossRef] [Green Version]
- Enasescu, D.A.; Moisescu, M.G.; Imre, M.; Greabu, M.; Ripszky Totan, A.; Stanescu-Spinu, I.; Burcea, M.; Albu, C.; Miricescu, D. Lutein Treatment Effects on the Redox Status and Metalloproteinase-9 (MMP-9) in Oral Cancer Squamous Cells-Are There Therapeutical Hopes? Materials 2021, 14, 2968. [Google Scholar] [CrossRef]
- Natsumeda, Y.; Ikegami, T.; Olah, E.; Weber, G. Significance of purine salvage in circumventing the action of antimetabolites in rat hepatoma cells. Cancer Res. 1989, 49, 88–92. [Google Scholar]
- Roy, S.; Ghosh, S.; Mallick, P.; Maity, P. Acivicin with glutaminase regulates proliferation and invasion of human MCF-7 and OAW-42 cells--an in vitro study. Indian J. Exp. Biol. 2008, 46, 22–26. [Google Scholar]
- Willoughby, L.F.; Schlosser, T.; Manning, S.A.; Parisot, J.P.; Street, I.P.; Richardson, H.E.; Humbert, P.O.; Brumby, A.M. An in vivo large-scale chemical screening platform using Drosophila for anti-cancer drug discovery. Dis. Models Mech. 2013, 6, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Peters, G.J. Antipyrimidine effects of five different pyrimidine de novo synthesis inhibitors in three head and neck cancer cell lines. Nucleosides Nucleotides Nucleic Acids 2018, 37, 329–339. [Google Scholar] [CrossRef]
- Sodium Stibogluconate and IFNa-2b Followed by CDDP, VLB and DTIC Treating Pts. With Advanced Melanoma or Other Cancers. Available online: https://clinicaltrials.gov/ct2/show/NCT00498979?term=PTPN6&draw=2&rank=1 (accessed on 29 June 2022).
- Copper (Cu) 64-DOTA-Trastuzumab PET Imaging in Predicting Response to Treatment with Trastuzumab and Pertuzumab Before Surgery in Patients with HER2 Positive Breast Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02827877?term=serpina&cond=Cancer&draw=2&rank=1 (accessed on 29 June 2022).
- Chandrashekar, D.S.; Bashel, B.; Balasubramanya, S.A.H.; Creighton, C.J.; Rodriguez, I.P.; Chakravarthi, B.V.S.K.; Varambally, S. UALCAN: A portal for facilitating tumor subgroup gene expression and survival analyses. Neoplasia 2017, 19, 649–658. [Google Scholar] [CrossRef]
- Ohshima, K.; Nojima, S.; Tahara, S.; Kurashige, M.; Hori, Y.; Hagiwara, K.; Okuzaki, D.; Oki, S.; Wada, N.; Ikeda, J.I.; et al. Argininosuccinate Synthase 1-Deficiency Enhances the Cell Sensitivity to Arginine through Decreased DEPTOR Expression in Endometrial Cancer. Sci. Rep. 2017, 7, 45504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillon, B.J.; Prieto, V.G.; Curley, S.A.; Ensor, C.M.; Holtsberg, F.W.; Bomalaski, J.S.; Clark, M.A. Incidence and distribution of argininosuccinate synthetase deficiency in human cancers. Cancer 2004, 100, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Tsai, W.-B.; Wangpaichitr, M.; Tsukamoto, T.; Savaraj, N.; Feun, L.G.; Kuo, M.T. Arginine Deiminase Resistance in Melanoma Cells Is Associated with Metabolic Reprogramming, Glucose Dependence, and Glutamine Addiction. Molecular Cancer Ther. 2013, 12, 2581–2590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slomovitz, B.M.; Jiang, Y.; Yates, M.S.; Soliman, P.T.; Johnston, T.; Nowakowski, M.; Levenback, C.; Zhang, Q.; Ring, K.; Munsell, M.F.; et al. Phase II study of everolimus and letrozole in patients with recurrent endometrial carcinoma. J. Clin. Oncol. 2015, 33, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Vale, C.L.; Tierney, J.; Bull, S.J.; Symonds, P.R. Chemotherapy for advanced, recurrent or metastatic endometrial carcinoma. Cochrane Database Syst. Rev. 2012, 2012, CD003915. [Google Scholar] [CrossRef]
- Cheung, E.C.; Ludwig, R.L.; Vousden, K.H. Mitochondrial localization of TIGAR under hypoxia stimulates HK2 and lowers ROS and cell death. Proc. Natl. Acad. Sci. USA 2012, 109, 20491–20496. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Zeng, J.; Xie, R.; Schulz, M.J.; Tedesco, R.; Qu, J.; Erhard, K.F.; Mack, J.F.; Raha, K.; Rendina, A.R.; et al. Discovery of a Novel 2,6-Disubstituted Glucosamine Series of Potent and Selective Hexokinase 2 Inhibitors. ACS Med. Chem. Lett. 2016, 7, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Nawaz, M.H.; Ferreira, J.C.; Nedyalkova, L.; Zhu, H.; Carrasco-Lopez, C.; Kirmizialtin, S.; Rabeh, W.M. The catalytic inactivation of the N-half of human hexokinase 2 and structural and biochemical characterization of its mitochondrial conformation. Biosci. Rep. 2018, 38, BSR20171666. [Google Scholar] [CrossRef] [Green Version]
- Chiara, F.; Castellaro, D.; Marin, O.; Petronilli, V.; Brusilow, W.S.; Juhaszova, M.; Sollott, S.J.; Forte, M.; Bernardi, P.; Rasola, A. Hexokinase II detachment from mitochondria triggers apoptosis through the permeability transition pore independent of voltage-dependent anion channels. PLoS ONE 2008, 3, e1852. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Ma, A.; Jin, Y.; Pan, G.; Wang, C. LncRNA SNHG16 induced by TFAP2A modulates glycolysis and proliferation of endometrial carcinoma through miR-490-3p/HK2 axis. Am. J. Transl. Res. 2019, 11, 7137–7145. [Google Scholar]
- Cerella, C.; Dicato, M.; Diederich, M. Modulatory roles of glycolytic enzymes in cell death. Biochem. Pharmacol. 2014, 92, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Pajak, B.; Siwiak, E.; Sołtyka, M.; Priebe, A.; Zieliński, R.; Fokt, I.; Ziemniak, M.; Jaśkiewicz, A.; Borowski, R.; Domoradzki, T.; et al. 2-Deoxy-d-Glucose and Its Analogs: From Diagnostic to Therapeutic Agents. Int. J. Mol. Sci. 2019, 21, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Li, J.; Wang, F.; Hu, J.; Wang, S.; Sun, Y. 2-Deoxy-D-glucose targeting of glucose metabolism in cancer cells as a potential therapy. Cancer Lett. 2014, 355, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Akin, O. (Ed.) Atlas of Gynecologic Oncology Imaging; Springer: New York, NY, USA, 2014. [Google Scholar]
- Xi, H.; Kurtoglu, M.; Lampidis, T.J. The wonders of 2-deoxy-D-glucose. IUBMB Life 2014, 66, 110–121. [Google Scholar] [CrossRef]
- Hernlund, E.; Ihrlund, L.S.; Khan, O.; Ates, Y.O.; Linder, S.; Panaretakis, T.; Shoshan, M.C. Potentiation of chemotherapeutic drugs by energy metabolism inhibitors 2-deoxyglucose and etomoxir. Int. J. Cancer 2008, 123, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Hirota, H.; Belfi, C.A.; Berger, S.J.; Berger, N.A. Hypersensitivity to DNA cross-linking agents associated with up-regulation of glucose-regulated stress protein GRP78. Cancer Res. 1997, 57, 5112–5116. [Google Scholar]
- Yamada, M.; Tomida, A.; Yun, J.; Cai, B.; Yoshikawa, H.; Taketani, Y.; Tsuruo, T. Cellular sensitization to cisplatin and carboplatin with decreased removal of platinum-DNA adduct by glucose-regulated stress. Cancer Chemother Pharm. 1999, 44, 59–64. [Google Scholar] [CrossRef]
- Mese, H.; Sasaki, A.; Nakayama, S.; Yokoyama, S.; Sawada, S.; Ishikawa, T.; Matsumura, T. Analysis of cellular sensitization with cisplatin-induced apoptosis by glucose-starved stress in cisplatin-sensitive and -resistant A431 cell line. Anticancer Res. 2001, 21, 1029–1033. [Google Scholar]
- Singh, S.P.; Gao, Y.; Singh, L.D.; Kunapuli, S.P.; Ravindra, R. Role of microtubules in glucose uptake by C6 glioma cells. Pharm. Toxicol. 1998, 83, 83–89. [Google Scholar] [CrossRef]
- Yan, L.; Tu, B.; Yao, J.; Gong, J.; Carugo, A.; Bristow, C.A.; Wang, Q.; Zhu, C.; Dai, B.; Kang, Y.; et al. Targeting Glucose Metabolism Sensitizes Pancreatic Cancer to MEK Inhibition. Cancer Res. 2021, 81, 4054–4065. [Google Scholar] [CrossRef]
- Stein, M.; Lin, H.; Jeyamohan, C.; Dvorzhinski, D.; Gounder, M.; Bray, K.; Eddy, S.; Goodin, S.; White, E.; Dipaola, R.S. Targeting tumor metabolism with 2-deoxyglucose in patients with castrate-resistant prostate cancer and advanced malignancies. Prostate 2010, 70, 1388–1394. [Google Scholar] [CrossRef] [Green Version]
- Raez, L.E.; Papadopoulos, K.; Ricart, A.D.; Chiorean, E.G.; Dipaola, R.S.; Stein, M.N.; Rocha Lima, C.M.; Schlesselman, J.J.; Tolba, K.; Langmuir, V.K.; et al. A phase I dose-escalation trial of 2-deoxy-D-glucose alone or combined with docetaxel in patients with advanced solid tumors. Cancer Chemother Pharm. 2013, 71, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Kashima, H.; Shiozawa, T.; Miyamoto, T.; Suzuki, A.; Uchikawa, J.; Kurai, M.; Konishi, I. Autocrine stimulation of IGF1 in estrogen-induced growth of endometrial carcinoma cells: Involvement of the mitogen-activated protein kinase pathway followed by up-regulation of cyclin D1 and cyclin E. Endocr Relat Cancer 2009, 16, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ninomiya, Y.; Kato, K.; Takahashi, A.; Ueoka, Y.; Kamikihara, T.; Arima, T.; Matsuda, T.; Kato, H.; Nishida, J.; Wake, N. K-Ras and H-Ras activation promote distinct consequences on endometrial cell survival. Cancer Res. 2004, 64, 2759–2765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germann, U.A.; Furey, B.F.; Markland, W.; Hoover, R.R.; Aronov, A.M.; Roix, J.J.; Hale, M.; Boucher, D.M.; Sorrell, D.A.; Martinez-Botella, G.; et al. Targeting the MAPK Signaling Pathway in Cancer: Promising Preclinical Activity with the Novel Selective ERK1/2 Inhibitor BVD-523 (Ulixertinib). Mol. Cancer Ther. 2017, 16, 2351–2363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, G.; Campanini, N.; Goldoni, M.; Rodolfi, A.M.; Brigati, F.; Merisio, C.; Berretta, R. Immunohistochemical Detection of Hematopoietic Cell-specific Protein-Tyrosine Phosphatase (Tyrosine Phosphatase SHP-1) in a Series of Endometrioid and Serous Endometrial Carcinoma. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Pathak, M.K.; Yi, T. Sodium stibogluconate is a potent inhibitor of protein tyrosine phosphatases and augments cytokine responses in hemopoietic cell lines. J. Immunol. 2001, 167, 3391–3397. [Google Scholar] [CrossRef] [Green Version]
- Yi, T.; Elson, P.; Mitsuhashi, M.; Jacobs, B.; Hollovary, E.; Budd, T.G.; Spiro, T.; Triozzi, P.; Borden, E.C. Phosphatase inhibitor, sodium stibogluconate, in combination with interferon (IFN) alpha 2b: Phase I trials to identify pharmacodynamic and clinical effects. Oncotarget 2011, 2, 1155–1164. [Google Scholar] [CrossRef] [Green Version]
- Pelletier, J.; Sonenberg, N. The Organizing Principles of Eukaryotic Ribosome Recruitment. Annu. Rev. Biochem. 2019, 88, 307–335. [Google Scholar] [CrossRef]
- Thompson, P.A.; Eam, B.; Young, N.P.; Fish, S.; Chen, J.; Barrera, M.; Howard, H.; Sung, E.; Parra, A.; Staunton, J.; et al. Targeting Oncogene mRNA Translation in B-Cell Malignancies with eFT226, a Potent and Selective Inhibitor of eIF4A. Mol. Cancer Ther. 2021, 20, 26–36. [Google Scholar] [CrossRef]
- Ernst, J.T.; Thompson, P.A.; Nilewski, C.; Sprengeler, P.A.; Sperry, S.; Packard, G.; Michels, T.; Xiang, A.; Tran, C.; Wegerski, C.J.; et al. Design of Development Candidate eFT226, a First in Class Inhibitor of Eukaryotic Initiation Factor 4A RNA Helicase. J. Med. Chem. 2020, 63, 5879–5955. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.D.; Oshlack, A. A scaling normalization method for differential expression analysis of RNA-seq data. Genome Biol. 2010, 11, R25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, M.D.; McCarthy, D.J.; Smyth, G.K. edgeR: A Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 2010, 26, 139–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Black (n:12) | White (n:12) | American Indian (n:12) | Asian (n:10) | p | |
|---|---|---|---|---|---|
| Age (yrs) | 63.6 ± 13.5 | 59.2 ± 6.2 | 58.1 ± 10.5 | 64.1 ± 12.5 | 0.45 |
| BMI | 39.2 ± 10.3 | 35.4 ± 7.1 | 42.2 ± 8.7 | 38.6 ± 8.4 | 0.27 |
| Smoking | 2 | 7 | 2 | 1 | 0.29 |
| Hypertension | 5 | 9 | 7 | 4 | 0.012 |
| Alcohol use | 1 | 2 | 1 | 0 | 0.84 |
| NSAID use | 1 | 0 | 1 | 0 | 0.15 |
| Cardiovascular disease | 3 | 3 | 5 | 2 | 0.21 |
| Autoimmune disease | 1 | 0 | 0 | 0 | 0.44 |
| Diabetes | 8 | 3 | 7 | 2 | 0.011 |
| Race | Gene IDs | |
|---|---|---|
| Higher Concentration | Lower Concentration | |
| Black | AIF1, AGRN, ASS1, CUL3, DAG1, DPYSL2, EHD1, EIF4A2, EIF4G2, EPS15, F13A1, GMFG, GFM1, HK2, HTATSF1 IFI16, MAPK3, NES, NPEPL1, OXSR1, PTPN6, PTGDS, PFAS, RAB5B, RAD50, SCRN1, SNX1, SNTB1, SERPINB9, SARS2, TPP2, UBR4, USP47, WDR5, YWHAQ, | ATP2A2, APOC1, MAP1S, RPL4, RPL23, RPS16, SERPINA1, STT3A, ZMYND8 |
| American Indian | AGRN, ASS1, AIF1, CLINT1, CALD1, DAG1, EIF4G2, EPS15, F13A1, GFM1, HK2, HMGN2, KRT19, NPEPL1, SNX1, SNTB1, SARS2, UBR4, USP47, TPP2, WDR5 | DX3X, MAP1S, PFAS |
| Asian | APOC1, CKB, EIF4G2, F13A1, GBP2, GFM1, HMGN2, KRT19, NPEPL1, RAB5B, SNTB1, SERPING1, SARS2, SERPINA1, UBR4, USP47, VIM, WDR5 | CLINT1, DDX3X, EIF3E, GBAS, IFI16, PTPN6, OXSR1, RPL5, SLC25A3, STRBP |
| Gene Symbol | Expression in Endometrial Cancer vs. Normal Tissue ¥ [11] | Biomarker-Driven Therapy | Disease or Use | Clinical Trial Phase | Impact on Endometrial Cancer Patient Survival (TCGA) † [11] | Expression in Our Study Cohort |
|---|---|---|---|---|---|---|
| ASS1 | Lower (p < 0.0001) | Rapamycin/ mTOR inhibtors, or fluorouracil (5-FU) [12] | Multiple cancers | Rapamycin Approved/Phase 2 | Worse outcome with higher expression | AI (High) W (Low) |
| CKB | Lower (p < 0.0001) | RGX-202 [13,14] | Gastrointestinal cancer | Phase 1 | No | A (High) W (low) |
| EIF4A2 | No significant difference | Zotatifin [15] | Solid tumors | Phase 1–2 | Worse outcome with higher expression | B (High) W (Low) |
| HK2 | Higher (p < 0.0001) | 2-DG and analogs [16] | Prostate cancer, PET imaging | Phase 2 | No | B and AI (High) W (Low) |
| MAPK3 | Lower (p < 0.0001) | Ulixertinib [17] | Solid tumors | Phase 2 | No | B (High) W (Low) |
| OXSR1 | No significant difference | Lutein [18] | Oral cancer | Preclinical | No | B (High) A (Low) |
| PFAS | Higher (p = 0.0002) | Acivicin [19,20,21,22] | Liver cancer | Preclinical | No | B (High) AI (Low) |
| PTPN6 | Higher (p < 0.0001) | Sodium stibogluconate [23] | Melanoma | Phase 1 | Worse outcome with higher expression | B (High) A (Low) |
| SERPINA1 | Lower (p < 0.0001) | Trastuzumab [24]. | Breast cancer | Phase 2 (Exploratory Biomarker) | No | A and AI (High) B (low) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javadian, P.; Xu, C.; Sjoelund, V.; Borden, L.E.; Garland, J.; Benbrook, D.M. Identification of Candidate Biomarker and Drug Targets for Improving Endometrial Cancer Racial Disparities. Int. J. Mol. Sci. 2022, 23, 7779. https://doi.org/10.3390/ijms23147779
Javadian P, Xu C, Sjoelund V, Borden LE, Garland J, Benbrook DM. Identification of Candidate Biomarker and Drug Targets for Improving Endometrial Cancer Racial Disparities. International Journal of Molecular Sciences. 2022; 23(14):7779. https://doi.org/10.3390/ijms23147779
Chicago/Turabian StyleJavadian, Pouya, Chao Xu, Virginie Sjoelund, Lindsay E. Borden, Justin Garland, and Doris Mangiaracina Benbrook. 2022. "Identification of Candidate Biomarker and Drug Targets for Improving Endometrial Cancer Racial Disparities" International Journal of Molecular Sciences 23, no. 14: 7779. https://doi.org/10.3390/ijms23147779
APA StyleJavadian, P., Xu, C., Sjoelund, V., Borden, L. E., Garland, J., & Benbrook, D. M. (2022). Identification of Candidate Biomarker and Drug Targets for Improving Endometrial Cancer Racial Disparities. International Journal of Molecular Sciences, 23(14), 7779. https://doi.org/10.3390/ijms23147779